6. Breast
Authors: Dahnert, Wolfgang
Title: Radiology Review Manual, 6th Edition
Copyright 2007 Lippincott Williams & Wilkins
> Table of Contents > Breast
function show_scrollbar() {}
Breast
Differential Diagnosis of Breast Disorders
Variations in breast development
Unilateral Breast Development
may exist 2 years before other breast becomes palpable
Premature Thelarche
= breast development <8 years of age
Cause:
isolated idiopathic = mostly subtle overfunction of pituitary-ovarian axis
NO growth spurt/advanced bone age/menses
central precocious puberty
 enlargement of uterus + ovaries
enlargement of uterus + ovaries
- uni-/bilateral normal breast tissue
Congenital Anomalies
Polythelia
= more than normal number of nipples
Polymastia
= more than normal number of breasts
Amastia
= absence of mammary glands
Breast density
Asymmetric Breast Density
Benign
Postsurgical scarring
Noniatrogenic trauma
Postinflammatory fibrosis
Radial scar
Ectopic/accessory breast tissue (in axillary tail/close to abdomen)
Asymmetric breast development/asymmetric involution
Simple cyst
Fibrocystic conditions: fibrosis/sclerosing adenosis
Hormonal therapy: replacement, contraceptives
Malignant
Invasive ductal carcinoma: desmoplastic reaction
Invasive lobular carcinoma
Tubular carcinoma
Primary lymphoma of breast
Imaging Problems
Superimposed normal fibroglandular tissue
Lesion obscured by overlapping dense parenchyma
Lesion outside field of view
Breast Imaging Reporting and Data System (BI-RADS ) Categories
 Additional image evaluation may be necessary: off-angle/spot compression mammographic views; ultrasound
Additional image evaluation may be necessary: off-angle/spot compression mammographic views; ultrasound- Unexplained abnormalities warrant biopsy
Asymmetric Breast Tissue
= greater volume/density in one breast compared with corresponding area in contralateral breast
Density in One Projection
= density seen on only one standard mammographic view
Architectural Distortion
= focal area of distorted breast tissue (spiculations with common focal point/focal retraction/tethering) without definable central mass
Focal Asymmetric Density
= focal asymmetric density seen on two mammographic views but not identified as a true mass
Diffuse Increase in Breast Density
- generalized increased density
- skin thickening
- reticular pattern in subcutis
CANCER
Inflammatory breast cancer
Diffuse primary noninflammatory breast cancer
Diffuse metastatic breast cancer
Lymphoma/leukemia due to obstructive lymphedema of breast
INFECTIOUS mastitis
usually in lactating breast
RADIATION
diffuse exudative edema within weeks after beginning of radiation therapy
indurational fibrosis months after radiation therapy
EDEMA
Lymphatic obstruction: extensive axillary/intrathoracic lymphadenopathy, mediastinal/anterior chest wall tumor, axillary surgery
Generalized body edema: congestive heart failure (breast edema may be unilateral if patient in lateral decubitus position), hypoalbuminemia (renal disease, liver cirrhosis), fluid overload
HEMORRHAGE
Posttraumatic
Anticoagulation therapy
Bleeding diathesis
ACCIDENTAL INFUSION OF FLUID
into subcutaneous tissue
Enhancing Lesions on Breast MRI
Unilateral Diffuse Enhancement on MRI
Common
Parenchymal asymmetry
Fibrocystic changes
Adenosis
Unilateral implant
P.544
Rare
Normal: unfavorable cycle phase, HRT
Mastitis
Inflammatory breast cancer
Extensive carcinoma: diffuse lobular carcinoma, lymphangiosis, extensive DCIS
Prior ipsilateral radiotherapy within last few months
Round Homogeneously Enhancing Well-Demarcated Lesion on MRI
Common
Fibroadenoma: endotumoral septa
Adenoma
Papilloma
Carcinoma
Rare
Intramammary node:
- lipomatous hilum
Fat necrosis:
- macrocalcifications on mammogram
Granuloma
Carcinoma: esp. medullary form
Phylloides tumor
Metastasis
Ring-Enhancing Lesion on MRI
Common
1. Complicated cyst:
- narrow hyperintense ring on T2
2. Invasive carcinoma:
- broad ring of vital tumor, hypointense/isointense on T2
- shaggy rim
3. Superimposition of blood vessels: tubular structures on MIP
Rare
4. Adenosis
5. Abscess
6. Lymphadenitis
Multiple Homogeneously Enhancing Lesions with Well-defined Borders on MRI
Common
Fibrocystic changes
Fibroadenomas
Adenoma
Papilloma
Rare
Multicentric carcinoma
Metastases
Dendritic Enhancement on Breast MRI
Common
Adenosis
Fibrocystic change
DCIS
Motion artifacts on subtraction image
Superposition of intramammary veins
Rare
Previous galactography: history
Chronic mastitis
Lesion-in-Lesion Morphology on MRI
Giant juvenile fibroadenoma
Phyllodes tumor
Papilloma
Papillary carcinoma
Hemorrhage
Oval-shaped breast lesions
Mammographic Evaluation of Breast Masses
True mass or pseudomass?
SIZE
well-defined nodules <1.0 cm are of low risk for cancer
most likely benign nodules approaching 1 cm should be considered for ultrasound/aspiration/biopsy
SHAPE
increase in probability of malignancy: architectural distortion > irregular > lobulated > oval > round
MARGIN/CONTOUR (most important factor)
well-circumscribed mass with sharp abrupt transition from surrounding tissue is almost always benign
halo sign of apparent lucency = optical illusion of Mach effect + true radiolucent halo is almost always (92%) benign but not pathognomonic for benignity
microlobulated margin worrisome for cancer
obscured margin may represent infiltrative cancer
irregular ill-defined margin has a high probability of malignancy
spiculated margin due to
fibrous projections extending from main cancer mass
previous surgery
sclerosing duct hyperplasia (radial scar)
LOCATION
intramammary lymph node typically in upper outer quadrant (in 5% of all mammograms)
large hamartoma + abscess common in retro-/periareolar location
sebaceous cyst in subcutaneous tissue
X-Ray Attenuation = Density
fat-containing lesions are never malignant
high-density mass suspicious for carcinoma (higher density than equal volume of fibroglandular tissue due to fibrosis)
NUMBER
multiplicity of identical lesions decreases risk
INTERVAL CHANGE
enlarging mass needs biopsy
PATIENT RISK FACTORS
increasing age increases risk for malignancy
positive family history
history of previous abnormal breast biopsy
history of extramammary malignancy
Well-circumscribed Breast Mass
Well-defined nonpalpable lesions have a 4% risk of malignancy!
P.545
BENIGN
Cyst (45%)
Fibroadenoma
Sclerosing adenoma
Intraductal papilloma (intracystic/solid)
Galactocele
Sebaceous cyst
Pseudoangiomatous stromal hyperplasia
MALIGNANT
Medullary carcinoma
Mucinous carcinoma
Intracystic papillary carcinoma
Invasive ductal cancer not otherwise specified (rare)
Pathologic intramammary lymph node
Metastases to breast: melanoma, lymphoma/leukemia, lung cancer, hypernephroma
Well-circumscribed De Novo Mass in Woman >40 Years of Age
Cyst
Papilloma
Carcinoma
Sarcoma (rare)
Fibroadenoma (exceedingly rare)
Metastasis (extremely rare)
Fat-containing Breast Lesion
![]() Fat contained within a lesion proves benignity!
Fat contained within a lesion proves benignity!
Lipoma
Galactocele
= fluid with high lipid content (last phase)
during/shortly after lactation
Traumatic lipid cyst = fat necrosis = oil cyst
site of prior surgery/trauma
Focal collection of normal breast fat
Mixed Fat- and Water-density Lesion
Fibroadenolipoma/hamartoma
Intramammary lymph node
Galactocele
Hamartoma = lipofibroadenoma = fibroadenolipoma
Small superficial hematoma
Breast Lesion with Halo Sign
HIGH-DENSITY LESION
=vessels + parenchymal elements not visible in superimposed lesion
Cyst
Sebaceous cyst
Wart
LOW-DENSITY LESION
= vessels + parenchyma seen superimposed on lesion
Fibroadenoma
Galactocele
Cystosarcoma phylloides
Stellate/Spiculated Breast Lesion
= mass/architectural distortion characterized by thin lines radiating from its margins
The majority of invasive breast cancers are stellate (stellate:circular = 65:35)
93% of all stellate lesions are malignant (malignant:benign = 93:7)
Risk of malignancy:
75% for nonpalpable spiculated masses
32% for nonpalpable irregular masses
PSEUDOSTELLATE STRUCTURE
= Summation Shadow/Artifact
caused by fortuitous superimposition of normal fibrous + glandular structures; unveiled by rolled views, spot compression views microfocus magnification technique
BLACK STAR
- groups of fine straight/curvilinear fibrous strands bunched together like a broom
- circular/oval lucencies within center
- change in appearance from view to view
Radial scar = sclerosing duct hyperplasia (86%)
Sclerosing adenosis
Posttraumatic fat necrosis (11%)
WHITE STAR
- individual straight dense spicules
- central solid tumor mass
- little change in different views
malignant lesions
Invasive ductal carcinoma (65%) = scirrhous carcinoma
= desmoplastic reaction + secondary retraction of surrounding structures
clinical dimensions larger than mammographic size
- distinct central tumor mass with irregular margins
- length of spicules increases with tumor size
- localized skin thickening/retraction when spiculae extend to skin
- commonly associated with malignant-type calcifications
Invasive lobular carcinoma (21%)
palpable mass
- lack of central tumor mass
Tubular carcinoma (9%)
Other (5%)
benign lesions
Postoperative scar
correlation with history + site of biopsy
- scar diminishes in size + density over time
Postoperative hematoma
clinical information
- short-term mammographic follow-up confirms complete resolution
Breast abscess
clinical information
- high-density lesion with flamelike contour
Hyalinized fibroadenoma with fibrosis
- changing pattern with different projections
- may be accompanied by typical coarse calcifications of fibroadenomas
Granular cell myoblastoma
Fibromatosis
Extra-abdominal desmoid
P.546
mnemonic: Starfash
Summation shadow
Tumor (malignant)
Abscess
Radial scar
Fibroadenoma (hyalinized),
Fat necrosis
Adenosis (sclerosing)
Scar (postoperative)
Hematoma (postoperative)
Tumor-mimicking lesions
Phantom breast tumor = simulated mass
asymmetric density
- scalloped concave breast contour
- interspersed fatty elements
summation artifact = chance overlap of normal glandular breast structures
- failure to visualize tumor on more than one view
Silicone injections
Skin lesions
Dermal nevus
- sharp halo/fissured appearance
Skin calcifications
- lucent center (clue)
- superficial location (tangential views)
Sebaceous/epithelial inclusion cyst
Neurofibromatosis
Biopsy scar
Lymphedema
Lymph nodes
Frequency: 5.4% for intramammary nodes Location: axilla, subcutaneous tissue of axillary tail, lateral portion of pectoralis muscle, intramammary (typically in upper outer quadrant) - ovoid/bean-shaped mass(es) with fatty notch representing hilum
- central zone of radiolucency (fatty replacement of center) surrounded by crescent rim of cortex
- usually <1.5 cm (up to 4 cm) in size
- well-circumscribed with slightly lobulated margin
US:
- Vreniform hypoechoic rim with echogenic center
- echogenic hilum for entry and exit of vessels
Hemangioma
| Malignant Sonographic Characteristics (according to data from A.T. Stavros) | ||||
|---|---|---|---|---|
| US Characteristic | Sens. | Specif. | PPV | Rel. risk |
| Spiculation | 36.0 | 99.4 | 91.8 | 5.5 |
| Taller than wide | 41.6 | 98.1 | 81.2 | 4.9 |
| Angular margins | 83.2 | 92.0 | 67.5 | 4.0 |
| Acoustic shadowing | 48.8 | 94.7 | 64.9 | 3.9 |
| Branch pattern | 29.6 | 96.6 | 64.0 | 3.8 |
| Markedly hypoechoic | 68.8 | 60.1 | 60.1 | 3.6 |
| Calcifications | 27.2 | 96.3 | 59.6 | 3.6 |
| Duct extension | 24.8 | 95.2 | 50.8 | 3.0 |
| Microlobulation | 75.2 | 83.8 | 48.2 | 2.9 |
Solid Breast lesion by Ultrasound
Malignant Sonographic Characteristics
- Approximately 5 malignant features are found per cancer. The combination of 5 findings increases the sensitivity to 98.4%!
- spiculation = alternating straight lines radiating perpendicularly from surface of nodule
hypoechoic relative to echogenic fibrous tissue
hyperechoic relative to surrounding fat
- taller-than-wide lesion = AP dimension greater than craniocaudal/transverse dimension
- angular margin = contour of junction between hypo- or isoechoic solid nodule and surrounding tissue at acute /obtuse/90 angles
- acoustic shadowing behind all/part of nodule
(= fibroelastic host response to scirrhous cancer)
- central part of solid lesion very hypoechoic with respect to fat
- punctate echogenic calcifications within hypoechoic mass (acoustic shadowing commonly not present)
- radial extension/branch pattern (= intraductal component of breast cancer)
- microlobulation = many small lobulations at surface of solid nodule
Benign Sonographic Characteristics
- absence of any malignant characteristics
- A single malignant feature prohibits classification of a nodule as benign!
- marked hyperechogenic well-circumscribed nodule compared with fat = normal stromal fibrous tissue (may represent a palpable pseudomass/fibrous ridge)
- smooth well-circumscribed ellipsoid shape
- 2 3 smooth well-circumscribed gentle lobulations
- thin echogenic capsule
- kidney-shaped lesion = intramammary lymph node
- If specific benign features are not found the lesion is classified as indeterminate!
| Benign Sonographic Characteristics (according to data from A.T. Stavros) | ||||
|---|---|---|---|---|
| US Characteristic | Sens. | Specif. | NPV | Rel. risk |
| Hyperechoic | 100.0 | 7.4 | 100.0 | 0.00 |
| 3 lobulations | 99.2 | 19.4 | 99.2 | 0.05 |
| Ellipsoid shape | 97.6 | 51.2 | 99.1 | 0.05 |
| Thin echogenic capsule | 95.2 | 76.0 | 98.8 | 0.07 |
Breast calcifications
Indicative of focally active process; often requiring biopsy
- 75 80% of biopsied clusters of calcifications represent a benign process
- 10 30% of microcalcifications in asymptomatic patients are associated with cancers
| Composition: | hydroxyapatite/tricalcium phosphate/calcium oxalate |
Results of breast biopsies for microcalcification:
(without any other mammographic findings)
P.547
benign lesions (80%)
1. Mastopathy without proliferation 44% 2. Mastopathy with proliferation 28% 3. Fibroadenoma 4% 4. Solitary papilloma 2% 5. Miscellaneous 2% malignant lesions (20%)
1. Lobular carcinoma in situ
in 8% no spatial relationship to LCIS10% 2. Infiltrating carcinoma 6% 3. Ductal carcinoma in situ 4%
- A positive biopsy rate of >35% is desirable goal!
Location
intramammary
Ductal microcalcifications
- 0.1 0.3 mm in size, irregular, sometimes mixed linear + punctate
Occurrence: secretory disease, epithelial hyperplasia, atypical ductal hyperplasia, intraductal carcinoma Lobular microcalcifications
smooth round, similar in size + density
Occurrence: cystic hyperplasia, adenosis, sclerosing adenosis, atypical lobular hyperplasia, lobular carcinoma in situ, cancerization of lobules (= retrograde migration of ductal carcinoma to involve lobules), ductal carcinoma obstructing egress of lobular contents N.B.: lobular and ductal microcalcifications occur frequently in fibrocystic disease + breast cancer!
extramammary: arterial wall, duct wall, fibroadenoma, oil cyst, skin, etc.
Size
- malignant calcifications usually <0.5 mm; rarely >1.0 mm
Number
- <4 5 calcifications per 1 cm2 have a low probability for malignancy
Morphology
benign
Smooth round calcifications: formed in dilated acini of lobules
Solid/lucent-centered spheres: usually due to fat necrosis
Crescent-shaped calcifications that are concave on horizontal beam lateral projection = sedimented milk of calcium at bottom of cyst
Lucent-centered calcifications: around accumulated debris within ducts/in skin
Solid rod-shaped calcifications/lucent-centered tubular calcifications: formed within/around normal/ectatic ducts
Eggshell calcifications in rim of breast cysts
Calcifications with parallel track appearance = vascular calcifications
malignant
= calcified cellular secretions/necrotic cancer cells within ducts
- calcifications of
vermicular form
varying in size
linear/branching shape
Distribution
Clustered heterogeneous calcifications: adenosis, peripheral duct papilloma, hyperplasia, cancer
Segmental calcifications within single duct network: suspect for multifocal cancer within lobe
Regional/diffusely scattered calcifications with random distribution throughout large volumes of breast: almost always benign
Time course
malignant calcifications can remain stable for >5 years!
Density
Malignant Calcifications
Granular calcifications = resembling fine grains of salt
- amorphous, dotlike/elongated, fragmented
- grouped very closely together
- irregular in form, size, and density
Casting calcifications = fragmented cast of calcifications within ducts
- variable in size + length
- great variation in density within individual particles + among adjacent particles
- jagged irregular contour
- Y-shaped branching pattern
- clustered (>5 per focus within an area of 1 cm2)
Benign Calcifications
Lobular calcifications = arise within a spherical cavity of cystic hyperplasia, sclerosing adenosis, atypical lobular hyperplasia
- sharply outlined, homogeneous, solid, spherical pearl-like
- little variation in size
- numerous + scattered
- associated with considerable fibrosis
adenosis
- diffuse calcifications involving both breasts symmetrically
periductal fibrosis
- diffuse/grouped calcifications + irregular borders, simulating malignant process
Sedimented milk of calcium
Frequency: 4%
- multiple, bilateral, scattered/occasionally clustered calcifications within microcysts
- smudge-like particles at bottom of cyst on vertical beam
- crescent-shaped on horizontal projection = teacup-like
Plasma cell mastitis = periductal mastitis
- sharply marginated calcifications of uniform density = intraductal form
- sharply marginated hollow calcifications = periductal form
Peripheral eggshell calcifications
with radiolucent lesion
liponecrosis micro-/macrocystica calcificans (= fatty acids precipitate as calcium soaps at capsular surface) as calcified fat necrosis/calcified hematoma
- May mimic malignant calcifications!
with radiopaque lesion
degenerated fibroadenoma
macrocyst
- high uniform density in periphery
- usually subcutaneous
- no associated fibrosis
Papilloma
- solitary raspberry configuration in size of duct
- central/retroareolar
Degenerated fibroadenoma
- bizarre, coarse, sharply outlined, popcornlike very dense calcification within dense mass (= central myxoid degeneration)
- eggshell type calcification (= subcapsular myxoid degeneration)
Arterial calcifications
- parallel lines of calcifications
Dermal calcifications
Site: sebaceous glands
- hollow radiolucent center
- polygonal shape
- peripheral location (may project deep within breast even on 2 views at 90 angles)
- linear orientation when caught in tangent
- same size as skin pores
Proof: superficial marking technique Metastatic calcifications
Cause: 2 hyperparathyroidism (in up to 68%)
P.548
Calcifications in Branching Tubular Opacity
Ductal carcinoma in situ
Atypical ductal hyperplasia
Secretory disease
Peripheral papillomatosis
Vascular: calcified artery; Mondor disease (= thrombophlebitis of superficial vein)
Fat necrosis
S/P Galactography
Nipple & skin
Nipple Retraction
Positional
Relative to inflammation/edema of periareolar tissue
Congenital
Acquired (carcinoma, ductal ectasia)
| Galactographic Filling Defect | ||
|---|---|---|
| Type of Tumor | Single | Multiple |
| Multiple papilloma | 5.6% | 14.0% |
| Cancer | 0.05% | 9.7% |
Nipple Discharge
| Prevalence: | 7.4 % of breast surgeries |
Classification:
provoked
postovulatory state, duct ectasia, medication, stimulation by exercise, breast self-examination, sexual manipulation
Spontaneous
physiologic: pregnancy, lactation, galactorrhea, duct ectasia
pathologic: benign/malignant neoplasm, galactorrhea due to hyperprolactinemia from a pituitary adenoma
Unilateral
- Unilateral spontaneous discharge is significant + requires investigation!
Bilateral
- Expressed bilateral multipore blood-negative discharge is physiologic and benign!
Type of discharge:
Lactating breast: galactorrhea
Nonlactating breast:
normal:
1. milky
2. multicolored sticky (blue, green, gray, brown, black)
abnormal:
3. purulent: antibiotics, incision, drainage
surgically significant (in 14.3% cancerous)
4. clear/watery: cancer in 33%
5. bloody/sanguineous: cancer 28%,
6. pink/serosanguineous: cancer in 13%
7. yellow/serous: cancer in 6%
- The most common cause of bloody and serosanguineous discharge is intraductal papilloma (in 40%)!
- Exfoliative cytology not helpful (true positive in only 11%, false negative in 18%)
Site of origin:
Lobules + terminal duct lobular unit:
Galactorrhea
Fibrocystic changes
Larger lactiferous ducts (collecting duct, segmental duct, subsegmental duct)
Solitary papilloma
Papillary carcinoma
Duct ectasia
Galactography/Ductography
= injection of 0.2 0.3 mL of water-soluble contrast material (Conray 60 , Isovue ) through straight blunt 27-gauge pediatric sialography cannula (0.4 0.6 mm outer diameter)/30-gauge cannula/Jabczenski cannula (tip bent 90 )
Results of positive galactography:
papilloma (48%), benign conditions (42%), intraductal carcinoma (10%)
Contraindications to ductography:
history of severe allergy to iodinated contrast material, inability of patient to cooperate (debilitating anxiety, mental disorder), history of prior nipple surgery
DDx of intraductal defects:
gas bubble, clot, inspissated secretions, solitary intraductal papilloma, epithelial hyperplastic lesion, duct carcinoma
P.549
Secretory Disease
Retained lactiferous secretions
result of incomplete/prolonged involution of lactiferous ducts
- branching pattern of fat density in dense breast (high lipid content)
Prolonged inspissation of secretion + intraductal debris
= MAMMARY DUCT ECTASIA
- duct dilatation
- calcifications with linear orientation toward subareolar area a few mm long: rod-shaped/sausage-shaped/spherical with hollow center
Galactocele
Plasma cell mastitis
Skin Thickening of Breast
| Normal skin thickness: | 0.8 3 mm; may exceed 3 mm in inframammary region |
Localized Skin Thickening
Trauma (prior biopsy)
Carcinoma
Abscess
Nonsuppurative mastitis
Dermatologic conditions
GENERALIZED SKIN THICKENING
- Skin is thickened initially and to the greatest extent in the lower dependent portion of breast!
- overall increased density with coarse reticular pattern (= dilated lymph vessels + interstitial fluid triggering fibrosis)
Axillary lymphatic obstruction
Primary breast cancer
advanced breast cancer
invasive comedocarcinoma in large area
- Primary breast cancer not necessarily seen due to small size/hidden location (axillary tail, behind nipple)!
Primary malignant lymphatic disease (eg, lymphoma)
Intradermal + intramammary obstruction of lymph channels
Lymphatic spread of breast cancer from contralateral side
Inflammatory breast carcinoma = diffusely invasive ductal carcinoma
Mediastinal lymphatic blockage
Sarcoidosis
Hodgkin disease
Advanced bronchial/esophageal carcinoma
Actinomycosis
Advanced gynecologic malignancies from thoracoepigastric collaterals
Ovarian cancer
Uterine cancer
Inflammation
Acute mastitis
Retromamillary abscess
Fat necrosis
Radiation therapy
Reduction mammoplasty
Right heart failure
may be unilateral (R > L)/migrating with change in patient position (to avoid decubitus ulcer)
Nephrotic syndrome, anasarca
Dialysis
Renal transplant
Subcutaneous extravasation of pleural fluid following thoracentesis
Lymphadenopathy
nonpalpable
Radiographic features of normal lymph nodes:
- mass of low to moderate density
- sharply defined
- round to oval
- radiolucent fatty hilus (visible in 78%)
- <1 cm within breast tissue, <1.5 cm within axilla
Intramammary Lymphadenopathy
= adenopathy >1 cm surrounded by breast tissue
| N.B.: | nodes located high within axillary tail (= tail of Spence) are mammographically difficult to differentiate from inferior axillary lymph nodes |
Axillary Lymphadenopathy
= solid node >1.5 cm in size without fatty hilum
| N.B.: | lymph nodes of up to 3 cm may be normal if largely replaced by fat |
MALIGNANT
Metastasis from breast cancer in 26%
- Primary breast lesion may not be found in 33% of cases!
Metastases from non-breast primary (lung, melanoma, thyroid, GI tract, ovary)
Lymphoproliferative disease: lymphoma/chronic lymphocytic leukemia (17%)
- Bilateral axillary lymphadenopathy is suggestive of lymphoproliferative disease!
BENIGN
Nonspecific benign lymphadenopathy (29%)
Reactive nodal hyperplasia (breast infection/abscess/biopsy)
Collagen vascular disease: rheumatoid arthritis, systemic lupus erythematosus
Granulomatous disease: sarcoidosis
Psoriasis
HIV-related adenopathy
Silicone adenopathy
Radiographic features suspicious for malignancy:
- size increase of >100% over baseline
- size >3.3 cm
- change in shape
- spiculation of margins
- intranodal microcalcifications (without history of gold therapy)
- loss of radiolucent center/hilar notch
- increase in density
P.550
Mammography Report
based on BI-RADSR (Breast Imaging Reporting and Data System) published by the ACR (American College of Radiology)
Report Contents
Indication for exam
Comparison to previous studies
Breast Composition
Findings
Overall Assessment
| Bi-RADS Categories (American College of Radiology) | ||
|---|---|---|
| Mammography | Ultrasound | MRI |
| 0 need additional imaging evaluation or prior mammogram for comparison: eg, spot compression, magnification, special views, ultrasound | Need additional imaging: eg, an MRI for (1) palpable confirmed mass (2) recurrence versus scar after lumpectomy | Need additional imaging evaluation: eg, (1) technically unsatisfactory scan (2) screening MRI without kinetic imaging (3) incomplete information |
| 1 negative: symmetric breasts, no masses, architectural distortion, suspicious calcifications | Negative: no mass, architectural distortion, skin thickening, microcalcifications | Negative: symmetric breasts; no architectural distortion, abnormal enhancement, or mass |
| 2 Benign findings: eg, involuting calcified fibroadenoma, multiple secretory calcifications, oil cyst, lipoma, galactocele, hamartoma, intramammary node, vascular calcifications, implants, architectural distortion related to prior surgery | Benign findings: eg, simple cyst, intramammary lymph node, breast implant, stable postsurgical changes, probable fibroadenoma | Benign findings: hyalinized nonenhancing fibroadenoma, cyst, scar, fat-containing lesion (oil cyst, lipoma, galactocele, mixed-density hamartoma), breast implant |
| 3 probably benign (<2% risk of malignancy) initial short-interval follow-up suggested (in 6 months), not expected to change (over >2 years) after complete diagnostic work-up: eg, noncalcified circumscribed solid mass, focal asymmetry, cluster of round punctate calcifications | Probably benign short-interval followup suggested (<2% risk of malignancy): eg, classic findings of a fibroadenoma, nonpalpable complicated cyst, clustered microcysts | Probably benign short-interval follow-up suggested: a malignancy is highly unlikely |
| 4 Suspicious abnormality biopsy should be considered: not classic appearance of malignancy | Suspicious abnormality biopsy should be considered: intermediate (3 94%) probability of malignancy: e.g., a solid mass without all criteria of a fibroadenoma | Suspicious abnormality biopsy should be considered: lesion morphology not characteristic of breast cancer but of concern |
| 4a Low probability | ||
| 4b Intermediate probability | ||
| 4c Moderate probability | ||
| 5 Highly suggestive of malignancy ( 95% probability of cancer) appropriate action should be taken: eg, lesion could be considered for one-stage surgical treatment, however, biopsy usually required | Highly suggestive of malignancy (>95% probability) appropriate action should be taken: image-guided core needle biopsy | Highly suggestive of malignancy appropriate action should be taken: almost certainly malignant |
| 6 Known biopsy-proven malignancy eg, mammogram during neoadjuvant chemotherapy comparing it to pre-therapy mammogram | Known biopsy-proven malignancy eg, prior to chemotherapy, lumpectomy, mastectomy | Known biopsy-proven malignancy corresponding to the lesion imaged with MRI |
P.551
Lexicon Descriptors for Reporting
Mass
size shape round, oval, lobulated, irregular margins circumscribed, lobulated, obscured, indistinct, spiculated density relative to an equal volume of breast tissue: high, equal, low, fat location based on face of clock; depth (anterior, middle, posterior); subareolar; central; axillary Calcifications
benign skin, vascular, coarse popcornlike, large rodlike (secretory), round, lucent center, eggshell/rim, milk of calcium, suture, dystrophic, punctate indeterminate amorphous/indistinct probably malignant pleomorphic/heterogeneous (granular), linear branching/casting number size distribution grouped/clustered, linear, segmental, regional (within large volume of breast tissue), scattered/diffuse, multiple groups Associated Findings
skin thickening (diffuse, focal), retraction nipple retraction, inverted trabeculae thickening, architectural distortion axilla adenopathy
P.552
Breast Anatomy and Mammographic Technique
Breast development
Embryology
Milk line develops from ectodermal elements + extends from axillary region to groin; lack of regression leads to development of accessory breast tissue/accessory nipples
Tanner Stages
Stage I (prepubertal)
nipple elevates
- ill-defined hyperechoic retroareolar tissue
Stage II
| Cause: | estrogen for ductal + progesterone for lobuloalveolar development |
palpable subareolar bud = thelarche begins with onset of puberty (mean age, 9.8 years)
breast tissue + nipple arise as a single mound of tissue
- hyperechoic retroareolar nodule
- central star-shaped/linear hypoechoic area (simple branched ducts)
Stage III
enlargement + elevation of single mound
- hyperechoic glandular tissue extending away from retroareolar area
- central spider-shaped hypoechoic area
Stage IV (areolar mounding)
secondary mound develops (very transient) with nipple + areola projecting above the breast tissue
- hyperechoic periareolar fibroglandular tissue
- prominent central hypoechoic nodule
Stage V (mature breast)
regression of areola forming a smooth contour with the rest of the breast tissue
- hyperechoic glandular tissue
- increased subcutaneous adipose tissue anteriorly
- NO hypoechoic central nodule
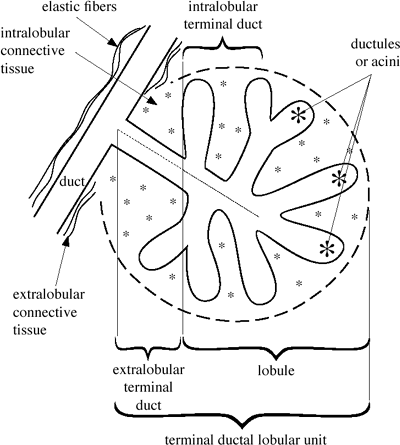 |
| Terminal Ductal Lobular Unit |
Breast Anatomy
Lobes
15 20 lobes disposed radially around nipple, each lobe has a main lactiferous duct of 2.0 4.5 mm converging at the nipple with an opening in the central portion of nipple
| Main duct: | branches dichotomously eventually forming terminal ductal lobular units |
| Histo: | epithelial cells, myoepithelial cells surrounded by extralobular connective tissue with elastic fibers |
Terminal Duct Lobular Unit (TDLU)
Extralobular terminal duct
Histo: lined by columnar cells + prominent coat of elastic fibers + outer layer of myoepithelium Lobule
intralobular terminal duct
Histo: lined by 2 layers of cuboidal cells + outer layer of myoepithelium ductules/acini
intralobular connective tissue
Size: 1 8 mm (most 1 2 mm) in diameter
Change:
reproductive age: cyclic proliferation (up to time of ovulation) + cyclic involution (during menstruation)
post menopause: regression with fatty replacement
Significance:
TDLU is site of fibroadenoma, epithelial cyst, apocrine metaplasia, adenosis (= proliferation of ductules + lobules), epitheliosis (= proliferation of mammary epithelial cells within preexisting ducts + lobules), ductal + lobular carcinoma in situ, infiltrating ductal + lobular carcinoma
Components of Normal Breast Parenchyma
Nodular densities surrounded by fat
1 2 mm = normal lobules
3 9 mm = adenosis
Linear densities
= ducts and their branches + surrounding elastic tissue
Structureless ground-glass density
= stroma/fibrosis with concave contours
Parenchymal Breast Pattern (L szl Tab r)
Pattern I
named QDY = quasi dysplasia (for Wolfe classification)
- concave contour from Cooper's ligaments
- evenly scattered 1 2 mm nodular densities (= normal terminal ductal lobular units)
- oval-shaped/circular lucent areas (= fatty replacement)
P.553
Pattern II
similar to N1 (Wolfe)
- total fatty replacement
- NO nodular densities
Pattern III
similar to P1 (Wolfe)
- normal parenchyma occupying <25% of breast volume in retroareolar location
Pattern IV = adenosis pattern
similar to P2 (Wolfe)
Cause: hypertrophy + hyperplasia of acini within lobules Histo: small ovoid proliferating cells with rare mitoses - scattered 3 7 mm nodular densities (= enlarged terminal ductal lobular units) = adenosis
- thick linear densities (= periductal elastic tissue proliferation with fibrosis) = fibroadenosis
- no change with increasing age (genetically determined)
Pattern V
similar to DY (Wolfe)
- uniformly dense parenchyma with smooth contour (= extensive fibrosis)
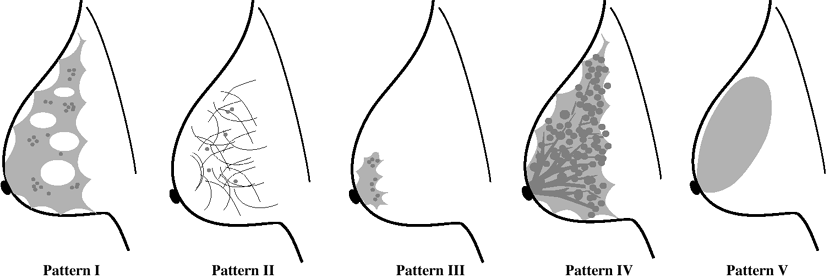 |
| Parenchymal Breast Patterns |
| Breast composition and parenchymal pattern | |||
|---|---|---|---|
| Composition (BI-RADS ) | Descriptor | Pattern (Tab r) | Descriptor |
| 1 | Almost entirely fatty breast | II | Completely involuted breast |
| 2 | Scattered fibroglandular tissue that could obscure a lesion | I | Normal premenopausal parenchyma |
| III | Involution with prominent retroareolar ducts | ||
| 3 | Heterogeneously dense tissue that may lower the sensitivity of mammography | IV | Adenosis pattern of dominant nodular and linear densities |
| 4 | Extremely dense breast tissue that lowers the sensitivity of mammography | V | Extensive structureless fibrosis |
Enhancement of Normal Parenchyma on MRI
Image 7 20 days after beginning of LMP
Proper enhancement present if:
veins contrasted on MIP
both internal mammary arteries depicted
nipple enhances
- increased enhancement under HRT with estrogen/during lactation (with great interindividual variations):
- linear patchy enhancement
- bilateral symmetric patchy enhancement
- confluent enhancement on late dynamic scan
- Hormone effects reverse after 30 60 days
- Breast involution after lactation takes 3 months
- decreased enhancement under antiestrogen treatment (eg, tamoxifen)
Lymphatic Drainage
Axillary nodes (97%)
level I = lateral to lateral edge of pectoralis minor
level II = behind pectoralis minor
level III = medial to medial edge of pectoralis minor
Internal mammary nodes (3%)
- characteristic radiolucent center (fat)
P.554
US:
- hypoechoic periphery + hyperechoic center
MR:
T1WI
- not recognizable within parenchyma
- recognizable in extraparenchymal location as oval well-circumscribed hypointense lesion with central hyperintense area
enhanced T1WI:
- no/slight enhancement in bland nodes
- strong enhancement + wash-out phenomenon simulating ring enhancement of malignancy in reactive inflammatory nodes
T2WI:
- no characteristic finding
| Descriptor of Signal Enhancement in Breast MRI | |
|---|---|
| Enhancement | SI increase compared to precontrast |
| None | 0% |
| Slight | <50% |
| Moderate | 50 100% |
| Strong | >100% |
Mammographic Film Reading Technique
Compare with earlier films
Scan forbidden areas
Milky Way = 2 3 cm wide area parallel to the edge of the pectoral muscle on MLO projection
No man's land = fatty replaced area between posterior border of parenchyma + chest wall on CC projection
Medial half of breast on CC view
Look for increased retroareolar density
Look for parenchymal contour retraction
Look for architectural distortion
Look for straight lines superimposed on normal scalloped contour
Compare left with right side
Don't stop looking after one lesion is found
Mammographic Technique
BEAM QUALITY
Molybdenum target material with characteristic emission peaks of 17.9 + 19.5 keV (lower average energy than tungsten)
FOCAL SPOT
0.1 0.4 mm (0.1 mm for magnification views)
TUBE OUTPUT
80 100 mA
EXPOSURE
without grid: 25 kV (optimum between contrast + penetration), exposure time of 1.0 seconds
with grid: 26 27 kV; exposure time of 2.3 seconds
microfocus magnification: 26 27 kV; 1.5 2.0 times magnification with 16 30 cm air gap
specimen radiography: 22 24 kV
FILTER
beryllium window (absorbs less radiation than glass tube)
molybdenum filter (0.03 mm): allows more of lower energy radiation to reach breast
REDUCTION OF SCATTER RADIATION
adequate compression (also improves contrast + decreases radiation dose)
beam collimation to <8 10 cm
air gap with microfocus magnification
(greater spatial resolution, 2 3-fold increase in radiation exposure)
Moving grid
grid if compressed breast >5 cm/very dense breast (facilitates perception, 2 3-fold increase in radiation exposure)
SCREEN-FILM COMBINATION
Intensifying screen phosphor
single screen systems
Film-screen contact
Mammography film with minimal base fog, sufficient maximum density + contrast
FILM PROCESSING
Processing time of 3 minutes (42 45 seconds in developing fluid) superior to 90-second processor for double-emulsion film (which creates underdevelopment + compensatory higher radiation exposure)
Developing temperature of 35 C (95 F)
Developing fluid replenishment rate:
450 500 mL replenisher per square meter of film
QUALITY CONTROL
Processor (daily)
with sensito-/densitometric measurements
(a) base fog <0.16 0.17
(b) maximum density >3.50
(c) contrast >1.9 2.0
X-ray unit (semiannually)
beam quality
phototimer
Average glandular dose:
<0.6 MGY per breast for nonmagnification film-screen mammogram (ACR accreditation requirement)
Screen/film technique (molybdenum target; 0.03 mm molybdenum filter, 28 kVp):
mean absorbed dose: 0.05 rad for CC view
0.06 rad for LAT view
Effective dose equivalent HE:
screen-film mammography 0.11 mSv
xeroradiographic mammography 0.78 mSv
chest 0.05 mSv
skull 0.15 mSv
abdomen 1.40 mSv
lumbar spine 2.20 mSv
Advantages of magnification mammography:
Sharpness effect = increased resolution
Noise effect = noise reduced by a factor equal to the degree of magnification
Air-gap effect = increased contrast by reduction in scattered radiation
Visual effect = improved perception and analysis of small detail
P.555
Factors Affecting Mammographic Image Quality
Radiographic Sharpness
= subjective impression of distinctness/perceptibility of structure boundary/edge
Radiographic contrast
= magnitude of optical density difference between structure of interest + surroundings influenced by
subject contrast
= ratio of x-ray intensity transmitted through one part of the breast to that transmitted through a more absorbing adjacent part; affected by
absorption differences in the breast (thickness, density, atomic number)
radiation quality (target material, kilovoltage, filtration)
scattered radiation (beam limitation, grid, compression)
receptor contrast
= component of radiographic contrast that determines how the x-ray intensity pattern will be related to the optical density pattern in the mammogram
affected by
film type
processing (chemicals, temperature, time, agitation)
photographic density
fog (storage, safelight, light leaks)
Radiographic blurring
lateral spreading of a structural boundary
(= distance over which the optical density between the structure and its surroundings changes)
motion
reduced by compression + short exposure time
geometric blurring
affected by
focal spot: size, shape, intensity distribution
focus-object distance (= cone length)
object-image distance
receptor blurring
= light diffusion (= spreading of the light emitted by the screen) affected by
phosphor thickness + particle size
light-absorbing dyes + pigments
screen-film contact
Radiographic Noise
= unwanted fluctuation in optical density
Radiographic mottle
= optical density variations consist of
receptor graininess
= optical density variation from random distribution of finite number of silver halide grains
quantum mottle (principal contributor to mottle)
= variation in optical density from random spatial distribution of x-ray quanta absorbed in image receptor
affected by
film speed + contrast
screen absorption + conversion efficiency
light diffusion
radiation quality
structure mottle
= optical density fluctuation from nonuniformity in the structure of the image receptor (eg, phosphor layer of intensifying screen)
Artifacts
= unwanted optical density variations in the form of blemishes on the mammogram
(a) improper film handling (static, crimp marks, fingerprints, scratches)
(b) improper exposure (fog)
(c) improper processing (streaks, spots, scratches)
(d) dirt + stains
P.556
Breast Disorders
Breast Cancer
| Incidence: | 1.5 4.5 cases per 1,000 women per year |
| Origin: | terminal ductal lobular unit |
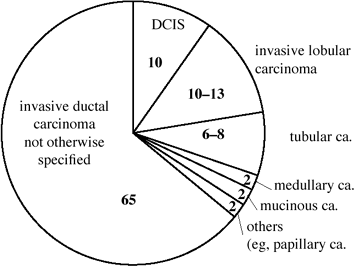 |
| Distribution of Breast Cancers in Screening Population (numbers are percentages) |
Noninvasive Breast Cancer (15%)
= malignant transformation of epithelial cells lining mammary ducts + lobules confined within boundaries of basement membrane
Rx: few data are available to provide insight into proper treatment
Ductal carcinoma in situ (DCIS)
= intraductal carcinoma
( cancer waiting to become malignant )
- 30% become invasive over 10 years
| Incidence: | 20 40% in screening population; 70% of noninvasive carcinomas |
| Age: | most >55 years (40 60 years) |
| Histo: | heterogeneous group of malignancies originating within extralobular terminal duct + without invasion of basement membrane; causes duct diameter increase from 90 to 360 m |
| Subgroups: | comedocarcinoma, non-comedocarcinomas (solid, micropapillary, cribriform) |
| Associated with: | ADH + invasive ductal carcinoma |
may persist for years without palpable abnormality (in screening population)
palpable mass (10%)/Paget disease of nipple/nipple discharge (in symptomatic patients)
- 50% of DCIS are >5 cm in size
- Histologic size of DCIS is independent of histologic subgroup
- Almost all comedo type DCIS contain significant microcalcifications
- DCIS often involves the nipple + subareolar ducts
Spectrum of mammographic findings:
- calcifications only (72%)
- soft-tissue abnormality + calcification (12%)
- soft-tissue abnormality only (10%)
- invisible (6%)
MR (50 60% sensitive, 18 100% FN [!]):
T1WI:
- isointense to surrounding parenchyma
enhanced T1WI:
- branching/spiculated/round enhancing lesion with ill-defined margins (in 90%)
- enhancement pattern typical of malignancy (in 30 50%)/nonspecific (in 40 55%)
- no enhancement (in 5 10%)
- no ring enhancement
T2WI:
- no specific findings
| Prognosis: | 98% survival after 13 years |
| Rx: | (1) Simple/modified mastectomy: cure rate of almost 100% (2) Local excision alone: local recurrence in 4 years: 19% for poorly differentiated 10% for moderately differentiated 0% for well differentiated (3) Lumpectomy + radiotherapy: 2 17% rate of recurrence |
Treatment problems:
Occult invasion in 5 20% of patients
Multifocality in 30%
(= >2 foci in same breast quadrant)
Multicentricity
(= >1 focus in different breast quadrants with a minimum distance of 2 cm)
in 14% of lesions <25 mm,
in 100% of lesions >50 mm
Axillary metastases in 1 2%
HIGH NUCLEAR GRADE DCIS ( COMEDO TYPE )
| Prevalence: | 60% of all DCIS |
| Precursor: | none; one stage development |
| Path: | comedo = pluglike appearance of necrotic material that can be expressed from the cut surface |
Characteristics:
nuclear grade: large/intermediate nuclei, numerous mitoses, aneuploidy
growth pattern: predominantly solid cell proliferation; atypically micropapillary/cribriform
necrosis: extensive (HALLMARK)
calcifications (90%): dystrophic/amorphous within necrosis in center of dilated ductal system outlining most of the lobe in classic solid growth pattern
estrogen- + progesterone-receptor negative
overexpression of c-erb B-2 oncogene product and P53 suppressor gene mutation
often symptomatic lesion with nipple discharge
- ductal system enlarged to 300 350 m
- linear/branching pattern of calcifications scattered in a large part of lobe/whole lobe
- large solid high-density casting calcifications (fragmented, coalesced, irregular) in solid growth pattern
- snake skin like / birch tree flowerlike dotted casting calcifications within necrosis of micropapillary/cribriform growth pattern
- palpable dominant mass without calcifications (very unusual)
- nipple discharge (rare)
P.557
| Prognosis: | higher recurrence rate than noncomedo-group |
LOW NUCLEAR GRADE DCIS ( NONCOMEDO TYPE )
| Prevalence: | 40% of all DCIS |
Precursor lesion:
atypical ductal hyperplasia (ADH) with slight/moderate/severe atypia
- 52 56% of ADH at core biopsy are associated with malignancy at excision!
Characteristics:
nuclear grade: monomorphic small round nuclei, few/no mitoses
growth pattern: predominantly micropapillary/cribriform; atypically solid cell proliferation (often coexist)
necrosis: not present in classic micropapillary/cribriform growth pattern
calcifications (50%): laminated/psammoma-like due to active secretion by malignant cells into duct lumen
- fine granular cotton ball calcifications in micropapillary/cribriform growth pattern
- coarse granular crushed stone / broken needle tip / arrowhead calcifications in less common solid growth pattern
- Size of noncomedo DCIS often underestimated mammographically (? due to lower density of calcifications at periphery of lesion)!
- palpable dominant mass without calcifications (intracystic papillary carcinoma, multifocal papillary carcinoma in situ)
- nonpalpable asymmetric density with architectural distortion
- occasionally serous/bloody nipple discharge + ductal filling defects on galactography
| Prognosis: | 30% eventually develop into invasive cancer |
| Risk of recurrence: | 2% |
| Dx: | surgical biopsy Core needle biopsy could result in diagnosis of only proliferative breast disease that is usually intermixed! |
Lobular Carcinoma In Situ (LCIS)
= arises in epithelium of blunt ducts of mammary lobules
- NOT a precancerous lesion BUT a marker for an increased risk of subsequent invasive cancer in either breast!
( Risk factor waiting to become malignant )
| Incidence: | 0.8 3.6% in screening population; 3 6 % of all breast malignancies;25% of all noninvasive carcinomas; high incidence during reproductive age but decreasing with age |
| Age: | most 40 54 years (earlier than DCIS/invasive tumors) |
| Histo: | monomorphous small cell population filling + expanding ductules of the lobule Synchronous invasive cancer in 5%! |
not palpable
- mammographically occult
- may atypically present as a noncalcified mass (in 7%), calcifications + mass (in 10%), asymmetric opacity (2%)
MR:
T1WI:
- isointense to breast parenchyma
enhanced T1WI:
- ill-defined enhancement with nonspecific intensity curves
- High frequency of multicentricity (50 70%) + bilaterality (30%)!
| Dx: | incidental microscopic finding depending on accident of biopsy (performed for unrelated reasons + findings) |
Prognosis:
20 30% develop invasive ductal > lobular carcinoma within 20 years after initial diagnosis
- 1% per year lifetime risk for invasive malignancy
- LCIS serves as a marker of increased risk for developing invasive carcinoma in either breast!
| Rx: | recommendations range from observation (with follow-up examinations every 3 6 months + annual mammograms) to unilateral/bilateral simple mastectomy |
Intracystic Papillary Carcinoma In Situ (0.5 2%)
= rare variant of noncomedo DCIS
| Age: | usually older postmenopausal woman; peak prevalence between 34 and 52 years |
| Histo: | papillary fronds within the wall of a cystically dilated duct |
well-circumscribed + freely movable
aspiration yields straw-colored/dark red/brown fluid (due to ruptured capillaries in cyst wall/necrosis of tumor cells); reaccumulation of fluid within 3 4 weeks
fluid cytology negative for cancer in 80%
- mean tumor size of 1.9 cm (range 0.4 7.5 cm) due to fast growth (from accumulation of fluid + proliferation of neoplastic cells)
- intracystic mass on pneumocystography
- solid intracystic mass on US
- round benign appearing mass with sharply circumscribed lobulated borders on mammography
| Rx: | lumpectomy |
| Prognosis: | 10-year survival of 100%; 10-year disease-free survival rate of 91% |
| DDx for mammogram: | mucinous/medullary ca., hematoma, metastasis |
P.558
Invasive Breast Cancer (85%)
MR:
- peripheral/rim enhancement
Infiltrating/Invasive Ductal Carcinoma (65%) of no special type/otherwise not specified (NOS)
- Most frequently encountered breast malignancy
- 10% false-negative ratio
| Age: | any (peak, 50 60 years) |
Histo:
grade I = well-differentiated
grade II = moderately differentiated
grade III = poorly differentiated
Strong fibrotic component!
palpable (70% are first palpated by the patient)
larger by palpation than on mammogram
often poorly movable + indolent
| Location: | multifocal in 15%; bilateral in 5% |
- spiculated mass (36%) is PRINCIPAL FINDING
- lobulated/round/oval
- increased central density
- malignant calcifications (45 60%)
US:
- ill-defined hypoechoic mass with hyperechoic margins
- central/peripheral acoustic shadowing
MR (88 98% sensitive):
T1WI:
- isointense to parenchyma; hypointense to fat
enhanced T1WI:
- round/ovoid/spiculated lesion with ill-defined margins
- ring enhancement in up to 50% with centripetal progression
- strong (in 60%)/moderate (in 35%)/mild (in 5%) contrast uptake
- plateau (most frequent)/wash-out (often)/continuous increase (rare) on postinitial phase
- dilated veins draining the tumor
T2WI:
- iso- to hypointense to parenchyma
- occasionally hyperintense edematous zone
Infiltrating/Invasive Lobular Carcinoma (5 10%)
= neoplasm arising from terminal ductules of breast lobules
- 2nd most common form of invasive breast cancer; 30 50% of patients will develop a second primary in same/opposite breast within 20 years
- Most frequently missed breast cancer (difficult to detect mammographically + clinically) with 19 43% false-negative rate (occult in dense breast)
Median age: 45 56 years; 2% of all ILC occur in women <35 years Path: multicentricity (30%) + bilaterality (10%); tendency to grow around ducts, vessels, and lobules without destruction of anatomic structures ( Indian file /targetoid growth); desmoplastic stromal reaction Histo: 20% grade I, 64% grade II, 16% grade III Metastases: GI tract, gynecologic organs, peritoneum, retroperitoneum, carcinomatous meningitis palpable in 69%:
area of subtle skin thickening/induration
large hard mass/fine nodularity
- architectural distortion (= retraction of normal glandular tissue with thickening + disturbance of fibrous septa) in 18 30% is MOST COMMON MAMMOGRAPHIC FINDING
Histo: straight single file of uniform small cells with round oval nuclei ( Indian files ) growing around ducts resulting in subtle changes in architecture - irregular spiculated mass >1 cm (16 28%)
- poorly defined mass spicules <1 cm (22%)
- asymmetric opacity (= ill-defined area of increased opacity without central tumor nidus) in 8 19%
- round/ovoid mass with regular borders (1%)
- microcalcifications (0 24%)
- retraction of skin (25%) + nipple (26%)
- skin thickening
- May be evident on ONLY one standard view CC > ML > MLO view)!
MR (83 100% sensitive):
T1WI:
- isointense to parenchyma
enhanced T1WI:
- moderate/strong initial enhancement
- postinitial plateau (frequently)/wash-out (occasionally)/continuous increase (rare)
- lack of mass effect + amorphous asymmetry
- lack of mass effect + amorphous asymmetry
- ring enhancement of nodular tumor form (in up to 50%)
T2WI:
- iso- to hypointense to breast parenchyma
Prognosis: poor due to late diagnosis N.B.: difficulties in early diagnosis result in disproportionate potential for malpractice suits! Tubular Carcinoma (6 8%)
= well-differentiated form of ductal carcinoma
low grade: bilateral in 1:3
high grade: bilateral in 1:300
Associated with: lobular carcinoma in situ in 40% Mean age: 40 49 years positive family history in 40%
nonpalpable
- high-opacity nodule with spiculated margins
- <17 mm in diameter; mean diameter of 8 mm
MR:
T1WI:
- stellate hypointense lesion well seen in fat
enhanced T1WI:
- stellate tumor with moderate/strong initial uptake
- ring enhancement rare
- postinitial plateau (frequent)/wash-out (rare) /continuous increase (very rare)
T2WI:
- iso-/slightly hypointense to parenchyma
- occasional peritumoral edematous zone
DDx: radial scar Medullary Carcinoma (2%)
= SOLID CIRCUMSCRIBED CARCINOMA
- Fastest growing breast cancer!
- distinct/indistinct margins
- Often associated with BRCA gene!
P.559
Path: well-circumscribed mass with nodular architecture + lobulated contour; central necrosis is common in larger tumors; reminiscent of medullary cavity of bone Histo: intense lymphoplasmocytic reaction (reflecting host resistance); propensity for syncytial growth; no glands Incidence: 11% of breast cancers in women <35 years of age; 40 50% of medullary cancers in women <50 years of age Mean age: 46 54 years softer than average breast cancer
Mean size: 2 3 cm - well-defined round/oval noncalcified uniformly dense mass (hemorrhage) with lobulated margin
- may have partial/complete halo sign
US:
- hypoechoic mass with some degree of through transmission
- distinct/indistinct margins
- large central cystic component
MR:
- irregular internal architecture (no septa!)
T1WI:
- well-circumscribed hypointense lesion difficult to detect in parenchyma
enhanced T1WI:
- moderately/strongly enhancing round/ovoid lesion with smooth edge
- ring enhancement occasionally
- postinitial plateau (frequent)/wash-out (occasionally)/continuous increase (rare)
T2WI:
- iso- or mildly hypointense to parenchyma
DDx: myxoid fibroadenoma Prognosis: 92% 10-year survival rate Mucinous/Colloid Carcinoma (1.5 2%)
Path:
pure form: aggregates of tumor cells surrounded by abundant pools of extracellular mucin (gelatinous/colloid fluid)
mixed form: contains areas of infiltrating ductal carcinoma not surrounded by mucin
Age: 1% in women <35 years; 7% of carcinomas in women >75 years slow growth rate of pure form
swish / crush sensation during palpation
60% estrogen-receptor positive
- well-circumscribed usually lobulated mass of round/ovoid shape
- pleomorphic clustered/clumped amorphous/punctate calcifications (rare)
- may enlarge fast (through mucin production)
- solid mass on US
MR:
T1WI:
well-circumscribed round/ovoid hypointense lesion difficult to detect in parenchyma
enhanced T1WI:
- very strong (usually)/moderate (occasionally)/slight (rare) initial uptake
- rarely ring enhancement
- postinitial plateau (frequent)/wash-out (occasionally)/continuous increase (very rare)
T2WI:
- iso-/slightly hypointense to parenchyma
- hyperintense center with thin rim
Prognosis: favorable Papillary Carcinoma (1 2 4%)
= rare ductal carcinoma forming papillary structures
N.B.: Do not confuse with micropapillary/cribriform growth pattern of ductal carcinoma Histo: multilayered papillary projections extending from vascularized stalks; no myoepithelial layer (as in benign lesions); neurosecretory granules + positive CEA-reactivity in 85% (absent in benign lesions) Types: (a) multiple intraductal carcinomas with papillary configuration
(b) Intracystic papillary carcinoma = in situ malignancy
(c) invasive carcinoma with papillary growth pattern (microscopic frond formation)Age: 25 89 (mean 50 60) years; peak age of 40 75 years palpable mass (67%)
nipple discharge (22 35%) often tinged with blood
rich in estrogen and progesterone receptors
Location: single nodule in central portion of breast; multiple nodules extending from subareolar area to periphery of breast - multinodular pattern (55%) = lobulated mass/cluster of well-defined contiguous nodules
- solitary well-circumscribed round/ovoid nodule with average diameter of 2 3 cm
- usually confined to single quadrant
- associated microcalcifications in 60%
- multiple filling defects/disruption of an irregular duct segment/complete obstruction of duct system at galactography
US:
solid hypoechoic mass with lobulated smooth margins + acoustic enhancement
blood flow on color Doppler
MR:
T1WI:
- well-circumscribed hypointense retroareolar lesion
enhanced T1WI:
- strong initial enhancement
- ring enhancement possible
- postinitial plateau/wash-out
T2WI:
- well-circumscribed lesion of intermediate intensity in signal-intense cyst
Prognosis: 90% 5-year survival after simple mastectomy + axillary node dissection DDx: solitary central duct papilloma; multiple peripheral benign papillomas P.560
Paget Disease of the Nipple (5%)
Inflammatory Breast Carcinoma
= tumor emboli within dermal lymphatics (angiolymphatic spread)
Prevalence: 1 2 4% of breast cancers Age: 52 years (on average) Histo: infiltrating ductal carcinoma Location: L > R breast; bilaterality in 30 55% rapid symptomatic development over 1/3 of breast surface:
palpable tumor (63%)
erythema of skin (13 64%)
peau d'orange edema of skin (13%)
nipple retraction (13%)
palpable axillary adenopathy (in up to 91%)
- tumor mass malignant-type calcifications
- diffusely increased breast density
- stromal coarsening (50%)
- thickening of Cooper ligaments
- extensive skin thickening (71%)
MR:
T1WI:
- skin thickening
enhanced T1WI:
- strong increased uptake in thickened skin + tumor infiltrated parenchyma
- occasionally delineation of primary tumor
T2WI:
- diffuse increase in intensity compared to contralateral breast
- sometimes hypovascular tumor surrounded by nontumoral edema
| Dx: | skin biopsy |
| Prognosis: | 2% 5-year survival; median survival time of 7 months (untreated) + 18 months (after radical mastectomy) |
| DDx: | mastitis (test treatment with macrolide antibiotic azithromycin, eg, Zithromax Z-pak ) |
Epidemiology of Breast Cancer
| Incidence: | 2 5 breast cancers/1,000 women; in USA >142,000 new cases per year (of which 25,000 are in situ); 25% of all female malignancies |
- 12% lifetime risk of breast cancer = 1 in 9 women will develop breast cancer during her life!
| Age: | 0.3 2% in women <30 years of age; 15% in women <40 years of age;85% in women >30 years of age |
| Mortality: | 43,000 deaths per year |
- Death rate has remained stable for past 60 years!
Risk Factors (increasing risk):
Demographic Factors in Breast Cancer
increasing age (66% of cancers in women >50 years):
Age Prevalence of Breast Cancer 25 5:100,000 1:19,608 40 80:100,000 1:1,250 45 1075:100,000 1:93 50 180:100,000 1:555 55 3030:100,000 1:33 60 240:100,00060 1:416 Relative Risk Compared with Woman of Age 60 30 years of age 0.07 35 years of age 0.19 40 years of age 0.35 50 years of age 0.71 60 years of age 1.00 70 years of age 1.27 80 years of age 1.45 Ashkenazi Jewish women + nuns
upper > lower social class
unmarried > married women
Whites > Blacks after age 40
REPRODUCTIVE VARIABLES IN BREAST CANCER
nulliparous > parous:
Relative Risk Compared with Nulliparous: age at 1st pregnancy <19 years 0.5 age at 1st pregnancy 20 30 years age at 1st pregnancy 30 34 years 1.0 age at 1st pregnancy >35 years >1.0 first full-term pregnancy after age 35: 2 risk
low parity > high parity
early age at menarche (<12 years):
relative risk compared with onset of regular ovulatory cycle:
Menarche <12 Menarche >12 immediately 3.7 1.6 1 4 years 2.3 1.6 late age at menopause: relative risk compared with menopause before age 44 years:
natural menopause >55 years of age 2.0
early bilateral oophorectomy: relative risk compared with menopause between ages 45 49 years:
artificial menopause at 50 54 years 1.34
artificial menopause before age 45 0.77
Multiple Primary Cancers in Breast Cancer
4 5 increase in risk for cancer in contralateral breast
increased risk after ovarian + endometrial cancer
BRCA
= mutation of tumor suppressor gene
BRCA 1 (breast cancer 1) on long arm of chromosome 17
BRCA 2 (breast cancer 2) on chromosome 13 involved in 5 10% of all breast cancers
Family History of Breast Cancer
breast cancer in first-degree relative: Relative risk compared with negative family Hx:
(+) for mother 1.8
(+) for sister 2.5
(+) for mother + sister 5.6
25% of patients with carcinoma have a positive family history
carcinoma tends to affect successive generations approx. 10 years earlier
P.561
BENIGN BREAST DISEASE AND BREAST CANCER
2 4 increased risk with atypical hyperplasia relative risk compared with no biopsy:
benign breast disease in all patients 1.5
nonproliferative disease 0.9
proliferative disease without atypia 1.6
fibroadenoma + hyperplasia 3.5
atypical duct hyperplasia (ADH):
no family history of breast cancer 4.4
family history of breast cancer 8.9
PARENCHYMAL BREAST PATTERN AND BREAST CANCER
prominent duct pattern + extremely dense breasts according to Wolfe classification N1 (0.14%), P1 (0.52%), P2 (1.95%), DY (5.22%)
RADIATION EXPOSURE AND BREAST CANCER
excess risk of 3.5 6 cases per 1,000,000 women per year per rad after a minimum latent period of 10 years (atomic bomb, fluoroscopy during treatment of tuberculosis, irradiation for postpartum mastitis, Hodgkin disease)
GEOGRAPHY
Western + industrialized nations (highest incidence)
Asia, Latin America, Africa (decreased risk)
Breast Cancer Evaluation
Localizing Signs of Breast Cancer
= PRIMARY SIGNS OF BREAST CANCER
Dominant mass seen on two views with
Spiculation = stellate/star-burst appearance (= fine linear strands of tumor extension + desmoplastic response); scirrhus caused by:
infiltrating ductal carcinoma (75% of all invasive cancers)
invasive lobular carcinoma (occasionally)
- mass feels larger than its mammographic/sonographic size
DDx: prior biopsy/trauma/infection Predictive Value of radiographic signs of Malignancy related to Clinical Findings
Mammographic Sign Palpable Abnormality PPV (%) Classic for malignancy + 100 Classic for malignancy - 74 Microcalcifications* + 25 Microcalcifications* - 21 Indeterminate mammogram + 11 Indeterminate mass - 5 Benign mass + 2 Asymmetric density (? mass) + 4 Asymmetric density (? mass) - 0 Dilated vein 0 Skin thickening 0 Dilated duct 0 *(>3 punctate irregular microcalcifications in area <1 cm2) Smooth border
intracystic carcinoma (rare): subareolar area; bloody aspiration
medullary carcinoma: soft tumor
mucinous/colloid carcinoma: soft tumor
papillary carcinoma
- telltale signs: lobulation, small comet tail, flattening of one side of the lesion, slight irregularity
- halo sign (= Mach band) may be present
DDx: cyst (sonographic evaluation) Lobulation
appearance similar to fibroadenoma (only characteristic calcifications may exclude malignancy)
- The likelihood of malignancy increases with number of lobulations
clinical size of mass > radiographic size (Le Borgne's law)
Asymmetric density = star-shaped lesion
- distinct central tumor mass with volumetric rather than planar appearance (additional coned compression views!)
- denser relative to other areas (= vessels + trabeculae cannot be seen within high-density lesion)
- fat does not traverse density
- corona of spicules
- in any quadrant (but fatty replacement occurs last in upper outer quadrant)
DDx: postsurgical fibrosis, traumatic fat necrosis, sclerosing duct hyperplasia Microcalcifications
associated with malignant mass by mammogram in 40%, pathologically with special stains in 60%, on specimen radiography in 86%
- 20% of clustered microcalcifications represent a malignant process!
shape: fragmented, irregular contour, polymorphic, casting rod-shaped without polarity, Y-shaped branching pattern, granular salt and pepper pattern, reticular pattern
density: various densities
size: 100 300 m (usually); rarely up to 2 mm
distribution: tight cluster over an area of 1 cm2 or less is most suggestive; coursing along ductal system seen in ductal carcinoma with comedo elements
Architectural distortion
Cause: desmoplastic reaction - ragged irregular border
DDx: postsurgical fibrosis Interval change
neodensity = de novo developing density (in 6% malignant)
enlarging mass (malignant in 10 15%)
Enlarged single duct
(low probability for cancer in asymptomatic woman with normal breast palpation)
- solitary dilated duct >3 cm long
DDx: inspissated debris/blood, papilloma Diffuse increase in density (late finding)
Cause: (1) plugging of dermal lymphatics with tumor cells
(2) less flattening of sclerotic + fibrous elements of neoplasm in comparison with more compressible fibroglandular breast tissue
P.562
Nonlocalizing Signs of Breast Cancer
= Secondary Signs Of Breast Cancer
Asymmetric thickening
Asymmetric ducts
especially if discontinuous with subareolar area
Skin changes
skin retraction = dimpling of skin
Cause: desmoplastic reaction causes shortening of Cooper ligaments/direct extension of tumor to skin DDx: trauma, biopsy, abscess, burns skin thickening secondary to blocked lymphatic drainage/tumor in lymphatics
peau d'orange
DDx: normal in inframammary region Nipple/areolar abnormalities
retraction/flattening of nipple
DDx: normal variant Paget disease = eczematoid appearance of nipple + areola in ductal carcinoma
- associated with ductal calcifications toward the nipple
DDx: nipple eczema nipple discharge
spontaneous persistent discharge
need not be bloody
DDx: lactational discharge Abnormal veins
venous diameter ratio of >1.4:1 in 75% of cancers; late sign + thus not very important
Axillary nodes (sign of advanced/occult cancer)
- >1.5 cm without fatty center
DDx: reactive hyperplasia
Location of Breast Masses
benign + malignant masses are of similar distribution
@ upper outer quadrant (54%)
@ upper inner quadrant (14%)
@ lower outer quadrant (10%)
@ lower inner quadrant (7%)
@ retroareolar (15%)
- Mediolateral oblique view is important part of screening because it includes largest portion of breast tissue + considers most common location of cancers!
Metastatic Breast Cancer
@ Axillary lymph adenopathy
Incidence: 40 74% Risk for positive nodes: 30% if primary >1 cm,
15% if primary <1 cm@ Bone
@ Liver
Incidence: 48 60% US:
- hypoechoic (83%)/hyperechoic (17%) masses
Screening of Asymptomatic Patients
Definition of screening (World Health Organization):
A screening test must
be adequately sensitive and specific
be reproducible in its results
identify previously undiagnosed disease
be affordable
be acceptable to the public
include follow-up services
Guidelines of American Cancer Society, American College of Radiology, American Medical Association, National Cancer Institute:
Breast self-examination to begin at age 20
Breast examination by physician every 3 years between 20 40 years, in yearly intervals after age 40
Baseline mammogram between age 35 40; follow-up screening based upon parenchymal pattern + family Hx
Initial screening at 30 years if patient has first-degree relative with breast cancer in premenopausal years; follow-up screening based upon parenchymal pattern
Mammography at yearly intervals after age 40
All women who have had prior breast cancer require annual follow-up
Additional recommendations:
Screening at 2-year intervals for women >70 years
Baseline mammogram 10 years earlier than age of mother/sister when their cancer was diagnosed
Rate of detected abnormalities:
30 abnormalities in 1,000 screening mammograms:
20 23 benign lesions 7 10 cancers
Acceptable recall rate for screening examination:
10% for initial prevalence screening;
5% for subsequent incidence screening
Interval cancers:
10 20% of cancers surface between annual screenings
Role of Mammography
Overall detection rate:
58 69%; 8% if <1 cm in size
Mammographic accuracy:
88% correctly diagnosed by radiologist 27% detected only by mammography 8% misinterpretations 4% not detected 15 30% positive predictive value (national average):
25% PPV for women in 5th decade
50% PPV for women in 8th decade
Value of Screening Mammography
Indication:
decrease in cancer mortality through earlier detection + intervention when tumor size small + lymph nodes negative; tumor grade of no prognostic significance in tumors <10 mm in size
Health Insurance Plan (HIP) 1963 1969
randomized controlled study of 62,000 women aged 40 64
25 30% reduction in mortality in women >50 years (followed for 18 years)
25% reduction in mortality in women 40 49 years (followed for 18 years); no significant effect at 5- and 10-year follow-up
19% of cancers found by mammography alone
61% of cancers found at physical examination
effectiveness of screening <50 years of age is uncertain
P.563
Breast Cancer Detection Demonstration Project (BCDDP) 1973 1980
4,443 cancers found in 283,000 asymptomatic volunteers
41.6% of cancers found by mammography alone (77% with negative nodes)
8.7% of cancers found by physical examination alone
59% of noninfiltrating cancers found by mammography alone
25% of cancers were intraductal (vs. 5% in previous series)
21% of cancers found in women aged 40 49 years (mammography alone detected 35.4%)
51% of cancers found with both mammography + physical examination
Two-county Swedish trial 1977 1990
randomized controlled study of 78,000 women in study group + 56,700 in control group aged 40 74 years
single MLO mammogram at 2-year intervals for women <50 years of age
single MLO mammogram at 3-year intervals for women 50 years of age
40% reduction in mortality at 7 years in women 50 74 years
0% reduction in mortality at 7 years in women 40 49 years
Metaanalysis of combined results of 5 Swedish trials for women aged 39 49
29% reduction in breast cancer mortality with screening mammograms offered at intervals from 18 to 28 months
Occult versus Palpable Breast Cancer
- 27% are occult cancers (NO age difference)
Positive axillary nodes:
occult cancers (19%); palpable cancers (44%)
10-year survival:
occult cancers (65%); palpable cancers (25%)
Mammographically Missed Cancers
False-negative screening mammogram:
= pathologic diagnosis of breast cancer within 1 year after negative mammogram with the following types of misses:
lesion could not be seen in retrospect (25 33%) = acute cancer = cancer surfacing in screening interval
cancer undetected by first reader but correctly identified by second reader (14%)
cancer visible in retrospect on prior mammogram (61%)
Incidence: approx. 4 15 34% of all cancers; approx. 3 cancers:2,000 mammograms; 5 15 22% of palpable breast cancers - A second reader will detect an additional 5 15% of cancers!
Cause:
Interpretation error (52%):
benign appearance (18%): medullary carcinoma, colloid carcinoma, intracystic papillary carcinoma, some infiltrating ductal carcinomas
present on previous mammogram (17%)
seen on one view only (9%)
site of previous biopsy (8%)
Observer error (30 43%):
overlooked
presence of an obvious finding leads to overlooking of a more subtle lesion = satisfied search phenomenon
no knowledge of clinical finding
rushed interpretation
heavy caseload
extraneous distraction
eye fatigue
inexperience
Technical error (5%):
inadequate radiographic technique: improper positioning, inadequate compression, under- /overexposed image, poor screen-film contact, geometric motion blurring
failure to image region of interest
suboptimal viewing conditions: inadequate luminance of view boxes, extraneous view box light, high ambient room light
Tumor biology:
small tumor size
failure to incite desmoplastic reaction
(eg, invasive lobular carcinoma)
limitations of screen-film mammography in physically dense breasts
no associated microcalcifications
(approx. 50% of cancers)
developing soft-tissue radiopacity
stability of mammographic findings
- Malignant calcifications may be stable for up to 63 months
- A mass may not change for up to 4.5 years
Location of missed cancers:
retroglandular area (33%), lateral parenchyma (31%), central (18%), medial (13%), subareolar (4%)
Radiation-induced Breast Carcinoma
Lifetime risk with cumulative carcinogenic effect related to age!
women age <35: 7.5 additional cancers per 1 million irradiated women per year per rad
women age >35: 3.5 additional cancers per 1 million irradiated women per year per rad
P.564
Role of Breast Ultrasound
Indications:
- Ultrasound is no screening tool!
TARGETED EXAM
Initial study of palpable lump in patient <30 years of age/pregnant/lactating
- Ultrasound will not add useful information in an area that contains only fatty tissue on a mammogram!
Characterization of mammographic/palpable mass as fluid-filled/solid
- Ultrasound will add useful information if there is water-density tissue in the area of palpable abnormality!
- Differentiation of cystic from solid lesion is the principal role of ultrasound!
additional evaluation of nonpalpable abnormality with uncertain mammographic diagnosis
search for focal lesion as cause for mammographic asymmetric density
confirmation of lesion seen in one mammographic projection only
WHOLE-BREAST EXAM
Breast secretions
Suspected leaks from silicone implant
Follow-up of multiple known mammographic/sonographic lesions
Radiographically dense breast with strong family history of breast cancer
Metastases thought to be of breast origin, but with negative clinical + mammographic exam
Mammography not possible: radiophobic patient, bedridden patient, after mastectomy
interventional PROCEDURE
Ultrasound-guided cyst aspiration
Ultrasound-guided core biopsy
Ultrasound-guided ductography, if
secretions cannot be expressed
duct cannot be cannulated
| Accuracy: | 98% accuracy for cysts; 99% accuracy for solid masses; small carcinomas have the least characteristic features |
Role of Breast MRI
Indications:
young patient with positive BCRCA screen
dense breast + high-risk lesion of LCIS
palpable mass + negative mammo- + sonogram
axillary node malignancy + negative mammogram
planning for biopsy to determine scar versus tumor
staging:
tumor size: MRI more accurate in estimate of tumor size than mammography/ultrasound
detection of extensive intraductal component: MRI superior to mammography
multifocality (25 50%):
in 70% detected by MRI only
multicentricity(15 30%):
in 50% detected by MRI only
bilaterality (5%):
in 75% detected by MRI only
before + after 2nd cycle of neoadjuvant chemotherapy to separate responders from nonresponders
chest wall invasion
status post lumpectomy with positive margins
status post mastectomy + breast reconstruction with implant (yearly screening)
implant imaging
repeated indeterminate mammogram
| Sensitivity: | 72 93 100% |
- A normal MR mammogram
correctly rules out malignancy in >96%
means no invasive cancer >3 mm
means no further exam for 2 years (for 1 year if BRCA positive)
may miss: DCIS, LCIS, lobular cancer, tubular cancer
| Timing of MR: | 7 20 days after beginning of cycle; 6 months after open biopsy; 12 months after radiation therapy |
MR:
- Malignant morphology always trumps kinetics!
- reduced signal on T2WI
- irregular morphology
- lymphangitic bridges/streaks
- contrast enhancement:
- rapid increase in signal intensity after contrast injection = rapid wash-in
- 90/90 rule = cancers show an SI increase of >90% in the first 90 seconds!
- markedly higher amplitude than normal parenchymal tissue
- plateau/fast wash-out in postinitial phase
- arterial feeder sign
- intense early rim/peripheral enhancement ( central necrosis)
- centripetal progression of enhancement
- malignant mass margination
Slowly/Nonenhancing Breast Cancer on MRI
Lobular carcinoma
Tubular carcinoma
Mucinous carcinoma
Grade I invasive ductal carcinoma
Indication for Screening Breast Mri (if score > 2.0)
| History | Score |
|---|---|
| BRCA 1 or | 2 2.0 |
| Personal history of breast/ovarian cancer | 2.0 |
| Breast cancer in mother <60 years | 1.0 |
| Breast cancer in sibling <60 years | 0.5 |
| Menstruation >35 years | 0.5 |
| Nulliparous | 0.5 |
| First pregnancy >30 years | 0.5 |
| Breast cancer in first-degree relative (nonsibling) | 0.5 |
| Ashkenazi Jew | 0.5 |
| Dense breast | 0.5 |
P.565
BI-RADS Score for Breast MRI
| Descriptor | Score | |
|---|---|---|
| Major feature | ||
| Peak enhancement in 90-seconds | 2.0 | |
| Centripetal wash-in | 2.0 | |
| Spiculated lesion | 2.0 | |
| Rapid wash-out | 2.0 | |
| T2 isointense mass | 1.0 | |
| Initial contrast uptake >100% | 1.0 | |
| Minor feature | ||
| Perilesional edema (T2/STIR) | 1.0 | |
| Branching lesion | 1.0 | |
| Dendritic configuration adjacent to primary | 1.0 | |
| Heterogeneous lesion on T2 | 1.0 | |
| Size of lesion >10 mm | 0.5 | |
| Lobulated margins of lesion | 0.5 | |
| Interpretation | ||
| Compatible with malignancy | >7 | |
| Probably malignant | >5 | |
| Indeterminate | 3 5 | |
| Probably benign | <3 | |
| Compatible with benignity | <1 |
Role of Stereotactic Biopsy
| Indications: | obviously malignant nonpalpable lesion, indeterminate likely benign lesion, anxiety over lesion |
| Targets: | well-defined solid mass, indistinct/spiculated mass, clustered microcalcifications |
| Advantage: | single-stage surgical procedure |
| Problematic: | 3 5-mm small lesion, fine scattered microcalcifications, indistinct density, area of architectural distortion |
Excision:
radial scar suspected (in up to 28% associated with tubular carcinoma), lesion close to chest wall, lesion in axillary tail, very superficial lesion, atypia/atypical hyperplasia (in 49 61% associated with malignancy), carcinoma in situ (in 9 20% associated with invasion), branching microcalcifications suggestive of DCIS with comedo necrosis
| Sensitivity: | 85 99% with core needle biopsy (100% specific), 68 93% with fine-needle aspiration (88 100% specific) |
| Miss rate: | 3 8% for stereotactic biopsy, 3% for surgery |
Breast Cyst
| Incidence: | most common single cause of breast lumps between 35 and 55 years of age |
| Age: | any; most common in later reproductive years + around menopause |
| Histo: | cyst wall lined by single layer of (a) flattened epithelial cells; cyst fluid with Na+/ K+ ratio 3 (b) epithelial cells with apocrine metaplasia (secretory function); cyst fluid with Na+/K+ ratio <3 |
| Cause: | fluid cannot be absorbed due to obstruction of extralobular terminal duct by fibrosis/intraductal epithelial proliferation |
size changes over time
Simple Breast Cyst
- well-defined flattened oval/round (if under pressure) mammographic mass + surrounding halo (DDx: well-defined solid mass)
- solitary/multiple
- needle aspiration of fluid (proof) + postaspiration mammogram as new baseline
US (98 100% accuracy):
- Correlate with palpation/mammogram as to size, shape, location, surrounding tissue density!
- spherical/ovoid lesion with anechoic center
- well-circumscribed thin echogenic capsule
- posterior acoustic enhancement (may be difficult to demonstrate in small/deeply situated cysts)
- thin edge shadows
- occasionally multilocular thin septations/cluster of cysts
MR:
T1WI:
- well-circumscribed hypointense lesion without discernible cyst wall; well seen within adipose parenchyma; poorly seen in normal parenchyma
enhanced T1WI:
- no change in signal intensity; improved demarcation due to enhancement of surrounding parenchyma
T2WI:
- well-circumscribed hyperintense lesion with homogeneous internal texture (detectable at a diameter of ~ 2 mm)
Pneumocystogram (for symptomatic cysts)
- air remains mammographically detectable for up to 3 weeks
- therapeutic effect of air insufflation (equal to 60 70% of aspirated fluid volume): no cyst recurrence in 85 94% (40 45% cyst recurrence without air insufflation)
Complex/Complicated Breast Cyst
= any cyst that does not meet criteria of simple cyst
| Cause: | fibrocystic changes (vast majority), infection, malignancy (extremely rare) 0.3% of all breast cancers are intracystic |
- Patients with apocrine cysts are at greater risk to develop breast cancer!
- uniformly thick wall + tenderness = inflammation/infection
- diffuse low-level internal echoes (= foam cyst):
with mobility upon increase in power output
= subcellular material like protein globs, floating cholesterol crystals, cellular debris
without mobility upon increase in power output = cells like foamy macrophages, apocrine metaplasia, epithelial cells, pus, blood
- fluid-debris level
Rx: aspiration to rule out blood/pus P.566
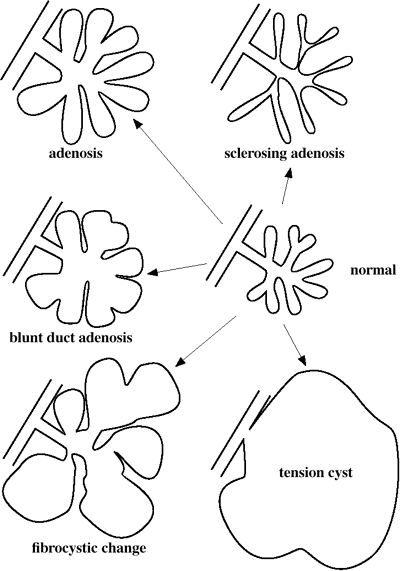
Benign Disease of the Terminal Ductal Lobular Unit - thick septation/eccentric wall thickening
further characterized by protruding ill-defined outer margin, convex microlobulated inner margin ( mural nodule ), nonmobile mass with coarse heterogeneous echotexture, CD flow within thickening
Rx: treated like solid nodule - spongelike cluster of microcysts
Rx: treated like solid nodule MR:
T1WI:
- hyper-/isointense cyst content (hemorrhage) sign of sedimentation
enhanced T1WI:
- thick ring-enhancing cyst wall (inflammation)
- slight contrast uptake in surrounding tissue (= reactive hyperemia)
| Rx: | complete aspiration (assures benign cause), core needle biopsy (if partially/nonaspiratable) |
| DDx: | artifactual scatter in superficial/deep small cysts, fibroadenoma, papilloma, carcinoma |
Cyst Aspiration
inspection of cyst fluid:
normal: turbid greenish/grayish/black fluid
abnormal: straw-colored clear fluid/dark blood
- needle moves within nonaspiratable complex cyst
- fluid without blood should be discarded
- bloody fluid should be examined cytologically
Carcinoma Of Male Breast
| Incidence: | 0.2%; 1,400 new cases/year with 300 deaths 3.7% of male breast carcinomas occur in men with Klinefelter syndrome! |
| Peak age: | 60 69 years |
| At risk: | (males with increased estrogen levels) |
Klinefelter syndrome (20-fold risk over normals):
XXY chromosomes
Liver disease: cirrhosis, schistosomiasis, malnutrition
Radiation therapy to chest (latent period of 12 35 years)
Occupational heat exposure (diminished testicular function)
Testicular atrophy: injury, mumps orchitis, undescended testes
Jewish background
Family history in male/female (in up to 30%)
- Gynecomastia is NOT a risk factor!
| Histo: | same as in females; infiltrating ductal carcinoma (majority); invasive lobular carcinoma distinctly uncommon (tubular structures usually not found in male breast) |
firm painless retroareolar/upper-outer-quadrant mass
breast swelling, bloody nipple discharge, retraction
| Location: | L > R breast; bilaterality is uncommon |
- resembles scirrhous carcinoma of female breast
- usually located eccentrically
- calcifications fewer + more scattered + more round + larger
- enlarged axillary nodes (in 50% at time of presentation)
- metastases to pleura, lung, bone, liver
| Delay in diagnosis from onset of symptoms: | 6 18 months |
| Rx: | surgery, hormonal manipulation (85% estrogen receptor and 75% progesterone receptor positive) |
| Prognosis: | 5-year survival rate for stage 1 = 82 100%, for stage 2 = 44 77%, for stage 3 = 16 45%, for stage 4 = 4 8% (same as for women!) |
| DDx: | breast abscess, gynecomastia, epidermal inclusion cyst |
Chronic Abscess of Breast
COLD ABSCESS usually seen in lactating women
fever, pain, increased WBC (clinical diagnosis)
rapid response to antibiotics
| Location: | most commonly in central/subareolar area |
- ill-defined mass of increased density with flamelike contour
- secondary changes common: architectural distortion, nipple + areolar retraction, lymphedema, skin thickening, pathologic axillary nodes
- liquefied center can be aspirated
US:
- anechoic/nearly anechoic area with posterior enhancement
MR:
T1WI:
- hyperintense round/ovoid lesion (high protein content)
enhanced T1WI:
- no contrast uptake centrally
- strong enhancement of abscess wall
T2WI:
- hyperintense round/oval lesion
P.567
| DDx: | seroma |
Phyllodes tumor
| Incidence: | 1: 6,300 examinations; 0.3 1.5% of all breast tumors; 3% of all fibroadenomas |
| Age: | 5th-6th decade (mean age of 45 years, occasionally in women >20 years of age |
| Histo: | similar to fibroadenoma but with increased cellularity + pleomorphism (wide variations in size, shape, differentiation) of its stromal elements; fibroepithelial tumor with leaflike (phylloides) growth pattern = branching projections of tissue into cystic cavities; cavernous structures contain mucus; cystic degeneration + hemorrhage |
sense of fullness
rapidly enlarging breast mass; periods of remission
huge, firm, mobile, discrete, lobulated, smooth mass
thinning + livid discoloration of skin, wide veins, shining skin
large homogeneous noncalcified mass with smooth
polylobulated margins mimicking fibroadenoma
rapid growth to large size (>6 10 cm), may fill entire breast
occasional halo sign (due to compression of surrounding tissue)
US:
- round/lobulated tumor with well-demarcated border
- posterior acoustic shadow
- fluid-filled clefts in large tumors
MR:
T1WI:
- hypo-/isointense to parenchyma
- hypointense regions of cystic/necrotic changes (occasionally)
enhanced T1WI:
- strong initial uptake in solid tumor component
- continuous increase/plateau in postinitial phase
- increasing demarcation of nonenhancing cystic components (mass-in-mass morphology)
T2WI:
- iso - to hyperintense to parenchyma
- hyperintense regions of cystic/necrotic changes (occasionally)
| DDx: | fibroadenoma |
Benign Phyllodes tumor
= FIBROADENOMA PHYLLODES = GIANT FIBROADENOMA
= benign giant form of intracanalicular fibroadenoma
| Histo: | low mitotic activity (0 4 mitoses/10 HPF) |
| Cx: | in 5 10% degeneration into malignant fibrous histiocytoma/fibrosarcoma/liposarcoma/chondrosarcoma/osteosarcoma with local invasion + hematogenous metastases to lung, pleura, bone (axillary metastases quite rare) |
| Prognosis: | 15 20% recurrence rate if not completely excised |
Malignant Phyllodes Tumor
= CYSTOSARCOMA PHYLLODES = ADENOSARCOMA
| Histo: | high mitotic activity (>5 mitoses/10 HPF) in a predominantly sarcomatous differentiation |
| Prognosis: | hematogenous spread in 20% |
Dermatopathic Lymphadenopathy
= benign reactive lymphadenopathy within breast associated with cutaneous rashes
| Cause: | exfoliative dermatitis, erythroderma, psoriasis, atopic dermatitis, skin infection) |
| Histo: | follicular pattern retained, germinal centers enlarged, enlarged paracortical area with pale-staining cells (lymphocytes, Langerhans cells, interdigitating reticulum cells) |
mobile nontender firm subcutaneous nodules
| Location: | often bilateral |
| Site: | predominantly upper outer quadrant |
- regional subcentimeter masses with central/peripheral radiolucent notches
Epidermal Inclusion Cyst
= benign cutaneous/subcutaneous lesion
| Cause: | congenital, metaplasia, trauma (needle biopsy, reduction mammoplasty), obstructed hair follicle |
| Path: | cyst filled with keratin |
| Histo: | stratified squamous epithelium |
smooth round nodule attached to skin with blackened pore, movable against underlying tissue
- circumscribed round/oval iso-/high-density mass of 0.8 10.0 cm in diameter
- may contain heterogeneous microcalcifications
US:
- circumscribed hypoechoic solid mass extending into dermis
| DDx: | sebaceous cyst (epithelial cysts containing sebaceous glands) |
Fat Necrosis of Breast
= TRAUMATIC LIPID CYST = OIL CYST
= aseptic saponification of fat by tissue lipase after local destruction of fat cells with release of lipids + hemorrhage + fibrotic proliferation
| Etiology: | direct external trauma (seat belt injury), breast biopsy, reduction mammoplasty, implant removal, breast reconstruction, irradiation, nodular panniculitis (Weber-Christian disease), ductal ectasia of chronic mastitis, foreign body reaction (silicone, paraffin) |
| Incidence: | 0.5% of breast biopsies |
| At risk: | middle-aged obese women with fatty pendulous breasts |
| Histo: | cavity with oily material surrounded by foam cells (= lipid-laden macrophages) |
history of trauma in 40% (eg, prior surgery, radiation >6 months ago, reduction mammoplasty, lumpectomy)
usually clinically occult
firm, slightly fixed tender/painless mass
skin retraction (50%)
yellowish fatty fluid on aspiration
| Location: | anywhere; more common in superficial periareolar region; near biopsy site/surgical scar |
- early: ill-defined irregular spiculated dense mass (indistinguishable from carcinoma if associated with distortion, skin thickening, retraction)
- later:well-circumscribed mass with translucent areas at center (= homogeneous fat density of oil cyst) surrounded by thin pseudocapsule (in old lesions)
- calcifies in 4 7% (= liponecrosis macrocystica calcificans):
- occasionally curvilinear/eggshell calcification in wall
- fine spicules of low density vary with projection
- localized skin thickening/retraction possible
P.568
US:
- hypo-/anechoic mass with ill-/well-defined margins acoustic shadowing
- complex cyst with mural nodules/echogenic bands
MR:
T1WI:
- signal intensity equal to parenchyma
- round lesion with hyperintense fat signal (oil cyst)
- signal loss with macrocalcifications
enhanced T1WI:
- localized ill-defined area of moderate enhancement + continuous postinitial increase (granulation tissue) within 6 months after trauma
- no enhancement in late lesion/oil cyst
T2WI:
- ill-defined hyperintense area (reactive edema of fresh lesion)
- round lesion with central signal intensity of fat (in oil cyst)
Weber-Christian Disease
= nonsuppurative panniculitis with recurrent bouts of inflammation = areas of fat necrosis, involving subcutaneous fat + fat within internal organs
accompanied by fever + nodules over trunk and limbs
Fibroadenoma
= ADULT-TYPE FIBROADENOMA
= estrogen-induced benign tumor originating from TDLU; forms during adolescence; pregnancy + lactation are growth stimulants; regression after menopause (mucoid degeneration, hyalinization, involution of epithelial components, calcification)
| Incidence: | 3rd most common type of breast lesion after fibrocystic disease + carcinoma; most common benign solid tumor in women of childbearing age (~10%) |
| Age: | mean age of 30 years (range 13 80 years); median age 25 years; most common breast tumor under age 25 years |
Hormonal influence:
slight enlargement at end of menstrual cycle + during pregnancy; regresses after menopause; may occur in postmenopausal women receiving estrogen replacement therapy
| Histo: | mixture of proliferated fibrous stroma + epithelial ductal structures (a) intracanalicular fibroadenoma compressing ducts (b) pericanalicular fibroadenoma without duct compression (c) combination Cellular FA = predominantly epithelial elements in younger women Fibrous FA = predominantly fibrotic elements in older women |
firm, smooth, sometimes lobulated, freely movable mass
in 35% not palpable
NO skin fixation
rarely tender/painful
clinical size = radiographic size
| Size: | 1 5 cm (in 60%) |
| Location: | multifocal in 15 25%; bilateral in 4% |
- circular/oval-shaped lesion of low density
- nodular/lobulated contour when larger (areas with different growth rates)
- smooth, discrete margins (indistinguishable from cysts when small)
- often with halo sign
- smoothly contoured calcifications of high + fairly equal density in 3% due to necrosis from regressive changes in older patients:
peripheral subcapsular myxoid degeneration
- peripheral marginal ringlike calcifications
central myxoid degeneration
- popcorn type of calcification (PATHOGNOMONIC)
calcifications within ductal elements
- pleomorphic linear branching pattern
- Calcifications enlarge as soft-tissue component regresses!
US:
- round (3%)/oval mass (96%) with length-to-depth ratio of >1.4 (in carcinomas usually <1.4)
- hypoechoic similar to fat lobules (80 96%)/hyperechoic/mixed pattern/anechoic/isoechoic compared with adjacent fibroglandular tissue
- homogeneous (48 89%)/inhomogeneous (12 52%) texture
- regular (57%)/lobulated (15 31%)/irregular (6 58%) contour
- hump and dip sign = small focal contour bulge immediately contiguous with a small sulcus (57%)
- intratumoral bright echoes (10%) = macrocalcifications
- posterior acoustic enhancement (17 25%)/acoustic shadow without calcifications (9 11%)
- echogenic halo (capsule) with lateral shadowing
- slight compressibility of tumor
MR:
T1WI:
- iso-/mildly hypointense compared to parenchyma
- more obvious in fatty tissue
- endotumoral signal loss due to macrocalcifications
enhanced T1WI:
- very strong enhancement (with proportionately larger epithelial component)
- postinitial continuous increase/plateau
- endotumoral septa with mild contrast uptake
T2WI:
- high signal intensity (for tumor with proportionately larger epithelial component)
- occasionally endotumoral septations (caused by fibrotic component)
- iso-/slightly hypointense compared to breast parenchyma (for predominantly fibrotic tumor)
| DDx: | adenosis tumor/florid adenosis |
Juvenile/Giant/Cellular Fibroadenoma
= fibroadenoma >5 cm in diameter/weighing >500 g
| Cause: | hyperplasia + distortion of normal breast lobules secondary to hormonal imbalances between estradiol + progesterone levels |
| Age: | any (mostly in adolescent girls) |
| Histo: | more glandular + more stromal cellularity than adult type of fibroadenoma; ductal epithelial hyperplasia |
P.569
rapidly enlarging well-circumscribed nontender mass
dilated superficial veins, stretched skin
- discrete mass with rounded borders
MR:
T1WI:
- iso- to slightly hypointense round/oval mass difficult to separate from normal breast parenchyma
enhanced T1WI:
- strong enhancement with sharp demarcation from surrounding tissue + endotumoral septations
T2WI:
- typically hyperintense
| DDx: | medullary/mucinous/papillary carcinoma/carcinoma within fibroadenoma |
Fibrocystic Changes
MAZOPLASIA = MASTITIS FIBROSA CYSTICA = CHRONIC CYSTIC MASTITIS = CYSTIC DISEASE = GENERALIZED BREAST HYPERPLASIA = DESQUAMATED EPITHELIAL HYPERPLASIA = fibroadenomatosis = MAMMARY DYSPLASIA = Schimmelbusch DISEASE = FIBROUS MASTITIS = MAMMARY PROLIFERATIVE DISEASE
- Not a disease since found in 72% of screening population >55 years of age
- The College of American Pathologists suggests use of the term fibrocystic changes/condition in mammography reports!
| Incidence: | most common diffuse breast disorder; in 51% of 3,000 autopsies |
| Age: | 35 55 years |
| Etiology: | exaggeration of normal cyclical proliferation + involution of the breast with production + incomplete absorption of fluid by apocrine cells due to hormonal imbalance |
asymptomatic in macrocystic disease
fullness, tenderness, pain in microcystic disease
palpable nodules + thickening
symptoms occur with ovulation; regression with pregnancy + menopause
Histo:
overgrowth of fibrous connective tissue = stromal fibrosis, fibroadenoma
cystic dilatation of ducts + cyst formation (in 100% microscopic, in 20% macroscopic)
hyperplasia of ducts + lobules + acini = adenosis; ductal papillomatosis
- individual round/ovoid cysts with discrete smooth margins
- lobulated multilocular cyst
- enlarged nodular pattern (= fluid-distended lobules + extensive extralobular fibrous connective tissue overgrowth)
- teacup-like curvilinear thin calcifications with horizontal beam + low-density round calcifications in craniocaudal projection = milk of calcium (4%)
- oyster pearl like /psammoma-like calcifications
- involutional type calcifications = very fine punctate calcifications evenly distributed within one/more lobes against a fatty background (from mild degree of hyperplasia in subsequently atrophied glandular tissue)
US:
- ductal pattern, ductectasia, cysts, ill-defined focal lesions
MR:
T1WI:
- hypointense compared to intramammary adipose tissue
- interspersed hypointense cysts of varying sizes
enhanced T1WI:
- patchy to diffuse increased enhancement (correlating with degree of adenosis)
- Avoid scheduling patient during 1st and 4th week of menstrual cycle/under HRT
- continuous rise after postinitial phase
T2WI:
- occasionally diffusely increased signal intensity (in 2nd half of menstrual cycle/under HRT)
- interspersed hyperintense cysts of varying sizes
Risk for invasive breast carcinoma:
NO INCREASED RISK (70%)
Nonproliferative lesions: adenosis, florid adenosis, apocrine metaplasia without atypia, macro-/microcysts, duct ectasia, fibrosis, mild hyperplasia (more than 2 but not more than 4 epithelial cells deep), mastitis, periductal mastitis, squamous metaplasia
Fibroadenoma
SLIGHTLY INCREASED RISK (1.5 2 times):
Moderate + florid solid/papillary hyperplasia
Papilloma with fibrovascular core
Sclerosing adenosis
MODERATELY INCREASED RISK (5 times):
Ductal/lobular atypical hyperplasia (borderline lesion with some features of carcinoma in situ)
HIGH RISK (8 11 times):
Atypical hyperplasia + family history of breast cancer
Ductal/lobular carcinoma in situ
Adenosis
| Age: | all |
| Path: | lobulocentric lesion derived from TDLU with distortion and effacement of underlying lobules |
| Histo: | epithelial and myoepithelial proliferation of ductules + lobules with nuclear pleomorphism + increase in cell size |
- increase in size of TDLUs to 3 7 mm
- snowflake pattern of widespread ill-defined nodular densities
- often round intralobular microcalcifications/milk of calcium (less common + less extensive than in sclerosing adenosis)
US:
- adenosis lobules are sonographically iso- to mildly hypoechoic compared with fat
MR:
- no abnormalities on T1WI/T2WI
- usually strong, occasionally branching contrast uptake in focal areas of adenosis
| DDx: | malignancy |
Sclerosing Adenosis
| Path: | myoepithelial proliferation + reactive stromal fibrosis |
| Histo: | stromal sclerosis involving >50% of all TDLUs, which become elongated + distorted + compressed by sclerosis |
| DDx: | tubular carcinoma (absence of basement membrane + myoepithelial cells); radial scar (more extensive fibrosis + central fibrocollagenous scar) |
P.570
palpable mass (rare) = adenosis tumor
| Rarely associated with: | lobular carcinoma in situ > ductal carcinoma in situ |
- Sclerosing adenosis is not a risk factor/precursor of breast cancer
- calcifications in 50%
focal form
- focal cluster of microcalcifications
- focally dense breast appearing as a nodule/spiculated lesion
diffuse form
- adenosis + diffusely scattered calcifications (calcifications in cystically dilated acinar structure)
- diffusely dense breast
| DDx: | other spiculated lesions |
Adenosis Tumor = Florid Adenosis
| Average age: | 30 years |
| Histo: | focal proliferation of ductules and lobular glands with hyperplasia of epithelial + myoepithelial cells |
firm clinically discrete/ill-defined mass
- nodular mass usually <2 cm in diameter
- microcalcifications
| DDx: | fibroadenoma |
Fibrosis
- round/oval clustered microcalcifications with smooth contours + associated fine granular calcifications filling lobules
Atypical Lobular Hyperplasia
= proliferation of round cells of LCIS type growing along terminal ducts in permeative fashion (pagetoid growth) between benign epithelium + basal myoepithelium BUT NOT completely obliterating terminal ductal lumina/distending lobules (as in lobular carcinoma in situ)
- no mammographic correlate
Atypical Ductal Hyperplasia
= low-grade intraductal proliferation with partial/incompletely developed features of noncomedo DCIS
- frequent calcifications
Classification of Fibrocystic Changes
| Grade | Frequency | Histological Category | Breast Cancer Risk |
|---|---|---|---|
| I | 70% | Nonproliferative lesion | 0 |
| II | 25% | Proliferative lesion without atypia | 2x |
| III | 5% | Proliferative lesion with atypia | 4 5x |
Intraductal Papillomatosis
= hyperplastic polypoid lesions within a duct
| Age: | perimenopausal |
spontaneous bloody/serous/serosanguinous nipple discharge (most common cause of nipple discharge)
- small retroareolar opacity (= dilated duct) extending 2 3 cm into breast
- intraluminal filling defect on galactography
Fibrous Nodule Of The Breast
= FIBROUS DISEASE OF THE BREAST = FIBROUS DISEASE = FIBROSIS OF THE BREAST = FIBROUS MASTOPATHY = FIBROUS TUMOR OF THE BREAST
| Frequency: | 3 4% of benign masses; 8% of surgical breast specimens |
| Histo: | focally dense collagenous stroma surrounding atrophic epithelium; NONSPECIFIC |
| Age: | 20 50 years; only 8% postmenopausal |
palpable/nonpalpable mass: edge merges into surrounding dense tissue
| Location: | unilateral (80 85%)/bilateral (15 20%) |
- circumscribed (55%)/indistinct (32%) margin
- suggestive of malignancy (11%): irregular shape, spiculated margin, posterior acoustic shadowing
| DDx: | fibroadenoma, malignancy |
Galactocele
= retention of fatty material in areas of cystic duct dilatation appearing during/shortly after lactation
| Cause: | ? abrupt suppression of lactation/obstructed milk duct |
| Age: | occurs during/shortly after lactation |
thick inspissated milky fluid (colostrum)
| Location: | retroareolar area |
- large radiopaque lesion of water density (1st phase)
- smaller lesion of mixed density + fat-water level with horizontal beam (2nd phase)
- small radiolucent lesion resembling lipoma
- fluid-calcium level
US:
- complex mass
| Dx: | aspiration of milky fluid |
Granular Cell Tumor
= GRANULAR CELL MYOBLASTOMA (1926)
= benign tumor, occasionally locally invasive + metastasizing
| Origin: | Schwann cell (positive for S-100 marker protein) |
| Prevalence: | 1:1,000 primary breast carcinomas |
| Age: | 20 59 (mean 34) years; 76% for African-Americans |
| Histo: | rounded groups of large polygonal cells with small dark regular nuclei + abundant eosinophilic granular cytoplasm; immunoreactive to S-100 protein |
| DDx: | carcinoma, lymphoma, metastasis Fine-needle aspirate may be difficult to interpret! |
| Location: | tongue (most common), oropharynx, GI tract, skin, bronchial wall, subcutaneous tissue (6 8%), biliary tract (1%) |
| Site: | more commonly other than upper outer quadrant |
asymmetric lump with slow growth, hardness, skin fixation/retraction, ulceration
often fixed to pectoralis fascia
- well-circumscribed spiculated mass 1 3 cm in diameter
P.571
Gynecomastia
benign, usually reversible excessive development of the male breast
- NOT a risk factor for development of breast cancer!
Cause:
Hormonal
Cause: excess estrogens or decreased androgens
neonate: influence from maternal estrogens crossing placenta
puberty: high estradiol levels
Incidence: in up to 60 75% of healthy boys Age: 1 year after onset of puberty (13 14 years) Prognosis: subsides within 1 2 years senescence: decline in serum testosterone levels
hypogonadism (Klinefelter syndrome, anorchism, acquired testicular failure (eg, testicular neoplasm)
tumors: adrenal carcinoma, pituitary adenoma, testicular tumor, hyperthyroidism
Systemic disorders
advanced alcoholic cirrhosis, hemodialysis in chronic renal failure, chronic pulmonary disease (emphysema, TB), malnutrition
Drug-induced
anabolic steroids, estrogen treatment for prostate cancer, digitalis, cimetidine, thiazide, spironolactone, reserpine, isoniazid, ergotamine, marijuana
Neoplasm: hepatoma (with estrogen production)
Idiopathic
| mnemonic: | CODES |
Cirrhosis
Obesity
Digitalis
Estrogen
Spironolactone
| Incidence: | 85% of all male breast masses |
| Age: | neonatal period, adolescent boys (40%), men >50 years (32%) |
| Histo: | increased number of ducts, proliferation of duct epithelium, periductal edema, fibroplastic stroma, adipose tissue |
palpable firm mass >2 cm in subareolar region
| Location: | bilateral (63%), left-sided (27%), right-sided (10%) |
- mild prominence of subareolar ducts in flame-shaped distribution (focal type)
- homogeneously dense breast (diffuse type)
MR:
- hypointense retromamillary area
- no/slight contrast enhancement
| DDx: | pseudogynecomastia (= fatty proliferation in obesity) |
Hamartoma Of Breast
FIBROADENOLIPOMA = LIPOFIBROADENOMA = ADENOLIPOMA
| Incidence: | 2 16:10,000 mammograms |
| Mean age: | 45 (27 88) years |
| Histo: | normal/dysplastic mammary tissue composed of dense fibrous tissue + variable amount of fat, delineated from surrounding tissue without a true capsule |
soft, often nonpalpable (60%)
| Location: | retroareolar (30%), upper outer quadrant (35%) |
- round/ovoid well-circumscribed mass usually > 3 cm
- mixed density with mottled center (secondary to fat) = slice of sausage pattern
- thin smooth pseudocapsule (= thin layer of surrounding fibrous tissue)
- halo sign = peripheral radiolucent zone due to compression of surrounding tissue
- may contain calcifications
MR:
T1WI:
- well-circumscribed round/oval/lobulated lesion with pseudocapsular demarcation:
- intermediate intensity for parenchymal component
- high intensity for lipomatous component
- low intensity for cystic component
enhanced T1WI:
- no/strong enhancement in parenchymal component with continuous postinitial increase (dependent on vascularization)
T2WI:
- intermediate intensity for parenchymal + lipomatous components
- high intensity for cystic component
| DDx: | liposarcoma, Cowden disease |
Hematoma Of Breast
| Cause: | (1) surgery/biopsy (most common) (2) blunt trauma (3) coagulopathy (leukemia, thrombocytopenia) (4) anticoagulant therapy |
- well-defined ovoid mass (= hemorrhagic cyst)
- ill-defined mass with diffuse increased density (edema + hemorrhage)
- adjacent skin thickening/prominence of reticular structures
- regression within several weeks leaving (a) no trace, (b) architectural distortion, (c) incomplete resolution
- calcifications (occasionally)
US:
- hypoechoic mass with internal echoes
MR:
T1WI:
- homogeneous high signal sedimentation (fresh)
- low signal intensity + peripheral ring of high signal (deoxyhemoglobin of subacute hematoma)
enhanced T1WI:
- no uptake within hematoma
- moderate diffuse reactive enhancement surrounding hematoma + continuous postinitial increase
T2WI:
- homogeneous low signal intensity (fresh)
- low signal intensity + peripheral ring of low signal intensity
P.572
Juvenile Papillomatosis
| Path: | many aggregated cysts with interspersed dense stroma |
| Histo: | cysts lined by flat duct epithelium/epithelium with apocrine metaplasia, sclerosing adenosis, duct stasis; marked papillary hyperplasia of duct epithelium with often extreme atypia |
| Mean age: | 23 years (range of 12 48 years) |
localized palpable tumor
family history of breast cancer in 28% (affected first-degree relative in 8%; in one/more relatives in 28%)
| Prognosis: | development of synchronous (4%)/metachronous (4%) breast cancer after 8 9 years. |
| DDx: | fibroadenoma |
Lactating Adenoma
newly discovered painless mass during 3rd trimester of pregnancy/in lactating woman
| Etiology: | ? variant of fibroadenoma/tubular adenoma/lobular hyperplasia or de novo neoplasm |
| Path: | well-circumscribed yellow spherical mass with lobulated surface + rubbery firm texture and without capsule |
| Histo: | secretory lobules lined by granular and foamy to vacuolated cytoplasm + separated by delicate connective tissue |
firm freely movable painless mass
- homogeneously hypoechoic/isoechoic mass
- posterior acoustic enhancement (most)/shadowing
- fibrous septa
| Prognosis: | regression after completion of breast feeding |
| DDx: | breast carcinoma (1:1,300 1:6,200 pregnancies) |
Lipoma Of Breast
usually solitary asymptomatic slow-growing lesion
| Incidence: | extremely rare |
| Histo: | encapsulated tumor containing mature fat cells |
| Mean age: | 45 years + post menopause |
clinically often occult
soft, freely movable, well delineated
- usually >2 cm
- radiolucent tumor easily seen in dense breast; almost invisible in fatty breast
- discrete thin radiopaque line (= capsule), seen in most of its circumference
- displacement of adjacent breast parenchyma
- calcification with fat necrosis (extremely rare)
US:
- hypo- or hyperechoic lesion
MR:
T1WI:
- well-circumscribed hyperintense lesion
- thin hypointense capsule
- no contrast enhancement
T2WI:
- signal intensity equivalent to subcutaneous fat
| DDx: | fat lobule surrounded by trabeculae/suspensory ligaments |
Lymphoma Of Breast
Primary Lymphoma
= extranodal lymphoma of the breast without prior history of lymphoma/leukemia
Prevalence: 0.12 0.53% of all breast malignancies; 2.2% of all extranodal lymphomas asymptomatic
Secondary Lymphoma
- One of the most common type of metastatic lesions in the breast!
fever, pain
| Histo: | B-cell NHL (majority), Hodgkin disease, leukemia (CLL), plasmacytoma |
| Age: | 50 60 years; M < F |
| Location: | right-sided predominance; 13% bilateral |
- well/incompletely circumscribed round/oval lobulated mass/masses
- infiltrate with poorly defined borders
- NO calcifications/spiculations
- skin thickening + trabecular edema
- bilateral axillary adenopathy in 30 50%
US:
- oval/round homo-/heterogeneously hypoechoic mass/masses
- sharply defined/poorly defined borders
- posterior acoustic shadowing/enhancement
| Prognosis: | 3.4% 5-year disease-free survival for all stages; 50% remission rate with aggressive chemotherapy |
| Recurrence: | mostly in contralateral breast/other distant sites |
| DDx: | circumscribed breast carcinoma, fibroadenoma, phylloides tumor, metastatic disease |
Pseudolymphoma
= lymphoreticular lesion as an overwhelming response to trauma
Mammary Duct Ectasia
= PLASMA CELL MASTITIS = VARICOCELE TUMOR OF BREAST = MASTITIS OBLITERANS = COMEDOMASTITIS= PERIDUCTAL MASTITIS = SECRETORY DISEASE OF BREAST
= rare aseptic inflammation of subareolar area
Pathogenesis (speculative):
Stasis of intraductal secretion leads to duct dilatation + leakage of inspissated material into parenchyma giving rise to an aseptic chemical mastitis (periductal mastitis); the extravasated material is rich in fatty acids = nontraumatic fat necrosis
Periductal inflammation causes damage to elastic lamina of duct wall resulting in duct dilatation
| Histo: | ductal ectasia, heavily calcified ductal secretions; infiltration of plasma cells + giant cells + eosinophils |
| Mean age: | 54 years |
often asymptomatic
breast pain, nipple discharge, nipple retraction, mamillary fistula, subareolar breast mass
| Location: | subareolar, often bilateral + symmetric; may be unilateral + focal |
- dense triangular mass with apex toward nipple
- distended ducts connecting to nipple
- periphery blending with normal tissue
- multiple often bilateral dense round/oval calcifications with lucent center + polarity (= orientation toward nipple)
periductal
- oval/elongated calcified ring around dilated ducts with very dense periphery (surrounding deposits of fibrosis + fat necrosis)
intraductal
- fairly uniform linear, often needle-shaped calcifications of wide caliber, occasionally branching (within ducts/confined to duct walls)
- nipple retraction/skin thickening may occur
P.573
| Sequelae: | cholesterol granuloma |
| DDx: | breast cancer |
Mammoplasty
= COSMETIC BREAST SURGERY
Augmentation Mammoplasty
Most frequently performed plastic surgery in USA
| Frequency: | 150,000 procedures in 1993 (70% for cosmetic reasons, 30% for reconstruction); 1.8 million American women have breast implants (estimate) |
Methods:
Injection augmentation (no longer practiced): paraffin, silicone, fat from liposuction
Cx: tissue necrosis resulting in dense, hard, tender breast masses; lymphadenopathy; infection; granuloma formation (= siliconoma) Implants (prepectoral/subpectoral)
spongelike masses of Ivalon, Etheron, Teflon
Silicone elastomer (silastic) smooth/textured shell containing silicone oil/saline: >100 varieties of dimethyl polysiloxane
single lumen of polymerized methyl polysiloxane with smooth/textured outer silicone shell/polyurethane coating
double lumen with inner core of silicone + outer chamber of saline
reverse double-lumen = inner saline-filled lumen surrounded by silicone-filled envelope
triple lumen
expandable implant intraluminal valves = saline injection into port with gradual tissue expansion for breast reconstruction
Location: retroglandular/subpectoral
Autogenous tissue transplantation
(for breast reconstruction) with musculocutaneous flaps: transverse rectus abdominis muscle (TRAM), latissimus dorsi, tensor fasciae latae, gluteus maximus
Mammographic technique for implants:
Two standard views (CC and MLO views) for most posterior breast tissue
- 22 83% of fibroglandular breast tissue obscured by implant depending on size of breast + location of implant + degree of capsular contraction on standard views!
- The false-negative rate of mammography increases from 10 20% to 41% in patients with implants!
Two Eklund (= implant displacement) views (CC and 90 LAT views) for compression views of anterior breast tissue = push-back view = breast tissue pulled anteriorly in front of implant while implant is pushed posteriorly + superiorly thus excluding most of the implant
MR technique for implants:
Physical principle: resonant frequencies of water, fat (~220 Hz lower than water) and silicone (~100 Hz lower than fat) differ
Most effective sequence: inversion recovery (IR), which suppresses fat
with additional suppression of water = pure depiction of silicone
with additional suppression of silicone = pure depiction of saline component
Orientation: axial + sagittal (2 angulations mandatory)
Cx of silicone-gel-filled implant:
Capsular fibrosis (100%)
= normal host response to wall off foreign body
- low-intensity implant shell + fibrous capsule cannot be differentiated on MRI
- physiologic fluid may occupy space between implant shell + fibrous capsule
- radial folds (normal) = hypointense lines emanating from the fibrous capsule-shell junction as wrinkle
- gently undulating circumferential contour (normal)
Contracture (12 20%): more frequent with retroglandular implants; increasing with time
distortion of breast contour
hardening of breast
tightness, pain
- crenulated contour (US helpful)
- capsular calcifications at periphery of prosthesis
- focal bulge = herniation of a locally weakened fibrous capsule
- fibrous capsule delineated by US (unleaked silicone is echolucent)
- extensive periprosthetic calcifications
MR (low specificity):
- rounded implants with transverse diameter < 2x the anteroposterior diameter
- marked thickening of fibrous capsule
- signal-free periprosthetic zone of macrocalcifications
- complete absence of radial folds
- contrast enhancement from granulomatous inflammation
Rx: not health hazard; capsulotomy (release); capsulectomy (removal of scar tissue)
Implant migration
Cause: overdistension of implant pocket at surgery Rupture of prosthesis
= hole/tear in implant shell observed at surgery
Frequency: 0.2 6.0% Prevalence: >50% after 12 years Intact implant: 89% after 5 years, 51% after 12 years, 5% after 20 years Result: total/partial/no collapse of shell P.574
change in contour/location of implant
flattening of implant
breast pain
Gel bleed = silicone leaching (100% = normal condition as all implants bleed)
= leakage of microscopic quantities of silicone oil through semiporous but intact barrier shell made of silicone elastomer
- silicone-equivalent signal within keyhole-shaped terminal bend of radial folds + between capsule and implant shell
Dx: microscope Infection/hematoma formation
Localized pain/paresthesia
Intracapsular Rupture
= broken implant casing, which swims within silicone gel contained by intact fibrous capsule
| Incidence: | 80 90% of all ruptures |
Mammo (11 23% sensitive, 89 98% specific):
- bulging/peaking of implant contour (DDx: herniation through locally weakened capsule)
US (59 70% sensitive, 57 92% specific, 49% accurate):
- stepladder sign = series of parallel horizontal echogenic straight/curvilinear lines inside implant (= collapsed implant shell floating within silicone gel)
- heterogeneous aggregates of low- to medium-level echogenicity (65% sensitive, 57% specific)
| N.B.: | visualization of internal lumen within anechoic space in double-lumen implants can be confused on US with intracapsular rupture |
MR (81 94% sensitive, 93 97% specific, 84% accurate):
- multiple curvilinear low signal-intensity lines often parallel to fibrous capsule (corresponding to collapsed prosthesis shell inside the silicone-filled fibrous capsule):
- linguine sign = multiple hypointense wavy lines within implant (= pieces of free-floating collapsed envelope), 100% PPV
- in incomplete rupture inverted teardrop / noose / keyhole / lariat (= lasso) sign = loop-shaped hypointense structure contiguous with implant envelope (= small focal invagination/fold of shell with silicone on either side)
DDx: radial fold (extending from periphery perpendicular to surface directed toward center of implant) - water droplet sign = salad-oil sign = appearance of multiple droplets of fluid of extracapsular origin/saline-containing envelope within lumen of silicone implant (DDx: 1 2 droplets may be normal; after injection of saline/Betadine/antibiotics/steroids)
Extracapsular Rupture
= extrusion + migration of silicone droplets through tear in both implant shell + fibrous capsule
| Incidence: | up to 20% of all ruptures |
palpable breast masses
US:
- snowstorm / echogenic noise pattern = markedly hyperechoic nodule with well-defined anterior + indistinct echogenic noise posteriorly (= free silicone droplets mixed with breast tissue)
- highly echogenic area with acoustic shadowing
- hypoechoic masses almost indistinguishable from cysts + usually surrounded by echogenic noise (= large to medium-sized collections of free silicone) with low-level internal echoes
MR:
- discrete hypointense foci on fat-suppressed T1WI + hyperintense signal on water-suppressed T2WI in continuity with/separate from implant
- linguine sign = sign of associated intracapsular rupture
Mammography:
- lobular/spherical dense area of opacities adjacent to/separate from silicone implant
- rim calcifications
Extracapsular Spread of Silicone
| Source: | gel bleed, implant rupture (11 23%) more common with thinner shell + older implants |
silicone lymphadenopathy
paresthesia of arm (from nerve impingement secondary to fibrosis surrounding silicone migrated to axilla/brachial plexus)
silicone nipple discharge (rare)
migration to arm (+ constrictive neuropathy of radial nerve), subcutaneous tissue of lower abdominal wall, inguinal canal
- migration to ipsilateral chest wall + axillary nodes
- silicone droplets in breast in 11 23% (97% specific, 5% sensitive)
- granuloma formation (siliconoma) + fibrosis
= collection of silicone within breast parenchyma surrounded by a foreign-body granulomatous reaction
Reduction Mammoplasty
- swirled architectural distortion (in inferior breast best seen on mediolateral view)
- postsurgical distortion
- residual isolated islands of breast tissue
- fat necrosis
- dystrophic calcifications
- asymmetric tissue oriented in nonanatomic distribution
Mastitis
Acute Mastitis
= infection of the breast with primary ascending canalicular + secondary interstitial spread
| Age: | any |
tender swollen red breast (DDx: inflammatory carcinoma)
enlarged painful axillary lymph nodes
febrile, elevated ESR, leukocytosis
- diffuse increased density
- diffuse skin thickening
- swelling of breast
- enlarged axillary lymph nodes
- rapid resolution under antibiotic therapy
P.575
MR:
T1WI:
- circumscribed area of low signal intensity
- strong initial enhancement + postinitial plateau
| Cx: | abscess, fistula |
Puerperal Mastitis
= LACTATIONAL MASTITIS
= usually interstitial infection during lactational period
through infected nipple cracks
hematogenous
ascending via ducts = galactophoritis
| Organism: | Staphylococcus, Streptococcus |
| Rx: | incision + drainage |
Nonpuerperal Mastitis
Infected cyst
Purulent mastitis with abscess formation
Plasma cell mastitis
Nonspecific mastitis
Granulomatous Mastitis
Foreign-body granuloma
Specific disease (TB, sarcoidosis, leprosy, syphilis, actinomycosis, typhus)
Parasitic disease (hydatid disease, cysticercosis, filariasis, schistosomiasis)
Metastasis to Breast
| Incidence: | <1% |
| Mean age: | 43 years |
Intramammary primary:
commonly located in contralateral breast
Extramammary primary:
?leukemia/lymphoma > malignant melanoma > ovarian carcinoma > lung cancer > sarcoma
- In up to 40% no known history of primary cancer!
in children: rhabdomyosarcoma, leukemia, non-Hodgkin lymphoma
- round homogeneous mass with smooth margin
- solitary mass (85%), esp. in upper outer quadrant
- multiple masses; bilaterality in up to 30%
- skin adherence (25%) skin thickening
- axillary node involvement (40%)
Hemorrhagic Metastasis to Breast
Malignant melanoma
RCC
Choriocarcinoma
Kaposi sarcoma
Mondor disease
= rare usually self-limited thrombophlebitis of subcutaneous veins (mostly thoracoepigastric v.) of the breast/anterior chest wall
| Cause: | unknown; trauma, physical exertion, surgery, breast cancer, inflammation, dehydration |
| May be associated with: | carcinoma (in up to 12%), deep venous thrombosis |
painful tender palpable cordlike structure
skin dimpling, erythema
| Location: | usually lateral aspect of breast |
- linear ropelike tubular superficial structure beading
- rarely calcification of vein
US:
- superficial hypoechoic tubular structure containing low-level internal echoes (= thrombus)
| Prognosis: | resolves spontaneously in 2 4 weeks |
Paget Disease Of The Nipple
[Sir James Paget (1814 1899), surgeon and pathologist at St. Bartholomew's Hospital, London, England; first described in 1874]
uncommon manifestation of breast cancer characterized by infiltration of the nipple epidermis by adenocarcinoma
| Prevalence: | 2 3% of all breast cancers |
| Age: | all ages; peak between 40 and 60 years |
nipple changes (32%): erythema, scaling, erosion, ulceration, retraction of nipple and areola:
- Median delay of correct diagnosis by 6 11 months as features suggest a benign diagnosis of eczema!
nipple changes + palpable mass/thickening of breast (45%)
palpable mass/thickening of breast only (14%)
bloody nipple discharge + itching
Histo: Paget cell = large pleomorphic cells with pale cytoplasm arising in main secretory ducts and migrating into epidermis; histologically and biologically similar to comedocarcinoma Associated with:
extensive invasive (30%)/in situ ductal carcinoma (60%) limited to one duct in subareolar area/remote + multicentric
- negative mammogram in 50%
- nipple/areolar/skin thickening
- nipple retraction
- dilated duct
- linearly distributed subareolar/diffuse malignant microcalcifications
- discrete retroareolar soft-tissue mass/masses
MR:
T1WI:
- flattening/thickening of mamillary region
enhanced T1WI:
- variably no to strong initial uptake
- postinitial plateau/wash-out
- asymmetric enhancement of nipple
- retroareolar lymphatic enhancement
T2WI:
- rarely asymmetric areolar hyperintensity
| Dx: | cytologic smear of a weeping nipple secretion/excisional biopsy of a nipple lesion |
| Prognosis: | survival rate with palpable mass similar to infiltrating duct carcinoma; 85 90% 10-year survival rate without palpable mass; positive axillary nodes in 0 13% |
Papilloma Of Breast
= usually benign proliferation of ductal epithelial tissue
P.576
| Incidence: | rare; 1 2% of all benign tumors |
| Age: | 30 77 years (juvenile papillomatosis = 20 26 years); may occur in men |
| Histo: | hyperplastic proliferation of ductal epithelium; lesion may be pedunculated/broad-based; connective tissue stalk covered by epithelial cells proliferating in the form of apocrine metaplasia/solid hyperplasia may cause duct obstruction + distension to form an intracystic papilloma |
MR:
T1WI:
- round/oval tumor with signal isointense to parenchyma
- homo-/heterogeneous contrast enhancement stronger than surrounding parenchyma
- continuous postinitial increase/occasionally plateau
| DDx: | invasive papillary carcinoma |
Central Solitary Papilloma
| Location: | subareolar within major duct |
NOT premalignant
spontaneous usually bloody/serous (9 48%)/clear nipple discharge (52 88 100%):
- Most common cause of serous/sanguineous nipple discharge!
trigger point = nipple discharge produced upon compression of area with papilloma
intermittent mass disappearing with discharge
- negative mammogram/intraductal nodules in subareolar area
- asymmetrically dilated single duct
- subareolar amorphous coarse calcifications
- dilated duct with obstructing/distorting intraluminal filling defect on ductography (= galactography)
- intraductal hypoechoic mass in isolated dilated duct
| Cx: | 0 5 14% frequency of carcinoma development |
Peripheral Multiple Papillomas
| Location: | within terminal ductal lobular unit; bilateral in up to 14% |
In 10 38% associated with:
atypical ductal hyperplasia, lobular carcinoma in situ, papillary + cribriform intraductal cancers, radial scar
nipple discharge (20%)
- round/oval/slightly lobulated well-circumscribed nodules
- segmental distribution with dilated ducts extending from beneath the nipple (20%)
- may be associated with coarse microcalcifications
MR:
- usually not detectable on precontrast T1WI
| Cx: | 5% frequency of carcinoma development; increased risk dependent on degree of cellular atypia |
| Prognosis: | in 24% recurrence after surgical treatment |
Pseudoangiomatous Stromal Hyperplasia
= benign proliferative lesions of mammary stroma in a spectrum from focal incidental findings to clinically
+ mammographically evident breast masses
| Histo: | (a) incidental focal microscopic finding in 23% of all breast specimens (b) tumoral form (rare) |
Tumoral Form Of Pseudoangiomatous Stromal Hyperplasia
| Age: | 4 5th decade (range 14 67 years) |
| Histo: | proliferating myofibroblasts creating slit-like spaces positive for CD34 + muscle actin; similar in appearance to low-grade angiosarcoma |
single circumscribed palpable mass
- well-circumscribed 5 6 (range, 1 12)-cm mass
- growth over time recurrence after excisional biopsy
US:
- hypoechoic solid mass with slightly heterogeneous echotexture
- small cystic component
| DDx: | fibroadenoma, phylloides tumor |
Radial Scar
= SCLEROSING DUCT HYPERPLASIA = INDURATIVE MASTOPATHY = FOCAL FIBROUS DISEASE = BENIGN SCLEROSING DUCTAL PROLIFERATION = INFILTRATING EPITHELIOSIS = NONENCAPSULATED SCLEROSING LESION
= benign proliferative breast lesion (malignant potential is controversial) unrelated to prior surgery/trauma
| Incidence: | 0.1 2.0/1,000 screening mammograms; in 2 16% of mastectomy specimens |
| Cause: | ? localized inflammatory reaction,? chronic ischemia with slow infarction |
| Path: | scar sclerotic center composed of acellular connective tissue (= fibrosis) and elastin deposits (= elastosis); entrapped ductules with intact myoepithelial layer in sclerotic core; corona of distorted ducts + lobules composed of benign proliferations (sclerosing adenosis, ductal hyperplasia, cyst formation, papillomatosis) |
In up to 50% associated with:
tubular carcinoma, comedo carcinoma, invasive lobular carcinoma + contralateral breast cancer
- Avoid frozen section, core needle biopsy, fine-needle aspiration!
rarely palpable
- mean diameter of 0.33 cm (range, 0.1 0.6 cm)
- typically no central mass (BUT: irregular noncalcified mass often with architectural distortion)
- variable appearance in different projections (= radial scars are typically planar in configuration)
- oval/circular translucent areas at center
- very thin long spicules, clumped together centrally
- radiolucent linear structures (= fat) paralleling spicules ( black star appearance)
- no skin thickening/retraction
MR:
T1WI:
- stellate lesion with signal intensity equal to parenchyma (difficult/impossible to visualize within parenchyma; good in adipose tissue)
enhanced T1WI:
- slight to moderate uptake with nonspecific curve
T2WI:
- no characteristic finding
| Rx: | surgical excision required for definite diagnosis |
| DDx: | carcinoma, postsurgical scar, fat necrosis, fibromatosis, granular cell myoblastoma |
P.577
Sarcoma Of Breast
| Incidence: | <1 % of malignant mammary lesions |
| Age: | 45 55 years |
| Histo: | fibrosarcoma, rhabdomyosarcoma, osteogenic sarcoma, mixed malignant tumor of the breast, malignant fibrosarcoma and carcinoma, liposarcoma |
rapid growth (4 6 cm at time of detection)
- smooth/lobulated large dense mass
- well-defined outline
- palpated size similar to mammographic size
Angiosarcoma
= highly malignant vascular breast tumor
| Incidence: | 200 cases in world literature; 0.04% of all malignant breast tumors; 8% of all breast sarcomas | |
| Age: | 3rd 4th decade of life | |
| Histo: | hyperchromatic endothelial cells; network of communicating vascular spaces | |
| stage I: | cells with large nucleoli | |
| stage II: | endothelial lining displaying tufting + intraluminal papillary projections | |
| stage III: | mitoses, necrosis, marked hemorrhage | |
| Metastasis: | hematogenous spread to lung, skin, subcutaneous tissue, bone, liver, brain, ovary; NOT lymphatic | |
rapidly enlarging painless immobile breast mass
- skin thickening + nipple retraction
- large solitary mass with ill-defined nonspiculated border
US:
- well-defined multilobulated hypoechoic mass with hyperechoic areas (from hemorrhage)
| Prognosis: | 1.9 2.1 years mean survival; 14% overall 3-year survival rate |
| Rx: | simple mastectomy without axillary lymph node dissection |
| DDx: | phylloides tumor, lactating breast, juvenile hypertrophy Frequently misdiagnosed as lymphangioma/hemangioma! |
Seroma of breast
localized collection of wound serum after surgery
MR:
T1WI:
- circumscribed area of mildly hypointense signal
enhanced T1WI:
- contrast enhancement in surrounding parenchyma
T2WI:
- hyperintense area of fluid retention
EAN: 2147483647
Pages: 24