VIII - Hematopoietic System
Editors: Mills, Stacey E.
Title: Histology for Pathologists, 3rd Edition
Copyright 2007 Lippincott Williams & Wilkins
> Table of Contents > IX - Genitourinary Tract > 38 - Penis and Distal Urethra
38
Penis and Distal Urethra
Elsa F. Velazquez
Christopher J. Cold
Jos E. Barreto
Antonio L. Cubilla
Introduction
Three cylindrical, firmly adherent, tubular erectile tissues (the corpora cavernosa and the corpus spongiosum) and the pendulous urethra are the basic constituents of the penis that can be subdivided into a distal portion that includes glans, coronal sulcus, and foreskin and a proximal portion, the corpus or shaft (1) (Figure 38.1). The vast majority of penile carcinomas arise from the distal portion of the organ (Figure 38.2).
Distal Penis
Glans
Anatomic Levels of the Glans (Figure 38.2)
Epithelium
Lamina Propria
Corpus Spongiosum
Tunica Albuginea*
Corpus Cavernosum*
Footnote
* The distal portions of the corpora cavernosa encased by the tunica albuginea are part of the glans in 77% of the cases.
Anatomic Features
The conically shaped glans, covered by a pink smooth mucous membrane, is the most distal portion of the organ and shows in its central and ventral region, the meatus urethralis. The expanded anterior end of the corpus spongiosum, which has the shape of an obtuse cone similar to the cap of a mushroom, is the central and main tissue of the glans. It is molded over and attached to the blunt extremity of the corpora cavernosa and extends farther over their dorsal than their ventral surfaces (1). The base of this conus is an elevated rim or border, the corona, occupying 80% of the circumferential head of the glans; it is interrupted in the ventral portion of the glans by the mucosal fold of the
P.966
frenulum (Figure 38.1). The diameter of the corona is wider than the shaft and the remainder of the glans.Within the corpus spongiosum, there is the distal portion of the urethra that opens at the summit of the glans as a vertical, slitlike external orifice termed the urethral meatus (Figures 38.1,38.2). Normal anatomical structures frequently found in sexually active males and commonly located in the proximal glans are called pearly penile papules, hirsutoid papillomas, or papillomatosis corona penis or glandis (2,3,4,5). Grossly, they appear as 1- to 3-mm skin-colored, domed papules evenly distributed circumferentially around the corona and extending proximally on each side of the frenulum. They may be mistaken for warts and be the source of much anxiety for worried adolescents (2).
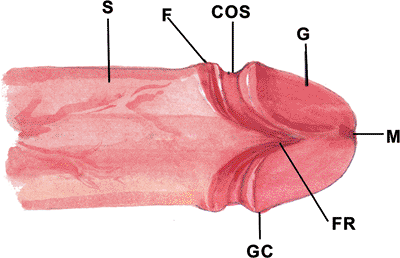 |
Figure 38.1 The penis can be subdivided in a distal portion that includes glans (G), coronal sulcus (COS), and foreskin (F) and a proximal portion, the corpus or shaft (S). (M urethral meatus; GC, glans corona; FR, frenulum) |
Considering the glans as the distal tissues to a line passing through the coronal sulcus, the distal portions of the corpora cavernosa encased by the tunica albuginea extend out into the glans in approximately 77% of the cases (Figure 38.3) (6). However, since they are the main constituents of the shaft, they are discussed in detail in that section.
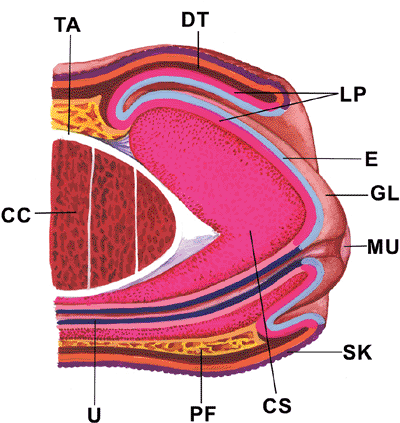 |
Figure 38.2 Diagram illustrating the distal portion of the penis, which includes glans (GL), coronal sulcus, and foreskin. (E, epithelium; LP, lamina propria; CS, corpus spongiosum; TA, tunica albuginea; CC, corpus cavernosum; DT, dartos; SK, skin; U, urethra; MU, meatus urethralis; PF, penile, or Buck's, fascia. |
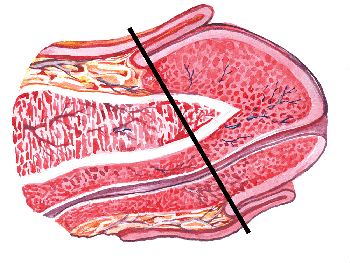 |
Figure 38.3 The distal portion of corpora cavernosa encased by the tunica albuginea is part of the glans in the majority of cases. The diagonal line passing through the coronal sulcus divides glans from shaft. |
Microscopic and Immunohistochemical Features
Epithelium
Both circumcised and intact (uncircumcised) men have partially keratinized stratified squamous epithelium five to six layers thick (Figure 38.4). Some textbooks state that the circumcised glans is much thicker and more keratinized than in an intact man, but no well-controlled studies support this belief. The superficial cells usually contain no glycogen. The normal squamous epithelium is usually positive for the cytokeratins AE1/AE3, 34Be12 and CK7, and the epithelial membrane antigen (EMA). It is negative for the cytokeratins CAM 5.2 and CK20. Langerhans
P.967
cells are found scattered among keratinocytes, and they are increased in number in different inflammatory conditions. Langerhans cells express S-100 protein and CD1a (Figure 38.5). Very rare Merkel cells are also present, and they are very difficult to demonstrate by routine or immunohistochemical techniques. They are usually negative for chromogranin and positive for CK20 (7). The glans epithelium and the mucosal epithelium of the foreskin appear to not contain melanocytes (8,9). Rarely, mucus-producing cells can be noted in the perimeatal region of the glans epithelium (10). They may be the source of the adenosquamous carcinoma of the glans penis. Intraepithelial free nerves ending close to the surface of the epithelium are noted (11). No adnexal or glandular structures are present in the glans. Histologically, the pearly penile papules appear like fibrovascular papillary projections lined by squamous epithelium (Figure 38.6) (2). No koilocytosis is seen in these structures.
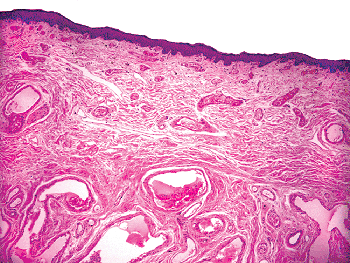 |
Figure 38.4 The three layers of the glans are noted: partially keratinized stratified squamous epithelium, lamina propria, and corpus spongiosum. |
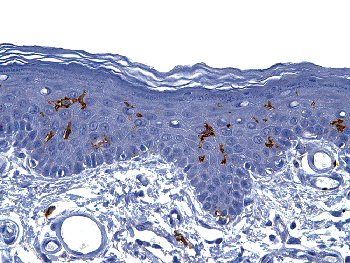 |
Figure 38.5 CD1a immunostain highlights the presence of scattered Langerhans cells in the glans epithelium. |
 |
Figure 38.6 Pearly penile papule appears histologically as a papillary structure with a fibrovascular core lined by squamous epithelium with no evidence of koilocytosis. |
Lamina Propria
The lamina propia is the prolongation of the foreskin lamina propria and separates the corpus spongiosum from the glans epithelium. In the glans, the loose connective tissue of the penile fascia and the fibrous tunica albuginea are lacking so that the lamina propria adheres firmly to the underlying corpus spongiosum (Figure 38.4) (12). The connective tissue of the lamina propria is somewhat similar to that of the corpus spongiosum, although it is more compact and contains fewer peripheral nerve bundles and elastic fibers than the erectile structure. The transition between lamina propria and corpus spongiosum is sometimes difficult to determine at medium or high magnifications. However, at low power or even after a careful gross inspection or with a magnifying lens, this delimitation is evident and follows a line corresponding to the geographic limit of the extension of venous sinuses of the corpus spongiosum. The thickness of the lamina propria varies from 1 mm at the glans corona to 2.5 mm near the meatus. Scattered specialized genital corpuscles are identifed in the lamina propria underneath the squamous epithelium. These genital corpuscles are found mainly in the glans corona and frenulum and may be less numerous in the glans when compared to the foreskin. Additional quantitative studies are needed to confirm or deny this belief. A predominance of free nerve endings over the genital corpuscles has been described in the glans (8,13). A few dermal Merkel cells have been identified at the end of the free nerves.
Corpus Spongiosum
The corpus spongiosum is the principal tissue component of the glans penis and is composed of specialized venous sinuses (Figure 38.7). In the glans, the erectile tissue has the character of a dense, venous plexus (12). As compared to the corpora cavernosa, the interstitial fibrous connective tissue of the corpus spongiosum is more abundant and
P.968
contains more elastic fibers and less smooth muscle bundles (14,15) (Figures 38.8,38.9). The stroma between the vascular spaces is a loose fibrous tissue containing some nerve endings and lymphatic vessels. In this erectile tissue, we also find nutritional veins and arteries (Figure 38.8).
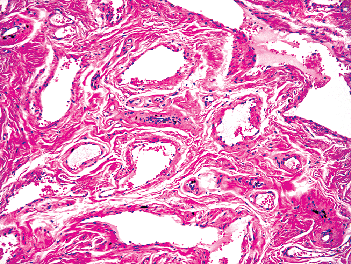 |
Figure 38.7 Glans. Higher power view of the corpus spongiosum showing specialized venous sinuses. |
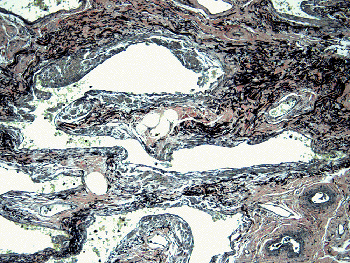 |
Figure 38.8 Corpus spongiosum. The interstitial fibrous connective tissue is more abundant and contains more elastic fibers than in the corpus cavernosum. Note the presence of nutritional veins and arteries in the interstitium of this erectile tissue. (Van Giesson's elastic stain.) |
Coronal Sulcus
Anatomic Levels of the Coronal Sulcus
Epithelium
Lamina Propria
Buck's Fascia
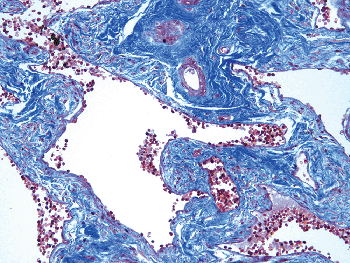 |
Figure 38.9 Corpus spongiosum. The interstitial fibrous connective tissue contains fewer smooth muscle fibers than does the corpus cavernosum (Masson's trichrome). |
Anatomic Features
The coronal sulcus is a narrow and circumferential cul-de-sac located proximal to the glans corona (Figure 38.1,38.2). It is found in both lateral and dorsal aspects of the penis but not in the ventral region, which is occupied by the frenulum, a mucosal fold that fixes the foreskin to the inferior portion of the glans, just below the urethral meatus. The mucous membrane of the glans continues to cover this region as well as the inner surface of the foreskin.
Microscopic and Immunohistochemical Features
Three histologic layers are seen in the coronal sulcus: (a) the squamous epithelium, identical to the glans epithelium; (b) a thin lamina propria, or chorion, which is a prolongation of the foreskin and glans lamina propria; and (c) Buck's fascia and the point of insertion of some of smooth muscle fibers coming from the penile body dartos (Figure 38.10).
The coronal sulcus has been reported as the most frequent site of so-called Tyson's glands (1,14,16,17,18,19,20), described as modified sebaceous glands and reported as responsible for smegma production. Smegma represents epithelial debris and secretions collected in this space (21). There has been some question about the existence of the Tyson's glands (8,21,22). Several studies with numerous tissue sections failed to demonstrate these glands (21,23). We could not find Tyson's glands in a pathologic study of 67 totally sectioned penises removed for carcinoma of the penis. Apparently the original descriptions by Tyson (24) were based on primate studies that could not be confirmed in humans. After circumcision, occasionally some sebaceous glands can be found in the mucosa adjacent to the skin. They are probably skin sebaceous glands misplaced after surgery. Sebaceous glands associated with or without
P.969
hair follicles are found in the penile shaft and cutaneous aspect of the foreskin. We have observed the presence of sebaceous glands that are nonrelated to hair follicles at the mucocutaneous junction of the foreskin and adjacent mucosa but not in the coronal sulcus. The presence of sebaceous gland hyperplasia or ectopic sebaceous glands (Fordyce's condition) is more frequent on the penile shaft and foreskin but may also occur in the glans (2).
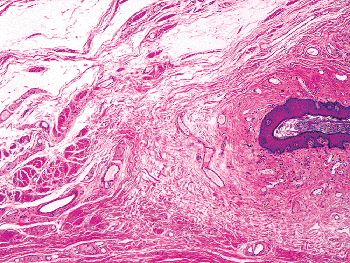 |
Figure 38.10 A section of the coronal sulcus. Histologic components of both glans and penile body are present. This specimen from an uncircumcised person (a portion of the foreskin is seen on top) shows the squamous epithelium (right), lamina propria below, then Buck's fascia and dartos smooth muscle bundles (left). |
Foreskin
Anatomic Levels of the Foreskin
Epidermis
Dermis
Dartos
Lamina propria
Epithelium
Anatomic Features and Circumcision
The foreskin, or prepuce, is a unique genital structure of primates that has been present for over 65 million years, and it is present in all living primates and most mammals. The foreskin is the prolongation of the shaft's skin and normally covers most of the glans, reflecting beyond itself and transforming into a mucosal inner surface. This mucous membrane covers the coronal sulcus as well as the surface of the glans (Figures 38.1,38.2). Grossly, the adult foreskin shows a cutaneous surface that is dark and wrinkled and a mucosal surface that is pink to tan (Figure 38.11).
From very early years to the present, there have been discussions and controversies regarding the role of the foreskin and the importance of circumcision (25,26,27,28), a type of surgery known to mankind as early as 12,000 BCE and practiced for religious or tribal rites by, among others, Egyptians, Jews, Muslims, and Aztecs (29,30). Although circumcision has been practiced for thousands of years, circumcision of infants has only been practiced for approximately 4000 years, as described in Genesis 17. Circumcision on the eighth day represents a mark of the covenant between God and the Jewish people. Genesis 17 marks a significant change in the circumcision ritual since before this time circumcision was always performed on young boys and adolescents. Preputial functions are related to protection of the glans from external irritation or contamination, and it has been shown that the foreskin is normal erogenous tissue (8,31,32).
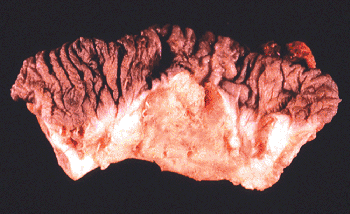 |
Figure 38.11 Gross appearance of an adult foreskin (prepuce). The cutaneous surface (top) is darker and more wrinkled. The mucosa (bottom) is pale beige and slightly irregular. A squamous cell carcinoma is present in the mucosal surface, the most common location of preputial carcinomas. |
In addition, it has been demonstrated that the squamous mucosa of the glans, coronal sulcus, and foreskin are fused during the embryologic development of the penis (Figure 38.12), and they can be considered as one tissue compartment. The fused mucosa of the glans and inner lining of the foreskin separate gradually over the years (8). Most newborn males show an unretracted foreskin at the time of delivery (33). When boys reach the age of 5 to 6 years, the foreskin can be completely retracted in most cases beyond the level of the glans corona, but in some cases this can be done only at puberty. According to these observations, a tight preputial orifice due to an immature preputial plate does not represent an adhesion but a normal stage of penile development. Therefore, neonatal circumcision before the foreskin has naturally separated involves tearing the common prepuce/glans mucosa apart, with the possible complications of excoriation and injury to the glans and ablation of the frenular artery and meatal stenosis (8).
On the other hand, different studies have been published suggesting that circumcision may reduce the risk of penile carcinoma, urinary tract infection, common sexually transmitted diseases, and human immunodeficiency virus
P.970
infection (25,34,35). It has also been proposed that the mucosal inner surface of the foreskin from newborns shows a propensity to be colonized by fimbriated bacteria, with the subsequent occurrence of serious urinary tract infection (36). A recent study suggested that male circumcision is beneficial because it is associated with a reduced risk of penile HPV (human papillomavirus) infection and, in the case of men with a history of multiple sexual partners, a reduced risk of cervical cancer in their current female partner (37). However, it appears clear that the risk of sexually transmitted disease, including HPV infection, correlates with sexual behavior, and behavioral factors appear to be a far more important risk factor than circumcision status.
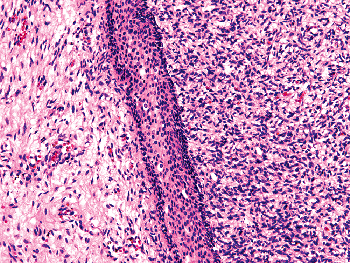 |
Figure 38.12 Fused squamous mucosa of the glans, coronal sulcus, and foreskin during the embryologic development of the penis. Note the common immature epithelial plate (center).The dense stromal cells of the glans will form the corpus spongiosum (right). The lamina propria of the glans is not yet formed. The foreskin is on the left. |
Review of existing literature supports that most children who are uncircumcised do well from a medical standpoint and, thus, the question of whether U.S. health care practitioners are subjecting neonates to an unnecessary surgical procedure remains (35). The clearest medical benefit of circumcision is the relative reduction in the risk for a urinary tract infection, especially in early infancy. Although this risk is real, the absolute numbers are small (risk ranges from 1 in 100 to 1 in 1000). Most of the other medical benefits of circumcision probably can be realized without circumcision as long as access to clean water and proper penile hygiene are achieved (35). Moreover, proper hygiene and access to clean water has been shown to reduce the rate of development of squamous cell carcinoma of the penis in the uncircumcised population (38), and the American Academy of Pediatrics stated that the benefits of male circumcision are not significant enough to merit its routine use. (35).
In adult populations, the variable length of the foreskin has motivated some studies, especially those related to the relation of length and amount of smegma in the balanopreputial sulcus (25,30,39). Phimosis is found in 4% of boys 6 to 17 years of age, but with a diminishing incidence in later years (from 8% in the 6- to 7-year-old group to 1% in the 16- to 17-year-old group) (39). In nonphimotic boys, where the preputial space can be inspected, smegma is present in 5% of the cases. Production of smegma appears to increase in quantity in the 16- to 17-year-old group (39). In a recent prospective study in a high-risk population, we found that long phimotic foreskins were significantly more frequent in patients with penile carcinoma as compared with the general population (25). Coexistence of a long foreskin and phimosis may explain the high incidence of penile cancer in some geographic regions, and circumcision in patients with long and phimotic foreskins living in high-risk areas may be indicated (25). However, additional studies are necessary to confirm whether the length of the foreskin is a significant risk factor, when all other known risk factors (multiple sex partners, foreskin tears, lack of indoor plumbing, tobacco use, etc.) are controlled. Also, studies in nonmestizo populations, in particular European countries that have low circumcision and low cancer rates, would be interesting.
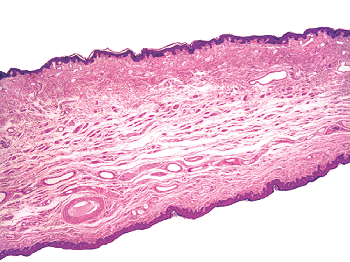 |
Figure 38.13 Full-thickness of the foreskin showing all five layers: keratinized stratified squamous epithelium (top), dermis, dartos, submucosa, and squamous epithelium of the mucosal portion (bottom). |
Microscopic and Immunohistochemical Features
The male foreskin is formed by a midline collision of ectoderm, neuroectoderm, and mesenchyme, resulting in a pentalaminar structure (8). There are five layers in the histologic evaluation of the foreskin (Figure 38.13):
The epidermis consists of a keratinized stratified squamous cell epithelium that is similar to the epidermis seen in the cutaneous tegument. Melanocytes, Langerhans cells, and Merkel cells are also present. Compared to the mucosal epithelium, the epidermis is thinner with better developed rete ridges and usually a pigmented basal layer (Figure 38.14). Vellous hairs, sebaceous, and sweat glands may be seen connected to the epidermis.
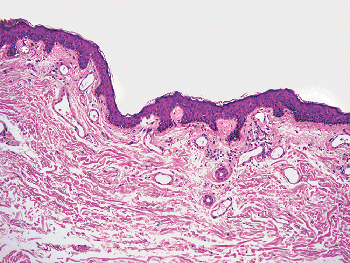
Figure 38.14 Compared to the mucosal epithelium, the epidermis is thinner with better developed rete ridges and usually a pigmented basal layer. The ductal portion of sweat glands connected to the epidermis can be appreciated in this photomicrograph.
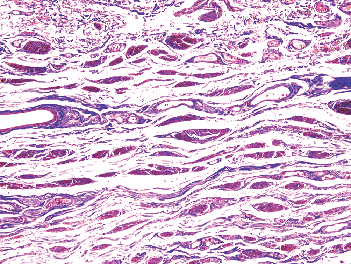
Figure 38.15 Smooth muscle bundles, the main component of the preputial dartos, are shown in red (Masson's trichrome).
The dermis of the foreskin consists of connective tissue with blood vessels and nerve bundles. Meissner corpuscles are present in the dermal papillae and a few Vater-Pacini corpuscles in deeper areas. Few vellous hair structures and sebaceous and sweat glands are noted, and they are not present beyond the dartos. The dermis appears to have more elastic fibers than does the lamina propria.
The dartos consists of smooth muscle fibers invested with elastic fibers, and it is the central axis of the foreskin (Figure 38.15). From the foreskin, the delicate penile dartos muscle surrounds the penile shaft and is continuous with the scrotal dartos muscle. Similar to the penile body dartos, the smooth muscle fibers vary in their disposition. At the level of the edge of the foreskin, the fibers are transversely arranged to form a sphincter to close this edge over the anterior end of the glans. There are numerous nerve endings in close association with the smooth muscle fibers (Figure 38.16). Nerve bundle density in the foreskin was noted to be highest in the ventral preputial tissue (mean: 17.9 bundles/nm) as opposed to lateral (8.6/nm) or dorsal (6.2/nm) tissues (40). A few Vater-Pacini corpuscles may be found scattered between these nerve bundles (Figure 38.17).
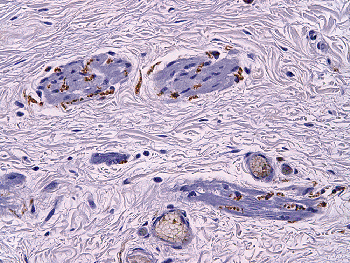
Figure 38.16 Neurofilament immunostain highlights numerous free nerve endings associated with smooth muscle bundles in the foreskin dartos.
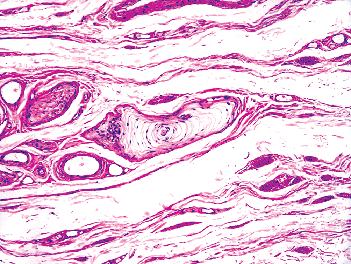
Figure 38.17 A Vater-Pacini corpuscle is present deep in the dartos layer of the foreskin.
The lamina propria, or chorion, is composed of a vascular connective tissue looser than the glans lamina propria. Scattered genital corpuscles and free nerve endings are seen in the lamina propria immediately underneath the epithelium. The genital corpuscles are usually found in clusters of three to five (Figure 38.18). Some authors believe that the corpuscular receptors are more numerous at the mucocutaneous junction of the foreskin; this assertion needs further study (8,31). The mucosal lamina propria is devoid of lanugo hair follicles and sweat and sebaceous glands. We have observed
P.972
a few specimens with rare sebaceous glands unrelated to hair structures at the mucocutaneous junction and immediately adjacent foreskin mucosa, but it is not clear if these represent ectopic glands or variation of normal anatomy.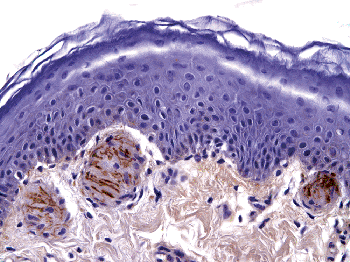
Figure 38.18 The genital corpuscles are usually found in clusters of three to five underneath the mucosal epithelium, in the lamina propria of the foreskin (neurofilament immunostain).
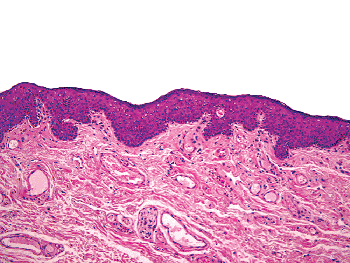
Figure 38.19 The squamous epithelium of the mucosal portion of the foreskin is usually thicker with more irregular and broad rete ridges than in the cutaneous portion. Adnexal structures are absent.
The squamous epithelium (Figure 38.19), which is identical to and a prolongation of the glans and coronal sulcus' epithelia except that the basal layer shows a progressive pigmentation toward the free edge of the foreskin where it reaches the skin epidermis. The immunohistochemical features of this epithelium are identical to the glans squamous epithelium. Langerhans and Merkel cells are present but not melanocytes. Intraepithelial nerves have been described (8,11).
P.971
Proximal Penis (Or Shaft)
Anatomical Levels of the Penile Shaft
Epidermis
Dermis
Dartos
Buck's fascia
Tunica Albuginea
Corpora cavernosa
Corpus spongiosum
Anatomic Features
The penile shaft, body, or corpus, of the penis is mainly composed of three cylindrical masses of erectile tissue, the two corpora cavernosa and a corpus spongiosum with central urethra (Figure 38.20A B). The posterior portion of the corpora cavernosa are two divergent and gradually tapering structures, called the crura, that insert in the ischiopubic bone from where they converge to fuse at the level of the inferior portion of the pubic symphysis. The distal three-fourths of the two corpora cavernosa are intimately bound together and make up the greater part of the shaft of the penis. They retain a uniform diameter in the shaft and terminate anteriorly in a bluntly rounded extremity, being embedded in a cap formed by the corpus spongiosum of the glans (1). The erectile tissue of the corpora cavernosa is a vast, spongelike system of irregular vascular spaces fed by the afferent arteries and drained by the efferent veins. In the flaccid condition of the organ, the cavernous spaces contain little blood and appear as collapsed irregular clefts. In erection they become large cavities engorged with blood under pressure (14).
The corpora cavernosa are surrounded by a firm, thick, fibrous envelope, the tunica albuginea. In the flaccid state the tunica albuginea measures 2 to 3 mm in thickness and becomes thinner (about 0.5 mm) during erection. On longitudinal sections of the organ, the albuginea covering the corpora cavernosa terminates in a > -shaped pattern variably ending beyond or at the level of coronal sulcus or, less frequently, behind it (Figure 38.20A B) (6). The tunica albuginea enveloping the corpora cavernosa is thicker and less elastic than that surrounding the corpus spongiosum (14,15). The superficial longitudinal fibers of the tunica albuginea form a single tube that encloses both corpora cavernosa while the deep fibers are arranged circularly around each corpus, forming the septum of the penis by their junction in the median plane (Figure 38.21) (1). The septum is thick and complete in the proximal shaft and discontinous distally. A shallow groove that marks their junction on the upper surfaces lodges the deep dorsal vein of the penis.
The corpus spongiosum and central urethra are located in the concave space on the undersurface of both corpora cavernosa (Figure 38.21). The middle portion of the corpus spongiosum located in the penile shaft is a uniform cylinder somewhat smaller than the corpus cavernosum. At its ends, it expands, the distal extremity forming the glans and the proximal forming the bulb. The urethra enters the corpus spongiosum 1 to 2 cm from the posterior extremity of the bulb by piercing the dorsal surface. The bulb is just superficial to the urogenital diaphragm, and its posterior portion projects backward towards the anus beyond the entrance of the urethra.
The three cylindrical structures forming the penile shaft are covered by a thin, delicate, and elastic skin. Beneath the dermis, there is a discontinuous smooth muscle layer called the dartos (Figure 38.21) embedded in a thin layer of connective tissue corresponding to the superficial fascia of the classical descriptions. Between the dartos and the albuginea, there is a highly elastic yellowish tubelike sheath encasing all three corpora cavernosa and spongiosum; this is designated as Buck's fascia (deep penile fascia of the classical descriptions) (Figures 38.20A B, 38.21). A septum of fascia extends inward between the corpora cavernosa and the corpus spongiosum, providing separate tubular investments for these columns of erectile tissue and dividing the penis into its dorsal (corpora cavernosa) and ventral (corpus spongiosum)
P.973
portions as can be also seen via CT (computed tomography) or MRI (magnetic resonance imaging) (41). When using the terms fascia or penile fascia in this chapter, we are referring to the Buck's fascia since the superficial fascia is just part of the connective tissue surrounding the dartos.
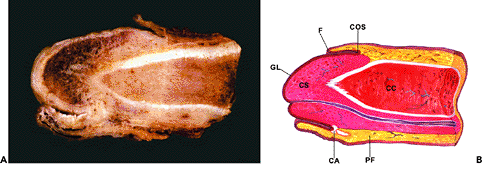 |
Figure 38.20 Gross picture (A) and diagram (B) of two longitudinal sections of a partial penectomy specimen with a small squamous cell carcinoma (CA) located in the coronal sulcus (COS). The albuginea (in white) surrounds the corpus cavernosum. The diagram from a parallel but more central section of the same specimen, illustrates the urethra running within the corpus spongiosum. (F, foreskin; GL, glans; PF, Buck's fascia; CS, corpus spongiosum; CC, corpus cavernosum). |
Microscopic Features
Skin
The skin covering the penile shaft is rugged and elastic. It shows a thin epidermis composed of a few cell layers and minimal keratinization. The epidermal papillae are thin and deep. The basal layer is hyperpigmented. Hair follicles are present in the dermis of the penile body and are more numerous in the proximal body. Hair follicles and other adnexa can extend out to the cutaneous foreskin in some individuals. They are scanty and contain no piloerector muscle. There are a few sebaceous glands not related to hair follicles. Occasionally there are also poorly developed sweat glands.
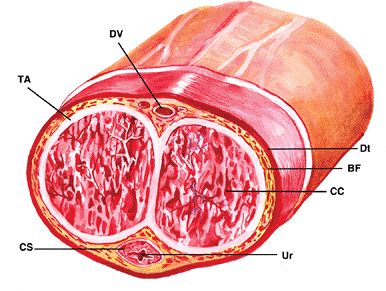 |
Figure 38.21 Cross section of the penis illustrating both corpora cavernosa (CC), each surrounded by the tunica albuginea (TA); they form the septum of the penis by their junction in the median plane. A shallow groove that marks their junction on the upper surfaces lodges the deep dorsal vein of the penis (DV). The dorsal arteries are located on both sides of the vein. Note the corpus spongiosum (CS) and central urethra (Ur) located in the concave space on the undersurface of both corpora cavernosa. (BF, Buck's fascia; Dt, dartos) |
Dartos
The penile dartos is composed of a discontinuous layer of smooth muscle fibers, variably arranged in transverse and longitudinal branches. Some bundles end at the balanopreputial sulcus while others run farther to become the preputial dartos. The dartos is embedded in a loose fibrovascular connective tissue with numerous nerve bundles that correspond to the superficial penile fascia of the classical anatomic description, and it is the skin equivalent of the penile hypodermis but without adipose tissue (1). The penile dartos, similar to scrotal smooth muscle fibers, produces a retraction of genital structures when the exterior temperature falls.
Buck's Fascia
The Buck's fascia is a fibroelastic continuous membrane that encases the corpora cavernosa and the corpus spongiosum. It is composed of loose connective tissue with numerous blood vessels and peripheral nerve bundles running within and beneath it. Vater-Pacini corpuscles are often seen in the penile fascia. The yellow color is related to the numerous elastic fibers and adipose tissue present in the fascia (Figure 38.22). The skin and dartos slide over this fascia. The Buck's fascia is a well-developed sheath of close up fibrovascular tissue that is very important from the
P.974
surgical pathology point of view since it is a frequent pathway of tumor invasion in penile cancer progression (42). This is most likely due to the loose quality of this tissue and the presence of numerous lymphovascular and neural structures. Some investigators point to Buck's fascia as the site of origin of Peyronie's disease (43).
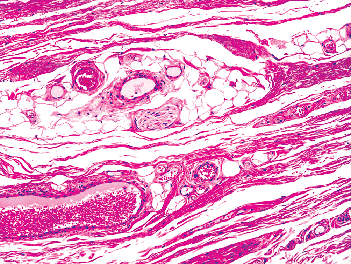 |
Figure 38.22 The Buck's fascia is composed of loose connective tissue with adipose cells and numerous blood vessels and peripheral nerve bundles. |
Tunica Albuginea
The tunica albuginea is a thick sheath of partially hyalinized collagen fibers covering both the corpora cavernosa and corpus spongiosum. It is a poorly vascular structure, with only a few branches of circumflex vessels traversing through it, as demonstrated by factor VIII and CD31 immunostains. It is mainly composed of collagen fibers arranged in an outer longitudinal and an inner circular layer (14,15). The outer layer, which appears to determine the variation in the thickness and strength of the tunica, is absent in the ventral portion of the corpus spongiosum, transforming this portion of tunica into a vulnerable area to perforation. This anatomic aspect probably explains why most prostheses tend to extrude in this area (44). The tunica albuginea forms an incomplete fibrous septum separating both corpora cavernosa. The collagen fibers are wavy in the flaccid state and become straight during erection. The fibers are arranged in such a way so as to permit some elasticity necessary for erection. Elastic fibers are rare in the tunica albuginea of the corpora cavernosa. The tunica albuginea surrounding the corpus spongiosum is thinner and contains more elastic fibers than the one around the corpora cavernosa. In some unusual cases of Fournier's gangrene (45), an infection of the lower urinary tract can spread to the corpus spongiosum. Eventually the tunica albuginea may be penetrated; and, with involvement of Buck's fascia, the infection can rapidly spread to the dartos and directly extend to Colles' scrotal fascia and Scarpa's fascia of the anterior abdominal wall. The infection can spread to the buttocks, thigh, and ischiorectal space (46). The tunica albuginea is probably the real barrier to infiltration of squamous cell carcinoma, contrary to the old concept that the Buck's fascia was the barrier to the spread of the cancer (47).
Corpora Cavernosa
The corpora cavernosa are the main anatomic structures used during erection. The substance of the corpora cavernosa consists of a three-dimensional network of trabeculae. These are composed of connective tissue and smooth muscle and are covered by endothelium, creating a network of interanastomosing vascular spaces between them. These spaces tend to be larger in the more central parts of each corpus cavernosum and smaller at their periphery (14,15). It seems that the smooth muscle bundles are the main component of the trabeculae in the corpora cavernosa (Figure 38.23). There is a highly structured criss-crossing of interconnected fibers and spaces that are tensed as the cylinder expands during erection (48,49). This creates an internal strength and rigidity that is far greater than that possible in a hollow tube filled to equivalent pressure. This specialized network appears to be necessary for erection (49). In the flaccid state, the vascular spaces are 1-mm slits that increase several times in diameter with erection. The interconnection between the venous sinuses is so wide that if a contrast is injected at one point, both corpora cavernosa can be immediately and completely visualized. The precise nature of vascular connections between the corpora cavernosa and corpus spongiosum remains controversial. Cavernospongious arterial anastomoses were described by different authors; however, their physiological role in erection remains unknown (50). These arterial anastomoses could explain
P.975
how drugs penetrate into the corpora cavernosa via the corpus spongiosum after transurethral diffusion (50,51). No arteriovenous shunts or venous connections were found between the corpora cavernosa and the corpus spongiosum (51).
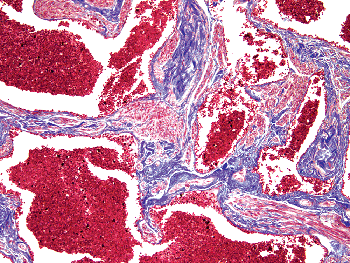 |
Figure 38.23 Corpus cavernosum. The interstitial fibrous connective tissue contains more smooth muscle fibers than in the corpus spongiosum (Masson's trichrome). |
A progressive increase of collagen fibers and decrease of smooth muscle and elastic fiber may be seen in the cavernous trabeculae over the course of time (52).
Corpus Spongiosum
In the corpus spongiosum of the shaft, there are widely interconnected, branching vascular spaces separated by trabeculae. These vascular spaces of variable caliber are lined by endothelial cells and are surrounded by a thin layer of smooth muscle fibers. These fibers coalesce in various extraluminal parts of the vessels to form the subendothelial cushions or polsters. Toward the urethra, the lacunae become continuous with a mucosal plexus of veins; at the periphery, they communicate with the venous network of the albuginea (12). Compared to the corpus spongiosum of the shaft, the substance of the glans corpus spongiosum is made up of convolutions of large veins rather than spaces separated by trabeculae (15).
The main differences between corpus spongiosum and corpora cavernosa from the penile shaft are that the blood spaces in the corpus spongiosum, unlike those of the corpora cavernosa, are the same size in peripheral and central areas and the trabeculae between them contain more elastic fibers, whereas smooth muscle bundles are relatively scarce when compared to the trabeculae of the corpora cavernosa (Figure 38.24) (14,15). However, there is variability and sometimes it can be difficult to distinguish corpus cavernosum from spongiosum by histology alone.
Distal Urethra
Anatomic Levels of the Urethra and Periurethral Tissues
Urethral Epithelium
Lamina Propria
Corpus Spongiosum
Tunica Albuginea
Buck's Fascia
Anatomic Features
The distal (anterior) urethra consists of the bulbous and penile (pendulous) segments. The 3- to 4-cm bulbous urethra is located between the inferior margin of the urogenital diaphragm and the penoscrotal junction and courses in the root of the penis within the bulb of the corpus spongiosum. The penile urethra measures approximately 15 cm in length and extends from the penoscrotal junction to the external meatus; it is closely associated to the corpus spongiosum that forms a protective cylindrical sheath around it (1,10,20). The distal 4 to 6 mm of the penile urethra corresponds to the fossa navicularis, a distal saccular expansion that is contiguous to the urethral meatus. The penile urethra has a more central position within the corpus spongiosum, in contrast to the more dorsally positioned bulbous urethra. The mucosa of the distal urethra has numerous recesses, called Morgagni's lacunae, which extend deeply into the mucin-secreting Littr 's glands that are present in the lateral walls of the bulbous and penile urethra. A stellate-shaped lumen can be noted in cross section of the penile urethra owing to these folds of epithelium and lamina propria (Figures 38.25A B). From the surgical pathology point of view the urethra with surrounding periurethral tissues is an important margin to be carefully evaluated in partial penectomy specimens with penile carcinoma since is the most frequent positive resection margin, as was shown in a recent review of penectomies with carcinoma (42). The anatomical levels at the urethral margin of resection are: epithelium, lamina propria, periurethral corpus spongiosum, tunica albuginea, and Buck's fascia (Figure 38.25B).
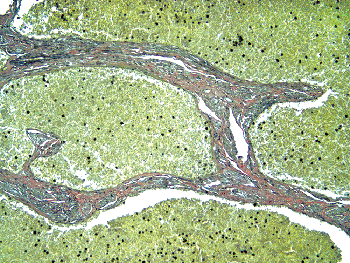 |
Figure 38.24 Corpus cavernosum. The interstitial fibrous connective tissue contains fewer elastic fibers than does the corpus spongiosum (van Giesson elastic stain). |
Microscopic and Immunohistochemical Features
Urethral Epithelium
There are two conflicting embryological explanations of the differentiation of the distal urethra: the ectodermal ingrowth theory (the distal urethra originates in the ectoderm, penetrating from glans to urethra) and the endodermal differentiation theory (distal urethra is formed by differentiation of endodermal tissues from urethra to
P.976
glans) (53,54). Independently of the embryogenesis, there are histological differences between the epithelium of the anterior urethra and the classical transitional urothelium of the posterior urethra and the urinary tract. The fossa navicularis is lined by nonkeratinizing squamous epithelium, and it is similar and continuous to the epithelium covering the glans penis. In the pendulous and bulbous urethra, the surface cell layer is columnar without the umbrella cells noted in bladder urothelium and prostatic urethra. In addition to the columnar cells, the epithelium of the anterior urethra is composed of 4 to 15 stratified layers of uniform small cells, usually categorized as stratified or pseudostratified columnar epithelium (Figure 38.26). The distinctive epithelium appears to be related to the squamous rather than to the transitional urothelium. This would explain the high frequency of squamous metaplasias, as well as the predominance of carcinomas of squamous type in the anterior urethra compared with a much higher frequency of transitional cell carcinomas in the prostatic urethra. The tumors in the membranous portion of the posterior urethra are more similar to those of the bulbous urethra. Adenocarcinomas preferentially arise in the bulbomembranous urethra; however, squamous cell carcinomas are significantly more frequent than adenocarcinomas in these portions (10). The frequent finding of intraepithelial precancerous lesions in the penile urethras of patients with penile squamous cell carcinoma is noteworthy because it indicates that the urethra participates either as a mechanical pathway of penile cancer progression in a continuous manner or as an independent site of primary tumor growth in discontinuous lesions (54).
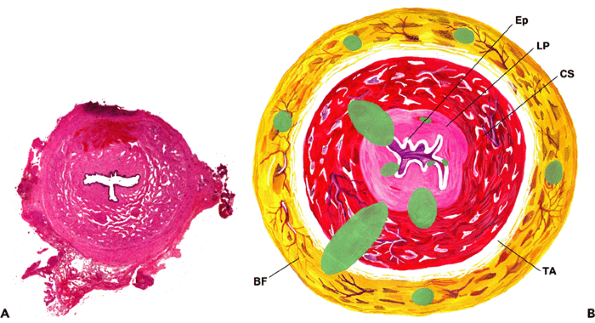 |
Figure 38.25 A. Cross section of the penile urethra and periurethral tissues. Note the stellate-shaped lumen at the center. B. Diagrammatic cross section of penile urethra and periurethral tissues. The anatomical levels at the urethral margin of resection are epithelium (Ep), lamina propria (LP), periurethral corpus spongiosum (CS), tunica albuginea (TA) and Buck's fascia (BF). |
Immunohistochemical studies show that the penile urethral epithelium expresses CK7, 34Be12, and p63 but is negative for CK20. The CK7 immunostain is positive in the upper layers of the epithelium, including the columnar cells (Figure 38.27), in contrast to the expression of p63 and 34Be12 that is mostly seen in basal and parabasal cells but not in the superficial layer of columnar cells (Figures 38.28,38.29). Occasional chromogranin-positive cells may be found close to the basal membrane by immunohistochemical stains.
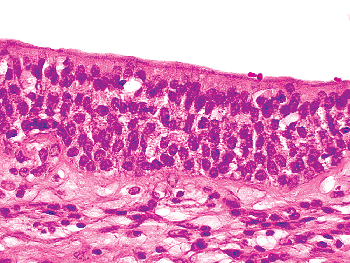 |
Figure 38.26 The epithelium of the anterior urethra is composed of columnar cells overlying 4 to 15 stratified layers of uniform small cells, usually categorized as stratified or pseudostratified columnar epithelium. |
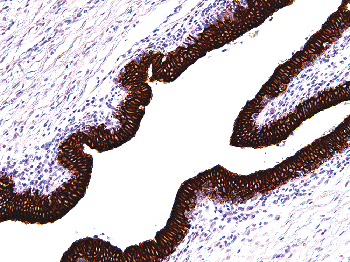 |
Figure 38.27 The expression of CK7 is seen in the upper layers of the urethral epithelium, including the columnar cells. |
P.977
Urethral and Periurethral Glands
There are two different types of glands in the anterior urethra: the intra- or juxtaepithelial glands, with a dense eosinophilic cytoplasm and rounded basal nuclei, and the classical mucinous Littr 's glands, with clear mucinous cytoplasm and basally compressed nuclei resembling pyloric glands of the gastrointestinal tract (Figure 38.30). There are histologic transitions from the intra- or juxtaepithelial glands with dense eosinophilic cytoplasm to more mucinous cells.
The recesses of the urethra (Morgagni's lacunae) are lined by paraurethral mucinous Littr 's glands. Littr 's glands are tubuloacinous mucous structures located along the full length of the corpus spongiosum, in close relation with erectile tissue (Figure 38.31). Littr 's glands end in the urethra at the level of the intraepithelial lacunae. Some cysts have been described as originating in the parameatal Littr 's glands (55). Inflammation of Littr 's glands can clinically simulate a tumor (56). Cohen et al. recognized the normal presence of prostatic epithelial cells in periurethral glands along the penile urethra. These minor prostatic glands may be entirely composed of prostatic cells or, more commonly, mixed prostatic and mucinous epithelium (57) (Figure 38.32). The same authors suggested that these glands may be partially responsible for the minimal but persistently elevated levels of serum PSA (prostate-specific antigen) in some cases of successful radical prostactectomy (57).
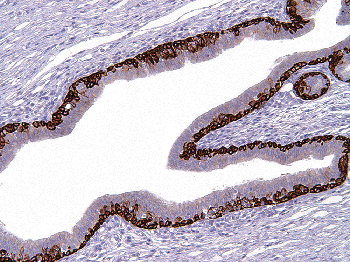 |
Figure 38.28 Urethral epithelium. Basal and parabasal cells express 34Be12. The superficial layers are negative. |
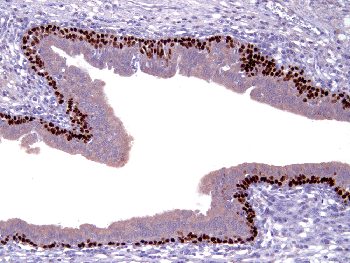 |
Figure 38.29 Urethral epithelium. In contrast to the superficial layers, basal and parabasal cells show p63 nuclear expression. |
The bulbourethral or Cowper's, glands are two small structures deeply located at the level of the membranous (or bulbous) urethra where they terminate in two small ducts (58). They are mucous-acinous structures (Figure 38.33). The clear cells of these glands can be confused with prostatic carcinoma in a core needle biopsy specimen.
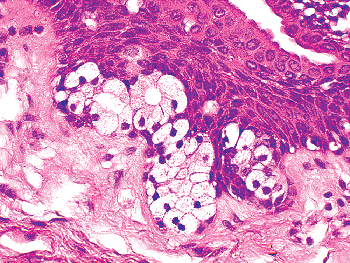 |
Figure 38.30 Penile urethra. A section illustrating intraepithelial mucinous glandular structures. |
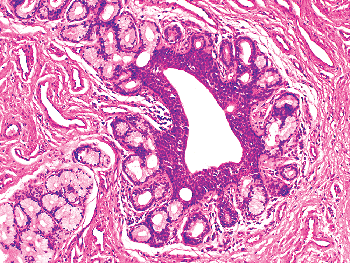 |
Figure 38.31 Penile urethra. Photomicrograph illustrating a cluster of tubular and acinar Littr 's mucous glands. |
P.978
Lamina Propria
The urethral lamina propria is a thin layer of loose fibrous and elastic tissue. Genital corpuscles are identified in the lamina propria of the most distal portion of the urethra, which is lined by squamous epithelium; however, they are not seen in other portions of the penile urethra. We have seen cases of lichen sclerosus affecting the glans and extending into the lamina propria of the anterior urethra (54).
The corpus spongiosum, tunica albuginea, and Buck's fascia were discussed in a previous section.
Arteries
The arteries of the penis are branches of the internal pudenda, which is a branch of the iliac. There are two systems: the dorsal and the cavernous arteries. The dorsal arteries are located from the base of the penis near and on both sides of the dorsal profunda vein within Buck's fascia and in the superior groove formed by the corpora cavernosa (Figure 38.21). Small-caliber branches, or circumflex arteries, irrigate the corpora cavernosa and the periurethral corpus spongiosum. They also perforate the albuginea to reach the corpora. The terminal branches irrigate the glans, and collateral branches provide the skin nutrients. Cavernous arteries penetrate the corpora cavernosa at the site where the corpora join, and they run longitudinally near the central septum, which divides the corpora. From the cavernous arteries originate the vasa vasorum, small arteries that irrigate the erectile tissues. The helicine branches also originate from the cavernous arteries, and they are responsible for filling the vascular spaces during the process of erection; their name derives from the fact that they are coiled and twisted along the trabeculae when the penis is flaccid (59,60). These arteries have thick muscular walls; and, in addition, many possess inner thickenings of longitudinal muscle fibers that bulge into their lumina. Many of the terminal branches of the helicine arteries open directly into the spaces of the erectile tissue.
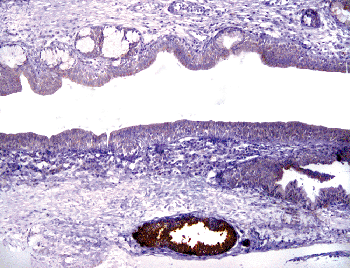 |
Figure 38.32 Some periurethral glands are positive with PSA (prostate-specific antigen) immunostain. |
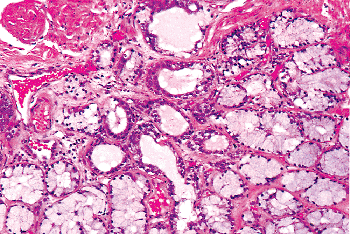 |
Figure 38.33 Bulbourethral (Cowper's) gland. Specimen was taken from autopsy and shows acinous-mucous structures, which are located deeply in the membranous urethra. (Courtesy Dr. Victor Reuter, Memorial Sloan-Kettering Cancer Center.) |
Veins
The superficial veins are irregularly distributed and easily noted under the skin. They end in the superficial dorsal vein; this vascular structure runs straight from the foreskin to the base of the penis. It drains the foreskin venous blood and the skin and is located in the space between the dermis and Buck's fascia. The deeper venous system, for which the axis is the deep dorsal vein, runs along the superficial dorsal vein but in a plane separated by the Buck's fascia (Figure 38.21). The circumflex veins originate in the periurethral
P.979
corpus spongiosum and terminate in the deep dorsal vein system. Similarly, there are veins originating in the corpora cavernosa that, after forming a small plexus at the base of the penis, terminate in the internal pudendal vein. The cavernous venous system, unlike the venous drainage from the glans penis, delays venous drainage and in doing so assists in maintaining erections (61).
Penile erection is a vascular phenomenon that results from trabecular smooth muscle relaxation, arterial dilation, and venous restriction. In further support of the concept of restriction of outflow is the observation that the walls of the circumflex veins are unusually muscular. In addition, these veins exhibit unique specializations of their lumina caller polsters. These are local accumulations of fibroblasts and smooth muscle cells beneath the endothelium that form conspicuous longitudinal thickenings or ridges that can be followed throughout hundreds of serial sections. These are believed to have a role in constricting the lumen and retarding venous outflow during erection (14). There are, however, controversies regarding the real presence and significance of the polsters in the penile veins and arteries, and some authors have proposed that they represent degenerative changes (62).
The deep dorsal vein of the penis has a connection with the vertebral veins, hence it is possible for metastases to make their way to the vertebrae or even to the skull and brain without going through the heart and lungs. Pyogenic organisms may be transported by the same route (1).
Lymphatics
The lymphatics of the foreskin spring from a network that covers its internal and external surfaces; they arise from the lateral aspect and converge dorsally with the skin of the shaft lymphatics to form 4 to 10 vessels that run toward the pubis, where they diverge to drain into the right and left superficial inguinal lymph nodes. The lymphatics draining the glands form a rich network that, beginning in the lamina propia, course toward the frenulum, where they coalesce with two or three trunks from the distal urethra to form several collecting trunks following the coronal sulcus. A collar of lymphatics entirely surrounds the corona, forming two or three trunks that run along the dorsal surface of the penis deep to the fascia and accompanied by the deep dorsal vein. At the presymphyseal region they form a rich anastomosing plexus draining into superficial and deep inguinal lymph nodes (63). The male urethra has a dense plexus in the muscosa. The lymphatic capillaries are especially abundant around the fossa navicularis (1). The lymphatics of the urethra, corpus spongiosum, and corpora cavernosa run toward the ventral surface of the body of the penis, reaching the raphe and the dorsum, where they run with the dorsal vein and end in the superficial and deep inguinal lymph nodes.
Nerves
The nerves originate in the sacral and lumbar plexuses. Peripheral nerves run along the arteries. Dorsal nerves are located external to the arteries, giving circumflex branches to the corpora cavernosa (64,65). The terminal branches end in the glans and foreskin. The dorsal nerve of the penis, the principal somatosensory nerve innervating the penis, consists of two populations of axons, one to innervate the penile shaft and urethra and the other to innervate the glans. Urethral innervation by the dorsal nerve of the penis supports the view that urethral afferent impulses are a component of reflex ejaculatory activity. The pattern of glanular innervation by the dorsal nerve of the penis identifies the glans as a sensory end organ for sexual reflexes. The undulating character of the dorsal nerve of the penis is a mechanism by which the nerve can accommodate to significant changes in penile length with erection (64). The dorsal nerve of the penis supplies the glans in most men, but branches of the perineal nerve can supply the ventral penis, frenulum, and periurethral area in some men.
References
1. Clemete CD, ed. Gray's Anatomy of the Human Body. 30th ed. Philadelphia: Lea & Febiger; 1985.
2. Bunker CB. Male Genital Skin Disease. Philadelphia: Elsevier Saunders; 2004.
3. Hyman AB, Brownstein MH. Tyson's glands. Ectopic sebaceous glands and papillomatosis penis. Arch Dermatol 1969;99:31 36.
4. Tanenbaum MH, Becker SW. Papillae of the corona of the glans penis. J Urol 1965;93:391 395.
5. Winer JH, Winer LH. Hirsutoid papillomas of the coronal margin of glans penis. J Urol 1955;74:375 378.
6. Cubilla AL, Piris A, Pfannl R, Rodriguez I, Aguero F, Young RH. Anatomic levels: important landmarks in penectomy specimens: a detailed anatomic and histologic study based on examination of 44 cases. Am J Surg Pathol 2001;25:1091 1094.
7. Moll I, Kuhn C, Moll R. Cytokeratin 20 is a general marker of cutaneous Merkel cells while certain neuronal proteins are absent. J Invest Dermatol 1995;104:910 915.
8. Cold CJ, Taylor JR. The prepuce. BJU Int 1999;83(suppl1):34 44.
9. Tuncali D, Bingul F, Talim B, Surucu S, Sahin F, Aslan G. Histologic characteristics of the human prepuce pertaining to its clinical behavior as a dual graft. Ann Plast Surg 2005;54:191 195.
10. Young RH, Srigley JR, Amin MB, Ulbright TM, Cubilla AL. Tumors of the prostate gland, seminal vesicles, male urethra and penis. In: Atlas of Tumor Pathology. 3rd series, fascicle. Washington, DC: Armed Forces Institute of Pathology; 2000.
11. Montagna W, Kligman AM, Carlisle KS. Atlas of Normal Human Skin. New York Springer-Verlag; 1992.
12. Kelly DE, Wood RL, Enders AC. Bailey's Textbook of Microscopic Anatomy. 18th ed. Baltimore: Williams & Wilkins; 1984.
13. Halata Z, Munger BL. The neuroanatomical basis for the protopathic sensibility of the human glans penis. Brain Res 1986;371:205 230.
14. Fawcett DW. In: Bloom and Fawcett: A Textbook of Histology. 11th ed. Philadelphia: WB Saunders; 1986.
15. Ham AW, Cormack DH. Histology. 8th ed. Philadelphia: JB Lippincott Company; 1979.
16. Hyman AB, Brownstein MH. Tyson's glands. Ectopic sebaceous glands and papillomatosis penis. Arch Dermatol. 1969;99:31 6.
17. Poirier P, Charpy A. Trait d'Anatomie humaine. Paris: Masson et Cie, 1901:183.
P.980
18. Saalfeld E. Ueber die Tyson'schen dr sen. Arch Mikr Anat 1899:212 218.
19. Tandler J, D meny P. Ueber Tyson'schen dr sen. Wiener Klin Wochen 1898;23:555 556.
20. Testut L, Latarjet A. Tratado de Anatom a Humana, Vol 4. 9th ed. Barcelona: Salvat; 1959.
21. Parkash S, Jeyakumar S, Subramanyan K, Chaudhuri S. Human subpreputial collection: its nature and formation. J Urol 1973;110:211 212.
22. Keith A, Shillitoe A. The preputial or odoriferous glands of man. Lancet 1904;1:146 148.
23. Sprunk H. Ueber die vermeintlichen Tyson'schen drauusen [dDissertation]. University of K nigsberg. Germany; 1897.
24. Tyson E. The anatomy of a pygmy compared with that of a monkey, an ape and a man. London: University of London Press; 1699.
25. Velazquez EF, Bock A, Soskin A, Codas R, Arbo M, Cubilla AL. Preputial variability and preferential association of long phimotic foreskins with penile cancer: an anatomic comparative study of types of foreskin in a general population and cancer patients. Am J Surg Pathol 2003;27:994 998.
26. Weiss C. Motives for male circumcision among preliterate and literate people. J Sex Res 1966;2:69 88.
27. Winberg J, Bollgren I, Gothefors L, Herthelius M, Tullus K. The prepuce: a mistake of nature? Lancet 1989;1:598 599.
28. Wynder EL, Licklider SD. The question of circumcision. Cancer 1960;13:442 445.
29. Arellano-Arroyo A. La cirug a entre los aztecas [tThesis]. Facultad de Medicina, Universidad Nacional Autonoma de Mexico, Ciudad de Mexico, Mexico; 1962.
30. Riveros M. Cancer del pene. Artes Gr ficas Zamphir polos. Asuncion 1968.
31. Taylor JR, Lockwood AP, Taylor AJ. The prepuce: specialized mucosa of the penis and its loss to circumcision. Br J Urol 1996;77:291 295.
32. Winkelmann RK. The erogenous zones: their nerve supply and its significance. Mayo Clin Proc 1959;34:39 47.
33. Ben-Ari J, Merlob P, Mimouni F, Reisner SH. Characteristics of the male genitalia in the newborn: penis. J Urol 1985;134:521 522.
34. Dillner J, von Krogh G, Horenblas S, Meijer CJ. Etiology of squamous cell carcinoma of the penis. Scand J Urol Nephrol Suppl 2000;205:189 193.
35. Lerman SE, Liao JC. Neonatal circumcision. Pediatr Clin North Am 2001;48:1539 1557.
36. Fussell EN, Kaack MB, Cherry R, Roberts JA. Adherence of bacteria to human foreskins. J Urol 1988;140:997 1001.
37. Castellsague X, Bosch FX, Munoz N, et al. Male circumcision, penile human papillomavirus infection, and cervical cancer in female partners. N Engl J Med 2002;346:1105 1112.
38. Frisch M, Friis S, Kjear SK, Melbye M. Falling incidence of penis cancer in an uncircumcised population (Denmark 1943 90). BMJ 1995;311:1471.
39. Oster J. Further fate of the foreskin: incidence of preputial adhesions, phimosis, and smegma among Danish schoolboys. Arch Dis Child 1968;43:200 203.
40. Modwing R, Valderrama E. Immunohistochemical analysis of nerve distributions pattern within preputial tissues. J Urol 1989;141(suppl 1):489A.
41. Hricak H, Marotti M, Gilbert TJ, et al. Normal penile anatomy and abnormal penile condition: evaluation with MR imaging. Radiology 1988;169:683 690.
42. Velazquez EF, Soskin A, Bock A, Codas R, Barreto JE, Cubilla AL. Positive resection margins in partial penectomies: sites of involvement and proposal of local routes of spread of penile squamous cell carcinoma. Am J Surg Pathol 2004;28:384 389.
43. Mostofi FK, Davis C Jr. Male reproductive system and prostate. In: Kissane JM, ed. Anderson's Pathology. 8th ed. Vol 1. St. Louis: CV Mosby; 1985.
44. Hsu GL, Brock G, Mart nez-Pineiro L, von Heyden B, Lue TF, Tanagho EA. Anatomy and strength of the tunica albuginea: its relevance to penile prosthesis extrusion. J Urol 1994;151:1205 1208.
45. Fournier AJ. Gangrene foudroyante de la verge. Semaine Med 1883;3:345 348.
46. Spirnack JP, Resnick MI, Hampel N, Persky L. Fournier's gangrene: report of 20 patients. J Urol 1984;131:289 291.
47. Oota K. Cancer of the penis in Japan. Rev Inst Nac Cancer (Mexico) 1964;15:289 292.
48. Goldstein AMB, Meehan JP, Zakhary R, Buckley PA, Rogers FA. New observations on microarchitecture of corpora cavernosa in man and possible relationship to mechanism of erection. Urology 1982;20:259 266.
49. Zinner NR, Sterling AM, Coleman RV, Ritter RC. The role of internal structure in human penile rigidity. J Urol 1989;141:221A.
50. Droupy S, Giuliano F, Jardin A, Benoit G. Cavernospongious shunts: anatomical study of intrapenile vascular pathways. Eur Urol 1999;36:123 128.
51. Vardi Y, Saenz de Tejada I. Functional and radiologic evidence of vascular communication between the spongiosal and cavernosal compartments of the penis. Urology 1997;49:749 752.
52. Fontana D, Rolle L, Lacivita A, et al. Modificazioni anatomo-funzionali dei corpi caverniosi nell'anziano. Arch Ital Urol Androl 1993;65:483 486.
53. Kurzrock EA, Baskin LS, Cunha GR. Ontogeny of the male urethra: theory of endodermal differentiation. Differentiation 1999;64:115 122.
54. Velazquez EF, Soskin A, Bock A, Codas R, Cai G, Cubilla AL. Epithelial abnormalities and precancerous lesions of anterior urethra in patients with penile carcinoma. A report of 89 cases. Mod Pathol 2005;18:917 923.
55. Shiraki IW. Parameatal cysts of the glans penis: a report of 9 cases. J Urol 1975;114:544 548.
56. Krawitt LN, Schechterman L. Inflammation of the periurethral glands of Littre simulating tumor. J Urol 1977;118:685.
57. Cohen RJ, Garrett K, Golding JL, Thomas RB, McNeal JE. Epithelial differentiation of the lower urinary tract with recognition of the minor prostatic glands. Hum Pathol 2002;33:905 909.
58. Bourne CW, Kilcoyne RF, Kraenzler EJ. Prominent lateral mucosal folds in the bulbous urethra. J Urol 1981;126:326 330.
59. Breza J, Aboseif SR, Orvis BR, Lue TF, Tanagho EA. Detailed anatomy of penile neurovascular structures: surgical significance. J Urol 1989;141:437 443.
60. Krane RJ. Sexual function and dysfunction. In: Walsh PC, Gittes R, Perlmutter AD, Stamey TA, eds. Campbell's Urology. 5th ed. Vol 1. Philadelphia: WB Saunders; 1986:700 735.
61. Fitzpatrick T. The corpus cavernosum intercommunicating venous drainage system. J Urol 1975;113:494 496.
62. Benson GS, McConnell JA, Schmidt WA. Penile polsters: functional structures or atherosclerotic changes? J Urol 1981;125:800 803.
63. Cun o B, Marcille M. Note sur les lymphatiques du gland. Bull Soc Anat Paris 1901;76:671 674.
64. Yang CC, Bradley WE. Peripheral distribution of the human dorsal nerve of the penis. J Urol 1998;159:1912 1916.
65. Lepor H, Gregerman M, Crosby R, Mostofi FK, Walsh PC. Precise localization of the autonomic nerves from the pelvic plexus to the corpora cavernosa: a detailed anatomical study of the adult male pelvis. J Urol 1985;133:207 212.