XX - Diagnostic Studies
Editors: Shields, Thomas W.; LoCicero, Joseph; Ponn, Ronald B.; Rusch, Valerie W.
Title: General Thoracic Surgery, 6th Edition
Copyright 2005 Lippincott Williams & Wilkins
> Table of Contents > Volume II > The Esophagus > Section XXIII - Benign Esophageal Disease > Chapter 148 - Esophageal Diverticula
Chapter 148
Esophageal Diverticula
Stephen D. Cassivi
Francis C. Nichols III
Claude Deschamps
Esophageal diverticula are acquired conditions of the esophagus occurring almost exclusively in adults. An esophageal diverticulum is an epithelial-lined blind pouch arising from the esophagus. There are two categories: pulsion diverticula and traction diverticula. Pulsion or pseudo-diverticula result from transmural pressure gradients that develop from within the esophagus. This results in herniation of the mucosa through a weak point in the muscle layer. Two types of pulsion diverticula are recognized: pharyngoesophageal (Zenker's) and epiphrenic. The second category comprises traction or true diverticula, which result from inflammation and fibrosis in adjacent lymph nodes and are composed of all layers of the esophageal wall. There also exists a very rare entity called diffuse intramural esophageal diverticulosis.
PHARYNGOESOPHAGEAL (ZENKER'S) DIVERTICULUM
Pharyngoesophageal diverticulum is the most common diverticulum of the esophagus and is situated posteriorly just proximal to the cricopharyngeus muscle. It is most prevalent in the fifth to eighth decades. Although first described in 1769 by the English surgeon Ludlow, the eponym refers to the German pathologist Zenker for the classic review written in collaboration with von Ziemssen in 1874.
Pathophysiology
The cause of pharyngoesophageal diverticulum is not completely understood. Because it is usually seen in patients older than 50 years, and rarely in those younger than 30 years, it is considered an acquired condition. Negus (1950) concluded, however, that the constant site of origin just above the cricopharyngeus muscle suggests the possibility of an anatomic weak point in the muscular layers, as well as some distal obstructive role of the cricopharyngeus muscle. Although considerable speculation about the nature of this obstruction has developed since the report of Zenker and von Ziemssen (1874), most of the proposals are based more on theory than on fact. Manometric studies conducted by Ellis and associates (1969) at the Mayo Clinic did not confirm the presence of either achalasia or hypertension of the cricopharyngeus in patients with this diverticulum. Nevertheless, those studies did define an abnormal temporal relation between pharyngeal contraction and sphincteric relaxation and contraction with swallowing. In patients with diverticula, upper esophageal sphincteric contraction occurred before completion of pharyngeal contraction. Thus, premature contraction of the upper sphincter was implicated as characteristic of pharyngoesophageal diverticula. Although these studies provided a definite pattern of the events occurring in patients with diverticula, they failed to define the cause of the diverticulum. The fact that premature sphincteric contraction was noted both in small, early diverticula as well as in large, established ones implicates cricopharyngeal incoordination as a potential cause.
A more recent evaluation by Lerut and colleagues (1988) of the characteristics of the muscles making up the upper esophageal sphincter area suggests that myogenic degeneration and neurogenic disease are not limited to just the cricopharyngeal muscle but affect the striated muscles as well. Therefore, incoordination of the cricopharyngeal muscle could be considered only one aspect of a more complex functional problem rather than a disease on its own, and a pharyngoesophageal diverticulum could be just one expression of this process. More recently, Cook and coauthors (1992) studied patients with Zenker's diverticula and controls using simultaneous videoradiography and manometry. They were able to document significantly reduced sphincter opening and greater intrabolus pressure in patients with Zenker's diverticulum. They concluded that the primary abnormality in patients with Zenker's diverticulum is one of incomplete upper esophageal sphincter opening rather than abnormal coordination between pharyngeal contraction and upper esophageal sphincter relaxation or opening.
P.2240
Thus, the act of swallowing in the presence of cricopharyngeal dysfunction, combined with the usual pressure phenomena during deglutition, is believed to generate sufficient transmural pressure to allow mucosal herniation through an anatomically weak point in the posterior pharynx above the cricopharyngeus muscle. Due to the recurrent nature of the pressures involved and the constant distention of the sac with ingested material, the established diverticulum enlarges progressively and descends dependently. The neck of the diverticulum hangs over the cricopharyngeus, and the sac becomes interposed between the esophagus and the vertebrae. Indeed, the advanced diverticulum may come to lie in the same vertical axis as the pharynx, permitting selective filling of the sac, which may compress and cause the adjacent esophagus to angle anteriorly. These anatomic changes further obstruct swallowing. Moreover, because the mouth of the diverticulum is above the cricopharyngeus, spontaneous emptying of the diverticulum is unimpeded and is often associated with laryngotracheal aspiration, as well as regurgitation into the mouth.
Symptoms and Diagnosis
Although a Zenker's diverticulum may be asymptomatic, most patients develop symptoms early in the course of the disease. Once the condition is established, it progresses both in size and in the frequency and severity of symptoms and complications. Characteristically, the symptoms consist of high cervical esophageal dysphagia, foul breath, noisy deglutition, and spontaneous regurgitation with or without coughing or choking episodes. The regurgitated food is characteristically fresh and undigested and is not bitter, sour, or contaminated by gastroduodenal secretions. The chief complications of pharyngoesophageal diverticulum are nutritional and respiratory. If the condition is neglected, weight loss, hoarseness, asthma, respiratory insufficiency, and pulmonary sepsis leading to abscess are all potential complications. A palpable cervical mass is rarely noted. Carcinoma arising in a pharyngoesophageal diverticulum, as reported by Wychulis and associates (1969) and more recently by Sauvanet and colleagues (1992), is extremely uncommon. Iatrogenic diverticular perforation may occur with esophageal intubation, instrumentation, or with the accidental ingestion of a foreign body.
The diagnosis is confirmed by a barium swallow, which demonstrates the sac (Fig. 148-1). Manometry and endoscopy are of little clinical value in this setting. However, if an endoscopy is indicated for other reasons, the endoscopist should be warned of the possibility of a pharyngoesophageal diverticulum because of the risk of instrumental perforation.
Treatment
The treatment of a pharyngoesophageal diverticulum is surgical. There is no medical therapy for this condition, and all patients with such diverticula should be considered candidates for surgical treatment, irrespective of the size of the diverticulum. Nutritional or chronic respiratory complications are not contraindications to the surgery. To the contrary, as emphasized by Payne (1992), operative repair in such patients should be performed promptly since recurrent episodes of aspiration are poorly tolerated in this elderly population. Advanced age is not a contraindication to surgical treatment. A review by Crescenzo and coauthors (1998) from the Mayo Clinic of patients 75 years of age or older who underwent surgical treatment of a Zenker's diverticulum demonstrated improvement in 94% and no operative deaths. Treatment is best performed on an elective basis while the pouch is of small or moderate size and before complications have occurred. When nutritional or respiratory complications are present or when neoplasia is suspected, surgical intervention is more urgent. Diverticular perforation is a surgical emergency.
Surgical treatment has evolved from the two-stage diverticulectomy of the early 1900s, which was popularized by Coldmarm and by C. H. Mayo and reported by Terracol and Sweet (1958) and by Lahey and Warren (1954). The one-stage diverticulectomy is highly successful, as reported by Harrington (1939), Sweet (1947), Shallow and Clerf (1948), Clagett and Payne (1960) and Payne and Clagett (1965). The successful Mayo Clinic experience with cricopharyngeal myotomy reported by Ellis and associates (1969), and similar reports by Orringer (1980), Duranceau and associates (1983), Gr goire and Duranceau (1991) and Shaw and colleagues (1996), led to recommendations for this procedure alone for small diverticula. Sutherland (1962) also reported cricopharyngeal myotomy alone. Cross and coauthors (1961) used it as an adjunct to extirpation, and Belsey (1966) as well as Duranceau (1983) and Lerut (1990, 1992) and their co-workers combined myotomy with diverticulopexy. Gutschow and associates (2002) recently compared these differing techniques in a retrospective review. They found that diverticulectomy without myotomy predisposed the patient to developing postoperative fistulae and late diverticular recurrences, thus emphasizing the importance of myotomy in the treatment of this disorder. Now, diverticulectomy combined with myotomy is utilized only for patients with larger sacs.
Other approaches also are successful. Dohlman and Mattsson (1959) first described peroral endoscopic diathermic division of the septum or common wall between the diverticulum and the esophagus. This technique was popularized in the United States by Holinger and Schild (1969) and in the Netherlands by van Overbeek (1977, 1994). Additionally, van Overbeek (1995) has described the use of a carbon dioxide laser to divide the common wall. Collard and co-workers (1993) and Peracchia and associates (1998) have used an endoluminal stapler to effect an endoscopic cricopharyngeal myotomy. Collard and co-workers' experience over 16 years was recently published by Gutschow and colleagues (2002). They showed that open techniques, including diverticulectomy, diverticulectomy with cricopharyngeal
P.2241
myotomy, and myotomy alone, provide improved symptomatic relief over endoscopic techniques. This was especially true with smaller diverticula.
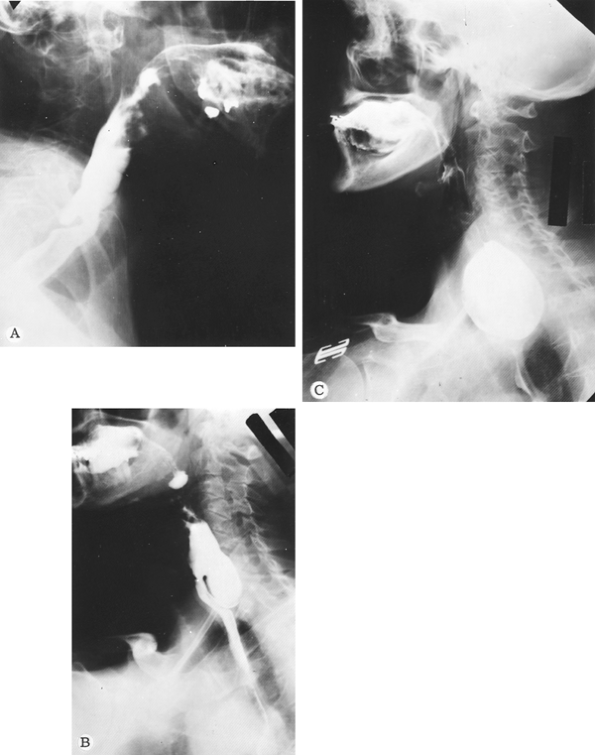 |
Fig. 148-1. Various sizes of pharyngoesophageal diverticula (lateral radiographic views). A. Small. B. Moderate. C. Large. |
Most patients undergoing surgical treatment require little or no preoperative preparation. Rarely are nutritional deficiencies severe enough to require preoperative parenteral hyperalimentation or gastrostomy. Prompt management of the diverticulum provides the best means of correcting most deficiencies. Suppurative lung diseases also often require definitive resolution of the diverticular problem before they can be managed effectively. Occasionally, esophageal bougienage improves obstructive symptoms and temporarily palliates nutritional and respiratory complications, but the patient usually is best served by prompt surgical treatment of the diverticulum.
Surgical Technique
Two techniques are currently used at the Mayo Clinic: cricopharyngeal myotomy alone for small sacs (Fig. 148-2) and one-stage pharyngoesophageal diverticulectomy with
P.2242
cricopharyngeal myotomy for the larger ones (Fig. 148-3). Regional cervical blocks or general anesthesia can be used satisfactorily; however, currently almost all patients receive general anesthesia with a cuffed endotracheal tube. This technique controls ventilation as well as the airway and prevents intraoperative aspiration. Various incisions can be used, depending on whether myotomy or diverticulectomy is planned. Right-handed surgeons find the left cervical approach easiest for exposing most diverticula, unless an uncommon right-sided origin of the diverticulum is preoperatively noted. Usually, an oblique incision paralleling the anterior border of the sternocleidomastoid muscle, extending from the level of the hyoid bone to a point 1 cm above the clavicle, is used. By retracting the sternocleidomastoid muscle and carotid sheath laterally and the thyroid gland and larynx medially, the retropharyngeal space and diverticulum are exposed. The diverticulum arises from the posterior wall of the pharynx just above the level where the omohyoid muscle crosses the incision (Fig. 148-4).
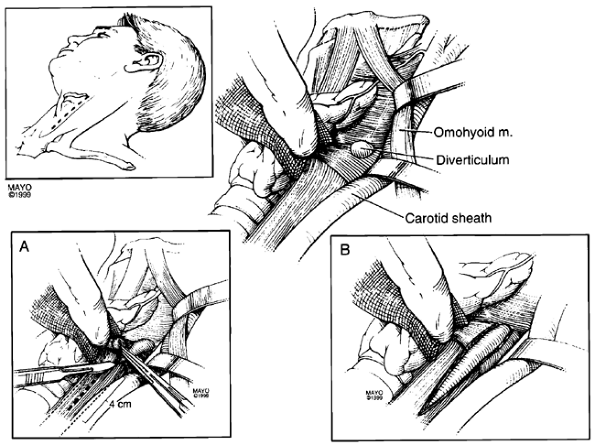 |
Fig. 148-2. Technique of cricopharyngeal myotomy. Myotomy alone is used for the treatment of small pharyngoesophageal diverticula. Exposure of the retropharyngeal space is gained through an oblique left cervical incision along the anterior border of the sternomastoid muscle (m.) (inset). Retraction of the sternomastoid and carotid sheath laterally and the thyroid, pharynx, and larynx medially provides exposure of the diverticulum, which is located at a cervical level where the omohyoid crosses the surgical field. Note that the omohyoid has been retracted cephalad to show the diverticulum. A. After connective tissue is dissected from the mucosal sac to identify the defect in the posterior pharyngeal wall (upper right corner), a posterior midline extramucosal myotomy is effected with a scalpel from the neck of the small sac inferiorly for a distance of 4 cm. B. Retraction of the edges of the cut muscle with a peanut dissector reveals an almond-shaped, diffuse bulge of mucosa through the myotomy. A small Jackson-Pratt drain is brought from the region of the myotomy and retropharyngeal space through a counterincision to the outside, and the platysma and skin are closed in layers. |
Once the diverticulum is identified, it is mobilized and elevated with a clamp. At this point, a 36F Maloney bougie may be introduced into the esophagus to facilitate the dissection. The surgeon must thoroughly dissect out the diverticulum, identifying the margins of the pharyngeal muscular defect through which the mucosal sac protrudes. The myotomy is performed with the dilator in place. It is initiated at the neck of the diverticulum and is extended inferiorly for approximately 4 cm. Simultaneously, the muscle is retracted laterally. The myotomy is placed at roughly 135 degrees laterally from the anterior aspect of the esophagus. Most sacs smaller than 2 cm simply disappear after the myotomy. For diverticula between 2 and 4 cm, the diverticulum may be transected and sewn or can be removed using a stapling device as described by Hoehn and Payne (1969). This improves the speed and accuracy of closure. To avoid stricture, the bougie is left in place while the stapler device is applied and fired. The bougie is removed, the mucosal closure is left uncovered, and a small suction drain (Jackson-Pratt) is placed in the retropharyngeal space. After the operation, the patient is managed routinely. Radiographic examination of the esophagus using contrast study may be done the next day, and if satisfactory, a soft diet is started. The drain is removed 2 days after the operation and the patient discharged home on the third postoperative day. A normal diet is resumed as tolerated.
Results
As Clagett and Payne (1960) reported, the results of the one-stage pharyngoesophageal diverticulectomy are excellent. From 1944 through 1971, 809 patients were treated at the Mayo Clinic by this means, with an operative mortality of 1.4%. The main complications were recurrent nerve palsy in 2.8% of cases and esophagocutaneous fistula in 2.5%. Usually, both complications are temporary and spontaneously resolve. In a 5- to 14-year follow-up of 164 surgical patients, Welsh and Payne (1973) found that 93% either were asymptomatic or had such rare and mild symptoms that they could be classified as having an excellent (82%) or a good (11%) result. Only 11 patients (6.7%) had poor results, with or without anatomic recurrence, and required additional treatment.
Since the 1970s at the Mayo Clinic, cricopharyngeal myotomy has been incorporated with equally satisfactory results. The incidence of late diverticular recurrence remains minimal, as reported by Payne and Reynolds (1982). Anatomic recurrence, as documented by contrast radiography,
P.2243
P.2244
is less likely to be symptomatic if the initial operation included a myotomy. Lerut and coauthors (1990) reported similar results: no postoperative mortality, minimal morbidity, and very good to excellent results in 96% of patients.
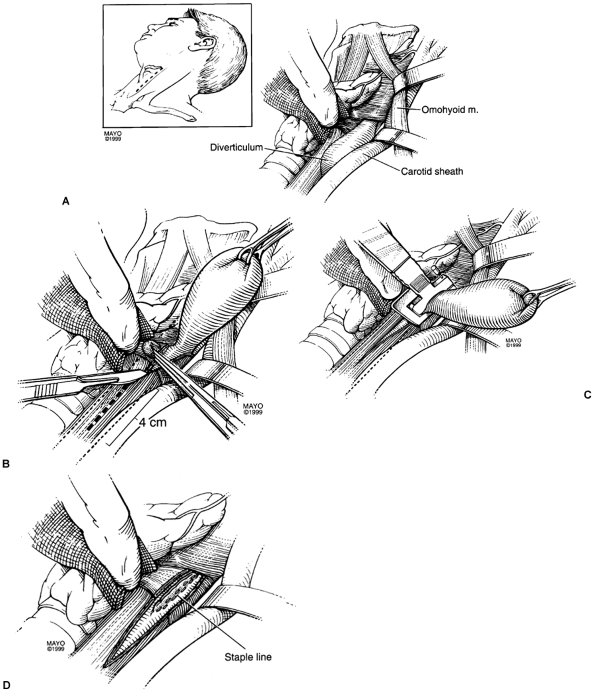 |
Fig. 148-3. One-stage pharyngoesophageal diverticulectomy with myotomy. This procedure is used in the management of medium- and large-sized diverticula. A. Medium-sized diverticulum is exposed through a left cervical incision, as for myotomy alone. Note that the omohyoid has been retracted cephalad and that a finger is used to retract the thyroid, rather than a metal instrument, to avoid injury to the recurrent nerve. The diverticulum has been dissected out to its neck and its apex held cephalad. B. With a 36F bougie in the esophagus, an extramucosal myotomy with the scalpel is completed for a distance of 4 cm. Depending on the size of the diverticulum, a TA-15, TA-30, or TA-55 stapling device is selected. Most require a TA-30 with 3.5-mm staples. C. The stapling device is oriented parallel to the long axis of the esophagus, and an indwelling 36F esophageal bougie is used to prevent stenosis and minimize the length of any luminal narrowing. D. The mucosal closure is left uncovered. Drainage and closure are effected as with myotomy alone. |
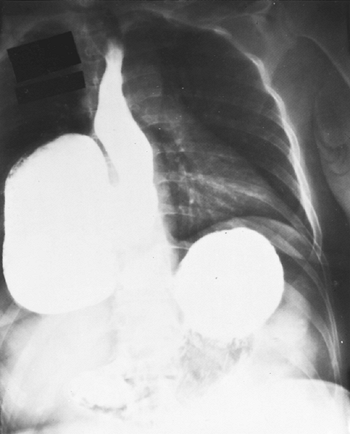 |
Fig. 148-4. Esophagus with a huge epiphrenic diverticulum occupying approximately one-half of the right side of the thorax. Note associated sliding esophageal hiatal hernia. |
Crescenzo and associates (1998) summarized the Mayo Clinic experience in patients 75 years and older. The median age was 79 years, with a range of 75 to 91 years. Preoperative symptoms included dysphagia in 69 patients (92%), regurgitation in 61 (1%), pneumonia in 9 (12%), halitosis in 3 (4%), and weight loss in 1 (1%). Gastroesophageal reflux symptoms were noted in 27 patients (36%). The diagnosis was made by barium swallow in 63 patients, by esophagoscopy in 5 patients, and by a combination of both in 7 patients. Surgical procedures included both diverticulectomy and myotomy in 57 patients (76%), myotomy alone in 9 patients (12%), diverticulopexy and myotomy in 5 patients (7%), and diverticulectomy alone in 4 (5%). There was no in-hospital mortality. Complications occurred in 8 patients (11%) and included esophagocutaneous fistula in 4, pneumonia and urinary tract infection in 1, and wound infection, myocardial infarction, and persistent diverticulum in 1 patient each. Follow-up was available in 72 patients (96%) and ranged from 8 days to 17 years, with a median of 3.3 years. At follow-up, 64 patients (88%) were asymptomatic, and 4 (6%) were improved with minimal symptoms. The remaining 4 patients (6%) had varying degrees of dysphagia, and all were treated with periodic esophageal dilations. The authors concluded that surgery for symptomatic Zenker's diverticulum in the elderly is safe, effective, and results in resolution of symptoms with improved quality of life in most patients.
Reoperation for recurrent pharyngoesophageal diverticulum is difficult. The reports of Huang (1984a) and Rocco (1999) and their co-workers show an increased risk of early postoperative morbidity. Patients who have had previous surgery for Zenker's diverticulum should be considered for reoperation only if they have definite evidence of a diverticulum on barium swallow and progressively disabling or life-threatening symptoms. Reoperation on the upper esophageal sphincter can be a technical challenge. Previous surgery causes obliterated tissue planes and friable esophageal mucosa. Payne (1992) reported that the use of an indwelling bougie is particularly helpful both as a landmark for the esophagus and as a mandrel, over which esophageal repair can be accomplished without fear of luminal compromise. We believe that diverticulectomy and cricopharyngeal myotomy is the treatment of choice for symptomatic patients with recurrent Zenker's diverticulum. Symptoms resolve in a majority of patients.
Cancer arising in a Zenker's diverticulum is rare. It appears to occur in chronically neglected or retained diverticula. Huang and associates (1984b) reported that in two patients with cancer totally confined to the sac, simple diverticulectomy provided long-term survival. More aggressive management is indicated if the malignancy extends beyond the sac.
EPIPHRENIC DIVERTICULUM
Epiphrenic diverticula are rare and may arise anywhere within the thoracic esophagus but are most common in the lower 10 cm. The exact prevalence of this condition is unknown because asymptomatic patients are usually not discovered. Most of these diverticula are found in middle-aged or elderly patients, and there is a slight predominance in men. The ratio of epiphrenic to pharyngoesophageal diverticula at the Mayo Clinic during the past four decades has been 1 to 5, as noted by Trastek and Payne (1989).
Pathophysiology
Mondiere (1833) postulated that pulsion diverticula are mucosal herniations occurring through the muscular wall associated with some form of obstruction to swallowing and the resultant increased intraluminal pressure. Although it is not surprising that symptoms were initially attributed solely to the saccular abnormality of the distal esophagus, the role of esophageal motility disorders in the genesis of this condition was reported on by Vinson (1934). With the advent of manometric studies, it became increasingly evident that functional obstruction of the distal esophagus may
P.2245
be not only the cause of the diverticulum but also a major cause of symptoms, as suggested by Habein and co-workers (1956a, 1956b). Benacci and colleagues (1993), from the Mayo Clinic, emphasize that achalasia, diffuse esophageal spasm, hypertensive lower esophageal sphincter, and nonspecific motor abnormalities have all been seen in conjunction with epiphrenic diverticula. However, motility disorders are not found in every patient, and when present, both the type of manometric disturbance and the severity of symptoms vary, as shown by Kaye (1974) as well as by Bontempo (1985), Debas (1980) and Dodds (1975) and their associates. Recently, Nehra and co-workers (2002), using the modern diagnostic technique of 24-hour ambulatory manometry, have prospectively studied the pathophysiology of epiphrenic diverticula. They found that abnormal esophageal motility was present in all patients with this problem and was likely the underlying cause leading to its development.
Symptoms and Diagnosis
Symptoms in patients with epiphrenic diverticula are variable. Many are asymptomatic, whereas others have only mild dysphagia that is readily managed with simple methods, such as thorough mastication and adequate fluids at mealtime. Benacci and associates (1993) found that the majority of patients are in this latter category, with the diverticulum often being a coincidental finding on barium swallow done for unrelated reasons. A small number of patients have progressive and frequently incapacitating symptoms, most often severe dysphagia, chest pain, food retention, regurgitation, and aspiration. The last two of these symptoms may become life-threatening because repeated episodes of pneumonia may result in progressive destruction of lung parenchyma. In our experience, the ratio of patients with absent or only minimal symptoms to those with incapacitating symptoms was 1.7 to 1.0.
All patients with a suspected epiphrenic diverticulum should have a barium upper gastrointestinal radiograph. Barium swallow provides proof of diagnosis (Fig. 148-5), serves as a baseline if the patient is asymptomatic, may provide clues to any associated motility disorder, and may detect other lesions, such as cancer, stricture, or hiatal hernia. Patients with incapacitating symptoms should have further evaluation with esophagoscopy and esophageal manometry. Esophagoscopy allows evaluation for esophagitis and the rare presence of cancer. Esophagoscopy may also be of value in removing retained debris from the sac preoperatively in patients with severe retention and regurgitation. Manometry is mandatory to define associated motility disorders. The manometric findings may help determine the length of esophagomyotomy required to relieve functional obstruction. However, because of the difficulty of passing the probe into the stomach, manometry may underestimate the extent of abnormal motility. Nehra and colleagues (2002) emphasize the importance of manometric evaluation and have improved their success of catheter positioning to 100% by endoscopic placement in difficult cases.
If gastroesophageal reflux is suspected, a 24-hour pH study can also be performed, as reported by Evander (1986) and Viard (1987) and their co-workers, before proceeding with an antireflux procedure on clinical findings alone. If not confirmed, the symptoms thought to be related to reflux might be caused by other conditions, such as abnormal motility or regurgitation of diverticular contents. Primary carcinoma has been noted with epiphrenic diverticula, as in the report of Allen and Clagett (1965), as have rare benign neoplasms, particularly leiomyoma and lipoma.
Treatment
The decision to proceed with surgical repair can be difficult. Simple medical measures often provide effective control in mildly symptomatic patients. In their publication describing 112 patients, Benacci and associates (1993) had 47 patients who were asymptomatic and were not surgically treated. Twenty patients were followed for a median of 4 years (range 1 to 17 years), and all remained asymptomatic. Fifteen additional patients had mild symptoms without surgical intervention, and none of these developed incapacitating symptoms during follow-up (median 11 years, range 1 to 25 years). Although only one-half of the asymptomatic or mildly symptomatic patients had long-term follow-up available for review, progressive symptoms did not develop in any of them.
Thus, we believe that patients with minimal symptoms should be managed conservatively and followed at regular intervals. If symptoms are incapacitating, an operation should be advised if the patient is otherwise in good health. Additionally, even when symptoms cannot be definitely attributed to the diverticulum, diverticulectomy should be considered when an operation is planned for the management of associated esophageal conditions. Neither the size nor the dependent location of the diverticulum correlated with symptoms in the report of Benacci and associates (1993). In contrast, based on their experience, Altorki and colleagues (1993) have recommended operative treatment in all patients with epiphrenic diverticulum in order to avoid subsequent complications.
Surgical Technique
Clairmont performed the first extirpation of an epiphrenic diverticulum, using an extrapleural approach, as cited by Moynihan (1927). Barrett (1933) first reported a transpleural approach. The most popular technique currently is a left transthoracic diverticulectomy, usually with a
P.2246
long extramucosal esophagomyotomy (Fig. 148-6). The sac is mobilized and the diverticulectomy performed longitudinally over a 50F dilator. Many prefer to use a stapling device and to close the muscular wall over the diverticular stump. An esophagomyotomy must be performed not only to prevent suture line leak and diverticular recurrence but also to relieve symptoms from the associated motility condition.
 |
Fig. 148-5. Surgical management of pulsion diverticulum of the lower portion of the esophagus. (inset). Placement of left posterolateral thoracotomy incision. A. Exposure of the diverticulum is obtained when the chest is entered over the top of the unresected eighth rib. Note that the esophagus has been delivered from its mediastinal bed, tapes have been passed around the esophagus, and the esophagus has been rotated to bring the diverticulum into view. The neck of the mucosal diverticulum has been dissected, identifying the defect in the esophageal muscular wall. B. With a 50F bougie dilator in place, a TA stapling device is used to transect and close the diverticulum, followed by closure of esophageal musculature over the mucosal suture line. The site of the diverticular incision has been rotated back to the right and is not visible. C. A long esophagomyotomy has been performed, extending from the esophagogastric junction to the aortic arch. The musculature of the esophagus has been freed from approximately 50% of the circumference of the esophageal mucosal tube to allow mucosa to bulge through the muscular incision. |
The esophagomyotomy is performed opposite the site of the diverticulectomy and should be carried onto the stomach for a few millimeters and extended cephalad through all regions of the esophagus documented to have abnormal motility. If motility is normal, the esophagomyotomy should be carried to a level above the diverticulum, which is usually between the inferior pulmonary vein and the arch of the aorta. Some surgeons, including Belsey (1966), as well as Evander (1986) and Little (1988) and their coauthors, have suggested that all patients undergoing an esophagomyotomy should have a concomitant antireflux procedure. Routine use of an antireflux procedure is controversial, and many surgeons do not perform one in the absence of preoperative gastroesophageal reflux or hiatal
P.2247
hernia. If either is present, a less obstructive antireflux procedure (i.e., a modified Belsey Mark IV fundoplication), as suggested by Little and co-workers (1988), should be performed.
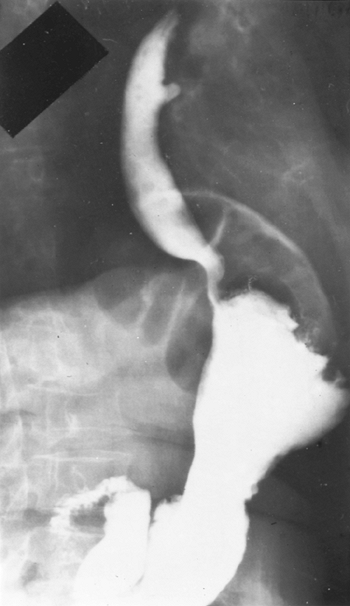 |
Fig. 148-6. Esophagus with traction diverticulum in the middle one-third of the thoracic portion in relation to subcarinal lymph nodes. Patient was asymptomatic. From Payne WS: Diverticula of the esophagus. In Payne WS, Olsen AM (eds): The Esophagus. Philadelphia: Lea&Febiger, 1974, p. 207. With permission. |
Recently, minimally invasive techniques have been proposed for the treatment of epiphrenic diverticula. Van der Peet and colleagues (2001) reported on their experience (n = 5) with a thoracoscopic approach. After Rosati and associates (1998) described less than satisfactory results with the thoracoscopic technique, they detailed their results (n = 4) with laparoscopic diverticulectomy, esophagomyotomy, and fundoplication. The benefit of the laparoscopic approach seems to derive from improved access for the myotomy portion of the procedure.
Results
Benacci and associates (1993) reviewed the Mayo Clinic experience with surgical treatment of epiphrenic diverticulum from 1975 to 1991. Among the 33 patients undergoing surgical resection, there were three operative deaths: two from esophageal leaks and one due to aspiration during a Gastrografin swallow. In all, six esophageal leaks occurred: Four were radiographic findings only and were asymptomatic. The need for meticulous surgical technique in these patients has been stressed by Orringer (1993). Paramount to achieving a good result is careful reapproximation of tissue and relief of distal obstruction.
Diverticulectomy without esophagomyotomy may be associated with recurrence or suture line complications. However, adverse sequelae are not inevitable should esophagomyotomy be omitted. One may infer from the available data that every effort should be made to correct associated esophageal conditions to minimize postoperative complications and symptoms. Early radiographic examination of the esophagus using water-soluble contrast medium prior to starting an oral diet is particularly valuable. This examination permits an assessment of the staple line at the diverticulectomy site and evaluation of the esophagogastric lumen and esophageal emptying. When a contained leak or obstruction is encountered, parenteral hyperalimentation is instituted. Restudy is performed weekly until resolution is documented. In case of a free leak in the pleural space, prompt reintervention should be considered. Patients generally are asymptomatic postoperatively if associated esophageal conditions have been adequately dealt with during the operation.
Follow-up in the 33 patients reported by Benacci and associates (1993) ranged from 4 months to 15 years, with a median of 6.9 years. Excluding the three operative deaths, all patients did well immediately after repair. Recurrent diverticulum has not developed in this group to date. Overall results were good or excellent in 22 patients (76%), fair in 5 (17%), and poor in 2 (7%). Fekete and Vonns (1992) have reported similar findings.
Surgical treatment of epiphrenic diverticulum results in resolution of symptoms in the majority of patients. Operative risks, however, are significant and relate to the difficulties in performing multiple concomitant procedures on the esophagus. Nonetheless, long-term results are acceptable and durable. Currently, there is a relative paucity of both experience and follow-up with the thoracoscopic and laparoscopic approaches. Their role in the treatment of epiphrenic diverticula remains to be defined. We hope that further understanding of the pathophysiology of epiphrenic diverticula will allow better selection of patients, reduced morbidity, and improved long-term results.
TRACTION DIVERTICULUM
The incidence of traction diverticula appears to parallel that of specific granulomatous disease, especially tuberculosis and histoplasmosis. Esophageal involvement by mediastinal granuloma is uncommon but may manifest as esophageal compression, stricture, diverticulum, sinus tract fistula, or tracheoesophageal fistula, as Dukes (1976) and MacCarty (1979) and their associates pointed out. Traction
P.2248
diverticula are usually of little clinical consequence. Because of the configuration and size of these diverticula (Fig. 148-7), symptoms are rare. Occasionally, dysphagia or odynophagia occurs, presumably due to compression, stricture, or inflammation in the diverticulum. Local esophagitis may occur, suggesting that the discharging caseous material may irritate the esophageal mucosa. Although traction diverticula are rarely complicated by esophageal motility disturbances, esophageal manometry is the most reliable means of defining these conditions. Fistulization to the tracheobronchial tree occasionally results from inflammatory necrosis of the originating granuloma, as described by Balthazar (1977). Similar but rarer communications have been found between the esophagus and great vessels, which Powell (1957), Cheitlin (1961) and Tucker (1994) and their co-workers reported. Most hemorrhagic manifestations, however, probably result from friable granulation tissue or erosion of small bronchial or esophageal vessels by calcific debris, as Schick and Yesner (1953) and Jonasson and Gunn (1965) pointed out.
When the condition is symptomatic, surgical treatment is indicated. Local excision of the diverticulum and adjacent inflammatory mass, with layered closure of the esophagus over an indwelling 40F to 50F catheter, is usually all that is required for the symptomatic uncomplicated traction diverticulum.
Fistulae with the respiratory tract or blood vessels require similar excisions as well as closure of the airway or vessel. Recurrence of fistula is minimized by the interposition of a viable pleural pedicle, connective tissue, or muscle flap. As with any esophageal suture line, care should be taken to eliminate any distal esophageal obstruction. Among the causes for acquired, nonmalignant esophagorespiratory fistulae seen at the Mayo Clinic, Wychulis and associates (1966) found that infection by tuberculosis or fungi was second only to trauma in frequency. Others, including Davis and co-workers (1956) and Hutchin and Lindskog (1964), have commented on the occurrence of this occult but common cause for acquired tracheoesophageal fistula. The chance that such a fistula would develop in a patient with a traction diverticulum of the esophagus is probably remote. Such a possibility, however, should be considered in a patient with chronic suppurative lung disease or in one with symptoms of cough after swallowing.
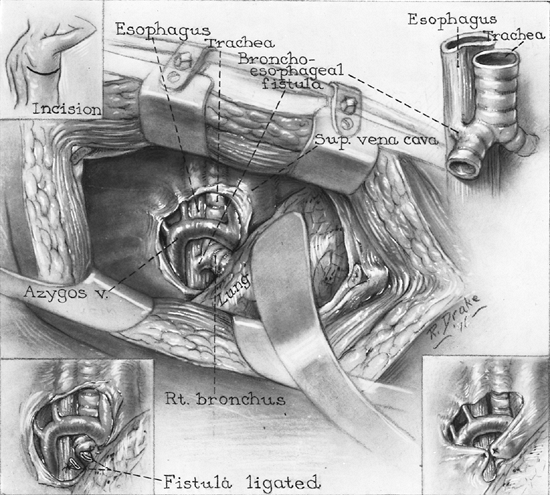 |
Fig. 148-7. Technique for closing acquired esophagobronchial fistula as a complication of a traction diverticulum of the esophagus (upper left inset). Right posterolateral thoracotomy incision (center). Surgical exposure. Lung has been retracted anteriorly. Note the relationship of the esophagus, right main bronchus, and fistula to neighboring structures (upper right and lower left insets). Fistula before division and after division and ligation (lower right inset). Method of interposing pedicles of mediastinal pleura between esophageal and bronchial closures. From Payne WS, Clagett OT: Pharyngeal and esophageal diverticula. In Ravitch MM, et al. (eds): Current Problems in Surgery. Chicago: Yearbook, 1965. With permission. |
In evaluating such patients, radiographic examination of the esophagus should be performed. Cinefluoroscopy during the ingestion of contrast medium usually defines the site and size of the communication and aids in screening patients suspected of having a fistula. Many such patients are actually aspirating ingested material through the larynx because of some mechanism other than a fistula. Endoscopic examination of both the esophagus and the tracheobronchial tree is indicated, and the orifices of the fistula usually can be identified. The introduction of methylene blue or other dye into the esophagus during bronchoscopy may facilitate this identification. Appropriate biopsy material should be obtained
P.2249
for histopathologic and microbiological study, although viable organisms are rarely identified. If symptoms suggest chronic pulmonary suppuration, computed tomographic (CT) scanning of the lungs is indicated. This will delineate the extent of bronchiectasis that might require surgical management at the time of fistula repair. In addition to division of the fistula and repair of the esophagus and airway, attention must be paid to correction of any distal esophageal obstruction, whether it is organic or is one of the defined esophageal motility disturbances.
Esophagovascular fistulas, such as those reported by Schick and Yesner (1953), Powell (1957) and Jonasson and Gunn (1965), are rare complications of traction diverticula. Impressive hemorrhage may occur without communication with a major vessel; fortunately, this may provide additional time for orderly study and treatment. Unfortunately, initial bleeding is sudden, massive, and fatal when major vessels are involved. In addition to standard endoscopic and radiographic studies, selective arteriography during active bleeding can help define the site of hemorrhage.
DIFFUSE INTRAMURAL ESOPHAGEAL DIVERTICULOSIS
Diffuse intramural esophageal diverticulosis is a rare disease that usually presents as dysphagia. These patients are commonly found to have high esophageal strictures secondary to chronic inflammation, and fibrosis. The pathologic basis of this disease was reviewed by Medeiros and colleagues (1988) and is thought to be due to dilatation of the deep esophageal glands within the wall of the esophagus, forming pseudo-diverticula. A clear association with a distinct motility disorder has not been found. Cases of rupture of these pseudo-diverticula have been reported, such as that of Abrams and colleagues (1995). Although there is no specific treatment for diffuse intramural esophageal diverticulosis, the strictures involved in this disease can usually be treated by bougie dilation for symptomatic relief.
REFERENCES
Abrams LJ, Levine MS, Laufer I: Esophageal peridiverticulitis: an unusual complication of esophageal intramural pseudodiverticulosis. Eur J Radiol 19:139, 1995.
Allen TH, Clagett OT: Changing concepts in the surgical treatment of pulsion diverticula of the lower esophagus. J Thorac Cardiovasc Surg 50: 455, 1965.
Altorki NK, Sunagawa M, Skinner DB: Thoracic esophageal diverticula: why is operation necessary? J Thorac Cardiovasc Surg 105:260, 1993.
Balthazar EJ: Esophagobronchial fistula secondary to ruptured traction diverticulum. Gastrointest Radiol 2:119, 1977.
Barrett NR: Diverticula of the thoracic oesophagus: report of a case in which the diverticulum was successfully resected. Lancet 1:1009, 1933.
Belsey R: Functional disease of the esophagus. J Thorac Cardiovasc Surg 52:164, 1966.
Benacci JC, et al: Epiphrenic diverticulum: results of surgical treatment. Ann Thorac Surg 55:1109, 1993.
Bontempo L, et al: Esophageal motor activity in patients with esophageal diverticula. In DeMeester TR, Skinner DB (eds): Esophageal Disorders, Pathophysiology and Therapy. New York: Raven Press, 1985, p. 427.
Cheitlin MD, Kamin EJ, Wilkes DJ: Midesophageal diverticulum: report of a case with fistulous connection with the superior vena cava. Arch Intern Med 107:252, 1961.
Clagett OT, Payne WS: Surgical treatment of pulsion diverticula of the hypopharynx: one-stage resection in 478 cases. Dis Chest 37:257, 1960.
Collard JM, Otte JB, Kestens PJ: Endoscopic stapling technique of esophagodiverticulostomy for Zenker's diverticulum. Ann Thorac Surg 56:573, 1993.
Cook IJ, et al: Pharyngeal (Zenker's) diverticulum is a disorder of upper esophageal sphincter opening. Gastroenterology 103:1229, 1992.
Crescenzo DG, et al: Zenker's diverticulum in the elderly: is operation justified? Ann Thorac Surg 66:347, 1998.
Cross FS, Johnson GF, Gerein AN: Esophageal diverticula: associated neuromuscular changes in the esophagus. Arch Surg 83:525, 1961.
Davis FW, Katz S, Peabody JW Jr: Broncholithiasis, a neglected cause of bronchoesophageal fistula. JAMA 160:555, 1956.
Debas HT, et al: Physiopathology of lower esophageal diverticulum and its implications for treatment. Surg Gynecol Obstet 151:593, 1980.
Dodds WJ, et al: Distribution of esophageal peristaltic pressure in normal subjects and patients with esophageal diverticulum. Gastroenterology 69:584, 1975.
Dohlman G, Mattsson O: The role of the cricopharyngeal muscle in cases of hypopharyngeal diverticula: a cineroentgenographic study. Am J Roentgenol 81:561, 1959.
Dukes RJ, et al: Esophageal involvement with mediastinal granuloma. JAMA 236:2313, 1976.
Duranceau AC, Rheault MJ, Jamieson GG: Physiologic response to cricopharyngeal myotomy and diverticulum suspension. Surgery 94:655, 1983.
Ellis FH Jr, et al: Cricopharyngeal myotomy for pharyngo-esophageal diverticulum. Ann Surg 170:340, 1969.
Evander A, et al: Diverticula of the mid and lower esophagus: pathogenesis and surgical management. World J Surg 10:820, 1986.
Fekete F, Vonns C: Surgical management of esophageal thoracic diverticula. Hepatogastroenterology 39:97, 1992.
Gr goire J, Duranceau A: Surgical management of Zenker's diverticulum. Hepatogastroenterology 39:132, 1991.
Gutschow CA, et al: Management of pharyngoesophageal (Zenker's) diverticulum: which technique? Ann Thorac Surg 74:1677, 2002.
Habein HC, Moersch HJ, Kirklin JW: Diverticula of the lower part of the esophagus: a clinical study of one hundred forty-nine nonsurgical cases. Arch Intern Med 97:768, 1956a.
Habein HC, et al: Surgical treatment of lower esophageal pulsion diverticula. Arch Surg 72:1018, 1956b.
Harrington SW: Pulsion diverticula of hypopharynx: a review of forty-one cases in which operation was performed and a report of two cases. Surg Gynecol Obstet 69:364, 1939.
Hoehn JG, Payne WS: Resection of pharyngoesophageal diverticulum using stapling device. Mayo Clin Proc 44:738, 1969.
Holinger PH, Schild JA: The Zenker's (hypopharyngeal) diverticulum. Ann Otol Rhinol Laryngol 78:679, 1969.
Huang B, Payne WS, Cameron AJ: Surgical management for recurrent pharyngoesophageal (Zenker's) diverticulum. Ann Thorac Surg 37:189, 1984a.
Huang B, Unni KK, Payne WS: Long-term survival following diverticulectomy for cancer in pharyngoesophageal (Zenker's) diverticulum. Ann Thorac Surg 38:207, 1984b.
Hutchin P, Lindskog GE: Acquired esophagobronchial fistula of infectious origin. J Thorac Cardiovasc Surg 48:1, 1964.
Jonasson OM, Gunn LC: Midesophageal diverticulum with hemorrhage: report of a case. Arch Surg 90:713, 1965.
Kaye MD: Oesophageal motor dysfunction in patients with diverticula of the mid-thoracic oesophagus. Thorax 29:666, 1974.
Lahey FH, Warren KW: Esophageal diverticula. Surg Gynecol Obstet 98: 1, 1954.
Lerut T, et al: Does the musculus cricopharyngeus play a role in the genesis of Zenker's diverticulum? Enzyme histochemical and contractility properties. In Siewert JR, Holscher AM (eds): Diseases of the Esophagus. New York: Springer, 1988.
Lerut T, et al: Pharyngo-oesophageal diverticulum (Zenker's): clinical, therapeutic, and morphological aspects. Acta Gastroenterol Belg 53: 330, 1990.
P.2250
Lerut T, et al: Zenker's diverticulum: is a myotomy of the cricopharyngeus useful? How long should it be? Hepatogastroenterology 39:127, 1992.
Little AG, et al: Surgical treatment of achalasia: results with esophagomyotomy and Belsey repair. Ann Thorac Surg 45:489, 1988.
Ludlow A: A case of obstructed deglutition, from a preternatural dilation of, and bag formed in the pharynx. Med Observations Inquiries, Soc Phys (London) 3:85, 1769.
MacCarty RL, et al: Radiographic findings in patients with esophageal involvement by mediastinal granuloma. Gastrointest Radiol 4:11, 1979.
Medeiros LJ, Doos WG, Balogh K: Esophageal intramural pseudodiverticulosis: a report of two cases with analysis of similar, less extensive changes in normal autopsy esophagi. Hum Pathol 19:928, 1988.
Mondiere JT: Notes sur quelques maladies de l'oesophage. Arch Gen Med Paris 3:28, 1833.
Moynihan B: Diverticula of the alimentary canal. Lancet 1:1061, 1927.
Negus VE: Pharyngeal diverticula: observations on their evolution and treatment. Br J Surg 38:129, 1950.
Nehra D, et al: Physiologic basis for the treatment of epiphrenic diverticulum. Ann Surg 235:346, 2002.
Orringer MB: Extended cervical esophagomyotomy for cricopharyngeal dysfunction. J Thorac Cardiovasc Surg 80:669, 1980.
Orringer MD: Epiphrenic diverticula: fact and fable [Editorial]. Ann Thorac Surg 55:1067, 1993.
Payne WS: Diverticula of the esophagus. In Payne WS, Olsen AM (eds): The Esophagus. Philadelphia: Lea&Febiger, 1974, p. 207. Payne WS: The treatment of pharyngoesophageal diverticulum: the simple and complex. Hepatogastroenterology 39:109, 1992.
Payne WS, Clagett OT: Pharyngeal and esophageal diverticula. Curr Probl Surg 3:131, 1965.
Payne WS, Reynolds RR: Surgical treatment of pharyngoesophageal diverticulum (Zenker's diverticulum). Surg Rounds 5:18, 1982.
Peracchia A, et al: Minimally invasive surgery for Zenker diverticulum: analysis of results in 95 consecutive patients. Arch Surg 133:695, 1998.
Powell MEA: A case of aorticoesophageal fistula. Br J Surg 45:55, 1957.
Rocco G, et al: Results of reoperation on the upper esophageal sphincter. J Thorac Cardiovasc Surg 117:28, 1999.
Rosati R, et al: Diverticulectomy, myotomy, and fundoplication through laparoscopy: a new option to treat epiphrenic esophageal diverticula? Ann Surg 227:174, 1998.
Sauvanet A, et al: Cancer on an esophageal diverticulum. Presse Med 21: 305, 1992.
Schick A, Yesner R: Traction diverticulum of esophagus with exsanguination: report of a case. Ann Intern Med 39:345, 1953.
Shallow TA, Clerf LH: One stage pharyngeal diverticulectomy: improved technique and analysis of 186 cases. Surg Gynecol Obstet 86:317, 1948.
Shaw DW, et al: Influence of surgery on deglutitive upper oesophageal sphincter mechanics in Zenker's diverticulum. Gut 38:806, 1996.
Sutherland HD: Cricopharyngeal achalasia. J Thorac Cardiovasc Surg 43: 114, 1962.
Sweet RH: Pulsion diverticulum of the pharyngoesophageal junction: technic of the one-stage operation; a preliminary report. Ann Surg 125: 41, 1947.
Terracol J, Sweet RH: Diseases of the Esophagus. Philadelphia: WB Saunders, 1958, p. 264.
Trastek VF, Payne WS: Esophageal diverticula. In Shields TW (ed): General Thoracic Surgery. Philadelphia: Lea and Febiger, 1989, p. 989.
Tucker LE, Aquino T, Sasser W: Mid-esophageal traction diverticulum: rare cause of massive upper gastrointestinal bleeding. Mol Med 91:140, 1994.
van der Peet DL, et al: Epiphrenic diverticula: minimal invasive approach and repair in five patients. Dis Esophagus 14:60, 2001.
van Overbeek JJM: The Hypopharyngeal Diverticulum: endoscopic treatment and manometry. Assen, Netherlands: Van Gorcum, 1977.
van Overbeek JJM: Meditation on the pathogenesis of hypopharyngeal (Zenker's) diverticulum and a report of endoscopic treatment in 545 patients. Ann Otol Rhinol Laryngol 103:178, 1994.
van Overbeek JJM: Microendoscopic CO2 laser surgery of the hypopharyngeal (Zenker's) diverticulum. Adv Otorhinolaryngol 49:140, 1995.
Viard H, et al: Le traitement chirurgical des diverticules de pulsion de l'oesophage. J Chir (Paris) 124:658, 1987.
Welsh GR, Payne WS: The present status of one-stage pharyngo-esophageal diverticulectomy. Surg Clin North Am 53:953, 1973
Vinson PP: Diverticula of the thoracic portion of the esophagus: report of forty-two cases. Arch Otolaryngol 19:508, 1934.
Wychulis AR, Ellis FH Jr, Anderson HA: Acquired nonmalignant esophagotracheobronchial fistula: report of 36 cases. JAMA 196:117, 1966.
Wychulis AR, Gunnlaugsson GH, Clagett OT: Carcinoma occurring in pharyngo-esophageal diverticulum: report of three cases. Surgery 66: 976, 1969.
Zenker FA, von Ziemssen H: Krankheiten des Oesophagus. In von Ziemssen H (ed): Handbuch der speziellen Pathologie und Therapie. Vol. 7, Part 1. Leipzig: FCW Vogel, 1874.
EAN: 2147483647
Pages: 203