46 - Chest Wall Tumors
Editors: Shields, Thomas W.; LoCicero, Joseph; Ponn, Ronald B.; Rusch, Valerie W.
Title: General Thoracic Surgery, 6th Edition
Copyright 2005 Lippincott Williams & Wilkins
> Table of Contents > Volume I - The Lung, Pleura, Diaphragm, and Chest Wall > Section XI - The Pleura > Chapter 56 - Pneumothorax
Chapter 56
Pneumothorax
Willard A. Fry
Kerry Paape
Pneumothorax, or air in the chest, is a phenomenon that has been appreciated since ancient time and has been well discussed by Lindskog and Halasz (1957), Killen and Gobbel (1968), Gobbel and associates (1963), Seremetis (1970), Kittle (1986), and Sahn and Heffner (2000), among many others. Hippocrates and Galen were aware of disease processes involving the pleural space. Adams (1960) notes that Vesalius, in the 16th century, was aware of the necessity for positive-pressure inflation of the trachea to keep the lungs expanded once the pressure seal of the pleural space had been broken. It was not until the 19th century, however, that physicians began to appreciate the various subtleties of disease in the pleural space. The development of the stethoscope by La nnec and the development of radiology by Roentgen brought great advances in the diagnosis of intrathoracic disease. By 1898, John B. Murphy, in Chicago, stimulated by his European colleagues, wrote about the use of artificial pneumothorax in the treatment of pulmonary tuberculosis. The designation of tuberculosis as the primary etiologic agent for spontaneous pneumothorax was finally put to rest by Kjaergaard in 1932.
The thoracic surgeon is called to treat pneumothorax on a regular basis, with the most common presentations being primary spontaneous pneumothorax and secondary pneumothorax after medical procedures. In some areas, pneumothorax associated with Pneumocystis carinii pneumonia is unusually common. Controversy continues over the best method to treat pneumothorax. The explosive development of thoracoscopy in the 1990s and the availability of purified talc have fueled the controversies. Some of the most heated debates in the current medical literature involve treatment programs for spontaneous pneumothorax. There are also significant geographic differences in treatment approach, particularly between America and Europe. In this chapter, we describe the means that we find the most practical and useful and list alternatives that we consider appropriate.
ETIOLOGY
The most common cause of primary spontaneous pneumothorax is the rupture of an apical subpleural bleb (Fig. 56-1). The etiology of such blebs is obscure. Some authors have postulated a difference in alveolar pressure in the upright human between the base and the apex of the lung. In the absence of an associated disorder, spontaneous pneumothorax is rarely seen before puberty. It is more common in men than in women by a ratio of 6:1, and it is more common in smokers than in nonsmokers, as described by Lindskog and Halasz (1957), as well as Bense (1987) and Sadikot (1997) and their associates. The typical patient with a spontaneous pneumothorax is a young, tall, thin man in late adolescence or early adulthood who experiences the sudden onset of chest pain and shortness of breath and who has not been engaging in any unusual or strenuous activity. This clinical picture is in contrast to that of the rarer condition of spontaneous pneumomediastinum, which is invariably associated with strenuous exertion, such as bench-press weight lifting. Children who present with spontaneous pneumothorax often have an underlying condition, such as cystic fibrosis, as described by Wilcox and colleagues (1995).
The causes of pneumothorax are listed in Table 56-1. Special mention must be made of secondary spontaneous pneumothorax associated with acquired immunodeficiency syndrome (AIDS) because it is prevalent in certain centers, as noted by Beers and colleagues (1990). Sepkowitz (1991), Coker (1993), Shanley (1991), and Renzi (1992) and their associates have raised the question of its precipitation by pentamidine aerosol. Wait and Dal Nogare (1994), as well as Metersky (1995) and Pastores (1996) and their colleagues, emphasize the gravity of spontaneous pneumothorax in AIDS patients with Pneumocystis pneumonia.
The most common sarcomas contributing to pneumothorax are osteosarcoma and synovial sarcomas, as reported by Dines and co-workers in 1973. Special mention is made of
P.795
spontaneous rupture of the esophagus, for if it presents as pneumothorax without gastrointestinal symptoms and if the diagnosis is not suspected, an unfavorable outcome is virtually certain. The physician should be alerted by the nature of the accompanying pleural fluid. In the instances of pneumothorax associated with asthma and mucus plugs, the postulated mechanism is obstructive atelectasis of one lobe or segment with hyperinflation of other portions of the lung and resultant parenchymal disruption (Fig. 56-2).
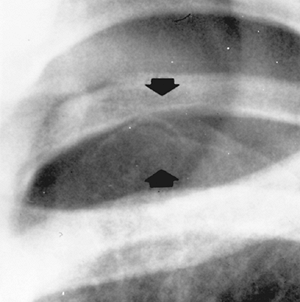 |
Fig. 56-1. Apical subpleural blebs (arrows) in an adolescent boy with a recurrent spontaneous pneumothorax. |
Spontaneous pneumothorax occurring in patients with established chronic obstructive pulmonary disease (COPD), especially with bulla formation, is troublesome. These patients tolerate even small degrees of collapse poorly, and they should be treated aggressively rather than by observation, as recommended by Dines and colleagues in 1970. This group of patients is discussed in detail in Chapter 84. Spontaneous pneumothorax complicating cystic fibrosis is treated differently because of the development of effective bipulmonary lung transplantation, described by Pasque and associates (1990). Whereas in years past, obliteration of the pleural space in cystic fibrosis patients prone to spontaneous pneumothorax was a high priority, less aggressive therapy is now being recommended to facilitate an easier operative field for the lung transplant surgeon. Flume (2003) recently reviewed some of these issues.
Shearin (1974), Maurer (1968), and Lillington (1972) and their colleagues have described catamenial pneumothorax, or pneumothorax that occurs, and recurs, during the first 3 days of menses. Fleisher and associates (1990) have reviewed the possible causes of this problem. In the classic descriptions, nonovulatory states, such as pregnancy and oral contraceptive use, were not associated with pneumothorax. We have encountered primary spontaneous pneumothorax complicating pregnancy more often than catamenial pneumothorax. This has also been described by Dhalla and Teskey (1985) and Van Winter and colleagues (1996).
Table 56-1. Classification of Pneumothorax | |
|---|---|
|
Spontaneous pneumothorax may occur as a rare manifestation of lung cancer. Steinhauslin and Cuttat (1985) described the possible mechanisms. They also noted that lung cancer is estimated to cause only 0.03% to 0.05% of cases of spontaneous pneumothorax. Another rare cause of spontaneous pneumothorax is lymphangioleiomyomatosis, which is seen in young women (see Chapter 118).
Pneumothorax in the neonatal period tends to be treated by the neonatologist and is listed only for completeness. Colombani and Haller (1990) presented a review of this subject.
Acquired pneumothorax is most often iatrogenic, except in institutions with a high incidence of civilian trauma. Transthoracic needle biopsy, the placement of central lines and pacemakers by percutaneous subclavian vein catheterization,
P.796
thoracocentesis, and transbronchoscopic lung biopsy are all frequent causes of pneumothorax. Many are directly related to physician experience, but the risk of inducing pneumothorax from such procedures is always present. Breathing high concentrations of oxygen before transthoracic needle procedures has been recommended (see Chapter 55). Farn and associates (1993) described pneumothorax during laparoscopic surgery as a sequela of previous transdiaphragmatic surgical intervention. Another cause of pneumothorax that is often overlooked is chest tube dysfunction attributable to inadequately sophisticated or callow medical personnel. Such situations include not refilling a water seal bottle with the appropriate amount of water, not filling the U-manometer in the Pleur-evac type of chest-drainage systems, and not adequately securing a chest tube to the chest-drainage system tubing, thereby permitting the occasional disconnection, with its resulting potential for an open pneumothorax.
 |
Fig. 56-2. Pneumothorax complicating asthma in a 12-year-old girl. A. Right upper lobe atelectasis attributed to mucus plugs. B. Pneumothorax attributed to overdistention of nonatelectatic lung. C. Reexpansion of the lung by tube thoracostomy with clearing of the atelectasis. D. Continued reexpansion of the lung after chest tube removal. |
P.797
Barotrauma pneumothorax is defined as that occurring in a patient receiving positive-pressure ventilation. It is always treated by intervention rather than observation because patients relying on mechanical ventilation are already in a compromised state and the positive airway pressure resulting from the mechanical ventilation is a setup for tension pneumothorax. Barotrauma pneumothorax is often attributed to areas of the lung that become overdistended during mechanical ventilation as other areas are consolidated and poorly ventilated. As a general rule, any barotrauma pneumothorax is an indication for tube thoracostomy, as suggested by Kirby and Ginsberg (1992). This topic is discussed in more detail in Chapter 71.
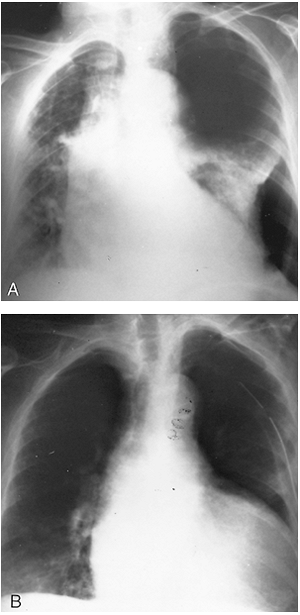 |
Fig. 56-3. Tension pneumothorax in a 72-year-old woman. It resulted from a focal bulla and eventually required surgical treatment. A. Shift of the mediastinum to the right side. A single adhesion kept part of the lung fixed to the chest wall. B. Prompt resolution of the pneumothorax with tube thoracostomy. Note return of the mediastinum to its normal position. |
Traumatic pneumothorax resulting from either blunt or penetrating chest trauma is dealt with in Chapter 70. We urge the placement of a chest tube for traumatic pneumothorax of whatever size whenever there is any other associated injury, because the prompt reexpansion of the collapsed lung immediately eliminates a treatment variable for that patient. Contact sports, such as football and hockey, occasionally produce a sports-related pneumothorax, as reported by Partridge and associates (1997), in the absence of a detectable rib fracture (Fig. 56-3).
PRESENTATION
The symptoms of spontaneous pneumothorax are the sudden onset of chest pain, shortness of breath, and cough. They can be mild or severe. True tension pneumothorax is relatively uncommon, but it is accompanied by tachycardia, sweating, hypotension, and pallor that are striking and that result from mediastinal shift, reduced preload, and intense stimulation of the sympathetic nervous system (Fig. 56-4). As previously mentioned, the usual primary spontaneous pneumothorax occurs without warning or precipitating activity. As the lung collapses, the leak is usually obliterated, thereby limiting the amount of collapse and a progression to tension pneumothorax.
The physical findings of a pneumothorax usually vary with the amount of collapse. If the collapse is significant, findings include diminished tactile fremitus, hyperresonance to percussion, and decreased breath sounds on the affected side. In instances of mild collapse, physical findings can be misleadingly normal, so that if the history suggests
P.798
pneumothorax and yet the physical examination is normal, a chest radiograph should be obtained. In instances of tension pneumothorax, the aforementioned classic physical findings are accentuated and accompanied by a tracheal shift to the uninvolved side, noted by palpation of the trachea in the suprasternal notch. A clinical diagnosis of tension pneumothorax made on the basis of appropriate history and physical findings is an adequate indication to allow for the emergency placement of a chest tube without preliminary confirmatory chest radiography if the clinical situation so demands, and we so instruct our students and house staff.
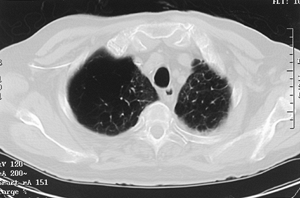 |
Fig. 56-4. Computed tomographic scan of the lungs of a 72-year-old man with extensive bullous disease who presented with a spontaneous pneumothorax. |
DIAGNOSIS
The chest radiograph is the standard procedure in making the diagnosis of a pneumothorax. It should be upright and preferably in the posteroanterior projection. It is possible to miss a pneumothorax in a semisupine portable anteroposterior view. If the patient cannot be upright, a lateral decubitus view with the suspect side positioned up may be helpful. Radiographs obtained in exhalation may accentuate the pneumothorax, but we have not found this technique useful enough in most clinical situations to warrant the double radiographic exposure.
Rhea and colleagues (1982) presented a nomogram for estimating the percentage of pneumothorax. Henry and colleagues (2003), in the recent British Thoracic Society guidelines for the management of spontaneous pneumothorax, recommend defining pneumothoraces as small, moderate, or large, with small defined as a small rim of air around the lung, moderate as lung collapsed halfway towards the heart border, and complete as airless lung, separate from the diaphragm. In general, the percentage of collapse is underestimated.
Skin folds are occasionally misread as pneumothorax. The skin fold artifact, however, has a denser shadow just under the line, which is the opposite of a pneumothorax, in which the lung is more dense in its central portion. Computed tomography of the lungs gives an excellent evaluation of pneumothorax, as shown by Warner (1991) and Lesur (1990) and their associates, but the cost-effectiveness of such a procedure must be questioned (Fig. 56-5).
Small fluid collections are frequently encountered if the pneumothorax lasts longer than 24 hours. The fluid is usually clear, and it is not necessary to analyze it. Large effusions often are bloody and suggest a torn vascular adhesion. Some patients may require immediate operation to control the hemorrhage from a vascular chest wall adhesion that has been torn, because such adhesions have a systemic arterial blood supply.
It is important to exclude a giant bulla in the differential diagnosis because tube drainage of such bullae is unrewarding.
The physiologic consequences of a pneumothorax range from minor, such as 10% spontaneous pneumothorax in a college student, to life-threatening, such as a tension pneumothorax in an older patient with already compromised cardiopulmonary function aggravated by mediastinal shift and compression of the contralateral lung. Gustman and coauthors (1983) described a laboratory model of tension pneumothorax resulting in respiratory failure. The consequences of airline travel and its attendant pressure abnormalities are discussed in Chapter 55. In general, patients with a known pneumothorax should not be encouraged to travel by air.
TREATMENT
Treatment options are listed in Table 56-2. A small spontaneous pneumothorax in an otherwise healthy patient can be observed and followed to its resorption (Fig. 56-6), although, as discussed by Carr (1963) and Lippert (1991) and their colleagues, the results of observational therapy have been under question. Baumann and Strange (1997) present a comprehensive review of treatment from the pulmonologist's point of view. As discussed in Chapter 55, supplying extra oxygen to such patients theoretically hastens the resolution of the pneumothorax, but the true cost-effectiveness of such treatment must be questioned. Kircher and Swartzel (1954) estimated that 1.5% of the air is reabsorbed over each 24-hour period.
Needle or small-catheter aspiration of a mild to moderate spontaneous pneumothorax may hasten the resolution if a persistent leak is absent, as noted by Delius and associates (1989). A plastic needle of the Medicut or Angiocath variety is recommended. Numerous manufacturers have available products. We tend to use what is supplied in a disposable thoracocentesis tray, which has a 14-gauge pliable Teflon catheter that can be advanced over a 17-gauge, 6-inch needle. The needle can be fitted to an automated two-way valve for easy aspiration. Needle aspiration has some particularly devoted advocates in the United Kingdom. The British Thoracic Society, as reported by Henry and colleagues (2003), recommends it as a primary treatment option for primary spontaneous pneumothorax. A. C. Miller (1998) presents a strong argument in favor of considering aspiration as initial therapy. We find that simple aspiration is particularly useful in a smaller pneumothorax with a delayed diagnosis, when the passage of time suggests that the process will be self-limited (see Fig. 56-3). Baumann and colleagues (2001), in a consensus statement prepared for the American College of Chest Physicians, found that there is increasing support in America for initial aspiration of clinically stable patients with small pneumothoraces. Noppen and associates (2002) did a randomized clinical trial comparing simple aspiration of first-episode primary spontaneous pneumothorax with tube thoracostomy and found little difference in patient outcome. Practice patterns vary widely and are often dependent on the type of treatment personnel available and their ability to handle initial follow-up.
A tube thoracostomy should be carried out for pneumothoraces greater than 30% to hasten recovery, or for lesser
P.799
degrees of collapse in patients with symptoms of associated disorders, such as heart disease or COPD. We prefer to use a 20F catheter directed toward the apex. If the tube is placed in the anterior to midaxillary line, less muscle tissue has to be traversed. On the other hand, an anterior tube placed through the second interspace does provide excellent apical air clearance. Anterior tubes are to be avoided in women of almost all ages for cosmetic and aesthetic reasons. Pneumothorax catheter kits are commercially available with 8F plastic catheters that can be inserted over a guide wire. Similar kits with pigtail catheters are also available, as noted by
P.800
Gammie and associates (1999). Foley catheters have been placed in the past, but we no longer recommend their use. It has been suggested that rubber tubes are more irritating than plastic tubes and that rubber tubes are preferable in patients with primary spontaneous pneumothorax because they promote focal pleural symphysis. We are unaware of any randomized clinical trial that has addressed this issue. Whether the tube is placed by clamp or by trocar is at the discretion of the thoracic surgeon. We tend to prefer the trocar technique for its speed and convenience (Fig. 56-7).
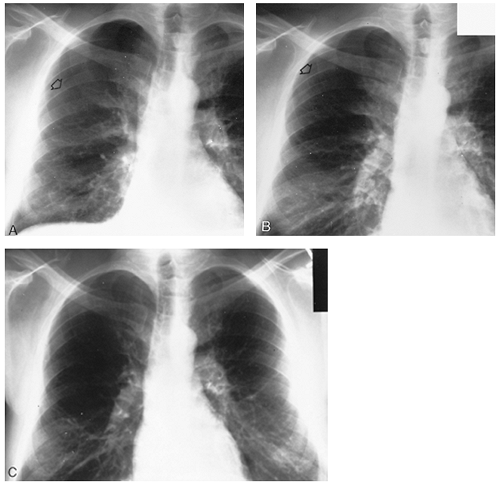 |
Fig. 56-5. Management of primary spontaneous pneumothorax (arrows) by observation, with complete resolution of the collapse. The patient was medically sophisticated, lived near the hospital, and had an occupation that was not physically demanding. A, B, and C were taken at weekly intervals. |
Table 56-2. Treatment Options for Pneumothorax | |
|---|---|
|
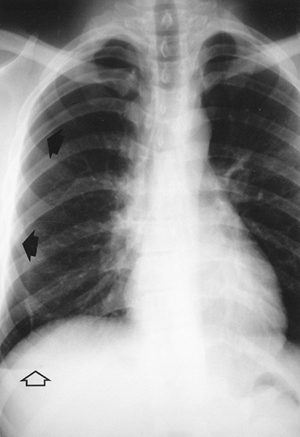 |
Fig. 56-6. Small pneumothorax (solid arrows) successfully treated by aspiration. This is also an example of a sports-related pneumothorax. The patient is a 20-year-old football player who was hit in the right chest by an opponent's helmet 2 days before this film. Note the air fluid level at the base (open arrow), which suggests a degree of chronicity. A single-needle aspiration immediately reexpanded the lung. There was no air leak. |
Small to medium pneumothoraces can be treated successfully on an outpatient basis, as described by Peters and Kubitschek (1984), as well as by Mercier (1976), Obeid (1985), and Cannon (1981) and their associates. Whether to use a water seal or Pleur-evac drainage system or a Heimlich valve is left to the discretion of the surgeon. We prefer a Pleur-evac drainage system set to water seal alone, and gentle suction of about 20 cm H2O is used only if the lung is not completely reexpanded. We tend to eschew routine suction so as to avoid reexpansion pulmonary edema, as described by Matsuura and colleagues (1991) and Light (1990) (Fig. 56-8). If the patient has a chest tube placed but is to be treated on an outpatient basis, we prefer a Heimlich valve arrangement.
Indications for operative intervention are listed in Table 56-3. Surgical treatment of a pneumothorax is recommended for a persistent air leak lasting 5 to 7 days, for a second recurrence in the typical patient, and for the first episode in a patient with only one lung (Fig. 56-9). Certain patient occupations (e.g., divers and airplane pilots) suggest that an operation should be performed after the first episode. The chance of recurrence is estimated at 20% to 50% by Seremetis (1970) and Lindskog and Halasz (1957).
The various surgical options are listed in Table 56-4. The preferred form of surgical treatment is much debated. Various agents have been placed in the pleural space to induce pleural symphysis. The list is long, but it includes silver nitrate, talc, hypertonic glucose, urea, oil, nitrogen mustard, and various antibiotics. A clinical trial described by Light and colleagues in 1990 suggested that intrapleural tetracycline instillation could reduce the incidence of recurrence. We believe, however, that the reduction in recurrence was not overwhelming, considering the short follow-up period. Tetracycline has become difficult to obtain in the United States, and most tetracycline enthusiasts have switched to doxycycline. Talc has been recommended by Weissberg (1990) and by van de Brekel (1993) and Almind (1989) and their associates, but talc therapy, whether by tube and slurry or by thoracoscopy with insufflation, should, in the opinion of many surgeons, be reserved for malignant effusions, not benign pneumothorax. However, Milanez (1994) and Tschopp (1997) and their co-workers report favorable experience with talc for spontaneous pneumothorax. Neither series gives long-term results, which is a matter of concern when dealing with benign disease.
Deslauriers (1980), Thomas (1993), and Murray (1993) and their colleagues, as well as Weeden and Smith (1983), reported series of open operations by limited lateral or axillary incision with bleb excision and pleural abrasion or limited apical pleurectomy with excellent results, low recurrence rates, and no mortality. Dumont and colleagues (1995) reported an excellent series of 400 such operations using a muscle-sparing incision with only one recurrence (0.25%). Our experience with such minithoracotomies has also been favorable. Such results should be kept in mind when reviewing video-assisted thoracic surgery (VATS) series. Complete parietal pleurectomy, popularized by Gaensler (1956), should be reserved for open treatment failures, for postpneumonectomy patients with a first pneumothorax, and for older patients, usually with COPD, with pneumothorax associated with bullous disease. Mills and Baisch (1965) and Clagett (1968) have raised serious objections to using parietal pleurectomy on a routine basis. Patients with known bilateral pneumothoraces (concurrent or separate) can be considered for bilateral treatment via median sternotomy. Bilateral VATS procedures at a single sitting may also be considered.
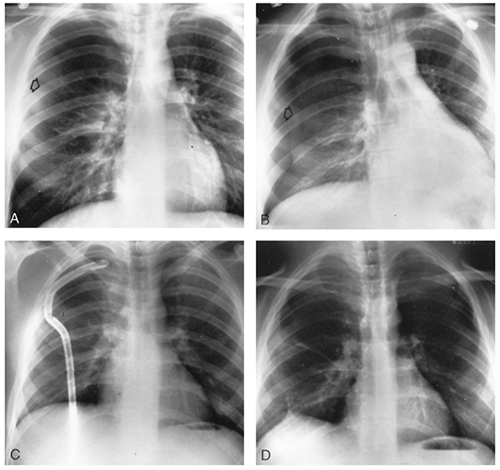 |
Fig. 56-7. Treatment of primary spontaneous pneumothorax by tube thoracostomy. A. On inspiration, there is significant collapse (arrow), estimated at 30% in a 22-year-old man. B. On exhalation, note accentuation of the pneumothorax (arrow) because the pleural air remains constant, but the thoracic volume is smaller. Note a slight shift of the mediastinum to the uninvolved side. C. Tube thoracostomy with a rubber tube directed to the apex. D. Follow-up chest radiograph demonstrated continued reexpansion of the lung. |
P.801
The goal of surgical treatment is to find the offending bleb, remove it, and do some manipulation to encourage adhesion formation, but not too dense an adhesion. It is hoped that such adhesions will keep the lung up should another bleb develop and leak in subsequent years. If no bleb is found, the apex of the upper lobe should be stapled off. In such instances, many surgeons recommend a limited apical pleurectomy. We generally abrade the parietal pleura over the upper half of the chest wall with dry gauze. Marlex mesh and cautery cleaning pads are also used.
In instances of catamenial pneumothorax, Bagan and associates (2003) recommend placing polyglactin mesh over the tendinous portion of the diaphragm to assist in occluding any occult diaphragmatic perforations. The incidence of recurrence appears elevated in catamenial pneumothorax, so this extra maneuver might be beneficial. They recommend a thoracotomy, because they secure the mesh to the diaphragm with multiple sutures placed at the diaphragm's periphery.
The role of thoracoscopy and VATS in the surgical treatment of pneumothorax is evolving. Preliminary reports by Melvin (1992), Nathanson (1991), Inderbitzi (1993) and their associates, as well as by LoCicero (1992), have been encouraging. Subsequent reports by Waller (1994), Naunheim (1995), Bertrand (1996), Mouroux (1996), Passlick (1998),
P.802
Hyland (2001), and Cardillo (2000) and their colleagues reinforce the earlier recommendations to consider VATS as the primary mode of surgical intervention. Most series do report a recurrence rate with VATS that is slightly higher than that with minithoracotomy. Our results using the VATS approach in the surgical treatment of pneumothorax have been similar. The offending bleb can often be identified and stapled with an Endo-GIA through the thoracoscope or with a TA-type stapler through an accessory incision, as described by Lewis and co-workers (1992). Using single-lung anesthesia and a double-lumen endotracheal tube, the anesthesiologist can apply gentle positive pressure to the operated lung to assist in locating the air leak. Pleural abrasion and pleurectomy can also be performed using VATS techniques.
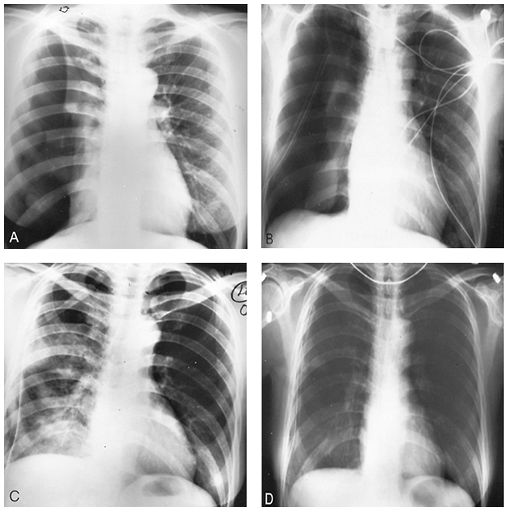 |
Fig. 56-8. Effect of suction and appearance of reexpansion pulmonary edema in a 52-year-old woman who was a smoker. A. Near-total collapse from primary spontaneous pneumothorax. An apical adhesion is noted (arrow). B. On water seal alone, reexpansion is only minimal. C. After application of suction of -20 cm H2O, the lung is completely reexpanded. Note the reexpansion pulmonary edema, which was asymptomatic in this case. |
Table 56-3. Indications for Operative Intervention for Pneumothorax | |
|---|---|
|
At present, our preference is to recommend treatment of the uncomplicated pneumothorax that nonetheless qualifies for surgical treatment by the VATS approach with stapling of the bleb, if found, or of the ever-present apical abnormality if no bleb as such is found. Pleural abrasion is done with dry
P.803
gauze that has been passed into the chest through the accessory incision or one of the ports. We still sometimes place two or three rubber chest tubes through the ports to encourage pleural irritation, and they usually are removed on the third postoperative day (Fig. 56-10). It is our impression that more surgeons use plastic drain tubes. We have already explained our preference for rubber drains. We prefer the more open surgical approach by axillary thoracotomy if we expect to encounter significant bullous disease or unusual adhesion formation, if there has been a previous surgical failure, or if a complete parietal pleurectomy is planned.
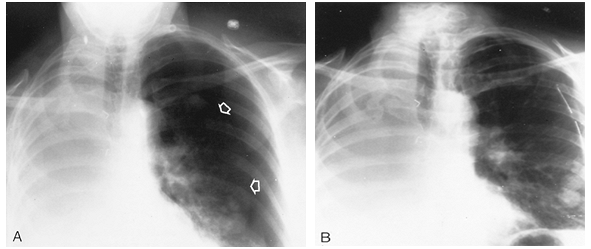 |
Fig. 56-9. Secondary spontaneous pneumothorax in a 50-year-old woman with only one lung. A. Significant, symptomatic collapse secondary to metastatic adenocarcinoma of the lung (arrows). B. Immediate reexpansion by tube thoracostomy. This woman's performance status was good; therefore, she underwent immediate parietal pleurectomy through a small axillary incision. |
Massard and associates (1998) present an excellent review of the recent and pertinent literature on VATS for pneumothorax. Cole (1995), Kim (1996), and J. D. Miller (2000) and their colleagues express doubt about the effectiveness of the VATS approach. Another series of patients reported by Dumont and co-workers (1997) also raises the issue of whether the recurrence rate is higher after VATS than after minithoracotomy. Lang-Lazdunski and associates (2003) report a large series of patients with good follow-up treated by thoracoscopic bleb excision and pleural abrasion, but they emphasize that some form of pleurectomy should be added when operating on patients with a targeted 0% recurrence rate, such as aviators, scuba divers, crew members of nuclear-powered submarines, or other military personnel with special professional requirements.
Table 56-4. Surgical Procedures for Pneumothorax | ||
|---|---|---|
|
The selection of surgical treatment in AIDS patients is more difficult, as described by Gerein (1991) and Crawford (1992) and their associates, as well as by Wait and Estrera (1992), because persistent air leak in spite of standard treatment implies a poor prognosis. Hauck and associates (1991)
P.804
described a thoracoscopic approach using a fibrin glue derivative. Torre and Belloni (1989) described use of a neodymium:yttrium-aluminum-garnet laser thoracoscopically. Patients in poor medical condition that renders them inoperable can also be effectively handled by using Heimlich valves, thus permitting hospital discharge in some instances.
 |
Fig. 56-10. Chest radiograph after video-assisted bleb excision and pleural abrasion in a 14-year-old boy (same patient as in Fig. 56-1). Three rubber tubes were placed through the three ports. He has had no recurrence in over a 15-year follow-up period. |
Some maneuvers in the treatment of pneumothorax deserve mention. A persistent air leak in a patient with a properly placed chest tube who is a poor operative risk can sometimes be encouraged to close by using pneumoperitoneum, as described by Brooks (1973). Sometimes, high-volume suction can get the lung out in patients with COPD who are poor operative candidates. The usual Pleur-evac-type drainage systems do not provide this type of suction, but the old-fashioned water seal bottle attached to a high-force suction source, such as the Emerson apparatus, accomplishes the task.
The training background of the physician treating pneumothorax by VATS is pertinent. Waller (1997) makes a persuasive argument that it be a thoracic surgeon. The culture of medical practice varies from community to community and from country to country. The ultimate goals are proper treatment and good patient care. We strongly believe that the thoracoscopist should be able to handle all surgical complications of a VATS procedure.
Finally, we plead for patience on behalf of the thoracic surgeon. Sometimes, it may be appropriate to try to aspirate a small pneumothorax. Other times, waiting a few more days allows an air leak to seal. On the other hand, if surgical treatment is going to be necessary, the sooner it is performed, the sooner that patient can resume a routine lifestyle.
REFERENCES
Adams WE: Pulmonary reserve and its influence on the development of lung surgery. J Thorac Cardiovasc Surg 40:141, 1960.
Almind M, Lange P, Viskum K: Spontaneous pneumothorax: comparison of simple drainage, talc pleurodesis, and tetracycline pleurodesis. Thorax 44:627, 1989.
Bagan P, et al: Catamenial pneumothorax: retrospective study of surgical treatment. Ann Thorac Surg 75:378, 2003.
Baumann MH, Strange C: Treatment of spontaneous pneumothorax: a more aggressive approach? Chest 112:789, 1997.
Baumann MH, et al: Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. Chest 119:590, 2001.
Beers MF, Sohn M, Swartz M: Recurrent pneumothorax in AIDS patients with Pneumocystis pneumonia. A clinicopathologic report of three cases and review of the literature. Chest 98:266, 1990.
Bense L, Eklund G, Wiman LG: Smoking and the increased risk of contracting spontaneous pneumothorax. Chest 92:1009, 1987.
Bertrand PC, et al: Immediate and long-term results after surgical treatment of primary spontaneous pneumothorax by VATS. Ann Thorac Surg 61:1641, 1996.
Brooks JW: Open thoracotomy in the management of spontaneous pneumothorax. Ann Surg 177:798, 1973.
Cannon WB, Mark JBD, Jamplis RW: Pneumothorax: a therapeutic update. Am J Surg 142:26, 1981.
Cardillo G, et al: Videothoracoscopic treatment of primary spontaneous pneumothorax: a 6-year experience. Ann Thorac Surg 69:357, 2000.
Carr DT, Silver AW, Ellis FH Jr: Management of spontaneous pneumothorax: with special reference to prognosis after various kinds of therapy. Mayo Clin Proc 38:103, 1963.
Clagett OT: The management of spontaneous pneumothorax. J Thorac Cardiovasc Surg 55:761, 1968.
Coker RJ, et al: Pneumothorax in patients with AIDS. Respir Med 87:43, 1993.
Cole FH Jr, et al: Video-assisted thoracic surgery: primary therapy for spontaneous pneumothorax? Ann Thorac Surg 60:931, 1995.
Colombani PM, Haller JA: Neonatal pneumothorax. In Deslauriers J, Lacquet LK (eds): Thoracic Surgery: Surgical Management of Pleural Diseases. St. Louis: CV Mosby, 1990, p. 149.
Crawford BK, et al: Treatment of AIDS-related bronchopleural fistula by pleurectomy. Ann Thorac Surg 54:212, 1992.
Delius RE, et al: Catheter aspiration for simple pneumothorax. Experience with 114 patients. Arch Surg 124:833, 1989.
Deslauriers J, et al: Transaxillary pleurectomy for treatment of spontaneous pneumothorax. Ann Thorac Surg 30:569, 1980.
Dhalla S, Teskey JM: Surgical management of recurrent spontaneous pneumothorax during pregnancy. Chest 88:301, 1985.
Dines DE, Clagett OT, Payne WS: Spontaneous pneumothorax in emphysema. Mayo Clin Proc 45:481, 1970.
Dines DE, et al: Malignant pulmonary neoplasms predisposing to spontaneous pneumothorax. Mayo Clin Proc 48:541, 1973.
Dumont P, et al: Surgical treatment of pneumothorax. Study of a series of 400 cases. Ann Chir 49:235, 1995.
Dumont P, et al: Does a thoracoscopic approach for surgical treatment of spontaneous pneumothorax represent progress? Eur J Cardiothorac Surg 11:27, 1997.
Farn J, Hammerman AM, Brunt LM: Intraoperative pneumothorax during laparoscopic cholecystectomy: a complication of prior transdiaphragmatic surgery. Surg Laparosc Endosc 3:219, 1993.
Fleisher AG, Clement PB, Nelems B: Catamenial pneumothorax: pathophysiology and management. In Deslauriers J, Lacquet LK (eds): Thoracic Surgery: Surgical Management of Pleural Diseases. St. Louis: CV Mosby, 1990, p. 132.
Flume PA: Pneumothorax in cystic fibrosis. Chest 123:217, 2003.
Gaensler EA: Parietal pleurectomy for recurrent spontaneous pneumothorax. Surg Gynecol Obstet 102:293, 1956.
Gammie JS, et al: The pigtail catheter for pleural drainage: a less invasive alternative to tube thoracostomy. JSLS 3:57, 1999.
Gerein AN, et al: Surgical management of pneumothorax in patients with acquired immunodeficiency syndrome. Arch Surg 126:1272, 1991.
Gobbel WG Jr, et al: Spontaneous pneumothorax. J Thorac Cardiovasc Surg 46:331, 1963.
Gustman P, Yerger L, Wanner A: Immediate cardiovascular effects of tension pneumothorax. Am Rev Respir Dis 127:171, 1983.
Hauck H, Bull PG, Pridun N: Complicated pneumothorax: short- and long-term results of endoscopic fibrin pleurodesis. World J Surg 15:146, 1991.
Henry M, Arnold T, Harvey J; Pleural Diseases Group, Standards of Care Committee, British Thoracic Society: BTS guidelines for the management of spontaneous pneumothorax. Thorax 58(suppl 2):ii39, 2003.
Hyland MJ, et al: Is video-assisted thoracoscopic surgery superior to limited axillary thoracotomy in the management of spontaneous pneumothorax? Can Respir J 8:339, 2001.
Inderbitzi RG, et al: Thoracoscopic pleurectomy for treatment of complicated spontaneous pneumothorax. J Thorac Cardiovasc Surg 105:84, 1993.
Killen DA, Gobbel WG Jr: Spontaneous Pneumothorax. Boston: Little, Brown, 1968, p. 1.
Kim KH, et al: Transaxillary minithoracotomy versus video-assisted thoracic surgery for spontaneous pneumothorax. Ann Thorac Surg 61:1510, 1996.
Kirby TJ, Ginsberg RJ: Management of the pneumothorax and barotrauma. Clin Chest Med 13:97, 1992.
Kircher LT Jr, Swartzel RL: Spontaneous pneumothorax and its treatment. JAMA 155:24, 1954.
Kittle CF: The surgical management of recurrent or persistent pneumothorax. In Kittle CF (ed): Current Controversies in Thoracic Surgery. Philadelphia: WB Saunders, 1986, p. 41.
Kjaergaard H: Spontaneous pneumothorax in the apparently healthy. Acta Med Scand 43(suppl):159, 1932.
Lang-Lazdunski L, et al: Videothoracoscopic bleb excision and pleural abrasion for the treatment of primary spontaneous pneumothorax: long-term results. Ann Thorac Surg 57:960, 2003.
Lesur O, et al: Computed tomography in the etiologic assessment of idiopathic spontaneous pneumothorax. Chest 98:341, 1990.
Lewis RJ, et al: One hundred consecutive patients undergoing video-assisted thoracic operations. Ann Thorac Surg 54:421, 1992.
P.805
Light RW: Reexpansion Pulmonary Edema in Pleural Diseases. 2nd Ed. Philadelphia: Lea & Febiger, 1990, p. 256.
Light RW, et al: Intrapleural tetracycline for the prevention of recurrent spontaneous pneumothorax. JAMA 264:2224, 1990.
Lillington GA, Mitchell SP, Wood GA: Catamenial pneumothorax. JAMA 219:1328, 1972.
Lindskog GE, Halasz NA: Spontaneous pneumothorax. Arch Surg 75:693, 1957.
Lippert HL, et al: Independent risk factors for cumulative recurrence rate after first spontaneous pneumothorax. Eur Respir J 4:324, 1991.
LoCicero J: Minimally invasive thoracic surgery, video-assisted thoracic surgery and thoracoscopy. Chest 102:330, 1992.
Massard G, Thomas P, Wilhm J-M: Minimally invasive management for first and recurrent pneumothorax. Current review. Ann Thorac Surg 66:592, 1998.
Matsuura Y, et al: Clinical analysis of reexpansion pulmonary edema. Chest 100:1562, 1991.
Maurer ER, Schaal JA, Mendez FL Jr: Chronic recurrence of spontaneous pneumothorax due to endometriosis of the diaphragm. JAMA 168:2013, 1968.
Melvin WS, Krasna MJ, McLaughlin JS: Thoracoscopic management of spontaneous pneumothorax. Chest 102:1877, 1992.
Mercier C, et al: Outpatient management of intercostal tube drainage in spontaneous pneumothorax. Ann Thorac Surg 22:163, 1976.
Metersky ML, et al: AIDS-related spontaneous pneumothorax. Risk factors and treatment. Chest 108:946, 1995.
Milanez JR, et al: Intrapleural talc for the prevention of recurrent pneumothorax. Chest 106:1162, 1994.
Miller AC: Treatment of spontaneous pneumothorax: the clinician's perspective on pneumothorax management [Letter]. Chest 113:1423, 1998.
Miller JD, et al: Comparison of videothoracoscopy and axillary thoracotomy for the treatment of spontaneous pneumothorax. Am Surg 66:1014, 2000.
Mills M, Baisch BF: Spontaneous pneumothorax. Ann Thorac Surg 1:286, 1965.
Mouroux J, et al: Video-assisted thoracoscopic treatment of spontaneous pneumothorax: technique and results of one hundred cases. J Thorac Cardiovasc Surg 112:385, 1996.
Murphy JB: Surgery of the lung. JAMA 31:151, 208, 281, 341, 1898.
Murray KD, et al: A limited axillary thoracotomy as primary treatment for recurrent spontaneous pneumothorax. Chest 103:137, 1993.
Nathanson LK, et al: Videothoracoscopic ligation of bulla and pleurectomy for spontaneous pneumothorax. Ann Thorac Surg 52:316, 1991.
Naunheim KS, et al: Safety and efficacy of video-assisted thoracic surgical techniques for the treatment of spontaneous pneumothorax. J Thorac Cardiovasc Surg 109:1198, 1995.
Noppen M, et al: Manual aspiration versus chest tube drainage in first episodes of primary spontaneous pneumothorax. Am J Respir Crit Care Med 165:1240, 2002.
Obeid FN, et al: Catheter aspiration for simple pneumothorax (CASP) in the outpatient management of simple traumatic pneumothorax. J Trauma 25:882, 1985.
Partridge RA, et al: Sports-related pneumothorax. Ann Emerg Med 30:539, 1997.
Pasque MK, et al: Improved technique for bilateral lung transplantation: rationale and initial clinical experience. Ann Thorac Surg 49:785, 1990.
Passlick B, et al: Efficiency of video-assisted thoracic surgery for primary and secondary spontaneous pneumothorax. Ann Thorac Surg 65:324, 1998.
Pastores SM, et al: Review: pneumothorax in patients with AIDS-related Pneumocystis carinii pneumonia. Am J Med Sci 312:229, 1996.
Peters J, Kubitschek KR: Clinical evaluation of a percutaneous pneumothorax catheter. Chest 86:714, 1984.
Renzi PM, et al: Bilateral pneumothoraces hasten mortality in AIDS patients receiving secondary prophylaxis with aerosolized pentamidine. Chest 102:491, 1992.
Rhea JT, DeLuca SA, Greene RE: Determining the size of pneumothorax in the upright patient. Radiology 144:733, 1982.
Sadikot RT, et al: Recurrence of primary spontaneous pneumothorax. Thorax 52:805, 1997.
Sahn SA, Heffner JE: Primary care: spontaneous pneumothorax. N Engl J Med 342:868, 2000.
Sepkowitz KA, et al: Pneumothorax in AIDS. Ann Intern Med 114:455, 1991.
Seremetis MG: The management of spontaneous pneumothorax. Chest 57: 65, 1970.
Shanley DJ, et al: Spontaneous pneumothorax in AIDS patients with recurrent Pneumocystis carinii pneumonia despite aerosolized pentamidine prophylaxis. Chest 99:502, 1991.
Shearin RPN, Hepper NGG, Payne WS: Recurrent spontaneous pneumothorax concurrent with menses. Mayo Clin Proc 49:98, 1974.
Steinhauslin CA, Cuttat JF: Spontaneous pneumothorax: a complication of lung cancer? Chest 88:709, 1985.
Thomas P, et al: R sultats du traitement chirurgical des pneumothorax persistants ou r cidivants. Ann Chir 47:136, 1993.
Torre M, Belloni P: Nd:YAG laser pleurodesis through thoracoscopy: new curative therapy in spontaneous pneumothorax. Ann Thorac Surg 47:887, 1989.
Tschopp JM, Brutsche M, Frey JG: Treatment of complicated spontaneous pneumothorax by simple talc pleurodesis under thoracoscopy and local anesthesia. Thorax 52:329, 1997.
van de Brekel JA, Duurkens VAM, Vanderschueren RGJ: Pneumothorax. Results of thoracoscopy and pleurodesis with talc poudrage and thoracotomy. Chest 103:345, 1993.
Van Winter JT, et al: Management of spontaneous pneumothorax during pregnancy: case report and review of the literature. Mayo Clin Proc 71:249, 1996.
Wait MA, Dal Nogare AR: Treatment of AIDS-related spontaneous pneumothorax: a decade of experience. Chest 106:693, 1994.
Wait MA, Estrera A: Changing clinical spectrum of spontaneous pneumothorax. Am J Surg 164:528, 1992.
Waller DA: Video-assisted thoracoscopic surgery (VATS) in the management of spontaneous pneumothorax. Thorax 52:307, 1997.
Waller DA, Forty J, Morritt GN: Video-assisted thoracoscopic surgery versus thoracotomy for spontaneous pneumothorax. Ann Thorac Surg 58:372, 1994.
Warner BW, Bailey WW, Shipley RT: Value of computed tomography of the lung in the management of primary spontaneous pneumothorax. Am J Surg 162:39, 1991.
Weeden D, Smith GH: Surgical experience in the management of spontaneous pneumothorax, 1972 82. Thorax 38:737, 1983.
Weissberg D: Role of chemical methods to induce adhesive pleuritis. In Deslauriers J, Lacquet LK (eds): Thoracic Surgery: Surgical Management of Pleural Diseases. St. Louis: CV Mosby, 1990, p. 130.
Wilcox DT, et al: Spontaneous pneumothorax: a single-institution, 12-year experience in patients under 16 years of age. J Pediatric Surg 30:1452, 1995.
EAN: 2147483647
Pages: 203
- Measuring and Managing E-Business Initiatives Through the Balanced Scorecard
- A View on Knowledge Management: Utilizing a Balanced Scorecard Methodology for Analyzing Knowledge Metrics
- Measuring ROI in E-Commerce Applications: Analysis to Action
- Governing Information Technology Through COBIT
- Governance Structures for IT in the Health Care Industry