5 - Physiologic Insulin Replacement Therapy
Authors: Unger, Jeff
Title: Diabetes Management in the Primary Care Setting, 1st Edition
Copyright 2007 Lippincott Williams & Wilkins
> Table of Contents > 5 - Physiologic Insulin Replacement Therapy
function show_scrollbar() {}
5
Physiologic Insulin Replacement Therapy
Take Home Points
Understanding the pharmacokinetics and glucodynamic profiles of different insulin preparations is necessary to direct patients toward the treatment protocols that will allow them to maintain a safe and practical level of hemoglobin A1C (A1C)
Patients with type 2 diabetes mellitus (T2DM) may be able to attain an A1C of 7% or less using treat-to-target protocols with either basal insulin or mixed insulin analogue added to oral agents
Most patients with type 1 diabetes mellitus (T1DM) should optimize their management using basal-bolus insulin
Doses of bolus and basal insulin may be easily determined by calculating the patient's total daily insulin dose, the insulin-to-carbohydrate ratio, and the insulin sensitivity (correction) factor
Inhaled insulin (INH) may be an appropriate therapy for patients with insulin-requiring diabetes
Patients contemplating pregnancy should have their glycemic control optimized for 6 months before conception using a physiologic basal-bolus insulin regimen
Patients with severe insulin resistance may be successfully treated with highly concentrated U-500 insulin
Insulin is the most powerful and versatile pharmacologic agent available to control hyperglycemia
If you think a patient requires insulin, you are probably correct
Convincing patients to transition to insulin therapy requires physicians to treat both their insulin resistance and their resistance to insulin.
Case 1: Is Intensification of Diabetes Management Really Necessary?
Kevin is referred by another physician for management of his diabetes. The referring physician believes that Kevin has been noncompliant with his diabetes regimen and is growing frustrated trying to manage his case. Kevin is 26 years
P.193
old and works as an electrical engineer. After being diagnosed with type 1 diabetes mellitus (T1DM) 2 years ago, Kevin has been using two daily injections of insulin consisting of neutral protamine Hagedorn (NPH) 20 U with a sliding scale dose of regular insulin for both breakfast and dinner. Kevin is checking his blood glucose levels twice daily. Occasionally he guesses at how much regular insulin to use rather than confirms his preprandial glucose with an actual test. Over the past 5 months, Kevin, who lives alone, has had three episodes of severe hypoglycemia, including one at work that required transportation to the emergency department. Twice a month Kevin boards an airplane for cross-country trips to the company headquarters in New Jersey. Last month he was hospitalized overnight after arriving on the East Coast with a blood glucose level of 615 mg per dL (seems as though Kevin forgot to bring his regular insulin along with him on the trip and tried to get by using only NPH).
Kevin's father died of renal failure secondary to T1DM diabetes at age 52. His sister, age 22, was recently diagnosed as having gestational diabetes. Although he has no diabetes-related complications at this time, Kevin admits to feeling miserable most of the time, especially after eating. In fact, he has lost 10 lb in the past 2 months, experiences up to four episodes of nocturia, and feels constantly fatigued.
Why even check my blood sugars? Nothing I do seems to have any influence on them anyway. I mean, there's no rhyme or reason to any of the numbers. Last night I went to bed with a blood sugar of 110 and today I wake up with a 325! Its almost like I snuck off sleep walking in the middle of the night just to eat some Twinkies! Talk about frustrating and worst of all are those trips to the emergency room (ER) for severe hypoglycemia. Used to be that I could feel 'em coming on. Now, they just hit, sometimes when I'm driving. I don't think that's safe. I don't even know what to eat anymore. Sometimes I skip meals and the sugar still goes high. What the heck is going on here? I feel like I'm on a bungee cord, only I don't really want to jump off the bridge. I just want to get my life back in order!
On physical exam, Kevin is 6 feet tall and weighs 160 pounds. His blood pressure (BP) is 106/74 mm Hg and his pulse is 74 beats per minute and regular. His nondilated eye and neurologic exams are normal, although he does appear to be slightly dehydrated. With the exception of a low high-density lipoprotein cholesterol (HDL-C) and slightly elevated triglyceride level, Kevin's lab work is essentially unremarkable. He has no evidence of proteinuria. His random blood glucose level is 395 mg per dL and his urinalysis demonstrates 1 + ketones. The point-of-service hemoglobin A1C (A1C) is 12.2%.
Based on the patient's intake history and physical examination and the available laboratory data, the primary care physician (PCP) should address the following therapeutic concerns:
Why should Kevin's diabetes be intensively treated at this time?
Assuming Kevin's glycemic control improves, what is the likelihood of being able to reduce his long-term risk of eye, kidney, and heart disease?
What is Kevin's ultimate A1C target? Once the A1C target is achieved, how long should control be maintained to induce his protective metabolic memory?
How can Kevin's diabetes be treated to target rather than toward failure?
What insulin regimen will allow Kevin to achieve physiologic control of his diabetes that most resembles the glucodynamic profile of a normally functioning pancreas?
What is this patient's estimated total daily dose (TDD) of insulin, his calculated insulin sensitivity (correction) factor, and insulin-to-carbohydrate ratio?
How is the preprandial dose of insulin determined?
How could one calculate Kevin's insulin action onset personal lag time ?
How can Kevin learn to avoid hypoglycemia by understanding the concept of insulin stacking ?
Is inhaled insulin appropriate for Kevin?
How can Kevin's adherence to the intensified insulin regimen be enhanced?
P.194
Introduction
History of Insulin
The discovery of insulin in 1922 by Frederick Banting and Charles Best remains one of the most dramatic achievements in the history of medicine. Before the availability of insulin, a child newly diagnosed with T1DM survived on average 1 year.1 Patients were treated with caloric-restricted diets averaging 500 to 700 calories per day. So strict were these dietary restrictions that patients were forced to count out the exact number of berries that they could eat per day and would be labeled as noncompliant if they added any extra food to their daily dietary intake. Surviving patients with diabetes would lose an extraordinary amount of weight yet would remain under the threshold for developing diabetic ketoacidosis (DKA) as long as they could maintain their starvation diets.
Leonard Thompson, 14 years old, was the first patient ever to receive an injection of insulin. Weighing only 65 lb on admission to Toronto General Hospital 2 years after being diagnosed with diabetes, Leonard appeared pale, with a distended abdomen and breath that smelled of acetone. All of us knew that he was doomed, wrote a senior medical student in attendance.2 The boy had survived on a caloric intake of only 450 calories daily, just enough to keep him from becoming ketotic. Anxious to try out his unpurified pancreatic extract on human subjects rather than dogs, Dr. Banting, a general surgeon by trade, injected Leonard with 15 mL of a thick brown muck on January 11, 1922. (The dose chosen was 50% of the dose thought to be appropriate for a dog of equal weight.) Leonard's blood glucose dropped from 440 mg per dL to 320 mg per dL and he continued to have ketonuria. Unfortunately, Leonard developed multiple sterile abscesses from the injections. Banting thought
P.195
that his experiment was a failure, despite the 25% improvement in glycemic response to the extract.
A biochemist, James Collip (who shared the Nobel Prize for Medicine with Banting and Best in 1923), was able to purify the extract in his own laboratory. On January 23, 1922, Leonard Thompson received 5 mL of the purified drug followed by a second dose of 20 mL 6 hours later. The next day he received two 10-mL injections. His initial blood glucose level of 520 mg per dL fell to 120 mg per dL within 24 hours and his ketonuria disappeared. The patient's condition continued to improve with the insulin extract.
Compliance was one of Leonard's weaker points. During a celebration marking the 10th anniversary of the discovery of insulin, the world's poster boy for diabetes became comatose after consuming an excessive amount of alcohol and party pastries. Fortune again prevailed, allowing Leonard to survive another hospitalization until finally succumbing to pneumonia at age 27.
The first commercial insulin preparations contained numerous impurities and varied in potency by up to 25% per lot. In the 1930s the first long-acting preparation, protamine zinc insulin (PZI), was marketed, which reduced the number of injections required for adequate insulin replacement.3 PZI was used once daily without adding any short-acting insulin, setting a trend that lasted until the 1950s when NPH and zinc insulin (Lente) were marketed. For the next 25 years, diabetes was treated using two injections of NPH and regular insulin featuring the famous 2/3:1/3 ratio, in which higher doses of the insulins were given with breakfast. In the 1980s, the introduction of human insulin eliminated commonly observed insulin allergies and the cosmetically disfiguring immune-mediated lipoatrophy requiring patients to rotate the site of their injections to prevent areas of skin atrophy.4 In the 1990s, the relationship between improving glycemic control and reducing diabetes-related complications was confirmed.5,6
The absorption patterns and pharmacologic actions of the standard insulins did not match the physiologic nature of endogenous insulin. Patients experienced wide daily glycemic changes, including hypoglycemia, while maintaining acceptable A1C levels. In an attempt to mimic normal pancreatic endogenous insulin action, insulin analogues were developed. The first insulin analogue, lispro, was introduced in 1996 followed shortly thereafter by insulin aspart. The newest fast-acting analogue, insulin glulisine, became available in 2005. Table 5-1 lists the currently marketed insulin analogue preparations. Insulin analogues are more physiologic than NPH and regular insulin, thereby allowing patients to experience more flexibility and safety with their treatment regimens.
Pathogenesis of Type 1 Diabetes
The term diabetes represents a syndrome of disorders all characterized by an impairment of pancreatic beta cells' ability to secrete insulin. The American Diabetes Association (ADA) and the World Health Organization
P.196
(WHO) recognize two forms of diabetes. T1DM results from pancreatic beta-cell destruction secondary to an autoimmune process or an uncertain (idiopathic) etiology. These patients are prone to ketoacidosis. Diseases that secondarily result in pancreatic cell destruction (cystic fibrosis) are not classified as T1DM. Patients with type 2 diabetes mellitus (T2DM) have deficient insulin secretion from the pancreatic beta cell in association with peripheral insulin resistance. There is no evidence of autoimmunity in patients with T2DM whose pathophysiology appears to be genetically and environmentally predetermined.
TABLE 5-1 Currently Marketed Insulin Analogue Preparations | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Epidemiologic studies have suggested two distinct peak occurrences of T1DM: during puberty and near age 40.7 Ten percent to 30% of patients with T2DM also develop autoantibodies similar to patients with T1DM. These patients are referred to as having latent autoimmune diabetes in adults (LADA).
Initially, patients with T1DM have a protracted preclinical phase during which time autoantibodies can be detected against their pancreatic beta cells in genetically susceptible individuals.8 At least 80% to 90% of the beta-cell mass must be lost before the patient develops hyperglycemia. Both a reduction in beta-cell mass and the direct inhibition of insulin secretion by cytokines appear to result in a hyperglycemic state.9
Patients who are likely to progress to T1DM develop insulin autoantibodies (IAAs), glutamic acid decarboxylase antibodies (GADAbs), islet cell antibodies (ICAs), and insulinoma associated protein-2 autoantibodies (IA-2Abs). Interestingly, some patients who do not develop diabetes also produce these autoimmune markers. However, unlike patients with T1DM, their autoantibody levels tend to wax and wane over time. Patients who are more
P.197
at risk for developing T1DM often have two or more autoantibodies present at any given time.10 The presence of IAAs appears to place patients most at risk for developing childhood T1DM.11
LADA is a slowly progressive form of autoimmune diabetes characterized by adult age at diagnosis, the presence of diabetes-associated autoantibodies, and the lack of insulin requirement at the time of diagnosis. The fact that insulin is not required for treatment at the time of diagnosis is intended to distinguish LADA from adult-onset T1DM and T2DM.
Some have referred to this disorder as being type 1.5 diabetes mellitus.12 Patients with LADA tend to have a more aggressive disease than T2DM, characterized by a shorter time to failure of oral hypoglycemic agents and progressive beta-cell failure leading to insulin deficiency. Eighty percent to 90% of patients with LADA will require insulin within the first few years after diagnosis.13 Therefore, physicians should differentiate LADA from T2DM whenever possible. LADA has also been diagnosed with increasing frequency in children who appeared to have T2DM.14
Several clinical phenotypes are useful in differentiating LADA from T2DM. When compared with T2DM patients, individuals with LADA at the time of their initial diagnosis of diabetes appear to have many of the following clinical and laboratory characteristics15:
Lower body mass index (BMI)
More common symptom presentation such as polyuria and polydipsia
Lower mean waist and hip circumference
Lower waist-to-hip ratio
Shorter duration of diet or oral antidiabetic treatment before requiring insulin therapy
Higher A1C levels
Our ability to classify patients as having either T1DM, LADA, or T2DM is dependent on the evaluation of autoimmune markers in patients who clinically present as having T2DM. Immunologic differences exist between T1DM and LADA. LADA patients are often positive for only a single autoantibody, whereas T1DM patients frequently have two or more autoantibodies detectable at diagnosis.12 LADA patients are more likely to test positive for GAD or ICAs but not IAA and IA-2Ab.12
Because patients with LADA more rapidly lose their ability to produce endogenous insulin within the first few years after their diagnosis, they soon require exogenous insulin for treatment of their diabetes. Therefore, once a patient is suspected of having LADA, insulin should be initiated to maintain better glycemic control early during the course of the disease, to limit glycemic variability, and to prevent diabetes complications during a variable transition period of beta-cell functional decline. What remains uncertain is whether early insulin treatment in patients with LADA will result in beta rest and beta-cell preservation.
P.198
Case 2: Should This Patient Be Transitioned to Insulin or Maintained on Oral Agents?
Alex is a 44-year-old Hispanic man who was referred to you by a colleague concerned because of the inability to control Alex's blood glucose levels. Two years ago, he was diagnosed with T2DM after experiencing acute onset of weight loss, polyuria, polydipsia, and blurry vision. Both parents had T2DM. His father died of an acute myocardial infarction (MI) at age 58 and his mother suffered from chronic kidney disease before dying of a stroke at age 67. When first evaluated by his family physician, Alex had an A1C of 11%. After being placed on glipizide XL 20 mg at bedtime, the patient's symptoms resolved and his A1C dropped to 8.2% within 4 months. Metformin was added to the treatment regimen after the A1C began to rise once again 6 months after the initial diagnosis. At the time of his consultation with you, Alex's clinical and laboratory findings included the following:
BMI: 27 kg per m2
BP: 144/88 mm Hg
Waist circumference: 38 inches
Random blood glucose: 243 mg per dL
Point-of-service A1C: 12.1%
In the belief that the patient had LADA, autoantibody studies were ordered, including GAD, ICA, and IAA. The patient tested positive only for the presence of GADAb. Therefore, the patient was advised to discontinue his oral agents and begin a mixed analogue using BIAsp 70/30 10 U before breakfast and 10 U before dinner. The patient was placed on a treat-to-target protocol allowing him to adjust his AM and dinner doses of insulin based on average glucose levels taken over a 3-day period. The fasting glucose target was lower than 110 mg per dL, whereas the predinner target was 140 mg per dL. Within 4 weeks the patient was taking 18 U of BIAsp 70/30 15 minutes before breakfast and 24 U 15 minutes before dinner. A review of his home blood glucose meter downloads demonstrated a mean fasting blood glucose of 108 mg per dL and a mean predinner level of 124 mg per dL. Eighty-four percent of his total glucose levels were within the range of 70 to 170 mg per dL. Four months later his point-of-service A1C was 6.8%. Alex had gained 4 pounds over 4 months but felt so good that he hired a personal trainer and began to incorporate light resistance training into his daily cardiovascular workouts (his stress echocardiogram was normal). Although the mixed insulin analogue appears to be providing both basal and prandial insulin coverage, Alex was informed that further intensification of his insulin regimen would most likely be required in the future. The importance of maintaining an A1C of less than 7% for as long as possible early after being diagnosed with diabetes was stressed to this patient. Close watch over the patient's self-monitoring glucose levels as well as his A1C measurements would dictate the necessity of further intensification.
P.199
Setting the Sights on the Patient's Glycemic Target
Diabetes either induces or is a contributor to considerable morbidity in the form of metabolic complications, vision disorders, peripheral and autonomic neuropathy, kidney disease, peripheral vascular disease, wound infections, amputations, heart disease, stroke, digestive disorders, oral disease, and depression. Nearly all aspects of a patient's life are affected by the ability to limit exposure to hyperglycemia both in the fasting and postabsorptive state. Diabetes reduces life expectancy by 5 to 10 years.16 Many of the complications of diabetes occur when patients are in the prime seasons of their lives, when their earning potentials are highest and during a period when life is to be enjoyed. Yet the effects of microvascular and macrovascular disease can become stressful and disabling both from a personal and financial perspective.
Although diabetes is not curable, two large controlled studies (Table 5-2), the Diabetes Control and Complications Trial (DCCT)5 and the U.K. Prospective Diabetes Study (UKPDS),6 have demonstrated the relationship between intensive glycemic control and reduction in morbidity (Fig. 5-1). The Kumamoto study17 has also shown the importance of reducing the A1C levels using insulin in patients with T2DM. Achieving an A1C less than 7% can markedly reduce the risk of long-term complications and is now the standard of care in clinical practice.18 The UKPDS, the largest and longest trial ever conducted for patients with T2DM, reported that each 1% reduction in A1C was accompanied by a 21% decrease in any endpoint related to diabetes and in diabetes-related mortality, a 14% decrease in MI, a 43% decrease in amputation or death from peripheral vascular disease, and a 37% decrease risk for microvascular complications.
The DCCT reported that lowering the A1C to less than 7.2% reduced the risk of retinopathy, neuropathy, and nephropathy by 60%. Intensively managed patients lived on average 5 years longer and experienced more than 15 years of complication-free living when compared with patients treated with one or two daily insulin injections.
P.200
TABLE 5-2 Summary of Risk Reduction Associated with Improved Glycemic Control in Major Controlled Diabetes Trials | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||
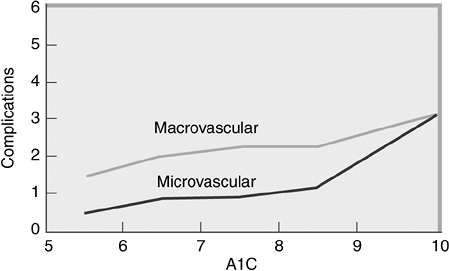 |
Figure 5-1 Reduction in A1C Can Lower Diabetes-related Complications. The U.K. Prospective Diabetes Study (UKPDS) demonstrated that intensively managing patients with type 2 diabetes (T2DM) and lowering A1C levels can significantly reduce the risk of microvascular and macrovascular complications. Note that there is no A1C threshold. The lower the A1C the lower the risk of diabetes-related complications. (From Stratton IM, Adler AI, Neil HAW, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes: prospective observational study. BMJ. 2000;321:405 412, with permission.) |
The benefits of intensive diabetes management appear to have long-term benefits. The Epidemiology of Diabetes Intervention and Complications Study (EDIC) evaluated patients who had been enrolled in the completed DCCT.19,20,21,22 During this 4-year observational study, all participants were intensively managed by community-based physicians. Armed with the evidence-based knowledge regarding the benefits of diabetes management intensification, the original conventionally treated patients reduced their mean A1C from 9.1% to 8.1%. However, the mean A1C level rose from 7.2% to 7.9% in the originally treated intensively managed cohort, primarily because the level of personalized care available within the community setting was substantially less than patients received during the DCCT. Despite their gradual rise in A1C levels, the originally managed intensive therapy patients in the DCCT had a 57% reduction in first occurrence of stroke, MI, or death from cardiovascular disease when compared with the conventionally treated patients during EDIC.23
Progression of retinopathy from the DCCT closeout examination to the eighth year of the EDIC follow-up was reduced by 63% in the group that graduated from the intensively managed cohort of the DCCT, when compared with the conventionally treated patients.23 This reduction in retinopathy progression occurred although glycemic control during EDIC was similar in both groups. Furthermore, the development of albuminuria (<300 mg per 24 hours) from the conclusion of the DCCT to EDIC years 7 and 8 was reduced 83% in the group receiving prior intensive treatment. In fact, almost no progression to this clinically ominous stage of nephropathy was noted in the intensively treated patients who maintained a mean A1C of 7% for 6 years during the DCCT.24
P.201
More than 90% of the treatment group differences in retinopathy and nephropathy outcomes after 4 years of the EDIC study could be explained by the mean DCCT A1C levels.24 Therefore, intensive treatment that results in near normal glycemia, and perhaps minimal glycemic variability, if initiated within 6 years from the onset of diabetes diagnosis and implemented long enough (approximately 4 to 6 years), has beneficial effects extending for at least 8 years. An alternative interpretation of the DCCT and EDIC results suggests that the glucotoxic effects of hyperglycemia (A1C >9%) can persist for at least 8 years.
Patients who are fortunate enough to maintain an A1C of less than 7% for 4 to 6 years soon after being diagnosed with diabetes are less likely to develop complications, because of their ability to induce a protective state of metabolic memory19,20,21,22 In theory, once metabolic memory has been established, any future deterioration in glycemic control would be far less likely to be associated with significant complications. Although the DCCT and EDIC evaluated patients with T1DM, most authorities believe that patients with T2DM who are unable to achieve an A1C of less than 8.5% should be transitioned to insulin therapy without hesitation.25
The current American College of Endocrinology glycemic targets are as follows26:
A1C of 6.5% or lower
Fasting plasma glucose less than 110 mg per dL
2-hour postprandial plasma glucose less than 140 mg per dL
These targets are achievable in primary care. Patients newly diagnosed with T2DM should immediately incorporate both lifestyle interventions (physical activity, medical nutrition therapy, self blood glucose monitoring, diabetes education) and pharmacotherapy into their treatment regimens. Should an individual not be able to achieve an A1C of less than 7%, the regimen should be intensified without hesitation. Insulin (given by either injection or inhalation) with oral agents,27 an incretin mimetic,27a or pramlintide27b should improve the glycemic control.
Early use of insulin therapy is frequently necessary for timely achievement of glycemic goals. In T2DM, glycemic targets can be reached by using basal insulin plus oral agents,28,29 basal-bolus insulin regimens, or premixed insulin analogues.30,31,32 Basal-bolus insulin regimens or insulin pump therapy is indicated for all patients with T1DM.
Insulin therapy should be tailored to minimize hypoglycemic events. Hypoglycemia is less of a risk in patients with T2DM than in those with T1DM. Switching patients away from the older human insulin formulations [NPH and regular human insulin (RHI)] in favor of the newer insulin analogues has been shown to reduce the incidence of hypoglycemia.26 Any form of diabetes management should be individualized to meet the specific needs and conditions of the patient. For example, not every person should be treated to the American Association of Clinical Endocrinology (AACE) recommended target. A 75-year-old grandmother who lives alone and continues to self-inject insulin
P.202
4 months after having endured a hip replacement procedure would certainly be advised to strictly avoid hypoglycemia. Simply keeping this patient free of diabetes symptoms with an A1C target of 8% to 9% might be perfectly acceptable. A more aggressive and intensive approach to diabetes management is warranted in nearly all patients with newly diagnosed T1DM or T2DM.
Primary Care Physicians Can Reduce the Costs of Managing Diabetes
Diabetes is a chronic and costly disease. The annual cost of managing a patient with diabetes is $13,243, approximately six times the per capita cost of an individual without diabetes. Of the $132 billion annual tab for treating Americans with diabetes, $25 billion is spent on managing chronic complications and hospital costs related to hyperglycemia; 52% of these direct costs are devoted to caring for patients older than age 50. By 2020, more than $192 billion will be spent in the United States on diabetes care33 (Fig. 5-2). Reducing the A1C from 10% to 7% decreases the cost of diabetes management by 75%.34
P.203
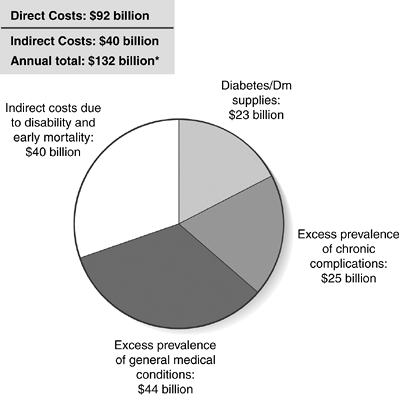 |
Figure 5-2 Economic Consequences of Diabetes in the United States (Approximate 2002 U.S. Dollars). (From Hogan P, Dall T, Nikolov P. American Diabetes Association. Economic costs of diabetes in the US in 2002. Diabetes Care. 2003;26:917 932, with permission.) |
Is intensive diabetes management cost effective? Assuming that 120,000 people in the United States meet the DCCT eligibility criteria, implementation of the intensive rather than conventional therapy protocol would result in a gain of 920,000 years of sight; 691,000 years free from end-stage renal failure; 678,000 years free from lower extremity amputations; and 611,000 years of life. The cost of intensive care in this population would be $4 billion over the lifetime of this population or $28,661 cost per year of life gained. From a healthcare system perspective, the annual cost of intensive therapy ($4,500) is well within the range of cost-effectiveness considered to represent a good value.35
Cost is also a factor when considering how best to intensify diabetes therapy. The simultaneous use of three different oral agents may cost the patient more than $350 per month, whereas a single dose of basal insulin plus a sulfonyl-urea will cost about $90.36
Discussing the I Word with Patients and Their Families
Diabetes is a progressive disease. The UKPDS demonstrated that over time patients' glycemic control worsens no matter what treatment regimen is used (sulfonylureas, metformin, insulin, or diet and exercise).37 Diabetes control does not deteriorate due to lack of patient adherence to their prescribed treatment plans. By the time one is diagnosed as having T2DM, approximately 50% of the pancreatic beta-cell mass has been depleted.37 Of the more than 5,000 patients who participated in the UKPDS, only 9% were able to maintain an A1C less than 7% after 9 years with lifestyle intervention alone compared with 12% of the metformin and 17% of the sulfonylurea patients. The failure of oral medications to improve glycemic control parallels the reduction in ability of the pancreatic beta cells to produce and secrete insulin in response to increasing levels of hyperglycemia. As insulin resistance becomes more severe in association with insulinopenia, nearly all patients with T2DM will eventually require exogenous insulin to achieve the ADA targeted A1C of less than 7%.
Diabetes control in the United States is deteriorating despite the introduction of new oral agents, incretin mimetics, and insulin formulations over the past 2 decades. The percentage of patients with diabetes achieving an A1C less than 7% from 1988 to 1994 was 45%, whereas from 1999 to 2000 only 38% of patients were able to attain this target A1C.38 Physicians must attempt to preserve beta-cell function for as long as possible while recognizing that deterioration in glycemia requires the intensification of treatment paradigms. Allowing patients to linger with high A1C levels will only invite complications to sprout their roots, leading to irreversible end-organ damage. Encouraging a more rapid and progressive approach to intensifying diabetes
P.204
management, a process referred to as clinical inertia, can be achieved as follows:
One should be confident that improving glycemic control will help delay or prevent diabetes-related complications.
Physicians and patients may choose from a variety of different insulin formulations, delivery systems, and treatment protocols as they work toward treatment intensification. Armed with so many management options, each patient can be afforded an opportunity to achieve his or her targeted A1C while minimizing the likelihood of developing long-term diabetes complications.
The clinician should regularly monitor A1C levels in addition to fasting and postprandial glucose readings. One should make appropriate adjustments in treatment plans in a timely fashion. A prospective population-based study by Brown et al.38a suggested that patients with A1C levels exceeding 8% experience a delay in intensification of their therapy of up to 26 months if they are using metformin and 35 months when they use a sulfonylurea as monotherapy. Some patients with T1DM have remained on the same insulin dosing regimen for years despite changes in their weight, meal or work schedules, and changes in symptomatology. One should remember that diabetes management is a work in progress. Doses of insulin that worked well last Tuesday may not be appropriate on the weekend or even prior to the start of the patient's menstrual cycle. Many of these dosing adjustments can be patient-driven. Others must be addressed and prescribed directly by the physician. For example, patients who are able to count carbohydrates can learn to safely dose their premeal insulin levels. However, the decision to intensify therapy from two injections daily to a multiple daily dose regimen should be initiated by the physician.
The physician should always encourage patients to make healthy lifestyle decisions. Behavioral interventions should be reviewed at each visit. This only takes a few moments, yet is critical to a patient's well-being. For example, one should ask a patient, Do you still remember how to treat hypoglycemia? You know, the rule of 15? The International Diabetes Center (IDC) in Minneapolis, Minnesota, has pioneered the use of group education in an effort to reach more people with diabetes. This educational approach has been shown to be as effective as traditional one-on-one education but at substantial cost savings.39 Another innovative approach used by the IDC has been to deploy a certified diabetic educator (CDE) to the worksite of major employers in the community. This intervention had a positive effect on metabolic and educational outcomes.39
One should solicit skillful diabetes educators to assist with patient education. Diabetes is a complicated metabolic disorder. Patients can have successful short- and long-term outcomes using physiologic insulin replacement therapy only if provided with intensive diabetes educational opportunities. CDEs are excellent resources for all aspects of diabetes training. The
P.205
American Association of Diabetes Educators can assist in locating qualified CDEs for patients. (Web site: http://members.aadenet.org/Scriptcontent/map.cfm. Phone: 1-800-338 3633.) Some pharmaceutical companies also provide grants that sponsor CDE group visits to private practices. The CDEs will gladly speak on any aspect of diabetes education that is of interest to the group (diabetes screening, use of insulin delivery devices, management and avoidance of hypoglycemia, exercise, home blood glucose monitoring, sick day protocols, pump therapy, continuous glucose sensing, limb protection, preconception planning, etc.). One should not hesitate to ask the pharmaceutical sales representatives about these outstanding free programs.Pharmaceutical Company Complimentary CDE/Educational Programs Offered Novo Nordisku CDE Direct Eli Lilly Managing Your Diabetes Program (MYD) Sanofi-Aventis A1C Champions Table 5-3 summarizes the barriers that both patients and physicians have toward insulin therapy and offers some solutions as to their resolution. Together, clinicians and patients must work to reduce not only insulin resistance but resistance to insulin.
Timely referrals to specialists can be useful in preventing diabetes-related complications. Communication between the PCP and the specialist is essential in optimizing care. One should be certain that important documentation accompanies the patient to each specialty visit. A patient referred to a nephrologist would likely have a much more efficient visit if the history, physical, and pertinent laboratory studies were in the hands of the consultant at the time of the visit rather than for the patient to simply show up and declare, My doctor sent me here because I got some sick kidneys! Consultants should always be reminded to report any decisions regarding patient management directly to the PCP.
Case 3: Illustrating the Importance of Primary Care Physician and Specialty Communication in the Comanagement of Patients with Diabetes
Juanita is a 66-year-old Hispanic patient with a 20-year history of poorly controlled T1DM, chronic kidney disease, and diabetic amyotrophy. She decided to consult an orthopaedic specialist on her own for terrible leg pains. After a brief workup, which consisted of a magnetic resonance image (MRI) of the knee, a decision was made to perform a total joint replacement on her arthritic right knee. Although the surgeon considered the procedure a great success, the patient had persistent pain postoperatively, which actually worsened over
P.206
P.207
P.208
P.209
a 3-month period. The frustrated surgeon could not understand why the patient was complaining of so much pain when the bone scan and postoperative x-rays showed no evidence of osteomyelitis. The 12 visits of physical therapy also appeared to worsen her discomfort to the point where she became incapacitated by the pain. She was having increasing difficulty with her balance and could not tolerate having any bed sheets come in contact with her feet. Four months after having her knee replacement surgery, she returned to her PCP.
TABLE 5-3 Barriers to Initiation of Insulin Therapy and Potential Clinical Solutions | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
On examination the patient exhibited hyperalgesia, allodynia, and loss of ankle reflexes bilaterally, which was worse on the right (postoperative) extremity. The patient wore a slipper on the right foot to lessen the effects of her painful peripheral diabetic neuropathic pain (Fig. 5-3). The PCP placed the patient on duloxetine, which resulted in a 50% improvement in her overall pain intensity within 3 weeks. Communication between the specialist and the PCP is of utmost importance when managing patients with diabetes. Had the surgeon discussed this case with the PCP prior to operating he would have realized that a more conservative approach was warranted. Not only was this patient's pain the result of diabetic peripheral neuropathy rather than arthritis but her fasting blood glucose level on the day of surgery was 323 mg per dL. The PCP was unaware that the patient was even hospitalized. Had the specialist been concerned about the patient's preoperative laboratory studies (including her A1C of 12.2%), the surgery would have been canceled until she was medically cleared to undergo the procedure. On the second postoperative day, the patient developed acute renal failure.
P.210
 |
Figure 5-3 Severe Diabetic Peripheral Neuropathic Pain Involving the Patient's Right Leg and Foot. The patient is wearing a slipper on her symptomatic side to minimize the hyperalgesia (exaggerated response to pain), which she experiences while wearing sandals. (Photo courtesy of Jeff Unger, MD.) |
Despite being the drug of choice for most patients with diabetes, insulin has a bad reputation with patients and even some physicians. Insulin is often viewed at the drug of last resort one that is reserved for those whose diabetes self-management skills are suboptimal. In reality, if a physician believes a patient requires insulin, chances are he or she does!
Misperceptions regarding insulin therapy have developed into an insulin resistance syndrome championed by patients and physicians alike. How can a physician change the mindset of a patient with poorly controlled diabetes regarding the perception of insulin therapy?
My mom had diabetes, and it was no big deal for her for over 20 years. She rarely saw a doctor, never paid much attention to it, and it never really bothered her. But then her doctor finally convinced her to start insulin and bam! Over the next year she started having problems with her eyes, and P.211
then there were the terrible pains in her feet. Eventually she lost both of her legs. No doubt about it, insulin was the culprit. And now you want me to start shots? No way!
Oral agents lower A1C levels by 1% to 2% (see Chapter 4). If the patient's A1C is higher than 9%, there is very little chance that oral agents alone will move the A1C into the targeted range of less than 7%. Prolonged continuation of oral agents is not warranted in these situations. Poorly controlled patients with significant postprandial hyperglycemia experience anxiety, depression, fatigue, and a hedonistic personality.40 One should ask patients with poorly controlled diabetes how energetic and outgoing they feel 1 to 2 hours after eating their largest meal of the day. Most will respond by saying: I can barely keep my eyes open. My wife wants me to go places and do things, but every joint in my body hurts. I know I'm getting a little irritable these days. Wouldn't you if you worked my kind of hours?
Using a positive, nonthreatening, educational approach, nearly all patients can be convinced that transitioning to insulin would be a good idea. Insulin should never be used as a threat or in a punishing manner for any patient: OK, Sadie, if you can't get your blood sugars controlled by your next visit in 6 months, we'll not hesitate to start you on the needle! This is your last chance to work on that diet and start your exercise program that I've been telling you about for the past 12 years!
One excellent way for patients to understand the effects of hyperglycemia on their bodies and how insulin can immediately improve their symptoms is to use the following visual imagery:
The blood of someone without diabetes is fresh, clean, clear, and pure, just like mountain spring water. On hot days, I bet it could even quench your thirst! On the other hand, someone with diabetes has blood that is sticky, thick and gooey. The blood of someone with diabetes sticks to just about everything your eyes, skin, joints, blood vessels, nerves, kidneys, and heart. In fact, that's how we determine someone's A1C. The more sugar in the blood, the more likely your hemoglobin (which carries oxygen) is going to get stuck in the syrup. High A1C represents sticky blood. By the way, would you want to drink a cup of maple syrup for breakfast every day or a glass of ice water? Now, we can change that syrupy, sticky blood into some clear mountain spring water pretty quickly. All we have to do is use insulin. Shall we try?
Table 5-4 lists some other suggestions that may be helpful in preparing patients for the use of insulin therapy.
Optimizing Adherence with Insulin Therapy
Once insulin therapy is prescribed and accepted, patient adherence to their treatment protocol may diminish. Whereas electronic monitoring studies have documented that patients on oral agents take 67% to 85% of their total doses, up to 66% of insulin prescriptions in patients with T2DM go unfilled.
P.212
Insulin adherence among patients with T2DM is only 60%.41 Reasons for missed insulin doses include forgotten injection time (43%), forgotten supplies (58%), postponement of injections (58%), and purposeful omissions (33%).42 Adolescents may omit injections before check-ups or use lower doses of insulin than children, suggesting the expression of autonomy by dropping doses.43 Some women omit doses to control weight44. Pen users have lower A1C levels than those using syringes and vials (7.64% vs. 8.55%).45 Switching from vials and syringes to insulin pen injectors can improve metabolic control and quality of life for patients with diabetes.46 Pen users tend to miss fewer scheduled injections, demonstrate better treatment regimen compliance, and have a more positive attitude toward using insulin therapy than patients using vials and syringes.47
TABLE 5-4 Helpful Hints to Prepare Patients for the Use of Insulin | |
|---|---|
|
Table 5-5 suggests ways to improve adherence with the prescribed insulin treatment regimen, and Table 5-6 provides helpful Web sites to promote patient adherence.
Another key barrier to initiating and optimizing insulin therapy is fear of inducing hypoglycemia. Hypoglycemia is the rate-limiting, short-term complication that often restricts the ability to intensify insulin therapy. If
P.213
P.214
patients never experienced hypoglycemia, management of diabetes would certainly be simplified. Learning how to avoid, recognize, monitor for, and treat hypoglycemia is an important aspect of diabetes education. The inappropriate timing of supplemental insulin (insulin stacking) doses to correct hyperglycemia must be discussed in detail with all patients (Fig. 5-4).
P.215
TABLE 5-5 Improving Adherence with Insulin Regimens | ||
|---|---|---|
|
TABLE 5-6 Web Sites with Information That Can Help Enhance Patient Adherence to Lifestyle Choices and Pharmacologic Therapy | |
|---|---|
|
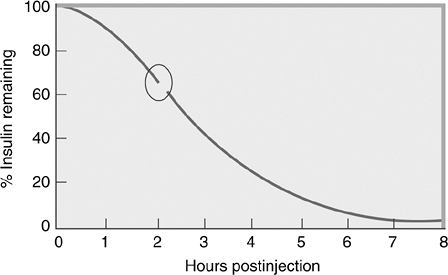 |
Figure 5-4 Insulin Stacking: Rapid-acting Analogue Insulin Action Disappearance Curves. This graph demonstrates the amount of insulin remaining in the subcutaneous depot over time following a subcutaneous injection. After 2 hours (circle), 64% of the original dose remains in the depot and waiting to act. Thus, if 10 U of insulin is given at 10 AM, 6 U remains as active drug at noon. The glucose-lowering effects of rapid-acting analogues persist for up to 6 hours following a subcutaneous injection. If one gives a correction bolus prior to the time the insulin is completely absorbed, hypoglycemia is likely to occur. For example, if the blood glucose level is 200 mg per dL at noon and the patient injects an additional 6 U for lunchtime, the subcutaneous depot has now been increased to 12 U. Patients should always calculate how much insulin remains in the original subcutaneous depot before injecting supplemental insulin. Insulin stacking is a major cause of hypoglycemia and can easily be avoided. |
Hypoglycemia: The Facts
Ninety percent of patients using insulin have experienced a hypoglycemic episode.48
Risk factors for hypoglycemia in patients with T2DM include a prior history of having hypoglycemia as well as the duration of insulin treatment.49
Although the exact level at which one defines hypoglycemia is debated, the glycemic threshold for activation of the anti-insulin neuroendocrine counterregulatory response occurs at a plasma glucose level of 70 mg per dL.50,51
Relative hypoglycemia is defined as the sensation of hypoglycemic symptoms when the plasma glucose levels are normal or above normal. Patients with poorly controlled hyperglycemia may experience relative hypoglycemia as their therapy is intensified. No treatment is needed, although patients should monitor and record their blood glucose levels when they feel symptomatic. Symptoms associated with relative hypoglycemia usually disappear within 2 to 4 weeks when the brain adjusts to the lower ambient glucose levels.52
The opposite is true in intensively controlled individuals with diabetes. They may not recognize hypoglycemia until their plasma glucose is considerably lower than the normal physiologic glycemic thresholds. The changes in glycemic thresholds can be caused acutely by antecedent hypoglycemia and chronically by persistent hyperglycemia.53
Although mild to moderate hypoglycemia may be a fact of life for intensively managed patients with T1DM or T2DM, a single episode of antecedent prolonged morning hypoglycemia can blunt both the counterregulatory hormone and the symptomatic response to subsequent hypoglycemia.54 Repeated episodes of hypoglycemia result in a form of diabetic autonomic neuropathy known as hypoglycemic unawareness. Patients experience a lower glycemic threshold for activation of counterregulatory defenses against hypoglycemia and a limitation to their ability to perceive the symptoms of hypoglycemia, further delaying their efforts to restore euglycemia.55
Neuroendocrine response to hypoglycemia is blunted in patients with advanced T2DM.56 In particular, the normal glucagon response to hypoglycemia is virtually absent in such patients. The glycemic thresholds for autonomic and symptomatic responses to hypoglycemia are shifted to lower glucose concentrations by recent antecedent hypoglycemia. Thus, even in T2DM, hypoglycemia begets hypoglycemia, potentially resulting in hypoglycemic unawareness.
Hypoglycemic symptoms are related to the brain and the sympathetic nervous system. Decreased levels of glucose lead to deficient cerebral glucose availability (i.e., neuroglycopenia) that can manifest as confusion, difficulty with concentration, irritability, hallucinations, focal impairments (e.g., hemiplegia), and eventually coma and death. Stimulation of the sympathoadrenal nervous system leads to sweating, palpitations, tremulousness, anxiety, and hunger. The adrenergic symptoms often precede the neuroglycopenic symptoms and thus provide an early warning system for the patient (Table 5-7).
P.216
TABLE 5-7 Differentiating Adrenergic from Neuroglycopenic Hypoglycemic Symptoms | ||||||
|---|---|---|---|---|---|---|
| ||||||
Minimizing the Risks of Hypoglycemia
The clinician should frequently review the aspects of diabetes self-management that may minimize the frequency and consequences of iatriogenic hypoglycemia: carbohydrate counting, proper timing of oral agents in relation to insulin or exenatide dosing, home blood glucose monitoring prior to driving, and adjustment of insulin dosages prior to exercise or increased physical activity.
The use of alcohol may limit the counterregulatory response of the liver to hypoglycemia. Insulin also minimizes hepatic glucose production. Therefore, patients using exogenous insulin should always eat if they consume alcohol, to avoid inducing severe and prolonged hypoglycemia.
Elderly patients at risk for developing hypoglycemia include those taking multiple oral agents in conjunction with exogenous insulin, impaired renal or hepatic metabolism, dementia, depression, history of a stroke, or suboptimal nutritional intake. The American Geriatrics Society has recommended an A1C of 7% or lower for healthy older adults and an A1C of 8% or lower for frail elderly patients.57
Substitution of preprandial regular insulin with rapid-acting insulin (e.g., glulisine, lispro, or aspart) reduces the frequency of daytime hypoglycemia. Similarly, substitution of a long-acting insulin analogue (e.g., glargine or detemir) for intermediate-acting insulins such as NPH or human premix 70/30 or 50/50 also reduces the frequency of nocturnal and daytime hypoglycemia.58,59
If a diagnosis of hypoglycemic unawareness is made, the solution will involve the acceptance of somewhat higher glucose levels in the short term. At least a 3-week period of meticulous avoidance of hypoglycemia could be
P.217
attempted with the goal of encouraging a return to awareness of hypoglycemia. With the return of symptomatic hypoglycemia, patients can once more work toward achieving better glycemic control.50,60
The Physician's Mission: Prescribe an Exogenous Insulin Regimen That Mimics the Normal Physiologic Insulin Response to Fasting and Postabsorptive Hyperglycemia
The ultimate goal of insulin replacement therapy is to mimic the normal insulin response to hyperglycemia in both the fasting and postprandial states. Individuals with normal glycemia produce enough insulin to keep blood glucose levels in a very narrow range (70 to 140 mg per dL). The concentration of glucose in the plasma of healthy individuals remains within a normal range despite large fluctuations in nutritional intake and physical activity. The fundamental reason for this is the precise balance between insulin secretion from pancreatic beta cells and insulin action on sensitive tissues, primarily adipose tissue, liver, and muscle. After healthy individuals eat, their plasma glucose concentration increases rapidly, peaks in 30 to 60 minutes, and returns to basal concentrations within 2 to 3 hours (Fig. 5-5).
Insulin is normally secreted into the portal circulation in two phases.61 In the fasting state, basal insulin is normally secreted at the approximate rate of 1 U per hour in order to minimize hepatic glucose production.62 Basal insulin also limits lipolysis and excess flux of free fatty acids to the liver, which can result in a state of postabsorptive insulin resistance. The circulating glucose levels are maintained at a level that allows for the extraction of this energy source by obligate glucose consumers such as the central nervous system. The lack of adequate basal insulin stimulates hormone-sensitive lipase and free fatty acid release from fat stores, which in turn stimulates hepatic production and release of ketone bodies, leading to ketogenesis in patients with T1DM. This is not usually seen in patients with T2DM because insulin resistance and persistent high levels of circulating endogenous insulin during the postprandial state maintain inhibition of hormone-sensitive lipase. Basal insulin may also be administered through continuous subcutaneous insulin infusion (CSII) with an insulin pump. Insulin pumps use rapid-acting insulin analogues that are infused subcutaneously throughout the day at predetermined rates.
The intake of food prompts a 5- to 10-times increase in prandial (bolus) insulin release from the pancreatic beta cells. With each meal a rapid first-phase insulin response occurs, which limits the rise in ambient plasma glucose levels. First-phase insulin response terminates quickly so that hypoglycemia does not occur. The second-phase insulin release follows to limit glycemic excursions as carbohydrates are being absorbed from the gastrointestinal tract. This postabsorptive state may last up to 6 hours per meal, depending on the food content. High fat meals (such as pizza) prolong the postabsorptive state.
P.218
A progressive reduction in first-phase insulin response is observed for a number of years prior to the development of T1DM and T2DM.61 Eventually the beta cells are unable to secrete insulin in response to a glucose or nonglucose stimulus, resulting in diabetes.
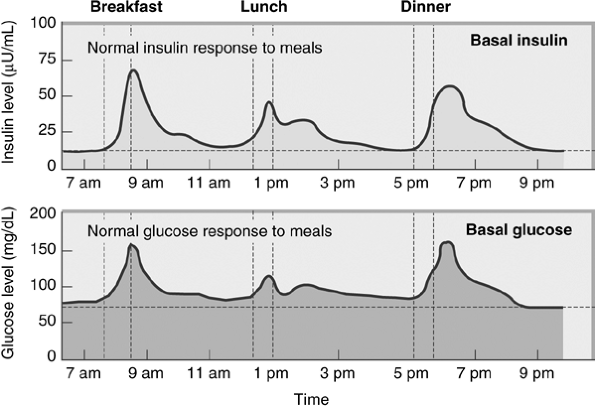 |
Figure 5-5 Normal Physiology of Insulin and Glucose in Response to Meals. Basal glucose levels are maintained in the fasting state as the liver produces glucose (via gluconeogenesis) to keep the blood glucose levels from falling into the hypoglycemic range (<60 mg per dL) (lower graph). Basal glucose is used primarily as an energy source for the central nervous system. As a person eats a meal, postprandial glucose levels rise, but remain less than 140 mg per dL as the carbohydrates are being absorbed from the gastrointestinal tract. Basal insulin is secreted by the pancreatic cells to prevent lipolysis from the adipose tissue and to prevent the liver from producing excessive levels of glucose in the fasting state (upper graph). Eating a meal will result in a rise in prandial insulin levels to maintain the euglycemic state. Normal variables of glucose and insulin homeostasis occur throughout the day. Note that breakfast results in a higher rise of postprandial glucose levels when compared with lunch, triggering a corresponding rise in prandial insulin release from the pancreatic cells. Everybody has insulin resistance in the early morning, because of rising levels of counterregulatory hormones (cortisol and growth hormone) before breakfast. To overcome the hyperglycemic effects of these hormones, the cells produce more insulin in the morning. Insulin resistance resolves by lunchtime, resulting in lower postprandial glucose elevations and lower levels of endogenous insulin release. The absorption of carbohydrates at supper is usually prolonged because most of the daily calories are eaten then. Also, fat content of foods tends to be higher at supper, delaying the absorption of carbohydrates from the gastrointestinal (GI) tract. Although similar amounts of prandial insulin are required for breakfast and dinner, the higher fat content at dinner requires endogenous insulin to be secreted over a longer period to prevent postprandial hyperglycemia. Patients with T1DM should be prescribed a basal-bolus insulin regimen that closely approximates this normal physiologic response to meals. |
Prandial insulin given at mealtimes should be administered to mimic both the first- and second-phase response, without inducing hypoglycemia. Prandial
P.219
insulin must have both a rapid peak onset of action and a duration of action that will continue until carbohydrate absorption is complete (approximately 3 to 4 hours after eating). Rapid-acting insulin analogues should be administered 10 to 15 minutes prior to starting a meal. This will allow plasma insulin levels to rise and minimize the elevation in postabsorptive hyperglycemia occurring within 10 to 15 minutes of beginning a meal. Regular human insulin requires a longer lag time of between 30 and 60 minutes, meaning that patients must wait for up to 1 hour after injecting before beginning their meal. Patients with preprandial glucose levels less than 70 mg per dL should minimize their lag times, whereas those with levels greater than 200 mg per dL should extend their lag times.
Patients can determine their personal insulin lag time using the following method. If the preprandial glucose level is between 100 and 150 mg per dL, the patient administers the prescribed insulin dose. Blood glucose monitoring should be performed every 15 minutes until the blood glucose level drops 25 mg per dL. The time required to reduce the blood glucose level 25 mg per dL can be considered the patient's personal lag time.
If blood glucose levels are elevated in the postabsorptive state, supplemental insulin may be administered to lower the ambient glucose level to a predetermined glycemic target.
Supplemental insulin doses are calculated based on the patient's total daily insulin dose (Table 5-8).
Physiologic insulin replacement regimens include the use of basal plus bolus insulin preparations and premixed insulin analogues. Nonphysiologic regimens include NPH with or without a rapid-acting insulin and a single dose of analogue basal insulin once or twice daily. When deciding on the best insulin regimen, one must consider the likelihood of inducing hypoglycemia, the age of the patient, the activity level of the patient (as strenuous exercise will rapidly increase the absorption of exogenous insulin), and the patient's lifestyle requirements (meal skipping, sleep and work schedule). Patients can increase the likelihood of success with a given prescribed insulin regimen by understanding the pharmacokinetic and glucodynamic profiles of the insulins prescribed. Once insulin is initiated, home blood glucose monitoring can be used to fine tune the doses and improve A1C levels.
The insulins that have been used historically to manage diabetes have pharmacodynamic (variability of absorption from injection site, time to peak effect, duration of action) and glucodynamic (ability to reduce hyperglycemia) effects that are often not physiologic. For example, injecting an obese patient with NPH 50 U may delay the drug's absorption, onset of action, and duration of glucose-lowering effect, resulting in considerable glycemic variability and unpredictable glucose-lowering effect. NPH exhibits variable insulin absorption when compared with basal insulin glargine and insulin pump therapy. The glucodynamics of insulin are more predictable with insulin analogues when compared with NPH and RHI.
Analogues are superior to RHI in their ability to control postprandial hyperglycemia,63 yet RHI and analogues appear to be similar in their ability
P.220
to improve A1C levels.64 When used in insulin pumps, analogues have been shown to be superior to RHI in improving A1C levels,65 which may delay or prevent the development of diabetes-related complications.
TABLE 5-8 Formulas Used to Calculate Insulin Doses for Intensified Basal-bolus Regimens | |
|---|---|
|
Insulin Analogue Formulations
Long-acting (Basal) Insulin Preparations
The two available analogue basal insulins include glargine and detemir. Insulin glargine's biochemical modifications of human insulin result in a shift of the isoelectric point slowing the absorption of the molecule from the
P.221
subcutaneous depot following injection. Once injected, glargine is absorbed at a relatively constant rate over 24 hours with minimal peaking. The glucodynamic effects of glargine improve within 7 days of treatment initiation.66 Whether insulin glargine is taken at dinner or bedtime has no influence on glycemic control.67
Insulin detemir is based on the principle of immediate insulin isolation. Following injection, detemir combines with albumin via the fatty acid side chain engineered into its insulin side chain and enters the circulatory system.68 Later, detemir leaves the circulation, dissociates from the albumin, and acts on the insulin receptor. When compared with NPH, detemir is less likely to induce hypoglycemia, demonstrates superior day-to-day intrasubject absorption variability, and results in weight loss rather than weight gain.69 Both glargine and detemir are available in pen injectors.
The NPH absorption, time to peak onset, and duration of action are not predictable, making this a poor basal insulin (Fig. 5-6). Long-acting insulin analogues have pharmacokinetic profiles that are more physiologic than that of NPH. One important glucodynamic parameter to consider when choosing an insulin is the degree of intrasubject day-to-day variability. Low variability correlates with a more predictable glycemic response throughout the day. For example, one must know that exercising within 1 to 2 hours of injecting a rapid-acting insulin analogue will, in all likelihood, result in a significant increase in absorption of that particular dose. The variability of insulin absorption is most predictable with a rapid-acting insulin analogue used via an insulin pump, minimal with detemir and glargine, and significant with NPH for patients with T1DM.70 This implies that patients using NPH insulin will have difficulty maintaining control of their glucose levels due to daily changes in the rates of insulin absorption for the injection site.
Other factors that influence the onset of action, duration of action, and absorption profiles of insulins include (a) the age of the patient, (b) the patient's weight, (c) the site of injection, and (d) the volume of insulin injected (insulin depot).71
Analogue glucodynamics for both short- and long-acting insulins are fairly consistent and predictable across all age groups. However, the clearance of human insulins in children is variable and dependent on the plasma concentration of circulating growth hormone.72 NPH insulin, when used in children, tends to reach peak concentrations more rapidly than in adults. Thus, children may be prone to developing nocturnal hypoglycemia when NPH is used before supper.73 The use of insulin analogues in children does provide a more physiologic pattern in comparison with human preparations. Children are known to be particularly vulnerable to variable absorption rates due to their unpredictable exercise patterns, tendency for low subcutaneous adiposity, and poor injection technique.
Human insulin absorption is dependent on the weight of the patient. Obesity tends to slow insulin absorption, resulting in even greater intrasubject variability of peak insulin levels.71 RHI regular and NPH insulin absorption
P.222
P.223
from subcutaneous injection sites is also volume dependent. The larger the dose of insulin injected, the slower the absorption. Using smaller human insulin injections improves absorption profiles.71
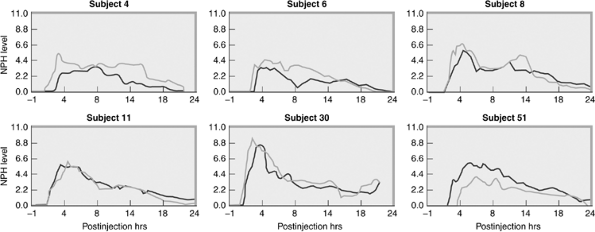 |
Figure 5-6 Variability of Absorption of Neutral Protamine Hagedorn (NPH). To test the variability of insulin absorption, nondiabetic volunteers received equal doses of NPH on two separate days while receiving intravenous glucose to maintain normal glucose levels. The diurnal variability of NPH absorption is 52%. In subject 6, the NPH level is peaking on the fi rst day 8 hours postinjection, but on the second day, the NPH level drops at the same time, only to rise again later in the day. This study suggests that NPH is not a predictable or reliable basal insulin. (From Scholtz HE, Pretorius SG, Wessels DH, et al. Pharmacokinetic and glucodynamic variability: assessment of insulin glargine, NPH insulin and insulin ultralente in healthy volunteers using a euglycaemic clamp technique. Diabetologia. 2005;48:1988 1945.) |
When using human insulins, the site of the injection must be consistent or the glucodynamic effects of the drugs will be less predictable. The fastest absorption of human insulin is from the abdomen, whereas the slowest absorption is from the legs. If NPH is injected into the abdomen before supper, the insulin-lowering effects may be observed quickly, resulting in a higher risk of postsupper hypoglycemia when used in combination with regular insulin. However, by morning, the levels of circulating NPH will be minimal, resulting in fasting hyperglycemia.
The use of both short- and long-acting insulin analogues can significantly improve glycemic control, because their glucodynamic action is independent of patient size, injection site, or size of the insulin depot.
Premixed Insulin Analogues
Premixed preparations combine rapid-acting (prandial) and long-duration (basal) insulins in a single vial or pen injector. Using these fixed-dose insulins can reduce dosing errors that may occur when patients attempt to mix NPH and regular insulin in the same syringe. If one combines NPH with a rapid-acting analogue, the injection must be immediate to avoid alteration in the glucose-lowering effects of the analogue. Patients with visual impairment may have a family member preload their rapid- and intermediate-acting insulin into syringes for use later in the day. However, this may result in absorption variability and hypoglycemia. Use of the premixed preparations is simple, user friendly, and more physiologic than NPH plus regular injections.
The human premixed insulins (Humulin 50/50, Humulin 70/30, Novolin 70/30) combine regular plus NPH in a single dose. Thirty units of 50/50 insulin would consist of 15 U regular plus 15 U of NPH. The 70/30 preparations consist of 70% NPH and 30% regular insulin (Table 5-1). When used, these insulins must be injected at least 30 minutes prior to mealtime.
Analogue premixed insulins include lispro Mix 75/25, lispro Mix 50/50, and aspart Mix 70/30 (Table 5-1). Unlike human mixed insulins, the analogues consist of a set percentage of rapid-acting insulin (either lispro or aspart) plus the rapid-acting insulin combined with protamine, which delays the absorption of that insulin component. By prolonging the duration of action of a percentage of aspart or lispro within the mixed insulin, protamine improves the glucodynamic effect of the insulin. A patient using a mixed insulin would receive the benefits of a basal and bolus insulin in a single injection. Thus, a 20-U dose of lispro 75/25 would contain 10 U of lispro plus 10 U of lispro plus protamine. The analogue premixed insulins should be injected 15 minutes prior to eating to minimize postprandial glycemic excursions.
Although less expensive than the analogues, the mixed insulins are less effective at minimizing postprandial glycemic excursions than analogue
P.224
premixed insulins.74 Premixed analogues can result in hypoglycemia. However, the incidence of severe hypoglycemia appears to be slightly higher for individuals using the human premixed formulations (2% to 14% of patients) versus those using the premixed analogues (2% to 8% of patients).75
Inhaled (Pulmonary) Insulin
Numerous attempts have been made to develop noninjectable routes of insulin delivery that are clinically effective, easy to administer, well tolerated, and demonstrate minimal long- or short-term adverse events. Of all of the potential noninvasive insulin-delivery options, the pulmonary route is the most clinically viable. The high permeability of the bronchial alveoli (often only having a single-cell border between the bronchial surface and the pulmonary vasculature system), coupled with the large lung surface area (approximating the size of a tennis court) and multiple target organs (500 million alveoli), provides favorable anatomy for efficient drug absorption and delivery.
Although physicians are aware of the need to intensify diabetes therapy in patients who are experiencing inadequate control, there is often reluctance to do so by both specialists and PCPs.76 The current paradigm for treatment of T2DM suggests that lifestyle interventions be initially prescribed, followed by initiation of monotherapy, followed by combination therapy, and ultimately by insulin. This process of intensification may take 8 to 10 years, during which time diabetes-related complications begin to present clinically.77 If the time course for intensification is reduced by 50%, patients can be started on insulin more quickly and show more rapid improvement toward a safe and acceptable A1C target (Fig. 5-7).
Inhaled insulin (INH) delivery may offer the physician an opportunity to introduce a patient to insulin faster than if only subcutaneous injections were available. INH can be given in combination with oral agents or with basal insulin. Human regular insulin and INH have very similar glucodynamic features78 (Table 5-9). INH has a more rapid onset of action, similar to a rapid-acting insulin analogue, while having an effective duration of action of 6 to 8 hours, comparable to RHI.
INH efficacy and safety have been assessed in more than 4,200 subjects with T1DM and T2DM.79,80,81 Some patients have used INH for as long as 7 years and continue to receive the drug as part of ongoing extension studies. Primary endpoints in multiple clinical trials include improvement in A1C. Secondary endpoints have evaluated postprandial glucose levels, fasting glucose levels, incidence of hypoglycemia, weight change, and patient-reported outcomes. Safety endpoints such as pulmonary function studies, adverse events, and the formation of insulin antibodies have all been evaluated. Excluded from INH clinical trials have been patients who have smoked at any time 6 months before initiation of INH, those with poorly controlled asthma or clinically significant pulmonary disease (based on baseline pulmonary function testing), or anyone with a significant chest radiograph abnormality.
P.225
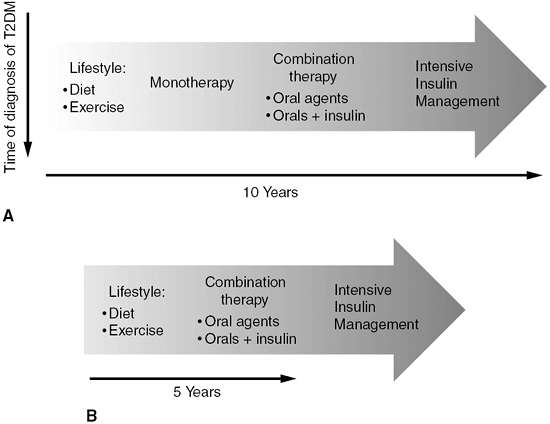 |
Figure 5-7 A: Traditionally, lifestyle intervention is used initially to manage patients with type 2 diabetes (T2DM). Over time, as glycemic control worsens, an oral agent is started. As diabetes control deteriorates over time, combination therapy using triple oral agents with or without a basal insulin is often prescribed. Patients may be reluctant to begin insulin therapy, and physicians may be reluctant to suggest this degree of diabetes intensification. On average, insulin is prescribed and initiated 10 years after a diagnosis of diabetes. This delay in using insulin may result in microvascular and macrovascular long-term complications. B: Moving more rapidly from lifestyle intervention to combination therapy and finally to the initiation of insulin may reduce by 50% the length of time one's glycemic control is poorly managed. This can be accomplished by considering combination therapy immediately in conjunction with lifestyle intervention. If the patient's A1C cannot be reduced to less than 7% after 4 months, consider intensification of the insulin regimen. |
Clinical trials comparing RHI and INH have consistently shown comparable improvements in A1C and postprandial and fasting glucose levels.82,83 Patients using INH experience less hypoglycemia and weight gain when compared with those using subcutaneous insulin.82,83 Patient satisfaction consistently favors the use of INH.82,83,84 Inhaled insulin as either monotherapy or add-on therapy improves glycemic control in patients with T2DM in whom lifestyle modification and/or oral therapy fails.85 Extension studies of up to 4 years in duration indicate that INH can maintain glycemic control in patients with T1DM or T2DM.86 Pulmonary function studies performed on patients using INH show no significant changes in forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), total lung capacity (TLC), and carbon monoxide diffusion capacity (DLCO) over time.82
P.226
TABLE 5-9 Characteristics of Human Insulin Preparations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
INH is highly acceptable to and preferred by patients with T1DM and T2DM when compared with subcutaneous insulin administration. In a patient satisfaction study,84 85% of patients treated with INH during an initial 12-week safety and efficacy trial chose to continue treatment during a 1-year extension study, whereas only 21% of patients initially treated with subcutaneous insulin chose to remain on injectable insulin. In the same trial, patients treated initially with subcutaneous insulin before switching to INH showed significant improvement in overall satisfaction from baseline over the course of the 1-year extension trial. Patients choosing to return to subcutaneous insulin administration from INH had lower satisfaction than with INH.
The most common adverse effects reported in the premarketing clinical trials include chest pain and cough. The chest pain occurred in 4.7% of Exubera-treated patients and 3.2% of the patients in the comparator (subcutaneous insulin) group and is best described as nonspecific. Two patients in the Exubera and one patient in the comparator group discontinued treatment due to chest pain.
P.227
Of patients taking Exubera, 29.5% experienced cough versus 9% of comparator patients. The cough, which was nonproductive and mild, occurred most commonly within minutes of inhaling the drug and decreased with continued use of Exubera.86a
The exact mechanism by which insulin absorption occurs across the pulmonary epithelium is unknown. Absorption of INH may be affected by the patient's age, the presence of an upper respiratory tract infection, or concomitant pulmonary disease. Although absorption of INH is similar across all age groups, the glucose-lowering effect is reduced in elderly patients.87
Absorption of INH is also affected by smoking. A study of nondiabetic active smokers without apparent pulmonary disease showed a 50% increase in rate of absorption and a 40% more rapid time to reach peak concentration.88 Within 1 week of smoking cessation, the pharmacokinetics of INH appear to normalize. However, once patients resume smoking, absorption and onset to peak concentration will again occur more rapidly.88 Thus, patients should be advised to stop smoking when using INH to reduce glycemic variability.
A primary concern for any patient using exogenous insulin is the immunologic safety of these products. High-dose INH delivered to the large alveolar surface triggers the lung's respiratory defenses and produces anti-insulin antibodies. The formation of anti-insulin antibodies [immunoglobulin (Ig)G] occurs with the use of subcutaneous and inhaled insulin.89 The primary reason for antibody production is the presence of impurities in the drug product. Although antibody production is higher with INH compared with subcutaneous insulin, this immunologic event is not clinically significant. Long-term safety studies are being conducted to determine the role of insulin antibodies in the metabolic control of diabetes and the effect of INH on the immune systems.
The initial dose of inhaled insulin is based on the body weight of the patient (Table 5-10). Unlike subcutaneous insulin, INH is dosed based on milligrams instead of units (U). Two doses of INH blister packs are available: 1 mg and 3 mg. A single blister pack is inserted into the handle of the inhalation device (Fig. 5-8) where a pneumatic device punctures the insulin pack, producing an insulin cloud, which is visible within the clear plastic chamber. Additional blister packets may be inserted one at a time into the handle depending on the prescribed dose. The insulin is inhaled slowly at the beginning of a deep breath. The volume of the holding chamber is less than 20% of a deep breath, making inhalation simple. Following inhalation, the patient holds the breath for 10 seconds. The insulin should be inhaled 10 minutes before mealtime. Dose adjustments in 1-mg increments can be made dependent on the average blood glucose readings taken before lunch, dinner, and bedtime over a 2- to 3-day period (Table 5-11). Some patients are also adept at carbohydrate counting successfully with inhaled insulin. Physicians who use INH should familiarize themselves with the marketed doses (Table 5-12) and the dose equivalents of INH versus rapid-acting prandial insulin analogues (Table 5-10).
P.228
TABLE 5-10 Suggested Dosing Protocol for Inhaled Insulin (INH) | |||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||
INH requires much more in-office training time than using other insulin delivery devices such as pen injectors or syringes and vials. Patients using the currently available inhalation device must load, puncture, release the insulin cloud, and inhale the insulin within 30 seconds for each blister pack used. The inhaler must be kept clean and various components should be replaced every 2 weeks (the replacement parts come with the insulin kits available through the pharmacy). In the author's experience, most patients become adept at using the inhalation chamber and self-titrating their prandial doses of insulin within 1 to 2 weeks of starting INH. Other than issues related to formulary coverage, drug costs, and the time required to train patients to use INH, this drug has been well received in the author's primary care practice.
INH can be used in combination with oral agents or basal insulin. Dose adjustments are determined based on targeted A1C and postprandial glucose level targets similar to those with subcutaneous insulin. Patients who develop an acute illness while on INH (such as pneumonia or bronchitis) or require hospitalization may need to be switched temporarily to subcutaneous insulin.
Although children have been included in clinical trials using INH, the treatment of children younger than 18 years is not recommended. There are also no data currently available on the use of INH during pregnancy. Several inhaled insulin products are in development at this time in addition to Exubera (Table 5-13).
INH is not a drug that will be embraced by every patient with diabetes. Those who are doing well on their current physiologic regimen or on insulin pump therapy would gain little advantage to switching to this form of therapy. One should remember that insulin is insulin, whether inhaled or injected.
P.229
The efficacy is similar for patients using subcutaneous insulin or INH. For patients who would like to use INH, one should consider keeping the following pre-Exubera checklist handy:
 |
Figure 5-8 Inhaled Insulin Blister Powder Packets Shown with an Inhalation Device. The packets are inserted into a chamber and opened by a pneumatic mechanism that releases an insulin cloud into the clear chamber. Within 60 seconds of the appearance of the insulin cloud, the patient inhales through the mouthpiece using a single breath. The patient is then instructed to hold his or her breath for 5 seconds. |
If the patient has T1DM, is a long-acting insulin analogue also being prescribed?
If the patient has T2DM, will oral therapy either as mono or combination therapy be continued?
Has the patient smoked within the past 6 months? (Effects of INH pharmacokinetics on passive cigarette smokers remain unknown.)
P.230
TABLE 5-11 Dose Titration of Exubera
Recommended Goal (mg/dL) If 2 of the Last 3 Measures for the Same Meal Are Not at Goal Prelunch test 90 130 Adjust prebreakfast dosea Predinner test 90 130 Adjust prelunch dosea Prebedtime test <180 Adjust predinner dosea Notes: (1) Due to the physics of crystallized insulin inhalation, consecutive inhalation of three 1-mg dose blisters results in significantly greater insulin exposure than inhaling one 3-mg dose blister. Thus, 1 mg 1 1 mg 1 1 mg DOES NOT 5 3 mg. (2) If a 3-mg blister is unavailable, patients should temporarily substitute two 1-mg blisters for a single 3-mg blister and carefully monitor their postprandial glucose levels. (3) The fewest number of blister packs should be used per dose. Thus, instead of using four single 1-mg blisters, inhale 1 mg 1 3 mg 5 4 mg 5 12 U of subcutaneous insulin.
aDose adjustments are in 1-mg increments (see Table 5-11).Does the patient have a history of asthma or pulmonary disease?
Has the patient had a spirometry (FEV1) assessed prior to the initiation of therapy? (All patients on INH should have a repeat spirometry performed after being on the drug for 6 months and every year thereafter.)
If the patient's FEV1 has shown a 20% or greater decline from baseline, the test should be repeated. If the decline is confirmed, the drug should be discontinued.
Is the patient willing to undergo the extensive training required for successful implementation and use of INH?
Does the patient have the financial resources (formulary coverage) to finance the use of the INH?
Would the patient most likely experience an improvement in overall quality of life while using INH versus subcutaneous insulin?
Will the patient be using carbohydrate counting or self blood glucose monitoring averages to perform dose titrations?
P.231
TABLE 5-12 Exubera Available in Two Combination Packs | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 5-13 Pulmonary Insulin Delivery Systems under Development | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Case 4: Initiation of Inhaled Insulin
Virginia is a 48-year-old woman diagnosed 3 years ago as having T2DM. Initially, her fasting glucose level of 235 mg per dL and her A1C was 8.9%. She had been symptomatic for 6 months prior to the date of diagnosis, complaining only of chronic fatigue and loss of appetite. She has gained 20 pounds in the past year. Virginia is 64 inches tall and weighs 220 pounds. She refuses to participate in an exercise program because her legs bother her whenever she walks. She is beginning to lose her balance and feels certain that she could fall at any time. On her initial visit to the office, she was placed on a glipizide XL 20 mg at bedtime. Eight weeks thereafter metformin 500 mg with breakfast and dinner was added to her regimen. As a result of this rapid intensification of diabetes therapy, her A1C fell to 6.7%. Virginia's mother had T2DM and suffered a fatal MI at age 56. Her mother also had experienced severe diabetic peripheral neuropathic pain. In addition, a 52-year-old brother was started on insulin last year.
Six months following successful intensification of her treatment program, Virginia's fasting glucose levels are averaging 170 mg per dL. Her A1C has increased to 8.6%. The doctor discusses the need for insulin therapy, but Virginia refuses, citing the concern that her mother was placed on insulin just 2 weeks before her death. Doctor, you may be right, but I know how much my mother suffered as soon as she started using the needle. She died before she could get the first vial refilled! Virginia knows in her heart, however, that her outcome will be similar to her mother's if she were to begin insulin injection therapy.
The doctor points out to Virginia the importance of improving the A1C and addresses her safety concerns regarding insulin. He informs Virginia that adding a third oral agent would, at best, lower her A1C to 7.4%, which is still above the
P.232
ideal glycemic target. Reluctantly, the physician adds a thiazolidinedione (TZD) to the patient's regimen and repeats the A1C test 4 months later. However, the A1C has increased to 9.2% and her fasting glucose levels are averaging 230 mg per dL. As the patient is becoming more symptomatic, the physician suggests adding inhaled insulin to augment her oral medication regimen. After realizing that the oral medications are no longer effective, the patient agrees to start INH.
After becoming familiar with the inhalation device, Virginia is advised to begin the following regimen:
Breakfast: Exubera 4 mg (3 mg + 1 mg)
Lunch: Exubera 4 mg (3 mg + 1 mg)
Dinner: Exubera 4 mg (3 mg + 1 mg)
Metformin 850 mg is continued with breakfast and dinner
Over the next 3 days her average blood glucose levels are as follows:
Prelunch: 194 mg per dL
Predinner: 222 mg per dL
Prebedtime: 187 mg per dL
She increases her premeal insulin doses by 1 mg per meal for a total of 15 mg per day. Over the next 3 days her average blood glucose levels are as follows:
Prelunch 126 mg per dL
Predinner: 110 mg per dL
Prebedtime: 156 mg per dL
Four months later her point-of-service A1C is 6.9% (reduction of 1.7%). She not only feels much better but delights in the fact that she has lost 5 pounds (most likely the result of having discontinued the TZD and the sulfonylurea).
Initiating Insulin Therapy in Patients with Type 2 Diabetes
Consensus opinion on how or when to initiate insulin treatment in patients with T2DM is lacking. In general, insulin should be initiated under the following circumstances:
Patients with LADA
Individuals with symptomatic diabetes (thirst, weight loss, visual impairment, paresthesias)
Patients with advanced renal or hepatic disease
Patients who are unable to tolerate oral agents
Patients with intercurrent events such as MI, cardiovascular accident, cerebrovascular accident (CVA), acute illness, or surgery
Patients with a triglyceride level higher than 700 mg per dL, especially in patients with coronary artery disease, as hypertriglyceridemia worsens insulin resistance and risk for cardiovascular events38
Patients who are unable to reduce their A1C less than 7% after using combination oral hypoglycemic agents for 4 months or longer
Patients using corticosteroids
A patient who is not responding to exenatide or is unable to achieve the targeted A1C while on exenatide
Patient becomes pregnant
P.233
Case 5: Initiation of Insulin Therapy Using Basal Insulin Plus Oral Agents
Mrs. Jones is a 54-year-old African-American patient who was diagnosed as having T2DM 7 years ago. She is currently taking pioglitazone 45 mg daily, glipizide XL 20 mg daily, and metformin 1 g twice a day. Her A1C is 9.0% and although she is symptomatic (blurred vision, fatigue, paresthesias in hands and feet) her autoimmune antibody studies are negative, indicating that she does not have LADA. Her father died of chronic renal failure secondary to diabetes at age 49. Mrs. Jones' physician suggests using insulin to improve her glycemic control. However, Mrs. Jones refuses to take insulin until she gets a second opinion from a specialist. There must be another pill I can use so that I don't have to start with that needle says the frustrated patient.
Mrs. Jones agrees to being placed on a continuous glucose sensor monitor (CGMS), which is inserted into the skin of her abdomen and worn for 3 days. The device allows the recording of nearly 300 interstitial glucose readings each day. The information is stored in the meter and then downloaded in the physician's office for interpretation (Fig. 5-9).
When the patient was shown the results of her CGMS, she admitted that continued use of oral agents alone was not warranted and she agreed to begin insulin therapy.
Before deciding which insulin regimen to use for a patient with T2DM, one must evaluate the following patient characteristics:
What is the lowest A1C target a patient can safely achieve?
Is the patient willing and able to perform home blood glucose monitoring?
How highly motivated is the patient toward achieving the targeted A1C goal?
Are there any comorbid medical complications that could make intensive insulin therapy risky (history of MI, stroke, visual impairment, hypoglycemic unawareness, and history of severe hypoglycemia requiring the assistance of another person for reversal)?
Are there any financial issues that might limit the patient's ability to afford treatment intensification?
Should the patient's initial therapy focus on improving the fasting for postprandial hyperglycemia?
P.234
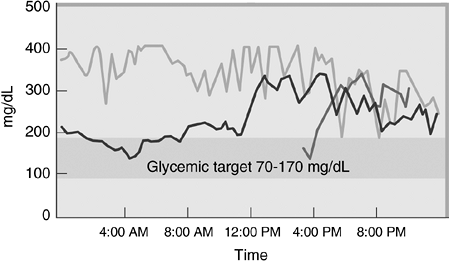 |
Figure 5-9 Mrs. Jones's Continuous Glucose Sensor Meter Reading. The continuous glucose sensor monitor (CGMS) reads interstitial glucose levels every 5 minutes over a 72-hour period and records the data points in a monitor worn on the patient's belt. When the monitor is downloaded onto a PC, the patient's glycemic patterns are easily visualized. The CGMS can detect interstitial glucose values ranging from 40 to 400 mg per dL. In this patient, interstitial glucose values are clearly above the prescribed target of 70 to 170 mg per dL. In fact, the straight lines at the top of the chart suggest that the patient's glucose excursions are exceeding 400 mg per dL for prolonged periods. |
Insulin remains the most powerful and versatile pharmacologic agent available to control hyperglycemia. Not only will the immediate and intensive use of insulin in Mrs. Jones improve her overall glycemic control but she will become less symptomatic. The treatment target should be to drive the A1C to less than 7% without inducing hypoglycemia or excessive weight gain. This target cannot be achieved with any agent other than exogenous insulin. As reported in the UKPDS, a 2% reduction in this patient's A1C should reduce her risk of microvascular complications by 74% and MI by 28%.90 Because this patient was diagnosed with T2DM 7 years ago, her exposure to hyperglycemia has been sustained for perhaps 17 years. Intensification of her diabetes regimen is mandated to minimize the progression of any of her possible long-term diabetes-related complications.
There are no medical contraindications to insulin therapy. Although no insulin has a category A pregnancy classification, regular and NPH insulin have been used extensively in pregnant women. Lispro has a category B classification and aspart, glulisine, detemir, and glargine have a category C classification. Glargine is approved for use in patients 6 years and older; no other insulins have an age restriction.
Weight gain is a common side effect of insulin therapy. In the UKPDS, patients taking insulin gained 4 kg more than those treated with diet therapy over 10 years. Weight gain can be minimized by increasing exercise, restricting calories, and administering metformin concurrently. Table 5-14 lists some of the many insulin protocols that may be considered in patients with T2DM.
P.235
TABLE 5-14 Insulin Protocol Options for Patients with Type 2 Diabetes | ||
|---|---|---|
|
The question always arises as to whether one should target the fasting or postprandial glucose levels for improvement based on the A1C. A recent study examined the relative contributions of the FPG and the PPG levels to the total A1C.91 The relative contribution of PPG excursions to A1C levels is predominant in patients whose diabetes is well controlled, whereas the contribution of fasting hyperglycemia to A1C increases gradually as overall glycemia deteriorates (Fig. 5-10). At lower A1C levels (i.e., <7.3%) the contribution of PPG was found to be two times greater than that of fasting hyperglycemia. However, for patients with A1Cs greater than 10.2% the reverse was found to be true. The crossover from primarily postprandial to fasting hyperglycemia contribution occurred at an A1C of approximately 8.4%. This has important clinical implications, because as a patient approaches the target A1C of lower than 7%, PPG excursions should be minimized. Patients with A1Cs greater than 8.5% might choose to focus initially on improving their fasting hyperglycemia.
The method one chooses for initiating insulin therapy should provide the patient with relief from diabetes-related symptoms (fatigue, thirst, hunger, weight loss, nocturia, blurred vision, dry skin, and, in women, vaginitis) and reduce the A1C toward the target of 7% or less. This requires that A1C testing be performed at least every 3 months to make certain that progress is being made toward improved glycemic control. Point-of-service A1C testing in the office setting would allow physicians to monitor progress at the time of the office visit rather than retrospectively once the patient's laboratory tests are viewed days later.92 Point-of-service A1C testing can be performed by a fingerstick method similar to checking a blood glucose level. Results are available within 5 minutes and the test accuracy is exceptional.92 Worsening
P.236
of glycemic control after initiating any insulin therapy should prompt one to consider an alternative treatment sooner than later.
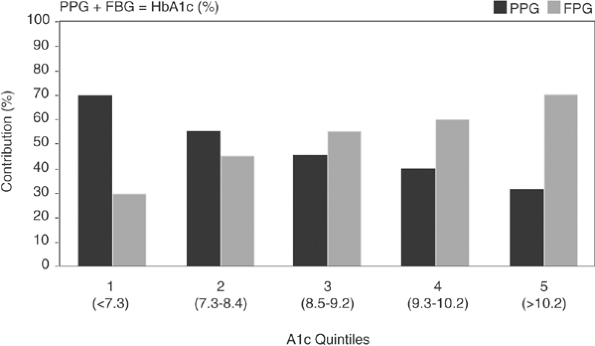 |
Figure 5-10 A1C Levels Less Than 8% Are Determined Primarily by Postprandial Glucose Levels. As A1C levels increase greater than 10.2%, more than 60% of the total A1C is based on fasting glucose levels. Therefore, patients with significant A1C elevations should focus on controlling fasting glucose excursions, whereas those with milder hyperglycemia should improve their postprandial glucose levels. FPG, fasting plasma glucose; PPG, postprandial glucose. (Adapted from Monnier L, Lapinski H, Colette C. Contributions of fasting and postprandial plasma increments to the overall diurnal hyperglycemia of type 2 diabetic patients. Variations with increasing levels of A1C. Diabetes Care. 2003;26:881 885.) |
A simple progression from oral agents can be accomplished by using a sulfonylurea with a basal insulin (glargine) in a treat-to-target protocol such as the one shown in Table 5-15. This treat-to-target regimen has allowed up to 60% of overweight T2DM patients with A1Cs ranging from 7.5% to 10% to reduce their A1C to 7% while remaining on their oral agents.29 Patients were able to achieve their targeted A1C within 6 months by simply titrating the dose of their basal insulin so that their average FPG levels would be lower than 100 mg per dL for 48 hours each week.
The basic principles one must consider when adding insulin to intensify the T2DM regimen include the following:
Using some form of a fixed-dose treat-to-target protocol, most patients will be able to achieve their targeted A1C levels.
Continuing one or more oral agents while adding a basal insulin will improve the likelihood of achieving the targeted A1C levels.93
Basal analogues cause less hypoglycemia and minimize glycemic variability in comparison to human NPH insulin.
P.237
TABLE 5-15 Treat-to-target Protocol Using Bedtime Insulin Glargine Plus an Oral AgentA
Fasting Plasma Glucose Average over the Past 2 Days (mg/dL) Insulin Glargine Dose Adjustment (U/day) 180 +8 140 180 +6 120 140 +4 100 120 +2 <72 within the past week 0 <56 within the past week -2 to -4 aThis forced-titration protocol required that patients be contacted by a research center on a weekly basis. Based on their mean glucose readings over the previous 2 days of a reporting period, the insulin dose was adjusted in an attempt to target fasting glucose levels to <100 mg/dL. With this protocol, nearly 60% of the 756 subjects using either NPH or basal insulin glargine were successful in achieving an A1C of 7% within 6 months.
Data from Riddle MC, Rosenstock J, Gerich J; Insulin Glargine 4002 Study Investigators. The treat-to-target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care. 2003;26:3080 3086.Adding basal insulin to oral agents is simpler than using mixed insulin analogues.
Although the ultimate goal in managing diabetes is to achieve a satisfactory A1C, one must also consider secondary outcomes, such as weight gain. The frequency and severity of hypoglycemic events must also be assessed. Always remember to put safety first when prescribing any form of intensified therapy.
Customized treat-to-target protocols should also be considered. An example of a customized regimen would be as follows:
Begin using 10 U of basal insulin at bedtime while continuing both the sulfonylurea and the metformin at the current dose.
Increase the dose of basal insulin every 3 days by 3 U until the FPG levels are between 70 and 110 mg per dL for 7 consecutive days.
If a single FPG level is less than 70 mg per dL during any 7-day period, reduce the basal insulin dose by 1 U.
Mrs. Jones (Case 5) was advised to begin using glargine 10 U at bedtime and increase the dose 3 U every 3 days until her FPG levels were between 70 and 110 mg per dL for 7 consecutive days. She continued to take metformin 1 g with breakfast and dinner and glipizide XL 20 mg at bedtime. After 12 weeks her daily glargine dose had steadily risen to 49 U, and her A1C had been reduced successfully from 9% to 7%. She had recorded a single episode of hypoglycemia in her computerized glucose meter download for which she
P.238
required no treatment. Mrs. Jones claimed that she was feeling significantly more energetic, despite gaining 2 pounds. The physician congratulates Mrs. Jones on her outstanding efforts toward intensification and advises her to continue home blood glucose monitoring both fasting and at bedtime (postprandial). An upward trend in glucose readings at either time could be an indication of disease progression that would require additional therapeutic intensification. Mrs. Jones understands that her diabetes treatment is a work in progress. Future therapeutic corrections in no way should be viewed as reflecting one's degree of compliance, but rather as a means by which intensification of diabetes control can be maintained indefinitely.
Case 6: Achieving A1C Targets Using Mixed Insulin Analogues
Bill is a 58-year-old man who was diagnosed with T2DM 14 years ago. Despite the use of glipizide XL 20 mg, metformin 2 g, and pioglitazone 45 mg daily, his diabetes control is deteriorating. He is experiencing distal paresthesias in his extremities and has erectile dysfunction. His last dilated funduscopic examination revealed proliferative retinopathy that was not present 12 months ago. Clinical information obtained at the time of today's visit reveals the following:
A1C = 9%
Meter downloads show that only 20% of his fasting glucose levels are between 70 and 170 mg per dL
Weight has dropped 3 pounds in the past month, yet the BMI remains elevated at 35 kg per m2
The decision is made to begin Bill on glargine 10 U in the morning while continuing the glipizide XL and metformin doses as before. The TZD will be stopped for fear of inducing additional weight gain. Bill is advised to call into the office each Monday with the results of his fasting blood glucose levels so that the dose of AM glargine can be increased to target fasting blood glucose levels less than 100 mg per dL.
Three months later, Bill returns for a follow-up. Using the treat-to-target protocol, the glargine dose has been increased to 48 U every morning. His home blood glucose meter downloads show that 55% of his readings are within the 70 to 170 mg per dL target. His point-of-service A1C has improved to 8.1% and he remains mildly symptomatic, complaining of increasing fatigue especially after meals. Although his fasting glucose levels are improved, the A1C target has not been attained. A decision is made to intensify Bill's insulin regimen.
Bill's physician knows that mixed insulin analogues can offer the following advantages:
Mixed insulin analogues offer coverage for both PPG and FPG in a single injection.32
More patients using mixed insulin analogues are able to attain the ADA-targeted A1C of less than 7% than are patients using glargine insulin alone.32
The mixed insulin analogues can be delivered via pen injectors, which improves dosing accuracy and patient satisfaction over syringes and vials.94
For patients having a fixed meal and activity schedule, mixed insulin analogues may offer a safe, simplistic, and effective alternative to basal-bolus insulin regimens. To achieve the lowest and safest A1C, mixed insulin analogues may be administered once, twice, or three times daily.31
Mixed insulin analogues are as effective as a basal-bolus regimen in allowing patients to safely achieve their targeted A1C levels.95
P.239
Bill is placed on NovoLog Mix 70/30 (BIAsp 70/30) 10 U 15 minutes before breakfast and 10 U 15 minutes before dinner. Metformin is continued as his only oral agent. The doses of the mixed insulin are titrated by the patient every 3 days to target an FPG less than 100 mg per dL and a predinner glucose less than 140 mg per dL. After 6 weeks, Bill reports that his prebreakfast dose of NovoLog Mix 70/30 is 36 U and his pre-dinner dose is 44 U. A review of his home blood glucose meter download data reveals that 50% of his glucose readings fall within the range of 70 to 170 mg per dL. He has recorded no numbers lower than 85 mg per dL. His 14-day glucose average is 144 mg per dL and his point-of-service A1C is 7.4%. Bill says he is feeling better but is concerned about his 4-pound weight gain, the high dose of insulin that he is using, and the fact this his blood glucose levels remain suboptimal.
As glycemic control worsens, intensification of the insulin regimen is necessary. One must attempt to target the lowest A1C that can be safely achieved, with the rate-limiting step most often being the risk of treatment-emergent hypoglycemia. Acceptance of insulin intensification may be improved if the prescribed insulin regimen is simplified and if the patient takes an active role in dosing self-determination. A simple way to lower A1C levels is with the use of mixed analogue insulins (Humalog Mix 75/25, Humalog Mix 50/50, NovoLog Mix 70/30). Clinical trials have demonstrated that up to 77% of patients with poorly controlled diabetes can achieve an A1C lower than 7% using analogue mixed insulin.30,96
Patients with T2DM who have A1C levels less than 8.5 % should focus on improving their postprandial glycemic control.91 Premixed insulin analogue treat-to-target protocols have been used successfully to achieve A1C levels less than 7% in more than 80% of type 2 patients.30,31,74,75,96 The premixed insulin analogues allow rapid intensification of diabetes therapy using user-friendly fixed-dose adjustment protocols. For example, in the 1-2-3 Premixed Study31 patients initially added once daily Novolog Mix 70/30 within 15 minutes of eating dinner while continuing their oral agent regimen (Table 5-16).
Insulin-na ve patients began treatment with 12 U of NovoLog Mix 70/30. Patients previously taking insulin injected either the same number of units of NovoLog Mix 70/30 as their prestudy basal insulin dose (up to 30 U) or
P.240
70% of their prestudy basal insulin dose if they were taking more than 30 U. Patients were instructed to self-adjust their dinner insulin doses every 3 to 4 days based on the average of three previous prebreakfast blood glucose values. After 12 weeks, those patients who did not achieve an A1C of 6.5% or less were told to add a second injection of NovoLog Mix 70/30 before breakfast. Those with blood glucose levels averaging less than 110 mg per dL began using 3 U before breakfast, whereas those with blood glucose levels greater than 110 mg per dL initially used 6 U. Forced dose adjustments were made every 3 days based on prebreakfast and predinner blood glucose values, and any oral insulin secretagogues used during phase 1 were discontinued.
TABLE 5-16 1, 2, 3 Premixed Study Adjustment Algorithmaa | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
After an additional 16 weeks, those patients who had not achieved an A1C of 6.5% or less added a third injection of NovoLog Mix 70/30 3 U before lunch. Prelunch dose adjustments were made every 3 to 4 days based on the 2-hour postlunch blood glucose averages. Patients could continue adjusting their prebreakfast or predinner insulin doses but were cautioned not to adjust more than one of these prandial doses at a time. A final A1C was performed on these three-times daily injectors 16 weeks after beginning their prelunch insulin. The 74% of patients who followed the treatment regimen and dose titration schedules until they either obtained their targeted A1C at the end of each phase or completed all three phases of study were very successful at improving their glycemic control. And 77% of these patients successfully achieved the American Association of Clinical Endocrinologists (AACE)
P.241
targeted A1C of less than 6.5% and 88% achieved the ADA targeted A1C of less than 7%. This study suggests that patients with T2DM can be treated successfully to target using a mixed insulin analogue and a fixed-dose adjustment protocol (Table 5-17).
TABLE 5-17 Using the 1-2-3 NovoLog Mix Forced Titration Protocola | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
This same protocol can be useful in clinical practice. Patients can be instructed to either self-adjust the insulin dose twice weekly or call the nurse twice a week to receive verbal instructions on dose adjustments. By rapidly adjusting premixed insulin, A1C improvement can occur within a matter of weeks not months. In the past, patients were more likely to be placed on a fixed dose of premixed insulin with dose adjustments occurring only once or twice a year, based on a lab-generated A1C. Thus, the rapid-fixed dose adjustment protocol appears to be much more efficient and can be used with any premixed insulin analogue, including Lispro Mix 75/25.
After determining that a patient should be transitioned to insulin therapy, should one begin treatment with a long-acting basal insulin analogue or could the patient achieve the target A1C goals using a mixed analogue insulin? The INITIATE trial32 evaluated 233 insulin-na ve patients whose blood glucose levels were not adequately controlled with oral diabetes medications (A1C levels are 8%). In the 28-week, open-label, parallel-group study, patients were randomized to taking either twice daily NovoLog Mix 70/30 before breakfast and dinner or a single dose of insulin glargine at bedtime. The initial doses of 5 to 6 U of NovoLog Mix or 10 to 12 U of glargine were titrated to achieve blood glucose levels of 80 to 110 mg per dL. Both study arms received metformin, and 10% of subjects in each arm also received a constant dose of pioglitazone throughout the trial. At the end of 28 weeks, 66% or fewer of
P.242
patients taking NovoLog Mix 70/30 reached the currently recommended ADA target A1C levels of less than 7.0% compared with 40% taking insulin glargine. Indeed, 42% of individuals on NovoLog Mix 70/30 achieved an A1C of 6.5% or lower compared with 28% receiving glargine. In the study, hypoglycemic events were the most common side effect reported in both groups. Major hypoglycemic events were rare, with no major events reported in the NovoLog Mix 70/30 group and one observed in the insulin glargine group. Minor hypoglycemia (episodes per year) was greater with NovoLog Mix 70/30 compared with insulin glargine. Based on the results of this study, NovoLog Mix 70/30 appears to be more effective than insulin glargine as an initial regimen for insulin-na ve patients with poorly controlled (A1C >8.5%) T2DM.
(Coaching) Physiologic Insulin Replacement Therapy
Most patients with T1DM and poorly controlled individuals with T2DM should be placed on physiologic insulin replacement therapy designed to simulate endogenous insulin secretion in both the fasting and fed state. This may best be accomplished by designing a basal-bolus regimen administered via either multiple daily injections (or inhalations) or insulin pump. Physiologic insulin replacement therapy is a work in progress. Insulin doses are in constant flux. Although the initial insulin doses are prescribed by the healthcare provider, the patient is responsible for ultimately determining the timing, injection site, dose, and monitoring of their individual regimens.
Patients who are prescribed physiologic-intensive insulin replacement therapy must be willing to think and act like a pancreas. Although most intensively treated patients are highly motivated, the following requirements lay the foundation for successful physiologic insulin replacement self-management:
Patients must understand basic insulin pharmacokinetics and the appropriate timing and location of the insulin injection, the use of supplemental dose adjustments, and the effect of exercise and nutrition content of meals. The pharmacokinetics of insulin preparations are summarized in Table 5-8.
Blood glucose levels must be checked before meals, to provide the appropriate amount of insulin, and 2 to 3 hours after meals in case supplemental insulin is necessary. Patients should monitor glucose levels before driving and before and after exercising.
Once blood glucose levels are tested, patients must understand the significance of the readings and be able to make intelligent decisions on how to respond to those test results.
Patients must be prepared to react to hypoglycemia appropriately. More importantly, patients should be knowledgeable about strategies to prevent hypoglycemia.
Frequent visits to the healthcare provider are imperative. Adjustments in basal-bolus insulin doses are often necessary and are best determined by the treating physician. Patients who rarely see physicians tend to have deterioration in their ability to maintain targeted glycemic control. The office visits also allow the patient to be monitored for any short- or long-term diabetes-related complication.
Patients must have a strategy for managing sick days. Patients should be prepared to alter their insulin doses in response to a viral infection, in preparation for outpatient surgery or procedures, when placed on corticosteroids, or prior to undergoing elective surgeries.
Long-distance traveling may cause wide glycemic excursions. How does one adjust the insulin regimen while traveling across time zones? (See Chapter 9.)
Insulin pen devices, in which audible clicks correspond to the number of units to be injected, can be prescribed for patients with visual impairment or for those who prefer them to syringes and vials. The type of insulin contained within the Novo Nordisk pens can also be identified by the different tactile indentations located on the top of the pen. Patients with visual impairment can determine if they are handling a pen containing a basal insulin, a rapid-acting analogue, or a mixed insulin analogue.
Some pen injectors (NovoPen Jr) offer the option of providing 0.5-U dosing for patients who are highly insulin sensitive.
P.243
All-to-target Regimen
After being placed on basal insulin and titrating the dose to achieve FPG levels less than 100 mg per dL, a patient who is still unable to achieve a targeted A1C of lower than 7% may be a candidate for an all-to-target intensification regimen.93 Assuming that dinner is the largest meal of the day, have the patient begin using a rapid-acting insulin analogue 15 minutes before mealtime. The initial dose of the insulin should be 0.1 U per kg. The patient can adjust the dose of the insulin based on the size of the meal, as indicated below.
For very large meals, add 3 U.
For moderate-sized meals, add 1 to 2 U.
For smaller than average meals, subtract 1 to 2 U.
Thus, patients will be using, on average, 8 to 13 U of rapid-acting insulin at dinner. This will minimize glycemic excursions during the largest meal of the day and should help reduce the patient's A1C. If the A1C does not reach the target within 3 months, add a second injection using a similar dosing protocol for breakfast. A third injection may be added for lunch after 3 additional months if the patient's A1C remains elevated. The use of the third injection places the patient on a basal-bolus insulin regimen.
P.244
Case 7: Setting Up the Parameters for Physiologic Insulin Replacement Therapy
Jodie is a 22-year-old elementary school teacher who was diagnosed with T1DM diabetes at age 4. Over the past 5 years she has used two daily injections of NPH and regular (20/10 for breakfast and 10/5 for dinner). On her first visit, her blood glucose meter is downloaded. Only 22% of her blood glucose readings are in the acceptable range of 70 to 170 mg per dL. She is currently using on average 22 U of insulin daily. Her daily glycemic variation is significant and ranges from 40 to 380 mg within a 24-hour period. Over the past month, 18% of her glucose readings are less than 60 mg per dL, and she becomes aware of low blood glucose levels only when they drop below 40 mg per dL. Over the past 2 years, she has made four visits to the emergency department with severe hypoglycemia but was never hospitalized overnight. Although she had an uneventful full-term pregnancy at age 19, she recently experienced two consecutive spontaneous first-trimester miscarriages. Her gynecologist (OB/GYN) told her that she is unlikely to carry a pregnancy to term due to her poorly controlled diabetes. Jodie works out 5 days a week at a women's fitness center. She is taking no medicines other than insulin. At the time of her last doctor visit (3 months ago), she was told by the doctor to keep up the good work. Pertinent physical exam and laboratory results include the following:
BMI = 23 kg per m2
Weight = 55 kg
BP = 140/88 mm Hg
Serum creatinine = 1.4 mg per dL
24-Hour urine protein = 447 mg per dL (normal <30 mg per dL)
Glomerular filtration rate (GFR) = 50 mL per minute (chronic kidney disease Stage 3)
Total cholesterol = 220 mg per dL (target <200 mg per dL)
Triglycerides = 185 mg per dL (target <150 mg per dL)
HDL-C = 40 mg per dL (target <55 mg per dL)
Low-density lipoprotein cholesterol (LDL-C) = 122 mg per dL (target <100 mg per dL)
Non HDL-C = 180 mg per dL (target <130 mg per dL)
Thyroid studies = Normal
Liver panel = Normal
A1C = 11.2 % (target <7%)
Jodie is in desperate need of an intensified insulin regimen. She has developed some significant diabetes-related comorbidities, such as hypoglycemic unawareness, chronic kidney disease, hypertension, proteinuria, and a mixed hyperlipidemia. There is little doubt that the underlying common denominator
P.245
for Jodie's multiple comorbidities has been her poorly controlled diabetes. This may be the make or break opportunity to help Jodie prevent long-term complications such as heart disease, neuropathy, kidney failure, and retinopathy. Should she desire pregnancy, her preconception A1C should be targeted to a range between 6.5% and 7%. Every patient wants to be successful. A patient such as Jodie, who, as a teacher, is obviously very intelligent and motivated, will certainly become an active participant in her own care, should she be given the proper tools and education. As Jodie's new physician, you are about to change her life forever by encouraging her to be successful in every aspect of her diabetes self-management. Where do you start?
How much insulin does Jodie really require in a 24-hour period? That is, what is her total daily dose of insulin?
How much of the total daily dose is used as basal insulin?
How much of the total daily dose is used as prandial (mealtime) insulin?
How can Jodie adjust her prandial insulin dose based on her premeal blood glucose level?
How can Jodie adjust her prandial insulin dose based on her anticipated carbohydrate intake for a given meal?
Should Jodie eat immediately following the injection?
If Jodie's blood glucose is elevated at any time, how much supplemental insulin can she administer to get back into a safer range?
The first step in placing a patient on a physiologic basal-bolus regimen is to determine her TDD of insulin. Because the physiologic basal-bolus regimen is an ongoing project, patients must also know what percentage of their TDD is applied toward their basal or prandial insulin, their insulin sensitivity (insulin correction) factor, and their insulin-to-carbohydrate ratio. These formulas are all noted in Table 5-8. Although these formulas are useful in initiating a basal-bolus regimen, the actual doses of insulin are based on many other factors, including (a) the premeal glucose level; (b) anticipated activity level following the meal; (c) the time of day in which a meal is consumed; (d) the fat, carbohydrate, and caffeine components glycemic index of the meal; (e) the presence of diabetes-related complications such as gastroparesis; (f) if alcohol is consumed with a meal; and (g) a history of hypoglycemic unawareness.
Fasting (basal) glucose levels are maintained throughout the day in a very narrow range (70 to 95 mg per dL). Basal glucose serves as the obligate source of energy for the central nervous system. As basal glucose levels drop, the liver converts glycogen into glucose to prevent hypoglycemia. As a person eats and glucose levels rise, insulin release from the pancreatic beta cells is accelerated and the liver begins to store glycogen while reducing the release of glucose (Fig. 5-11). Patients with diabetes will need to adjust their preprandial insulin
P.246
P.247
doses based on these same principles. In general, higher doses of insulin are required before breakfast (to overcome insulin resistance) and for supper (due to the higher carbohydrate and fat content of evening meals).
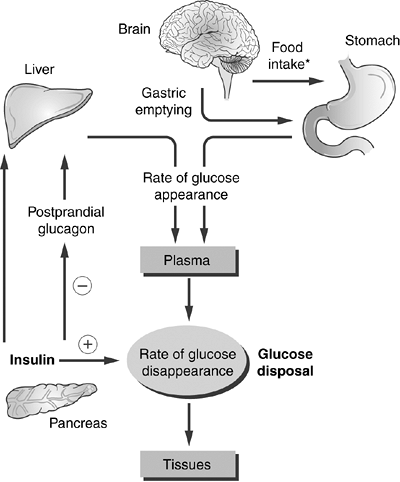 |
Figure 5-11 In the Fasting State, the Liver Converts Glycogen into Glucose, Which Is Released into the Portal Circulation to Prevent Hypoglycemia. Glycogenolysis is stimulated by the release of glucagon from the pancreatic alpha cells. Insulin produced by pancreatic beta cells blocks excessive glycogenolysis by preventing the release of glycogen. This interaction between insulin and the liver maintains basal glucose levels between 70 and 100 mg per dL. In the postprandial state, glucose is absorbed from the gastrointestinal tract. Endogenous plasma insulin levels increase in response to a meal. Insulin acts to induce glucose transportation across the cell membranes of skeletal muscles where the glucose is used as an energy source. Glycogenolysis is inhibited by the endogenous insulin. The brain uses plasma glucose as its obligate energy source and determines the quantity of food consumed during a meal. |
A number of methods may be used to help patients adjust their mealtime insulin doses. The simplest method is to provide a baseline dose of insulin for each meal that is equal to 0.1 U per kg. The patient can then adjust the dose of insulin as follows:
For very large meals, add 3 U.
For moderate-sized meals, add 1 to 2 U.
For smaller than average meals, subtract 1 to 2 U.
A second technique is to assign a baseline dose of insulin for each meal based simply on the size of the meal that the patient consumes. This technique might work best for shift-workers whose meal schedules and content are in a constant state of flux. The patient can add or subtract additional insulin based on the preprandial glucose level, as suggested in Table 5-18.
4 U insulin for small meals
6 U for average-sized meals
P.248
TABLE 5-18 Premeal Insulin Dose Adjustments Based on actual Blood Glucose Levels
Preprandial Glucose Level (mg/dL) Rapid-acting Insulin Dose Adjustment 40 -2 U; inject after finishing meal 41 80 -1 U 81 120 No change from baseline 121 160 +1 U 161 200 +2 U 201 240 +3 U 241 260 +4 U 261 280 +6 U 281 300 +8 U >300 Use insulin sensitivity factor (rule of 1,700). Correct to 150 mg/dL. Wait 1 h after injecting. Determine how much insulin remains to be absorbed. Count carbohydrates and dose accordingly. Example: A patient is instructed to administer 4 U of rapid-acting insulin before lunch. However, the actual dose of the insulin injected will be adjusted according to the preprandial glucose level. If the prelunch glucose is 221 mg/dL, the patient would use 4 + 3 = 7 U of insulin and inject within 10 to 15 minutes of eating. 10 U for large meals
2 U for snacks eaten 2 hours after a primary meal
Carbohydrate counting, in which 1 U of mealtime insulin is given for every 10 to 15 g of carbohydrates eaten, can also be used to approximate the dose of prandial insulin. However, patients must be forewarned that carb counting is effective at controlling postprandial glycemia only if the patient's general state of diabetes control is relatively stable. Patients with A1C levels greater than 8.5% should always strive to improve their fasting and postprandial glucose hyperglycemia before attempting to add carb counting to their treatment regimen.
Before eating, a patient will need to determine the preprandial glucose level and provide supplemental insulin if the levels are greater than 150 mg per dL or reduce the dose of insulin when less than 70 mg per dL (Table 5-18). This premeal dose adjustment is important, because if a patient eats while hyperglycemic, the glycemia will worsen quickly, resulting in a prolonged state of postprandial insulin resistance. If blood glucose levels are low prior to mealtime, the insulin dose is reduced and can be administered after finishing the meal.
Patients should check a 2- to 3-hour postprandial glucose level to determine if their best guess for prandial dosing of insulin was correct. If the 2- to 3-hour postprandial glucose is between 140 and 180 mg per dL, the patient knows that the correct dose of insulin was used for that particular meal. If the postprandial glucose level is lower than 70 mg per dL, too much insulin was dosed and the patient should be on alert for postprandial hypoglycemia. Frequent postprandial glucose determinations are helpful in allowing patients to develop dosing patterns that match the type and amount of food they often consume. For example, if a patient frequents a particular steak restaurant, with practice the patient knows that consuming a certain menu item will require 13 U of insulin added on to the necessary premeal correction factor.
Patients have been mistakenly taught to vary their injection sites throughout the body to prevent lipodystrophy at the injection site. However, human and analogue insulin preparations do not cause this disfiguring complication. Therefore, patients should be instructed to be consistent when choosing their injection sites. Rotating sites may increase intrasubject absorption variability, leading to unpredictable glycemic control.
Foods with a high glycemic index (e.g., white bread, potatoes, rice) necessitate higher doses of mealtime insulin than comparable portions of foods with a low glycemic index (e.g., peanut butter, dairy products, pasta, baked beans). Patients using basal-bolus insulin must be able to calculate the actual dose of insulin needed above the suggested baseline dose suggested by the physician (Fig. 5-12).
Ideally, Jodie's A1C should be in the range of 6.5% to 7% prior to attempting to become pregnant (see Chapter 8).
P.249
P.250
P.251
P.252
 |
Figure 5-12 Patient Information Sheet for Insulin Treatment Protocols. |
Jodie's physiologic insulin regimen based on her weight of 55 kg would be the following:
TDD
TDD: 55 kg 0.7 = 38.5 U (OK to round off to 40 U)
50% (20 U) applied to basal insulin either glargine or detemir given in AM or at bedtime (hs)
50% (20 U) applied to prandial insulin (rapid-acting insulin analogue or INH equivalent dose) as follows:
Breakfast: 7 U (This is her largest meal of the day.)
Lunch: 3 U (Jodie attends a yoga and Pilates class 5 days a week, 3 hours after lunch.)
Dinner: 6 U (Meal is typically high in protein. Patient is concerned about developing postexercise hypoglycemia.)
Insulin sensitivity (correction) factor
1,700/40 U = 42.5 (Round off to 40, meaning that 1 U of rapid-acting insulin analogue will reduce the baseline glucose level 40 mg per dL.) The target for glycemic correction for Jodie has been set at 150 mg per dL
Insulin-to-carbohydrate ratio
500/40 = 12.5 (Round off to 12, meaning that 1 U of rapid-acting insulin analogue will cover 12 g of carbohydrates.) When consuming 36 g of carbohydrates, she will require 3 U of insulin.
Lag times:
The lag time represents the approximate time a patient should delay beginning to eat a meal once the insulin is injected. General lag time rules are as follows:
| Preprandial Glucose Level (mg/dL) | Lag Time (min) |
|---|---|
| 70 | 0 |
| 71 150 | 15 |
| 151 240 | 30 |
| >241 | 45 60 |
Physiologic (basal-bolus insulin regimens) may not be appropriate for the following individuals:
Children younger than age 13 (due to the higher risk of hyperglycemia)
Elderly patients who live alone especially those with hypoglycemic unawareness
Patients with a history of stroke or cardiovascular disease in whom hypoglycemia may increase the likelihood of inducing a secondary event
Patients who are unwilling or unable to perform home blood glucose monitoring
Patients with limited financial means to cover the additional costs of multiple daily insulin injections and home blood glucose monitoring
P.253
Case 8: Preventing Recurring Hypoglycemia
Mrs. Simpson is 62 years old and has been using insulin for the past 20 years. Her A1C is 5.2% and she has no known diabetes-related long-term complications. However, she has three emergency department visits in the past year due to severe hypoglycemia. Although she has an emergency glucagon kit at home, her husband is afraid to give her the injection and prefers to call 911 whenever she passes out. Mrs. Simpson admits that she is obsessive-compulsive about managing her diabetes and does her best to maintain her blood glucose levels less than 100 mg per dL fasting and less than 140 mg per dL after meals. She tests her blood glucose levels up to eight times a day, often in the middle of the night. A review of last month's home monitoring downloads demonstrate that 25% of her glucose levels are less than 60 mg per dL. Mrs. Simpson was asked the following questions, and her answers are supplied:
At what glucose levels do you feel lows? to which she replied, less than 40 mg per dL.
How do you manage postprandial hyperglycemia? Her reply: Using my insulin sensitivity factor I will give a supplemental injection of insulin 2 hours after eating in order to get the sugar down below 150 mg per dL.
After giving the supplemental insulin injection, when do you recheck the blood glucose level? She said: Just prior to the next meal when I'm supposed to give another injection. Oh, but I also count my carbohydrates before I shoot!
A major cause of hypoglycemia is insulin stacking (Fig. 5-3). After rapid-acting insulin is injected subcutaneously, a depot is formed in the skin from which insulin continues to be absorbed for up to 6 hours. During this time, the amount of insulin that remains in the depot acting to reduce blood glucose levels can be calculated. For example, if a patient injects 10 U of a rapid-acting analogue at time 0 60% of the original 10 U (6 U) remains to be absorbed in that depot at time plus 2 hours. At time plus 4 hours, 1 U remains within the depot. The insulin within the depot will continue to lower plasma glucose levels for up to 6 hours after the original injection is performed. Patients who reinject another dose of insulin within 6 hours of the original injection establish yet another depot from which insulin will be absorbed. The insulin actions of both depots work additively to lower glucose levels. Injecting insulin before the prior insulin injection has been completely absorbed is known as insulin stacking.
As an example, Mrs. Simpson checks her blood glucose level 2 hours after eating breakfast at a local pancake house. She interprets the reading of 260 mg per dL as being too high. Her insulin sensitivity factor was calculated to suggest that 1 U of rapid-acting insulin lowers her glucose level by 25 mg per dL. Believing her targeted postprandial glucose level is less than 140 mg per dL, she injects 5 U of supplemental insulin. At noon, her prelunch glucose level is 110 mg per dL. She is going to eat a meal consisting of 80 g of carbohydrates. With
P.254
her insulin-to-carbohydrate ratio being 1:10, she decides to inject 8 U of rapid-acting insulin as she begins to eat. Two hours after eating she develops profuse sweating, confusion, and blurred vision and eventually loses consciousness. On her arrival in the emergency room, her plasma glucose level is 32 mg per dL. Mrs. Simpson stacked her insulin.
Two hours after giving supplemental insulin, she had 60% of her original 5 U remaining to be absorbed. By injecting an additional 8 U to cover her carbohydrate intake for lunch, she has really formed two separate insulin depots, with a combined total of 11 U of rapid-acting insulin. Had Mrs. Simpson been informed about insulin stacking, she would have subtracted 3 U from the 8 U she intended to provide to cover the lunch meal and checked her blood glucose level again 2 hours after eating to make certain she was not entering into a hypoglycemic state. In addition, the target for correction using supplemental insulin is 150 mg per dL to avoid iatrogenic hypoglycemia.
The frequency of hypoglycemia can be significantly reduced when patients are informed about insulin stacking. This is especially important for patients who have hypoglycemic unawareness and are unable to feel the symptoms of hypoglycemia before losing consciousness.
Case 9: Managing Severe Insulin Resistance
Fifty-six-year-old Rita has had diabetes for 12 years. Originally placed on oral agents, her last physician switched her to an intensive insulin therapy regimen 8 months ago. She is currently taking 45 U of lispro with each meal and 100 U of glargine at bedtime. Her most recent A1C is 9.8%. Her electronic home blood glucose download records show that she checks her blood glucose levels at least four times a day. Her average fasting blood glucose reading over the past 30 days is 275 mg per dL, and postprandial levels average 350 mg per dL. Her standard deviation is 45, and her mean blood glucose level is 265 mg per dL, indicating the presence of severe insulin resistance. Rita remains symptomatic, complaining of chronic fatigue, repeated vaginal infections, and paresthesias in her hands and feet. She weighs 100 kg and has a BMI of 38 kg per m2. After attending many courses on diabetes management, attempting pool exercise therapy, and meeting with registered dietitians and CDEs, Rita has all but given up her desire to improve her diabetes control. Her diabetes-related comorbidities include hypertension, depression, proteinuria, type 2B hyperlipidemia, mild sensory peripheral neuropathy, and nonproliferative retinopathy. Her thyroid studies and serum cortisol levels are normal. None of her routine medications were thought to be responsible for exacerbating her insulin resistance.
What can be done to further intensify Rita's diabetes management, allowing her to attain a safer level of glycemic control?
P.255
Insulin resistance is a serious therapeutic dilemma despite advances in oral agents and the introduction of insulin analogues. A normoglycemic individual consuming a standard diet secretes approximately 45 U per 24 hours, including 10 U for breakfast, 13 U for lunch, 14 U for dinner, and 8 basal U to suppress hepatic glucose production in the fasting state. At least 50% of the endogenous insulin released by the pancreas is extracted by the liver during the initial trans-hepatic passage so that the total peripheral delivery of insulin is approximately 22 U per day.97 Insulin resistance occurs when the hormone's action to lower blood glucose levels is severely impaired. In order for insulin action to occur, insulin must bind with receptors on the cell surfaces of skeletal muscles and adipose tissue. If insulin receptors are downregulated or absent, cells become unresponsive to insulin action. In response to prolonged and persistent hyperglycemia, the pancreas will produce an excessive amount of insulin in an attempt to restore ambient glucose levels to normal. However, the high levels of circulating endogenous insulin results in downregulation of insulin receptors and impairment of insulin action. Inflammatory cytokines may inhibit the expression of peroxisome proliferator-activated receptor (PPAR) genes leading to a state of insulin resistance.98 Some individuals may be insulin resistant despite having normal numbers of insulin receptors on their cell surfaces.99 Thus, the exact pathophysiology of insulin resistance is uncertain.
Patients in whom glycemic control deteriorates despite using more than 150 U of exogenous insulin daily are considered to be insulin resistant. As a result of having prolonged and significant hyperglycemia, these patients are symptomatic and frustrated over the lack of efficacy of different treatment protocols. One treatment option for treating insulin resistance is the use of human regular U-500 insulin. U-500 is five times more concentrated (500 U per mL) than the standard U-100 insulin (100 U per mL). Because U-500 insulin is highly concentrated, lower volumes of the drug can be injected, resulting in a smaller and more efficiently absorbed insulin depot. A patient who normally injects 50 U of U-100 prior to a meal needs to administer only 10 U of U-500.
A study by Neal100 showed that 20 insulin-resistant patients who were converted to U-500 insulin were able to lower their A1C from baseline (9.6%) by 1.1% over 3 to 6 months. The actual TDD of insulin did change significantly over the course of the 6-month trial. There was no reported significant hypoglycemia in any of the patients.
Knee et al.101 described a series of four patients treated with U-500 insulin by means of insulin pump therapy. Three months after conversion to U-500 therapy, the average A1C decreased from 10.8% to 7.6%, and within 6 months the average A1C was 7.3%. With use of U-500, the absolute volume of pumped insulin infused per day decreased by at least fourfold, leading to a cost savings for insulin of up to $2,600 per year, while the cost of pump supplies was reduced by up to $3,400 annually. All patients had subjective improvement in quality of life.
P.256
The mechanism of greater efficacy of U-500 insulin over U-100 insulin at equivalent doses is uncertain. When using U-500 insulin, patients should be instructed as follows:
A predetermined dose of U-500 is given prior to each meal. The dose of the insulin should not normally be adjusted to compensate for preprandial hyperglycemia.
If preprandial glucose levels are less than 70 mg per dL, one should inject the U-500 dose after eating.
U-500 insulin has a slower onset of action (60 minutes) when compared with U-100 rapid-acting insulin analogues. Therefore, after injecting one should delay eating for at least 45 to 60 minutes. Duration of action of U-500 is 4 to 6 hours.
U-500 insulin is used as prandial insulin only. Glargine or detemir should be administered as a basal insulin in conjunction with U-500.
Low-volume insulin syringes should be used for U-500 insulin injections. Dosing U-500 may be more difficult using 100-U syringes versus 30-U syringes.
Weight gain can be expected with U-500 insulin. However, improvement in A1C is usually apparent within 3 months. The risks of moderate weight gain appear to be less than the resulting effects of prolonged and uncontrolled hyperglycemia.
Patients tend to more energetic on U-500 when compared with using high-volume U-100 insulin.
Patients should be warned that many clinicians, nursing personnel, and pharmacists may be unfamiliar with U-500 insulin. Dosing errors may occur if someone other than the patient administers the insulin. For example, a patient receiving 10 U of U-500 insulin may develop severe hyperglycemia if given only 10 U of U-100.
U-500 insulin often must be special ordered by pharmacies. The physician should make certain the patient's pharmacy remains stocked with U-500 so that refills can be easily obtained.
Patients should be instructed on how to properly use a glucagon emergency kit for severe hypoglycemia. Glucagon kits should be kept at home and in the workplace.
For Rita, the U-500 insulin treatment regimen could be initiated as shown in the following table.
P.257
| Timing of Insulin Dose | Insulin Dose (units) | Site of Injection | Target Blood Glucose Level (mg/dL) |
|---|---|---|---|
| 4560 min before breakfast | 10 U-500 | Abdomen | 2- to 3-h postprandial <180 |
| 4560 min before lunch | 9 U-500 | Arm/abdomen | 2- to 3-h postprandial <180 |
| 4560 min before dinner | 11 U-500 | Arm/abdomen | 2- to 3-h postprandial <180 |
| 10 PM daily | 80 U glargine | Leg/arm | <100 fasting |
The injection of U-500 should be given in the abdomen before breakfast because insulin depots are absorbed fastest from the abdomen. Absorption from the arm is faster than from the leg. Glargine insulin absorption occurs regardless of the injection site. The doses of insulin can be altered based on the patient's ability to attain the targeted blood glucose levels. Three months after starting A1C therapy, an A1C should be repeated to determine if the patient is moving toward her selected target.
Case 10: Combining Insulin with Exenatide
Mrs. Woeckener, 61 years old, has a 24-year history of T1DM. Over the years, Mrs. W has been somewhat lax in her willingness to adhere to the treatment regimens as prescribed by her various physicians. As a result, she has developed multiple serious complications including the following:
Diabetic peripheral neuropathic pain
Autonomic neuropathy with gastroparesis, postural hypotension, and nocturnal diarrhea
Proliferative retinopathy effecting her vision
Chronic kidney disease stage 4 with a GFR = 28 mL per minute and a hemoglobin = 9.9 g
Coronary artery disease requiring the placement of two stents
Mrs. W had such severe insulin resistance that she showed little improvement in glycemic control using U-500 insulin 75 U daily in an insulin pump (the equivalent of 375 U of U-100 insulin). Her A1C was 12.2%. Her blood glucose meter download (Fig. 5-13A) shows that 90% of her blood glucose readings are higher than 170 mg per dL.
In a desperate attempt to improve the patient's glycemic control, she was placed on exenatide 5 g twice a day and showed immediate improvement in her blood glucose levels (Fig. 5-13B). She has had no episodes of hypoglycemia on combination therapy using exenatide 10 g daily. Her pre-exenatide and post-exenatide treatment parameters are shown in the following table.
| Parameter | June 26 | October 30 |
|---|---|---|
| A1C | 12.2% | 7.5% |
| Total daily dose of insulin | 375 U | 170 U |
| Average fasting glucose | 284 mg/dL | 162 mg/dL |
| Average 2-h postprandial glucose (dinner) | 375 mg/dL | 165 mg/dL |
| Weight | 95.4 kg | 90.1 kg |
Recently, I have had outstanding success combining U-500 insulin with twice- daily injections of exenatide. Although exenatide is not indicated for use in combination with insulin, many clinicians feel that certain patients may achieve
P.258
improved glycemic control, in association with weight loss in severely insulin-resistant patients.
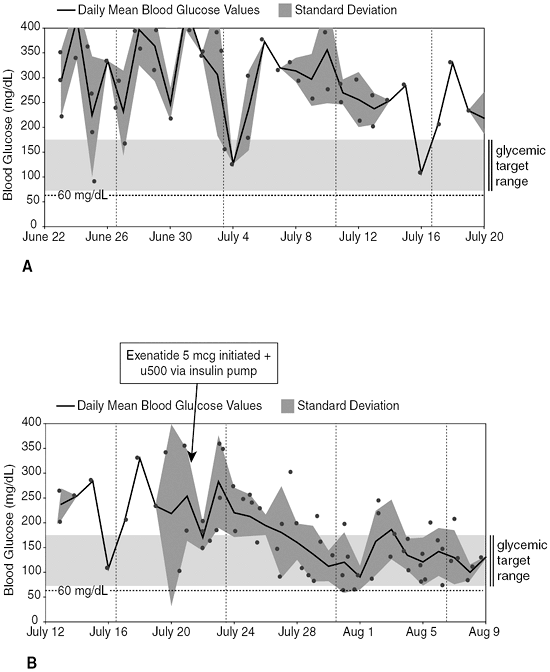 |
Figure 5-13 Mrs. W's Glucose Meter Download. A: Blood glucose meter download showing insulin resistance. B: Glucose meter download after starting therapy with exenatide 5 g twice a day. |
Patients who have erratic glycemic control may be stabilized with the use of pramlintide (see Chapter 12). Pramlintide's efficacy is based on the drug's ability to reduce postprandial glucose levels while improving gastric emptying and satiety.
P.259
Summary
Multiple treatment regimens can be considered when managing insulin-requiring diabetes.
Treatment regimen should be individualized although the ultimate goal is to target the lowest and safest A1C possible.
Using a treat-to-target protocol, patients with T2DM can rapidly have their insulin doses titrated to an A1C less than 7%.
Patients with T1DM should be placed on basal-bolus insulin therapy to approximate the normal physiologic first- and second-phase insulin response to basal and prandial glucose excursions. Dosing formulas are very helpful when implementing physiologic insulin replacement therapy.
Insulin stacking is a major cause of hypoglycemia. Once recognized, the frequency and severity of hypoglycemia can be significantly reduced.
Pulmonary insulin can be useful for patients with T1DM and T2DM.
In general, patients with A1C less than 8.3% should first attempt to improve postprandial glucose excursions, whereas patients with A1C greater than 8.5% should focus on improving fasting glucose levels.
Patients with suboptimal glycemic control who use more than 150 U of insulin per day may be candidates for preprandial concentrated U-500 insulin in conjunction with basal insulin.
For patients with T2DM who are unable to achieve ADA (<7%) or AACE ( 6.5%) targeted A1C goals the following initial treatment options are recommended.
| A1C Level | Recommended Initial Insulin Treatment Protocol |
|---|---|
| >8.5% |
|
| <8.5% |
|
Table 5-18 and Figure 5-12 provide patients with written instructions for their individual insulin regimens.
References
1. Bliss M. The Discovery of Insulin. Chicago: University of Chicago Press;1984:11 20.
2. The first clinical use of insulin. Diabetes. 1956;5:65 67.
3. Joslin EP. A diabetic manual for the mutual use of doctor and patient. 7th ed. Philadelphia: Lea & Febiger;1941.
4. Kumar O, Miller L, Mehtalia S. Use of dexamethasone in treatment of insulin lipoatrophy. Diabetes. 1977;26:296 299.
5. Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977 986.
P.260
6. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837 853.
7. Bruno G, Runzo C, Cavallo-Perin P, et al. Incidence of type 1 and type 2 diabetes in adults aged 30 49 years: the population-based registry in the province of Turin, Italy. Diabetes Care. 2005;28:2613 2619.
8. Seyfert-Margolis V, Gisler TD, Asare AL. Analysis of T-cell assays to measure autoimmune responses in subjects with type 1 diabetes. Diabetes. 2006;55:2588 2594.
9. Han X, Sun Y, Scott S, Bleich D. Tissue inhibitor of metalloproteinase-1 prevents cytokine-mediated dysfunction and cytotoxicity in pancreatic islets and beta-cells. Diabetes. 2001;50:1047 55.
10. Greenbaum CJ, Brooks-Worrell BM, Palmer JP, et al. Autoimmunity and prediction of insulin dependent diabetes mellitus. In: Marshall SM, Home PD, eds. The Diabetes Annual/8. Elsevier;1994:18 35.
11. Hoppu S, Ronkainen MS, Kimpimaki T, et al. Insulin autoantibody isotypes during the prediabetic process in young children with increased genetic risk of type 1 diabetes. Pediatr Res. 2004;55:236 242.
12. Juneja R, Palmer JP. Type 1 diabetes: myth or reality? Autoimmunity. 1999;29:65 83.
13. Borg H, Gottsater A, Fernlund P, et al. A 12-year prospective study of the relationship between islet antibodies and beta-cell function at and after the diagnosis in patients with adult-onset diabetes. Diabetes. 2002;51:1754 1762.
14. Hathout EH, Thomas W, El-Shahawy M, et al. Diabetic autoimmune markers in children and adolescents with type 2 diabetes. Pediatrics. 2001;107:E102.
15. Juneja R, Hirsch IB, Naik RG, et al. Islet cell antibodies and glutamic acid decarbosylase antibodies, but not the clinical phenotype, help to identify type 1 ( ) diabetes in patients presenting with type 2 diabetes. Metabolism. 2001;50:1008 1013.
16. Harris MI, Flegal KM, Cowie CC, et al. Prevalence of diabetes, impaired fasting glucose, and impaired glucose tolerance in U.S. adults: the Third National Health and Nutrition Examination Survey, 1988 1994. Diabetes Care. 1998;21:518 524.
17. Ohkubo Y, Kishikawa H, Araki E, et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes: a randomized prospective 6-year study. Diabetes Res Clin Pract. 1995;28:103 117.
18. American Diabetes Association. Standards of medical care for patients with diabetes mellitus (Position Statement). Diabetes Care. 2002;25:S33-S49.
19. The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Retinopathy and nephropathy in patients with type 1 diabetes four years after a trial of intensive therapy. N Engl J Med. 2000;342:381 389.
20. The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Group. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353;25. 2643 2653.
21. Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Intensive diabetes therapy and carotid intima-media thickness in type 1 diabetes mellitus. N Engl J Med. 2003;348:2294 2903.
22. Cleary P, Orchard T, Zinman B, et al. Coronary calcification in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) cohort. Diabetes. 2003;52(Suppl 2):A152-A152.
23. Writing Team for the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Sustained effect of intensive treatment of type 1 diabetes mellitus on development and progression of diabetic nephropathy: the Epidemiology of Diabetes Interventions and Complications (EDIC) study. JAMA. 2003;290: 2159 2167.
24. Genuth S. Insights from the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study on the use of intensive glycemic treatment to reduce the risk of complications of type 1 diabetes. Endocr Pract. 2006;12(Suppl 1): 34 41.
P.261
25. ACE/AACE Diabetes Recommendations Implementation Conference. Road Map For The Prevention and Treatment of Type Two Diabetes. Available at: http://www.aace.com/ meetings/consensus/odimplementation/roadmap.pdf#search=%22AACE%20Roadmap%22. Accessed August 28, 2006.
26. ACE/AACE consensus conference on the implementation of outpatient management of diabetes mellitus: consensus conference recommendations. Endocr Pract. 2006;12(Suppl 1):6 12.
27. Barnett AH, Dreyer M, Lange P, et al. An open, randomized, parallel-group study to compare the efficacy and safety profile of inhaled human insulin (Exubera) with glibenclamide as adjunctive therapy in patients with type 2 diabetes poorly controlled on metformin. Diabetes Care. 2006;29:1818 1825.
27a. Nadeau D. Clinical use of exenatide: the first of a new class of incretin mimetics. Diabetes Consult Collection, pp. 5 7, April 2006.
27b. Villa-Caballero L, Edelman SV. Clinical effects of incretin mimetic and amylin analog hormones. Diabetes Consult Collection, pp. 7 9, April 2006.
28. Hermansen K, Davies M, Derezinski T, et al. A 26-week, randomized, parallel, treat-to-target trial comparing insulin detemir with NPH insulin as add-on therapy to oral glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetes Care. 2006;29:1269 1274.
29. Riddle MC, Rosenstock J, Gerich J; Insulin Glargine 4002 Study Investigators. The treat-to-target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care. 2003;26: 3080 3086.
30. Jain R. Efficacy of biphasic insulin Aspart 70/30 in patients with T2DM not achieving glycemic targets on OADs with/without basal insulin therapy. Oral Presentation 278-OR, presented at the 65th annual meeting of the American Diabetes Association, June 12, 2005, San Diego, Ca.
31. Garber AJ, Wahlen J, Wahl T, et al. Attainment of glycaemic goals in type 2 diabetes with once-, twice-, or thrice-daily dosing with biphasic insulin aspart 70/30 (The 1 2 3 study). Diabetes Obesity Metab. 2006;8:58 66.
32. Raskin P, Allen E, Hollander P, et al.; INITIATE Study Group. Initiating insulin therapy in type 2 diabetes. A comparison of biphasic and basal insulin analogues. Diabetes Care. 2005; 28:260 265.
33. American Diabetes Association. Economic costs of diabetes in the U.S. in 2002. Diabetes Care. 2003;26:917 932.
34. Gilmer TP, O'Connor PJ, Manning WG, Rush WA. The cost to health plans of poor glycemic control. Diabetes Care. 1997;20:1847 1853.
35. The Diabetes Control and Complications Trial Research Group. Lifetime benefits and costs of intensive therapy as practices in the DCCT. JAMA. 1996;276:1409 1415.
36. www.drugstore.com. Accessed March 10, 2006.
37. UKPDS 16. Overview of six years' therapy of type 2 diabetes-a progressive disease. UKPDS Study Group. Diabetes. 1995;44:1249 1258.
38. Koro CE, Bourgeois N, Bowlin SJ, Fedder DO. Glycemic control from 1988 to 2000 among US adults diagnosed with type 2 diabetes. Diabetes Care. 2004;27:17 20.
38a. Brown JB, Nichols GA, Perry A. The burden of treatment failure in type 2 diabetes. Diabetes Care. 2004;27:1535 1540.
39. Rickheim PL, Weaver TW, Fladder JL, et al. Assessment of group versus individual diabetes education: a randomized study. Diabetes Care. 2002;25:269 274.
40. Sommerfield AJ, Deary IJ, Frier BM. Acute hyperglycemia alters mood state and impairs cognitive performance in people with type 2 diabetes. Diabetes Care. 2004;27:2335 2340.
41. Cramer JA. A systematic review of adherence with medications for diabetes. Diabetes Care. 2004;27:1218 1224.
42. Anderson RT, Marrero D, Skovlund SE, Cramer J, Schwartz S. Self-reported compliance with insulin injection therapy in subjects with type 1 and 2 diabetes [abstract]. Diabetes Metab. 2003;29:A275.
43. Polonsky WH, Anderson BJ, Lohrer PA, Aponte JE, Jacobson AM, Cole CF. Insulin omission in women with IDDM. Diabetes Care. 1994;17:1178 1185.
P.262
44. Weissberg-Benchell J, Glasgow AM, Tynan WD, Wirtz P, Turek J, Ward J. Adolescent diabetes management and mis-management. Diabetes Care. 1995;18:77 82.
45. Balkrishnan R, Rajagopalan R, Camacho FT, Hyuston SA, Murray FT, Anderson RT. Predictors of medication adherence and associated health care costs in an older population with type 2 diabetes mellitus: a longitudinal cohort study. Clin Ther. 2003;25:2958 2971.
46. Hornquist JO, Wikby A, Andersson PO, Dufva AM. Insulin-pen treatment, quality of life and metabolic control: retrospective intra-group evaluations. Diabetes Res Clin Pract. 1990;10: 221 230.
47. Graff MR, McClanahan MA. Assessment by patients with diabetes mellitus of two insulin pen delivery systems versus a vial and syringe. Clin Ther. 1998;20:486 496.
48. Cryer PE. Hypoglycemia: Pathophysiology, Diagnosis, and Treatment. New York: Oxford University Press; 1997.
49. Donnelly LA, Morris AD, Frier BM, Ellis JD, Donnan PT, Durrant R, et al. Frequency and predictors of hypoglycaemia in type 1 and insulin-treated type 2 diabetes: a population-based study. Diabet Med.2005;22:749 755.
50. Cryer PE. Current concepts: Diverse causes of hypoglycemia-associated autonomic failure in diabetes. N Engl J Med. 2004;350:2272 2279.
51. Diedrich L, Sandoval D, Davis SN. Hypoglycemia associated autonomic failure. Clin Auton Res. 2002;12:358 365.
52. Zammitt NN, Frier BM. Hypoglycemia in type 2 diabetes. Diabetes Care.2005;28:2948 2961.
53. Cryer PE. Hypoglycemia risk reduction in type 1 diabetes. Exp Clin Endocrinol Diabetes. 2001;109:S412 S423.
54. Davis SN, Tate D. Effects of morning hypoglycemia on neuroendocrine and metabolic responses to subsequent afternoon hypoglycemia in normal man. J Clin Endocrinol Metab. 2001;86:2043 2050.
55. Dagogo-Jack SE, Craft S, Cryer PE. Hypoglycemia-associated autonomic failure in insulin-dependent diabetes mellitus. J Clin Invest. 1993;91:819 828.
56. Segel SA, Paramore DS, Cryer PE. Hypoglycemia-associated autonomic failure in advanced type 2 diabetes. Diabetes. 2002;51:724 732.
57. Wright EE. Treat to target: ABCs for the elderly. DOC News.2006;3:4.
58. Heller SR, Amiel SA, Mansell P. Effect of the fast-acting insulin analog lispro on the risk of nocturnal hypoglycemia during intensified insulin therapy. Diabetes Care. 1999;22:1607 1611.
59. Ratner RE, Hirsch IB, Neifing JL, Garg SK, Mecca TE, Wilson CA. Less hypoglycemia with insulin glargine in intensive insulin therapy for type 1 diabetes. Diabetes Care. 2000;23:639 643.
60. Unger J, Marcus A. Insulin pump therapy: what you need to know. Emerg Med. 2002;34:P24 33.
61. Hirsch IB. Insulin analogues. N Engl J Med. 2005;352:174 183.
62. Kruszynska YT, Home PD, Hanning I, et al. Basal and 24-h C-peptide and insulin secretion rate in normal man. Diabetologia. 1987;30:16 21.
63. Home PD, Lindholm A, Hylleberg B, Round P. Improved glycemic control with insulin aspart: a multicenter randomized double-blind crossover trial in type 1 diabetic patients. Diabetes Care. 1998;21:1904 1909.
64. Gale EA. A randomized, controlled trial comparing insulin lispro with human soluble insulin in patients with Type 1 diabetes on intensified insulin therapy. Diabet Med. 2000;17:209 214.
65. Renner R, Pfutzner A, Trautmann M, Harzer O, Sauter K, Landgraf R. Use of insulin lispro in continuous subcutaneous insulin infusion treatment: results of a multicenter trial. Diabetes Care. 1999;22:784 788.
66. Bolli GB. Insulin treatment in type 1 diabetes. Endocr Pract. 2006;12(Suppl 1):105 109.
67. Rossetti P, Pampanelli S, Fanelli C, et al. Intensive replacement of basal insulin in patients with type 1 diabetes given rapid-acting insulin analog at mealtime: a 3-month comparison between administration of NPH insulin four times daily and glargine insulin at dinner or bedtime. Diabetes Care. 2003;26:1490 1496.
P.263
68. Goldman-Levine JD, Lee KW. Insulin Detemir a new basal insulin analogue. Ann Pharmacother. 2005;393:502 507.
69. Vague P, Selam JL, Svein S, et al. Insulin detemir is associated with more predictable glycemic control and reduced risk of hypoglycemia than NPH insulin in patients with type 1 diabetes on basal-bolus regimen with premeal insulin aspart. Diabetes Care. 2003;26:590 596.
70. Heise T, Nosek L, Biilmann R nn B, et al. Lower within-subject variability of insulin detemir in comparison to NPH insulin and insulin glargine in people with type 1 diabetes. Diabetes. 2004;53:1614 1620.
71. Unger J. Intensive insulin management of type 1 diabetes in the female patient. Female Patient. 1999;24:35 42.
72. Acerini CL, Cheetham TD, Edge JA, Dunger DB. Both insulin sensitivity and insulin clearance in children and young adults with type I (insulin-dependent) diabetes vary with growth hormone concentrations and with age. Diabetologia. 2000;43:61 68.
73. Mohn A, Strang S, Wernicke-Panten K, Lang AM, Edge JA, Dunger DB. Nocturnal glucose control and free insulin levels in children with type 1 diabetes by use of the long-acting insulin HOE 901 as part of a three-injection regimen. Diabetes Care. 2000;23:557 559.
74. McSorley PT, Bell PM, Jacobsen LV, et al. Twice-daily biphasic insulin aspart 30 versus biphasic human insulin 30: a double-blind crossover study in adults with type 2 diabetes mellitus. Clin Ther. 2002;24:530 539.
75. Davidson J, Vexiau P, Cucinotta D, et al. Biphasic insulin aspart 30: literature review of adverse events associated with treatment. Clin Ther. 2005;27(Suppl B):S75 S88.
76. Shah BR, Hux JE, Laupacis A, Zinman B, van Walraven C. Clinical inertia in response to inadequate glycemic control. Diabetes Care. 2005;28:600 606.
77. Brown JB, Nichols GA. Slow response to loss of glycemic control in type 2 diabetes mellitus. Am J Manag Care. 2003;9:213 217.
78. Scherbaum WA. Unlocking the opportunity of tight glycaemic control. Inhaled insulin: clinical efficacy. Diabetes Obesity Metab. 2005;7(Suppl 1):S9-S13.
79. Skyler JS, Cefalu WT, Kourides IA, Landschuz WH, Balagtas CC, Cheng S-L. Efficacy of inhaled human insulin in type 1 diabetes: a randomized proof-of-concept study. Lancet. 2001;357:331 335.
80. Cefalu WT, Skyler JS, Kourides IA, Landschulz WH, Balagtas CC, Cheng S-L. Inhaled human insulin treatment in patients with type 2 diabetes. Ann Intern Med. 2001;134:203 207.
81. Weiss SR, Cheng S-L, Kourides IA, Gelfand RA, Landschulz WH. Inhaled insulin improved glycemic control in patients with type 2 diabetes mellitus inadequately controlled with oral agents: a randomized controlled trial. Arch Intern Med. 2003;163:2277 2282.
82. Hollander PA, Blonde L, Rowe R, et al. Efficacy and safety of inhaled insulin (Exubera) compared with subcutaneous insulin therapy in patients with type 2 diabetes results of a 6-month, randomized, comparative trial. Diabetes Care. 2004;27:2356 2362.
83. Quattrin T, Belanger A, Bohannon NJV, Schwartz SL. Efficacy and safety of inhaled insulin (Exubera) compared with subcutaneous insulin therapy in patients with type 1 diabetes. Diabetes Care. 2004;27:2622 2627.
84. Rosenstock J, Cappelleri JC, Bolinder B, Gerber RA. Patient satisfaction and glycemic control after 1 year with inhaled insulin (Exubera) in patients with type 1 or type 2 diabetes. Diabetes Care. 2004;27:1318 1323.
85. DeFronzo RA, Bergenstal RM, Cefalu WT, et al. Efficacy of inhaled insulin in patients with type 2 diabetes not controlled with diet and exercise. A 12-week, randomized, comparative trial. Diabetes Care. 2005;28:1922 1928.
86. Skylar J. Sustained long-term efficacy and safety of inhaled insulin during 4 years of continuous therapy [abstract]. Diabetes. 2004;53(Suppl 2):A115.
86a. Dreyer M. Efficacy and 2-year pulmonary safety of inhaled insulin as adjunctive therapy with metformin or glibenclaminde in type 2 diabetes poorly controlled with oral monotherapy. Diabetologia. 2004;47(suppl 1):A44.
87. Henry RR, Mudaliar RR, Chu N, et al. Inhaled insulin in young and elderly type 2 diabetic patients using the AERx insulin diabetes management system: a pharmacokinetic and pharmacodynamic study [abstract]. EASD. 2002;38:A812.
P.264
88. Himmelman A, Jendle J, Mellen A, Petersen AH, Dahl UL, Wollmer P. The impact of smoking on inhaled insulin. Diabetes Care. 2003;26:677 682.
89. Fineberg SE, Kawabata T, Finco-Kent D, et al. Antibody response to inhaled insulin in patients with type 1 or type 2 diabetes. An analysis of initial phase II and III inhaled insulin (Exubera) trials and a two-year extension trial. J Clin Endocrinol Metab. 2005;90:3287 3294.
90. Stratton IM, Adler AI, Neil HAW, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321:405 412.
91. Monnier L, Lapinski H, Colette C. Contributions of fasting and postprandial plasma increments to the overall diurnal hyperglycemia of type 2 diabetic patients. Variations with increasing levels of A1C. Diabetes Care. 2003;26:881 885.
92. Unger J. Targeting glycemic control in the primary care setting. Female Patient. 2003;28: 12 16.
93. Riddle MC. Making the transition from oral to insulin therapy. Am J Med. 2005;118:14S-20S.
94. Rubin RR, Peyrot M. Quality of life, treatment satisfaction, and treatment preference associated with use of a pen device delivering a premixed 70/30 insulin aspart suspension (aspart protamine suspension/soluble aspart) versus alternative treatment strategies. Diabetes Care. 2004;27:2495 2497.
95. Liebel A, Prager R, Kaiser M, et al. Biphasic insulin aspart 30 (BIAsp 30), insulin detemir (IDet) and insulin aspart (IASP) allow patients with type 2 diabetes to reach A1C target: the PREFER study [abstract]. Diabetes. 2006;55(suppl 1):517.
96. Malone JK, Kerr LF, Campaigne BN, et al. Combined therapy with insulin lispro mix 75/25 plus metformin or insulin glargine plus metformin: a 16 week, randomized, open label, crossover study in patients with type 2 diabetes beginning insulin therapy. Clin Ther. 2005;26:2034 2044.
97. Eaton RP, Allen RC, Schade DS, Standefer JC. Normal insulin secretion: the goal of artificial insulin delivery systems? Diabetes Care. 1980;3:270 273.
98. Tanaka T, Itoh H, Doi K, et al. Down regulation of peroxisome proliferator-activated receptor gamma expression by inflammatory cytokines and its reversal by thiazolidinediones. Diabetologia. 1999;42:702 710.
99. Caro JF, Amatruda JM. Glucocorticoid-induced insulin resistance. The importance of postbinding events in the regulation of insulin binding, action, and degradation in freshly isolated and primary cultures of rat hepatocytes. J Clin Invest. 1982;69:866 875.
100. Neal MJ. Analysis of effectiveness of human U-500 insulin in patients unresponsive to conventional insulin therapy. Endocr Pract. 2005;11:305 308.
101. Knee TS, Seidensticker DF, Walton JL, Solberg LM, Lasseter DH. A novel use of U-500 insulin for continuous subcutaneous insulin infusion in patients with insulin resistance: a case series. Endocr Pract. 2003;9:181 186.
EAN: 2147483647
Pages: 19