51 - Congenital Posterolateral Diaphragmatic Hernias and Other Less Common Hernias of the Diaphragm in Infants and Children
Editors: Shields, Thomas W.; LoCicero, Joseph; Ponn, Ronald B.; Rusch, Valerie W.
Title: General Thoracic Surgery, 6th Edition
Copyright 2005 Lippincott Williams & Wilkins
> Table of Contents > Volume I - The Lung, Pleura, Diaphragm, and Chest Wall > Section XI - The Pleura > Chapter 62 - Thoracoplasty: Indications and Surgical Considerations
Chapter 62
Thoracoplasty: Indications and Surgical Considerations
Stanley C. Fell
The term thoracoplasty (TPL) refers to a spectrum of operations designed to reduce the volume of a hemithorax, achieved by multiple rib resections, allowing collapse of the chest wall and apposition of the parietal to the visceral or mediastinal pleura. These procedures have been used to obliterate a septic pleural space overlying unexpandable lung, to treat postpneumonectomy empyema, to compress cavitary pulmonary tuberculosis, and to reduce the pleural space when there is inadequate expansion of residual lung following pulmonary resection.
HISTORICAL CONTEXT
A detailed description of the development of TPL and its permutations is beyond the scope of this chapter and may be found in the writings of Alexander (1937), Hochberg (1960), and Meade (1961), from which this brief narrative is gleaned. Wide decostalization of the chest wall was employed by Estlander and Schede (1890) for the treatment of chronic empyema in the late 19th century, and the latter's procedure was used until the mid-20th century, when it was virtually abandoned because of its severe physiologic and cosmetic deformities, and replaced, when feasible, by decortication.
In 1819, Carson suggested that induced pneumothorax might promote healing of the diseased lung. Forlanini in 1882, having observed that clinical improvement sometimes occurred when spontaneous pneumothorax occurred in pulmonary tuberculosis, proposed and used artificial pneumothorax to collapse and compress these cavities. When induction of pneumothorax was unsuccessful because of adhesions, intrapleural pneumolysis was developed by Jacobeus in 1913. Other methods used to collapse the lung, such as phrenic nerve exeresis, pneumoperitoneum, and paraffin plombage, were inconsistently successful. In 1885, de Cerenville collapsed tuberculous cavities by resecting portions of the second and third ribs. In 1907, Friedrich resected ribs 2 through 9 in one stage. This procedure had an unacceptable level of morbidity and mortality even in its modifications by Sauerbruch. It remained for John Alexander, bedridden with spinal tuberculosis (Pott's disease) in 1925, to analyze the shortcomings of prior procedures and develop the operation that is used to this day as revised by Langston (1991).
INDICATIONS FOR THORACOPLASTY
In cases of tuberculosis, TPL was an operation suited for cavities in the upper portion of the lung, typically the apical and posterior segments of the upper lobe and the superior segment of the lower lobe. Large cavities in the apex of the lung and those situated medially in the paravertebral gutter are difficult to collapse by TPL. Cavities 5 cm or larger in diameter often could not be closed by TPL, and cavities that are distended because of partial bronchial obstruction (tension cavities) were also not responsive. Tuberculous bronchiectasis is another contraindication to TPL. Bilateral TPL is rarely performed but may be feasible if limited to three to five ribs on each side. Alexander (1937) reported cavitary closure in 93% of survivors, with a 10% mortality rate.
Indications for TPL have diminished considerably since the advent of decortication for unexpanded lung, intrathoracic muscle flap transposition for the treatment of empyema and bronchopleural fistula, and antibiotic therapy and pulmonary resection for tuberculosis. However, these procedures may fail. For example, decortication is doomed to failure if the lung is fibrotic and inexpansible. TPL can provide a simple, one-stage solution to a vexing problem. In cases where pulmonary resection for advanced lung cancer has been performed and complicated by bronchopleural fistula or empyema, the choice of muscle flap procedures versus
P.861
TPL must be considered. If the long-term prognosis for the patient is poor, he or she may be better served by a one-stage TPL rather than a multiple-stage muscle flap procedure and a prolonged period of hospitalization, as described by Pairolero and associates (1983).
To be effective, the classical extrapleural TPL requires that the parietal pleura be thin and pliable in order to obliterate the pleural space. This is not a relevant problem in the management of early bronchopleural fistula (BPF) and empyema. In chronic empyema, however well drained, the parietal pleura becomes so thick and stiff that space obliteration will not occur. Thus, the Grow (1946), Kergin (1953), and Andrews (1961) modifications of the TPL evolved.
ALEXANDER THORACOPLASTY FOR TUBERCULOSIS
In the last analysis, a thoracoplasty is used to close a pulmonary cavity that no other operations can close. John Alexander, 1937
The posterolateral TPL was originally performed in three stages, separated by 2 to 3 weeks in order to minimize the adverse effects of paradoxical chest wall motion on ventilation and on the ability to cough and expectorate (Fig.62-1). With the advent of antibiotic therapy for tuberculosis in 1945, and thus more localized disease, the stages were reduced to two. When TPL is performed for postpneumonectomy empyema, BPF, or incomplete lung expansion following lobectomy, it is a one-stage operation. The absence of lung under the TPL prevents the effects of chest wall paradoxic motion.
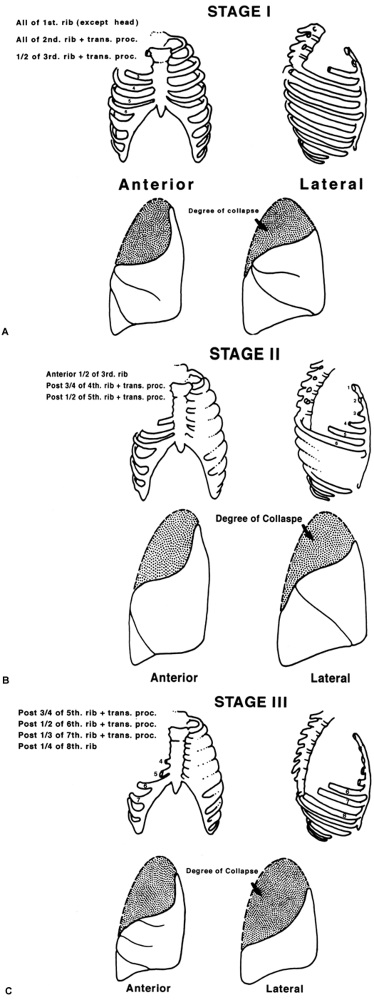 |
Fig. 62-1. Degrees of lung collapse after sequential stages of thoracoplasty for tuberculosis. Degrees of lung collapse after sequential stages of thoracoplasty for tuberculosis. |
Method
With the patient in the true lateral position under endotracheal anesthesia, heed Alexander's instruction: The uppermost arm should hang over the edge of the table so as to assist by its weight in the forward displacement of the scapula. The arm is protected by padding. Under no circumstances allow the anesthesiologist to fix or suspend the upper limb, since by so doing the scapula will invariably overhang and obscure the operative field. What follows is the technique of the Alexander TPL that I used in the 1950s in cases of sputum-positive pulmonary tuberculosis in patients deemed at high risk for resection
P.862
P.863
by reason of extent of disease or associated illness. Because several generations of thoracic surgeons have been trained in intercostal and muscle-sparing thoracotomies and have had little or no experience in the instrumentation required for TPL, the following may be of value. The Coryllos periosteal elevator is ideal for stripping the rib and invaluable for freeing the necks of ribs and the transverse processes. The Matson or Cameron Haight elevators are used for stripping both surfaces of the first rib (Fig. 62-2A). A sequestrum or lion-jaw bone-holding forceps is required to grasp the first rib after it is transected posteriorly (Fig. 62-2B). The ribs are transected with the conventional Bethune rib shears, and the Sauerbruch box-nosed rongeur is used to resect the rib necks and the transverse processes.
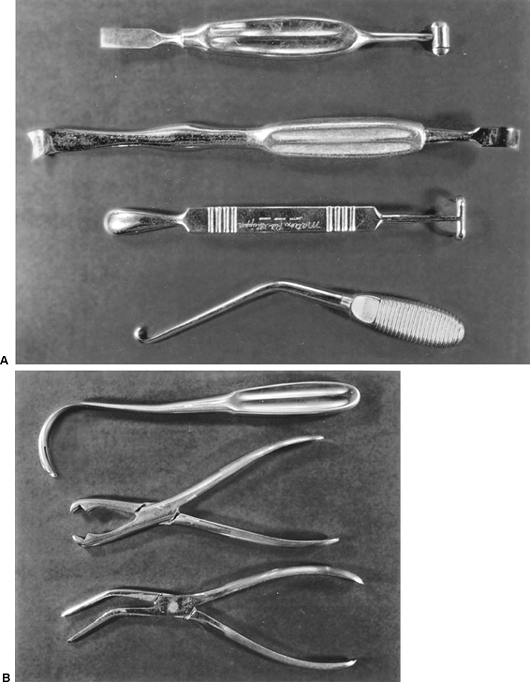 |
Fig. 62-2. A. From top to bottom: the Alexander, Coryllos, and Matteson elevators and the Sauerbruch first rib hook occasionally used for clearing the medial border of the first rib. B. From top to bottom: Semb retractor, lion-jaw forceps, sequestrum forceps. |
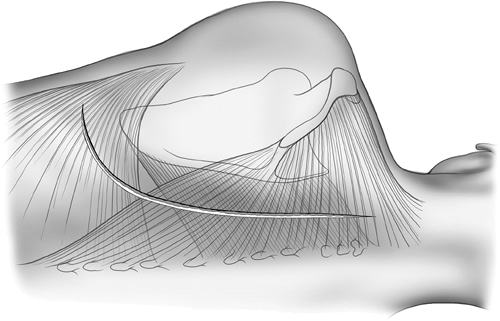 |
Fig. 62-3. Periscapular incision through the muscles of the chest wall. |
P.864
A periscapular incision is made commencing at the level of the first dorsal vertebra midway between the scapula and the spine and carried to two finger breadths below the angle of the scapula (Fig. 62-3). The trapezius, rhomboids, and upper portion of the latissimus dorsi muscles are divided in the line of the incision. If the use of the latisimus as an intrathoracic muscle flap is contemplated, it may be mobilized instead of being incised. The scapula is elevated. A 3-cm incision is made in the periosteum on the upper border of the of the sixth rib, and this periosteum is elevated, thus allowing a flange of a rib spreader to be inserted (Fig. 62-4). The rib spreader is opened and the upper
P.865
P.866
flange elevates and fixes the scapula, thus freeing the assistant for other duties. The attachments of the serratus anterior to the upper three ribs are visualized and transected 1 cm from their insertion on each rib using cautery. The insertions of the scalenus medius and posticus and serratus posterior superior are similarly divided from the upper two ribs (Fig. 62-5). Subperiosteal resection of the third, second, and first ribs is performed in that order, since the first rib is not well visualized until the two lower ribs are resected. Incising the periosteum with a scalpel rather than cautery allows for a cleaner and more rapid stripping of the ribs. The second and third ribs are resected from the transverse processes to the costochondral junction. The first rib requires special care in its management, and the surgeon must be familiar with the neurovascular relationships to the upper surface of the rib (Fig. 62-6). It is best approached by first freeing the lower surface of its periosteum and inserting a finger in that interval before using the
P.867
Haight or Matson elevators to elevate the periosteum on its upper surface (Fig. 62-7). The first rib is divided posteriorly 1 cm from the transverse process and retracted downward and outward with a bone-holding forceps (Fig. 62-8). The attachment of the scalenus anterior to the first rib is thus visualized, and it is carefully divided, avoiding injury to the subclavian vessels and the brachial plexus. The rib is similarly divided at the costochondral junction. After excision of the ribs, the sacrospinalus muscle is reflected medially and retracted with the Semb retractor. The transverse processes are exposed and, using the Coryllos periosteal elevator, the transverse processes and necks of the ribs are denuded and resected using the box-nosed rongeur, except for the transverse process of the first rib (Fig. 62-9). Hemostasis is obtained and the wound is closed in layers with absorbable sutures. If the pleura is opened, intercostal tube drainage is used until the pneumothorax has been evacuated. A bulky compression dressing is applied, taking care to avoid inhibiting respiratory excursions of the opposite hemithorax. The patient is encouraged to lie upon a bolster with the operative side down. Chest and arm physical therapy are used after each operative stage.
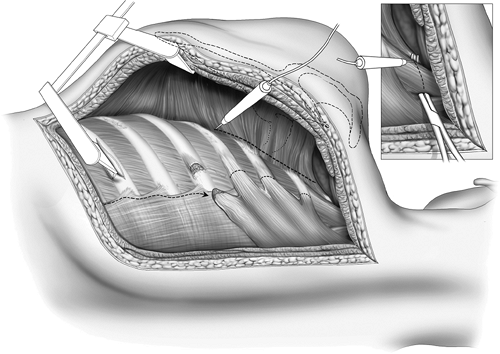 |
Fig. 62-4. A rib spreader elevates the scapular. Lower flange is maintained in position following an incision elevating the periosteum of a lower rib. The serratus muscles are removed from the ribs using cautery. |
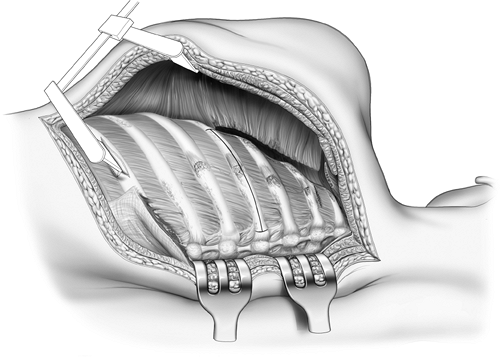 |
Fig. 62-5. The periosteum is incised and reflected and the ribs are removed from below upward. |
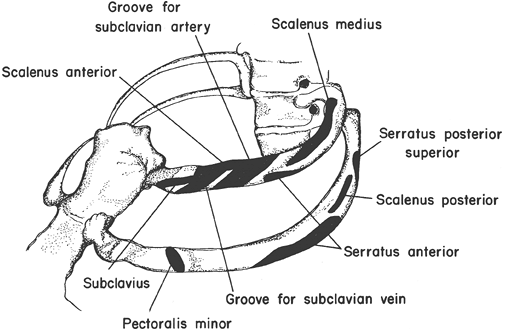 |
Fig. 62-6. Neurovascular and muscle relations to the first and second ribs. |
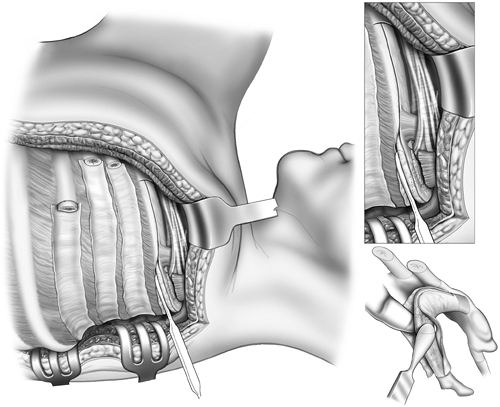 |
Fig. 62-7. Exposure of the first rib. |
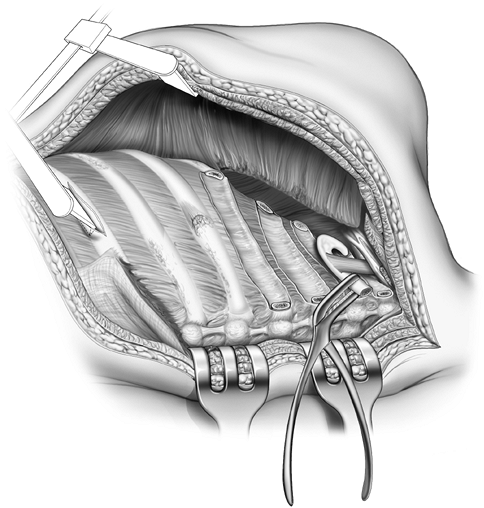 |
Fig. 62-8. The first rib has been divided posteriorly and grasped with sequestrum forceps. The scalenus is transected and the rib excised at its junction with the costal cartilage. |
In cases of apical cavities located posteriorly in the region of the paravertebral sulcus, it may be necessary to collapse them using the Semb apicolysis as described in 1935. After removing the first rib, the intercostal bundle between the first and second ribs is mobilized and divided, allowing access to the extrafascial plane. The apical parietal pleura is mobilized in this plane, taking care to avoid injury to subclavian vessels and the brachial plexus. This extrapleural tissue is depressed to a level no lower that the fourth vertebral body. Apicolysis is of particular value in the management of empyema reaching to this level, obviating the need for first rib resection.
Two to three weeks after the first-stage TPL, the second stage is performed. The lower half of the incision is opened and adhesions beneath the scapula are cleared by blunt dissection. The fourth rib is resected from the spine to the midaxillary line and shorter segments of the fifth and sixth ribs are resected leaving correspondingly longer anterior segments of these ribs, especially on the left side to allow for adequate coverage of the pericardium. If resection of the seventh rib is not required for the collapse of pulmonary cavities, the lower third of the scapular is resected subperiosteally in order that it not impinge on the seventh rib. Omitting this maneuver will result in painful shoulder girdle motion, often with a palpable click. Furthermore, the impingement of the scapular tip up on the seventh rib acts as a strut, increasing scoliosis (Fig. 62-10). The scapula is likely to splinter if resected with a rib shear. A Gigli saw or
P.868
an electric saw is preferable; the angle of resection should parallel the upper border of the seventh rib. As in the first stage, the paravertebral muscles are retracted and the rib necks and transverse processes are shortened.
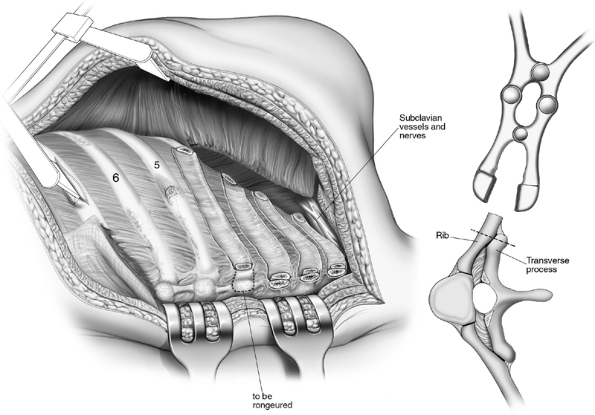 |
Fig. 62-9. Paravertebral muscles reflected and rib necks and transverse processes resected. |
TAILORING THORACOPLASTY
In cases of lobectomy for tuberculosis, a first-stage TPL had been executed preceding resection, or concomitant with it, when it was believed that incomplete expansion of remaining lung would occur, such as in instances when an upper lobectomy and superior segmentectomy were combined. These tailoring thoracoplasties fell into disrepute: The need for preresection TPL was not reliably predictable, thus adding a potentially useless procedure and making resection more difficult as well as incurring the risk for post-TPL spread of tuberculosis. Concomitant TPL had an adverse effect on postoperative ventilation, leading to retained secretions, atelectasis, and pneumonia ( drowned lung ). In cases of lobectomy in which an apical air space develops, complicated by fluid accumulation that does not diminish over a period of observation, and in which the development of empyema is a real possibility, the thorax is reentered, the pleural space d brided, and TPL performed, draining the pleural cavity with a chest tube. Alveolar pleural fistula will seal as the space obliterates. Space problems, if anticipated, may be prevented by pleural tenting or intraoperative or postoperative pneumoperitoneum. Persistent basilar spaces may also be managed by pneumoperitoneum. Basilar empyema requires open drainage, with or without interposition of muscle flaps, rather than TPL.
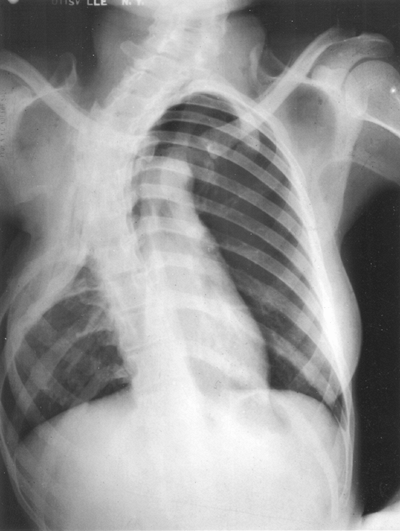 |
Fig. 62-10. Seven-rib thoracoplasty for extensive cavitary disease. Note the scoliosis. |
THORACOPLASTY FOR POSTPNEUMONECTOMY EMPYEMA AND BRONCHOPLEURAL FISTULA
When used for the management of postpneumonectomy empyema and BPF, TPL is performed in one stage resecting ribs 2 through 7 or 8 as required to obliterate the space. The
P.869
infected pleural space must have been adequately drained by open window thoracostomy, placed low on the chest wall, so as not to interfere with subsequent TPL. During the days or weeks in which the pleural space is being cleansed, appropriate antibiotics as well as nutritional support are employed, and attention is directed to associated medical illness. Bronchial fistula may close with this treatment. Occasionally, in the presence of a large fistula, extreme loss of tidal volume requires urgent TPL following evacuation of pleural fluid by tube drainage. Apicolysis obliterates the apical space, allowing for retention of the first rib, minimizing the functional and cosmetic deformities of the shoulder girdle. Thoracoplasty is accompanied by the application of local muscle, principally the intercostals, to buttress the bronchial fistula, reclosed if possible. The pleural cavity is drained until the pleural space is obliterated. The drain is backed out over a period of days. The subscapular space is also drained with a suction device. Resection of the necks of the ribs and the transverse processes may be required to ensure that there is not a gutter remaining that will harbor infection.
 |
Fig. 62-11. Schede thoracoplasty with massively deformed chest wall. |
THORACOPLASTY FOR CHRONIC EMPYEMA
When chronic empyema has existed for many months, the parietal wall becomes so thick and rigid that it cannot be brought into apposition with the visceral pleura or mediastinum by conventional extrapleural TPL. In the 1890s, the Schede TPL was used to obliterate a chronic empyema space over a destroyed lung. The operation was accompanied by massive blood loss and a mortality rate approaching 50%. Undesirable late sequelae included paradoxic chest wall motion, paresis of the abdominal wall, and a grotesque cosmetic defect (Fig. 62-11). The procedure consisted of creating a U-shaped flap of all the soft tissues of a chest wall overlying the empyema cavity and then resecting the ribs, intercostal muscles, and thick parietal pleura (Fig. 62-12). The previously elevated soft tissue flap was then allowed to fill the pleural space over packing. Horrigan and Snow (1990) modified the Schede TPL, closing the chest over drains, achieving early healing and acceptable cosmetic and functional results. Dissatisfaction with the
P.870
Schede procedure led to the development of other methods for intrapleural TPL to treat chronic empyema.
 |
Fig. 62-12. Technique of Schede thoracoplasty. A, B. Vertical incision in the midaxillary line and excision of the draining sinus. C. The incision is carried through the muscles to the chest wall and the muscles are reflected. The empyema cavity is entered and unroofed by excising the ribs and intervening intercostal muscles and neurovasculature structures. The cavity is completely saucerized. Intercostal vessels are controlled with suture ligatures. D. The cavity is packed with gauze and subsequently the chest wall muscles are allowed to approximate the visceral pleura. From Johnson K, Kirby C: Surgery of the Chest. Chicago: Year Book Medical, 1952. With permission. |
In 1946 Grow and independently in 1953 Kergin described an intrapleural TPL in which the thickened parietal pleura was resected and the intercostal muscles and neurovasculature were preserved and allowed to fall into the empyema space after resection of the ribs overlying the space. As described by Grow (1946), the operation includes resection of sufficient length and number to completely unroof the empyema cavity for a distance of 1 inch beyond all borders of the cavity. One rib above and one rib below the cavity are resected (Fig. 62-13). The intercostal bundles
P.871
are separated in the plane of the endothoracic fascia and retracted so that the entire thick parietal pleura overlying the empyema cavity is exposed and resected. The mediastinal pleura is d brided as required, and the intercostal bundles are allowed to fall into the cavity. An intercostal bundle is sutured over the site of a bronchial fistula if one is detected. The chest is drained and the wound closed with a large pressure dressing. The extrafascial space and the empyema space are drained if a fistula is present.
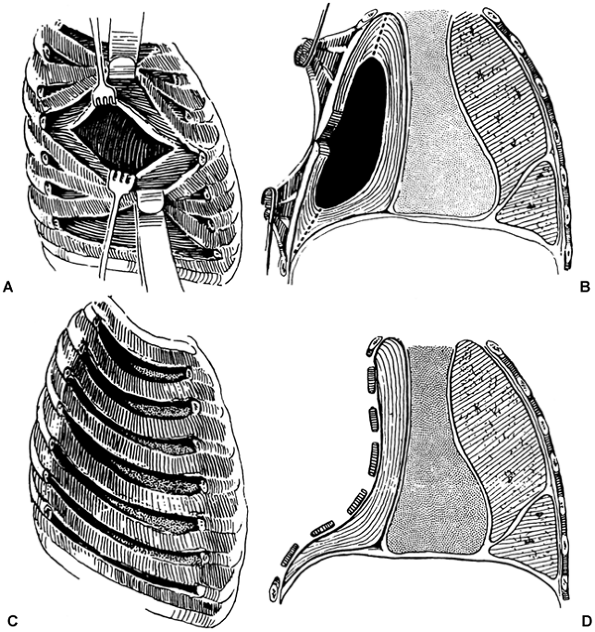 |
Fig. 62-13. Grow-Kergin thoracoplasty. A. The intercostal bundles are mobilized following the rib resections. B. The thick parietal peel is excised. C, D. The intercostal bundles are allowed to fall into the cavity. From Kergin FB: An operation for chronic pleural empyema. J Thorac Surg 26:430, 1953. With permission. |
Andrews (1961) reported a procedure he termed thoracomediastinal plication (subsequently referred to as the Andrews TPL) which proved successful in treating cases of empyema and BPF refractory to other methods of management. In essence, the procedure consists of rib resection, mobilizing the parietal pleural flap, curetting it to make it malleable, and suturing it to the mediastinal pleura. Paramount to the success of the operation is a well-drained and clean empyema space and sturdy granulation
P.872
of the mediastinal pleura, resulting from weeks to several months of open drainage and irrigation as stressed by Icard and associates (1999). Andrews (1961) achieved success in 33 of 35 cases. Dupon (1990) in a series of 73 patients, 62% of whom had bronchial fistula, reported complete healing in 84% with a 5.4% 30-day mortality rate. Icard and co-workers (1999) reported healing in 20 of 23 cases, the remainder successfully treated by revision of the TPL, with one death.
Method of Performing a Thoracomediastinal Plication
Following a posterolateral incision excising the previous pleurocutaneous fistula, subperiosteal resection of the ribs overlying the cavity allows for mobilization of the extraperiosteal flap (Fig. 62-14). This thick fibrous wall is made malleable by thinning the flap by sharp dissection, leaving a thin fibrous layer and maintaining integrity of the flap by not producing defects in the periosteum or intercostal muscle.
P.873
The mediastinal wall of the empyema space is curetted, leaving a clean fibrous layer. Bronchial fistulae are closed, if possible. Absorbable heavy mattress sutures are then applied between the parietal flap and the visceral or mediastinal wall, oriented so that they do not impinge on the intercostal vessels and nerves. The sutures are initially placed peripherally, and none are tied until all are in place. If the empyema space extends to the apex of the chest, limited apicolysis is performed and mattress sutures are placed between the serratus anterior and the depressed intercostal flap to obliterate the subscapular space and prevent infection in this area. The initial pleural incision is securely closed. A suction drain is placed superficial to the pleural flap prior to wound closure. If the seventh rib is not resected, the tip of the scapula is resected as previously described. Because resection of the transverse process and first rib are usually not required, postoperative scoliosis is minimal. The results of the use of an Andrews thoracoplasty are shown in Fig. 62-15.
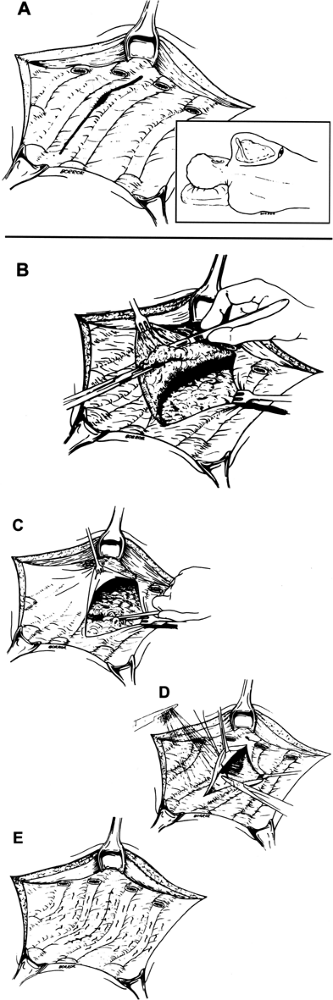 |
Fig. 62-14. Andrews thoracoplasty. A. Ribs overlying the empyema space are resected and the thick fibrous track excised. B. The parietal flap is thinned by sharp dissection. Andrews thoracoplasty. C. The mediastinal pleura is curetted. D, E. The mattress sutures approximate the parietal flap to the mediastinal pleura. From Andrews NC: Thoracomediastinal plication. J Thorac Surg 6:809, 1961. With permission. |
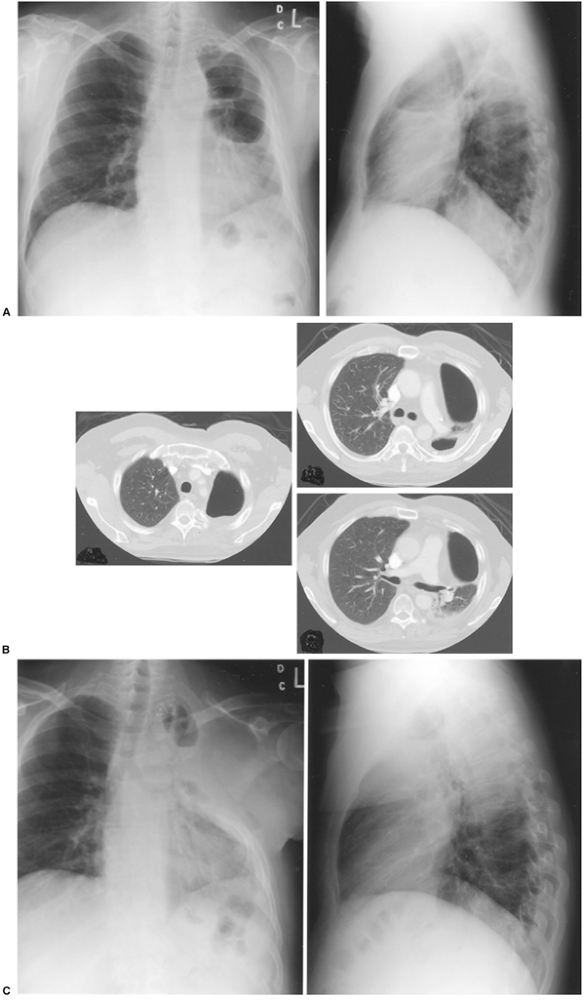 |
Fig. 62-15. A. A 49-year-old man, 2 years after left upper lobectomy associated with chemotherapy and radiotherapy and bronchopleural fistula. B. Note thick parietal pleura on computed tomographic scan. C. Status post Andrews thoracoplasty. Air in the soft tissues subsequently absorbed. Case of JB Putnam, M.D. |
P.874
P.875
PLOMBAGE THORACOPLASTY
The term plombe is derived from the French verb plomber, meaning to seal or to stop. Plombage was used in patients considered too ill for conventional TPL and had the following advantages: it could be performed in one stage, the mediastinum remained stable, and paradoxic ventilation did not occur; there was also less long-term effect on lung function, and the procedure could be performed bilaterally (in stages). The procedure is directly descended from extrapleural and extrafascial pneumonolysis, as practiced by Tuffier (1891) procedures that were ineffective in pulmonary tuberculosis. Formerly, a variety of materials were inserted into the extrafascial space, including oil, fat, blood, and paraffin, often with dismal late sequelae. In an effort to find a more biocompatible material, Woods and co-workers (1950) used methyl methacrylate spheres, similar to ping pong balls as the plombe, inserted in a plastic bag to prevent migration and to facilitate later removal (Fig. 62-16). Subsequently, he used only sheets of polyethylene as the plombe.
Method of Plombage Thoracoplasty
The operation consists of denuding the ribs overlying the cavity of their periosteum, depressing the soft tissues and then inserting the plombe in the bird cage of the denuded ribs (Fig. 62-17). Periosteum is only stripped from the lowest surface of the first rib and the ribs overlying the cavity to the rib necks. Minimal apicolysis is performed. The intercostal muscle bundles are cut anteriorly or posteriorly as required, to prevent their acting as a sling.
In 4 to 6 months the collapsed extraperiosteal tissues form a stable bony plate, thus preventing paradoxic ventilation. At that time the plombe and the ribs, now atrophied, are removed, leaving the first rib and transverse process.
Subsequently, Wilson and co-workers (1956) performed a series of one-stage plombage TPL in which the prosthesis was not removed. Despite Wilson's misgivings about leaving the plombe in situ, the one-stage procedure was embraced by other surgical groups and was more frequently performed than the original procedure. Thus, complications related to the implant were recorded years later. These include infection, migration of the plombe, mediastinal compression, erosion into the esophagus or bronchus, and development of cancer as recorded by Thompson and Entin (1969), Ashour (1985), Tsuda (1991), Horowitz (1992), and Massard (1997) and their colleagues. None of these complications has been reported in the two-stage procedure.
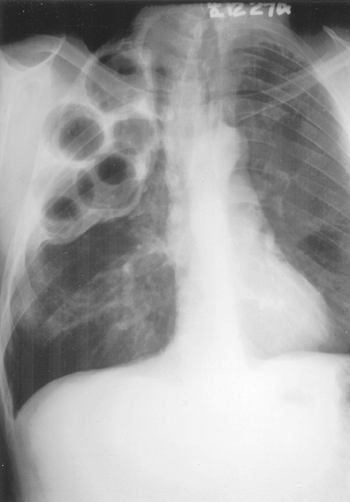 |
Fig. 62-16. Radiograph of an extraperiosteal plombage. |
P.876
The initial poor results with the use of paraffin as the plombage material were subsequently overcome by a change in the technique of the development of the space in which the paraffin was inserted. Creation of a suitable extraperiosteal space as described by Fox and Shields (1972) prevented apposition of the paraffin to the pleural surface. With this maneuver, serious early complications were avoided. However, late migration of the plombe occurred in approximately 25% of cases and removal was required and was accomplished with minimal complications. Tuberculous infection of the space was not encountered, and nontuberculous pyogenic infection with or without a BPF was seen in only 0.5% of 785 wax pack plombage thoracoplasties, as reported by Fox and associates (1962).
Interest in plombage abated with the introduction of drug therapy for tuberculosis in 1945, but the appearance of drug-resistant organisms and acquired immunodeficiency syndrome (AIDS) have rekindled interest in this procedure and its application, as discussed by Jouveshomme and associates (1998). As many as two-thirds of patients with multidrug-resistant tuberculosis are not candidates for resection because of extent of disease or poor pulmonary function, as noted by Iseman and colleagues (1990). The development of more physiologically inert plombes, notably tissue expanders and breast prostheses, by Mayer (1973) and Talamonte (1989) and their associates has given impetus to plombage therapy for pulmonary tuberculosis, since these devices have been successfully used for treating the postpneumonectomy syndrome by Wasserman (1979), Riveron (1990), Grillo (1992), and Kelly (2001) and their associates.
Iioka (1985) and Tatsumura (1990) and their associates have described plombage-type operations for the management
P.877
of cases of failed decortication or where decortication of underlying lung was not possible, with the plombe being serum that accumulates in the extraperiosteal space reported by the former, or extrapleural space, published by the latter, respectively. In neither procedures are the ribs resected. Iioka leaves the periosteum on the outer surface of the ribs and thins the parietal flap as in the Andrews' operation, decorticating the visceral peel and relying on suction drainage of the now cleansed pleura to guarantee apposition of the two surfaces. Watertight closure of the parietal flap is essential. Tatsumura and co-workers (1990) merely gently d bride the visceral pleural wall and mobilize only parietal pleura, not including intercostal muscles and periosteum, and drain both the pleural and extrapleural spaces. Although neither group reported extrapleural infection, this is a matter of concern.
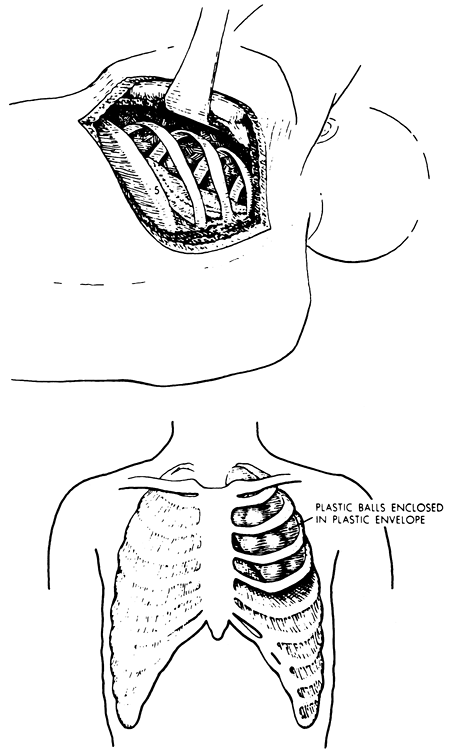 |
Fig. 62-17. Extraperiosteal plombage. A. The ribs are denuded, and the periosteum, intercostal bundles, and pleura are depressed over the cavity. B. The plombe is inserted into the extraperiosteal space. |
PULMONARY FUNCTION AFTER THORACOPLASTY
Gaensler and Streider (1951) noted a 27% reduction of vital capacity and a 21% loss of maximum voluntary ventilation following TPL over a nonfunctional lung. Bredin (1989) assessed long-term (approximately 30 years) survivors of TPL and observed a mixed obstructive and restrictive defect with no correlation between the number of ribs removed and pulmonary function. This is thought to be related to the minor degrees of scoliosis noted after TPL followed by physical therapy. The obstructive defect is believed to be due to chronic bronchitis associated with prior cigarette smoking. Westermann (1989) reported a vital capacity of 49% 30 years following the thoracoplasty, comparable with that of pneumonectomy. In comparing TPL with TPL and ipsilateral
P.878
pneumonectomy, the residual lung after TPL hardly contributed to pulmonary function. Furthermore, in the TPL plus pneumonectomy group, extensive TPL did not impair the ventilation-perfusion relationship in the remaining lung.
MORBIDITY AND MORTALITY AFTER STANDARD THORACOPLASTY
Postoperative complications relate directly to the underlying disease, associated medical illness, and possible technical misadventure such as injury to subclavian vessels and brachial plexus. Pulmonary complications of atelectasis and pneumonia can be minimized by vigorous chest physical therapy. Wound infection is not common, and subscapular wound infection may be avoided by meticulous hemostasis and wound drainage when indicated.
Multiple ribs and transverse process resection allow the contralateral intercostal muscles to function unapposed, inevitably leading to scoliosis and convexity to the operated side. First rib resection leads to elevation of the shoulder girdle. These deformities are more marked in patients under 40 years of age, and less marked in those over 60, in whom the spine is less mobile. If the first rib and transverse processes do not require resection, the degree of scoliosis is cosmetically acceptable and it, as well as shoulder girdle dysfunction, is ameliorated by physical therapy. Parenthetically, the cosmetic and functional sequelae of serratus interposition (scapular winging) and latissimus transfer (upper extremity dysfunction) have received scant scrutiny.
Mortality is similarly related to underlying disease rather than to the operative procedure. Perioperative deaths are more common in lung cancer cases and when bronchopleural fistula exists. Nevertheless, Icard and colleagues (1999) achieved a mortality rate of 4.3% with the Andrews TPL and healing in 20 of 23 cases. The remaining cases healed after a second procedure.
Upon reflection, it is apparent that thoracoplasty, a hoary antiquity that served to elevate thoracic surgery to the status of a recognized speciality, remains an occasionally useful operation. To paraphrase Alexander: in the last analysis, thoracoplasty is used to close a pleural space that no other operation can close.
REFERENCES
Alexander J: The Surgery of Pulmonary Tuberculosis. Philadelphia: Lea & Febiger, 1925.
Alexander J: The Collapse Therapy of Pulmonary Tuberculosis. Springfield, IL: Charles C Thomas, 1937.
Andrews NC: Thoracomediastinal plication. J Thorac Surg 41:809, 1961.
Ashour M, et al: Late complication of plombage thoracoplasty. Thorax 40: 394, 1985.
Bredin CP: Pulmonary function in long-term survivors of thoracoplasty. Chest 95:18, 1989.
Dupon H: Andrews technique of thoracomyopleuroplasty. In Deslauriers J (ed): Thoracic Surgery Management of Pleural Diseases. Philadelphia: CV Mosby, 1990, pp. 255 260.
Fox RT, Shields TW: Thoracoplasty. In Shields TW (ed): General Thoracic Surgery. 1st Ed. Philadelphia: Lea & Febiger, 1972, p. 351.
Fox RT, et al: Extraperiosteal plombage thoracoplasty. J Thorac Cardiovasc Surg 44:371, 1962.
Gaensler EA, Streider JW: Progressive changes in pulmonary function after pneumonectomy: the influence of thoracoplasty, pneumothorax, oleothorax, plastic sponge plombage in the side of the pneumonectomy. J Thorac Surg 22:1, 1951.
Grillo H, et al: Postpneumonectomy syndrome. Ann Thorac Surg 54:638, 1992.
Grow SB: Chronic pleural empyema. Dis Chest 12:26, 1946.
Hochberg LA: Thoracic Surgery Before the 20th Century. New York: Vantage Press, 1960.
Horowitz MD, et al: Late complications of plombage. Ann Thorac Surg 53:803, 1992.
Horrigan TP, Snow NJ: Thoracoplasty: current application to the infected pleural space. Ann Thorac Surg 50:695, 1990.
Icard P, et al. Andrews thoracoplasty, as a treatment of post-pneumonectomy empyema: experience in 23 cases. Ann Thorac Surg 68:12159, 1999.
Iioka S, et al: Surgical treatment of chronic empyema. A new one-stage operation. J Thorac Cardiovasc Surg 90:179, 1985.
Iseman M, et al: Surgical intervention in the treatment of pulmonary disease caused by drug-resistant Mycobacterium tuberculosis. Am Rev Respir Dis 141:623, 1990.
Johnson K, Kirby C: Surgery of the Chest. Chicago: Year Book Medical, 1952.
Jouveshomme S, et al: Preliminary results of collapse therapy with plombage for pulmonary disease caused by multidrug-resistant mycobacteria. Am J Resp Crit Care Med 157:1609, 1998.
Kelly RF, Hunter DW, Maddaus MA: Postpneumonectomy syndrome after left pneumonectomy. Ann Thorac Surg 71:701, 2001.
Kergin FC: An operation for chronic pleural empyema. J Thorac Surg 26: 430, 1953.
Langston HT: Thoracoplasty: the how and the why. Ann Thorac Surg 52: 1351, 1991.
Massard G, et al: Long-term complications of extraperiosteal plombage. Ann Thorac Surg 64:220, 1997.
Mayer JH III, Moore JD, Gago O: Silicone elastomer plombage for severe hemoptysis. Arch Surg 107:101, 1973.
Meade RH: A History of Thoracic Surgery. Springfield, IL: Charles C Thomas, 1961.
Pairolero PC, et al: Intrathoracic transposition of extrathoracic skeletal muscle. J Thorac Cardiovasc Surg 86:809, 1983.
Riveron FA, et al: Silastic prosthesis plombage for right postpneumonectomy syndrome. Ann Thorac Surg 50:465, 1990.
Schede M: Die Behandlung der Empyema. Verch Cong Innere Med Wiesb 9:41, 1890.
Semb C: Thoracoplasty with extrafascial apicolysis. Acta Chir Scand 76:1, 1935.
Talamonte MS, et al: A new method of extraperiosteal plombage for atypical pulmonary tuberculosis. Chest 96(suppl):2375, 1989.
Tatsumura T, et al: A new technique of one-stage eradication of long-standing chronic thoracic empyema. J Thorac Cardiovasc Surg 99:410, 1990.
Thompson JR, Entin SD: Primary extraskeletal chondrosarcoma. Report of a case arising in conjunction with extrapleural lucite ball plombage. Cancer 23:936, 1969.
Tsuda T, et al: Non-Hodgkin's lymphoma of the chest wall developing 37 years after plombage and thoracoplasty. Jpn J Med 30:438, 1991.
Wasserman K, et al: Post-pneumonectomy syndrome. Surgical correction using Silastic implants. Chest 75:78, 1979.
Westermann CJJ: Pulmonary function in long-term survivors of thoracoplasty. Chest 97:512, 1990.
Wilson NJ, et al: Extraperiosteal plombage thoracoplasty: operative technique and results. J Thorac Surg 32:797, 1956.
Woods FM, et al: Extraperiosteal temporary plombage in thoracoplasty. Dis Chest 18:401, 1950.
Reading References
Gregoire R, et al: Thoracoplasty: its forgotten role in the management of nontuberculous postpneumonectomy empyema. Can J Surg 30:343, 1987.
Peppas J, et al: Thoracoplasty in the context of current surgical practice. Ann Thorac Surg 56:903, 1993.
EAN: 2147483647
Pages: 203