7 - Urinary Tract Infection
Editors: Schrier, Robert W.
Title: Manual of Nephrology, 6th Edition
Copyright 2005 Lippincott Williams & Wilkins
> Table of Contents > 7 - The Patient with Urinary Tract Infection
function show_scrollbar() {}
7
The Patient with Urinary Tract Infection
Marilyn E. Levi
Jay Redington
L. Barth Reller
Urinary tract infections (UTIs) are some of the most common infections experienced by humans, exceeded in frequency among ambulatory patients only by respiratory and gastrointestinal infections. Indeed, bacterial infections of the urinary tract are the most common cause of both community-acquired and nosocomial infections for patients admitted to hospitals in the United States. The prognosis and management of UTIs, however, depend on the site of infection and any predisposing factors.
Definitions. Some definitions are necessary, because infection of the urinary tract may result from microbial invasion of any of the tissues extending from the urethral orifice to the renal cortex. Although the infection and resultant symptoms may be localized at one site, the presence of bacteria in the urine (bacteriuria) places the entire urinary system at risk of invasion by bacteria.
Significant bacteriuria is defined as the presence of 100,000 or more colony-forming units (CFU) of bacteria per mL of urine, although smaller colony counts can be of diagnostic importance, particularly in young women, where 1,000 bacteria per CFU may be associated with cystitis or acute uretheral syndrome.
Anatomic location. The first useful distinction is between upper (kidney) and lower (bladder, prostate, and urethra) UTIs. Infections confined to the bladder (cystitis), the urethra (urethritis), and the prostate (prostatitis) commonly cause dysuria, frequency, and urgency. Pyelonephritis is the nonspecific inflammation of the renal parenchyma; acute bacterial pyelonephritis is a clinical syndrome characterized by chills and fever, flank pain, and constitutional symptoms caused by the bacterial invasion of the kidney. Chronic pyelonephritis has a histopathology that is similar to tubulointerstitial nephritis, a renal disease caused by a variety of disorders, such as chronic obstructive uropathy, vesical ureteral reflux (reflux nephropathy), renal medullary disease, drugs and toxins, and possibly chronic or recurring renal bacteriuria.
Recurrence of UTI is the result of either relapse or reinfection; making this distinction is clinically important. Reinfection is a recurring infection due to a different microorganism, which is usually drug-susceptible. Most recurring episodes of cystourethritis are due to reinfection. Relapse is a return of infection due to the same microorganism, which often is drug-resistant. Most relapses occur after treatment of acute pyelonephritis or prostatitis. Finally, asymptomatic bacteriuria is an important clue to the presence of parenchymal infection somewhere in the urinary tract; however, the importance of the infection and the need for treatment depend on the age, sex, and underlying condition of the patient.
Complicated and uncomplicated UTIs. For the clinician, another important distinction is made between uncomplicated and complicated infections. An uncomplicated infection is an episode of cystourethritis following bacterial colonization of the urethral and bladder mucosae in the absence of upper tract disease. This type of infection is considered uncomplicated because sequelae are rare and exclusively due to the morbidity associated with reinfections in a subset of women. Complicated UTIs may also occur with pregnancy, diabetes, immunosuppression, structural abnormalities of the urinary tract, symptoms lasting for greater than 2 weeks, and previous pyelonephritis. Young women constitute a subset of patients with
P.92
pyelonephritis (acute uncomplicated pyelonephritis) who often respond well to therapy and may also have a low incidence of sequelae. In contrast, complicated infections include those involving parenchyma (pyelonephritis or prostatitis) and frequently occur in the setting of obstructive uropathy or after instrumentation. Episodes may be refractory to therapy, often resulting in relapses, and occasionally leading to significant sequelae such as sepsis, metastatic abscesses, and, rarely, acute renal failure.Several authors have proposed a clinical classification for the practicing clinician (1).
Asymptomatic bacteriuria
Acute uncomplicated cystitis in women
Recurrent infections in women
Acute uncomplicated pyelonephritis in women
Complicated UTIs in both sexes
Catheter-associated UTIs
Risk factors and pathogenesis. Early recognition and possible prevention depend on an understanding of the pathogenesis and epidemiology of UTIs. Figure 7-1 shows the major risk periods of life for symptomatic UTIs; the increasing prevalence of asymptomatic bacteriuria that accompanies aging is apparent. Much has been learned about the risk factors for UTIs (2). Associations have been established between UTI and age; pregnancy; sexual intercourse; use of diaphragms, condoms, and spermicides, particularly Nonoxynol-9; delayed postcoital micturition; menopause; and a history of recent UTI. Factors that do not seem to increase the risk include diet, use of tampons, clothing, and personal hygiene, including directions of cleansing after defecation and
P.93
bathing practices. Studies on pathogenesis have elucidated specific interactions between the host and microbes that are causally related to bacteriuria. Bacteria in the enteric flora periodically gain access to the genitourinary tract. How such bacteria actually migrate from the gastrointestinal tract to the periurethra is not known; close proximity of the anus in women is a likely factor. The subsequent bacterial colonization of uroepithelial cells is the biological phenomenon that sets the stage for persistent bacteriuria. The colonization of the periurethra often precedes the onset of bladder bacteriuria. P-fimbriated strains of Escherichia coli adhere to uroepithelial cells, in which glycolipids function as receptors in women who secrete blood group antigens. E. coli that encode for the type 1 pilus, which contains the adhesin FimH, recognizes multiple cell types associated with cystitis, sepsis, and meningitis. Immunocompromised patients may become infected with less virulent E. coli strains. Opposing colonization are several host factors, most notably acid pH, normal vaginal flora, and type-specific cervicovaginal antibodies.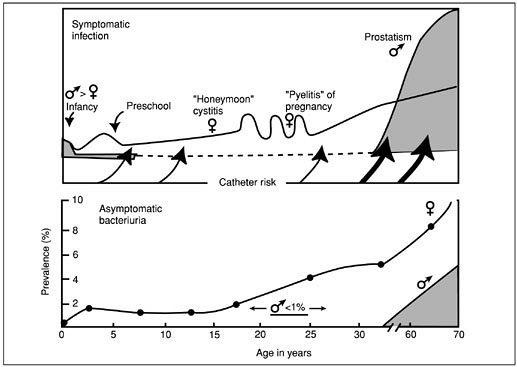
Figure 7-1. Frequency distribution of symptomatic urinary tract infections and prevalence of asymptomatic bacteriuria by age and sex (male, shaded area; female, line). (Modified from Jawetz's original concept. From Kunin CM. Detection, prevention and management of urinary tract infections, 4th ed. Philadelphia: Lea & Febiger, 1987. Reprinted with permission.)
After periurethral colonization, uropathogens gain access to the bladder via the urethra, to the kidneys via the ureters, and to the prostate via the ejaculatory ducts. The urethra and ureterovesical junction are mechanical barriers that prevent ascension. Aside from instrumentation and mechanical obstruction, however, factors promoting ascent of bacteria are not as well understood. In the bladder, organisms multiply, colonize the bladder mucosa, and invade the mucosal surface. Although urine adequately supports the growth of most uropathogens, the bladder has several mechanisms that prevent bacteriuria: (a) a mucopolysaccharide (urine slime) layer covers the bladder epithelium and prevents colonization; (b) Tamm-Horsfall protein, which is a component of uromucoid, adheres to P fimbriae and prevents colonization; and (c) urine flow and bladder contraction serve to prevent stasis and colonization. Bladder bacteriuria sets the stage for subsequent migration to the kidneys, where organisms such as P-fimbriated E. coli adhere to renal tubular cells. In fact, outside the setting of obstructive nephropathy, this strain of E. coli is the most common cause of pyelonephritis. With obstruction, however, bacterial adherence is ostensibly unimportant. Other host factors that prevent a renal infection are a high urine osmolality, high ammonium concentration, phagocytes, and increased urine flow rate.
Clinical setting
Asymptomatic bacteriuria is especially common in women, as evidenced by a minimum prevalence of 2% to 4% in young and 10% in elderly women and a 3 to 4 times higher prevalence of asymptomatic bacteruria in diabetic women compared to their nondiabetic counterparts. The cumulative prevalence of asymptomatic bacteriuria in women increases about 1% per decade throughout life. Of note, this phenomenon has been observed in different ethnic groups and geographic locations. In contrast to women, the occurrence of asymptomatic bacteriuria in men is rare until after the age of 60 years, at which time the prevalence increases per decade and often approaches the rate in elderly women. For example, in noncatheterized, institutionalized elderly men, the prevalence of bacteriuria exceeds 20%. Prostatic hypertrophy and increased likelihood of instrumentation are thought to account for the bacteriuria of older men. Moreover, differences between men and women in the rates of bacteriuria have been attributed to the shorter female urethra and its proximity to the vaginal and rectal mucosae and the abundant microbial flora of these areas.
Symptomatic UTIs occur in all age groups. Among newborns and infants, boys are affected more often than girls. When the urinary tract is the source of neonatal sepsis, serious underlying congenital anomalies are frequently present. During childhood, persistent bacteriuria, with or without repeated symptomatic episodes, occurs in a small group (less than 2%) of school-aged girls. Such girls, and also school-aged boys with bacteriuria, should have a urologic evaluation to detect correctable structural abnormalities when UTIs are documented. Sexually active women have a markedly increased
P.94
risk of episodes of cystitis. E. coli is the predominant organism in 75% to 90% of cases, whereas Staphylococcus saprophyticus is found in 5% to 15%, primarily in young women. The remainder of cases are due to enterococci and aerobic gram-negative rods, such as Klebsiella species and Proteus mirabilis.In the absence of prostatitis, bacteriuria and symptomatic UTIs are unusual in men. In fact, asymptomatic prostatitis is very common in men presenting with febrile UTIs. More recently, uropathogenic strains of E. coli have been recognized as causes of cystitis in young men at risk because of homosexuality and anal intercourse, lack of circumcision, or having a partner with vaginal colonization with such P-fimbriated E. coli. At any age, both sexes may develop symptomatic infections in the presence of risk factors that alter urinary flow.
Obstruction to urine flow
Congenital anomalies
Renal calculi
Ureteral occlusion (partial or total)
Vesicoureteral reflux
Residual urine in bladder
Neurogenic bladder
Urethral stricture
Prostatic hypertrophy
Instrumentation of urinary tract
Indwelling urinary catheter
Catheterization
Urethral dilation
Cystoscopy
Clinical features
Acute urethral syndrome. The cardinal symptoms of frequency and dysuria occur in more than 90% of ambulatory patients with acute genitourinary tract infections. One-third to one-half of all patients with frequency and dysuria, however, do not have significant bacteriuria, although most have pyuria. These patients have acute urethral syndrome, which can mimic both bladder and renal infections. Vaginitis, urethritis, and prostatitis are common causes of the acute urethral syndrome. Although certain signs and symptoms help to differentiate these clinical entities, a classic UTI can be definitively diagnosed only by quantitative cultures of urine.
Vaginitis. Approximately 20% of women in the United States have an episode of dysuria each year, and one-half of these seek medical care. The presence of an abnormal vaginal discharge (leukorrhea) and irritation makes vaginitis the likely cause of dysuria, unless a concomitant UTI can be confirmed by culture. Candida albicans, the most common specific cause of vaginitis, can be demonstrated readily by culture or by finding yeast cells in a Gram-stained smear of vaginal secretions or in a saline preparation with potassium hydroxide added. Trichomoniasis can be documented with a saline preparation that shows the motile protozoa of Trichomonas vaginalis. Nonspecific vaginitis most often is associated with Gardnerella vaginalis. A clue to this diagnosis is the presence of many small gram-negative bacilli that adhere to vaginal epithelial cells.
Urethritis. Acute urinary frequency, dysuria, and pyuria in the absence of vaginal symptoms favor a diagnosis of urethritis or UTI rather than vaginitis. Chlamydia trachomatis is a common cause of the acute urethral syndrome in women, as well as of nonspecific urethritis in men. Neisseria gonorrhoeae is also a widespread cause of urethritis and dysuria. The diagnosis and treatment of gonorrhea are now well standardized. Low colony count (100 to 1,000 CFU) infections with coliforms are now a recognized cause of urethritis in symptomatic young women with pyuria. Herpes simplex virus, usually type 2, is another sexually transmitted
P.95
agent that can cause severe dysuria through ulcerations in close proximity to the urethral orifice. The diagnosis of herpes progenitalis can be confirmed by finding giant multinucleated transformed cells in epidermal scrapings stained with Wright's stain (Tzanck smear), by isolating the virus in tissue culture, or by direct fluorescent antibody test.Prostatitis. Prostatitis is a common affliction in men that causes dysuria and urinary frequency in middle-aged and younger men more frequently than UTIs do. In addition, over 90% of men with febrile UTIs have asymptomatic prostatitis manifested by elevated prostate specific antigens (PSAs) and prostate volume. The PSA may remain elevated for up to 12 months. Prostate syndromes have classically been divided into four clinical entities: (a) acute bacterial prostatitis, (b) chronic bacterial prostatitis, (c) nonbacterial prostatitis, and (d) prostatodynia.
Acute bacterial prostatitis is easily distinguished from the other prostatitis syndromes by its acute characteristics. The patient often appears acutely ill, with the sudden onset of chills and fever, urinary frequency and urgency, dysuria, perineal and low back pain, and constitutional symptoms. Rectal examination should not be performed because of the risk of precipitating sepsis, but it may disclose an exquisitely tender, hot, and swollen prostate gland. Microscopical examination of the urine usually displays numerous white blood cells. Urine culture is usually positive for enteric gram-negative bacteria (especially E. coli); gram-positive bacteria (staphylococci and enterococci) are less frequently isolated.
Chronic bacterial prostatitis. A hallmark of chronic prostatitis is relapsing UTIs. Urinary frequency, dysuria, nocturia, and low back and perineal pain are the usual symptoms, although patients may have a minimum of symptoms between UTIs. The patient is often afebrile, does not appear acutely ill, and may have an unremarkable prostate examination. A proposed mechanism to explain the migration of bacteria into the prostate is by reflux of urine and bacteria into the prostatic ducts from the urethera. This syndrome is distinguished from other forms of chronic prostatitis by displaying an initial negative midstream urine examination and culture; after prostate massage, however, the urine displays a positive microscopical examination for white blood cells, and a uropathogen can be cultured (see section V). Nonbacterial prostatitis is the most common form of chronic prostatitis. It mimics chronic bacterial prostatitis clinically and displays inflammatory cells on post prostate massage specimens. However, bacteriologic cultures of urine and prostatic secretions are sterile. The etiology is unknown, but some evidence exists for an infectious etiology involving organisms that are difficult to culture.
Prostatodynia has also been referred to as chronic noninflammatory prostatitis. Clinically, it presents with symptoms similar to other forms of chronic prostatitis. It is distinguished by the absence of inflammatory cells or uropathogens from all specimens.
UTIs. Despite the mimicking syndromes, a presumptive diagnosis of infections of the urinary tract can be established economically by analyzing urine in patients with characteristic, albeit nonspecific, signs and symptoms. Acute uncomplicated UTIs occur mainly in women of childbearing age. The presenting features are only suggestive of the site of infection. Patients with bacterial cystourethritis, as distinct from urethritis caused by a sexually transmitted disease (STD) pathogen, will have had prior episodes, experienced symptoms for less than 1 week, and will experience suprapubic pain.
Laboratory diagnosis
Urine specimens for culture
Indications. The diagnosis of UTI, from simple cystitis to complicated pyelonephritis with sepsis, can be established with absolute certainty
P.96
only by quantitative cultures of urine. The major indications for urine cultures are:Patients with symptoms or signs of UTIs
Follow-up of recently treated UTI
Removal of indwelling urinary catheter
Screening for asymptomatic bacteriuria during pregnancy
Patients with obstructive uropathy and stasis before instrumentation
When universally applied, the first two indications may not be the most cost effective approach to diagnosing UTIs in nonpregnant, young-adult women. These individuals present with dysuria, urgency, and pyuria due to an uncomplicated episode of cystourethritis, with organisms usually susceptible to a variety of antimicrobial agents, or due to an STD pathogen such as gonococcus or chlamydia. Moreover, because the beneficial outcome of therapy is to minimize morbidity rather than prevent life-threatening complications, laboratory costs and use of resources can be minimized if pretreatment cultures are not ordered in this clinical setting. Therefore, women with symptoms consistent with simple uncomplicated lower tract disease and a positive urine dipstick can be treated without obtaining a urine culture. Additionally, if symptoms completely resolve, posttreatment cultures also are unnecessary for patients with uncomplicated infections.
Methods. Urine specimens must be cultured promptly within 2 hours or be preserved by refrigeration or a suitable chemical additive (e.g., boric acid sodium formate preservative). Acceptable methods of collection are:
Midstream urine voided into a sterile container after careful washing (water or saline) of external genitalia (any soap must be rinsed away)
Urine obtained by single catheterization or suprapubic needle aspiration of the bladder
Sterile needle aspiration of urine from the tube of a closed catheter drainage system (do not disconnect tubing to get specimen)
Not acceptable, because of constant contamination and the impossibility of quantitative counts, are tips from indwelling urinary catheters and urine obtained randomly, without adequate patient preparation. The clean-voided, midstream technique of collection is preferred whenever possible to avoid the risk of introducing infection at the time of catheterization, a hazard in elderly patients confined to bed, in men with condom catheters, and in diabetic patients with dysfunctional bladders. Because contamination is exceedingly rare in circumcised men, a clean-catch, midstream specimen is unnecessary in such patients. Occasionally, suprapubic aspiration of the bladder is necessary to verify infection. This technique has been most helpful in obtaining specimens from possibly septic infants and from adults in whom repeated clean-voided specimens have yielded equivocal colony counts on culture.
The usual microbial pathogens isolated from patients with UTIs are listed in Table 7-1. Results of cultures highly depend, however, on the clinical setting in which bacteriuria occurs. For example, E. coli is found in the urine of 80% to 90% of patients with acute uncomplicated cystitis and acute uncomplicated pyelonephritis. Many patients with staghorn calculi of the kidneys harbor urea-splitting Proteus organisms in their urine. Klebsiella, Pseudomonas aeruginosa, and Enterobacter infections are commonly acquired in the hospital. The presence of Staphylococcus aureus in the urine most often is a clue to concomitant staphylococcal bacteremia, unless an underlying risk factor exists. Microorganisms in young men are similar to the organisms that cause uncomplicated infections in women. Enterococci and coagulase-negative staphylococci are more common in elderly men, most likely representing recent instrumentation or catheterization. C. albicans is rarely encountered, except
P.97
P.98
in patients with indwelling catheters, nosocomial UTIs, or relapsing infections after multiple courses of antibiotic therapy. Although the likely microorganism and usual susceptibility patterns are sufficient to guide the initial empiric therapy of uncomplicated cystitis, adequate treatment of acute bacterial pyelonephritis and complicated UTIs necessitates precise therapy based on isolation of the causative bacterium and standardized antimicrobial susceptibility testing using the disc-diffusion or the broth- or agar-dilution methods.Table 7-1. Microbial Pathogens of Kidney and Bladder
Organism Uncomplicated cystitis: young womena (%) Pyelonephritis: outpatient, womenb (%) UTI: menc (%) Bacteremic UTIsd (%) Nosocomial UTIse (%) Gram-negative bacteria Escherichia coli 79 86 41 54 29 Klebsiella pneumoniae 3 4 3 9 8 Proteus 2 3 6 8 4 Enterobacter 0 0 1 2 4 Pseudomonas aeruginosa 0 0 NS 3 9 Gram-positive bacteria Staphylococcus saprophyticus 11 3 NS 0 0 Staphylococcus aureus 0 1 1 13 Staphylococcus not aureus 0 0 5 1 5 Enterococci 2 0 5 6 13 Other bacteria 0 4 19 4 15 Mixed infections 3 3 18 2 NS Yeast 0 0 0 3 13 NS, not stated; UTIs, urinary tract infections. aData from 607 episodes of cystitis; from Stamm WE. Urinary tract infections. In: Root RK, ed. Clinical infectious diseases: a practical approach, 1St ed. New York: Oxford University Press, 1999. bEighty-four episodes from Stamm 1992 and 54 nonhospitalized women; from Pinson AG, Philbrock JT, Lindbeck GH, Schorling JB, eds. Management of acute pyelonephritis in women: a cohort study. Am J Emerg Med 1994;12:271 278. cData from 223 outpatient males with symptoms; from Pead L, Maskell R. Urinary tract infections in adult men. J Infect 1981;3:71 78. d185 cases (excluding five cases of Candida albicans); from Ackermann RJ, Monroe PW. Bacteremic urinary tract infections in older people. J Am Geriat Soc 1996;44:927 933. e90% catheter-associated infections, 1991 experience at the University of Iowa (900-bed hospital); from Bronsema DA, Adams JR, Pallares R, Wenzel RP. Secular trends in rates and etiology of nosocomial urinary tract infections at a university hospital. J Urol 1993;150:414 416.
Interpretation of urine cultures. Organisms residing in the distal urethra and on pubic hairs contaminate voided, clean-catch specimens. This bacterial contamination must be distinguished from true infection or significant bacteriuria in urine cultures. Quantitative bacteriology makes this distinction. Because quantitation of bacteriuria is so important clinically, methods for culture of urine must enable the CFU number of a potential pathogen per mL of urine to be assessed. The standard procedure involves the use of calibrated bacteriologic loops that deliver a known volume of urine to the surface of agar plates. Proper plating techniques achieve isolated colonies that can be enumerated accurately. A satisfactory alternative for the diagnosis of uncomplicated UTIs is the dipslide method, which is particularly well suited to quantitative urine cultures in smaller clinics. Rapid methods based on filtration and colorimetry, bioluminescence, growth kinetics, and biochemical reactions are used increasingly to screen urine specimens for the presence of bacteria. The sensitivities of these rapid assays are in the range of 104 to 105 CFU per mL. The simplest screen is the paper-strip test for detection of leukocyte esterase and nitrite in first morning urine specimens. However, these methods are not a substitute for standard cultures in symptomatic patients with complicated UTIs.
Colony counts. Figure 7-2 shows a basic guide to the interpretation of quantitative cultures of urine. Colony counts greater than 105 CFU per mL in properly collected and transported specimens usually indicate infection. Colony counts of 103 or fewer CFU per mL from untreated patients are uncommon with true UTIs, except in symptomatic young
P.99
women with pyuria and urethritis, in whom colony counts of E. coli as low as 103 may be interpretable if the urine was obtained by single catheterization. Intermediate counts, especially with mixed flora, usually imply poor collection or delayed transport and culture. Brisk diuresis may transiently reduce an otherwise high colony count.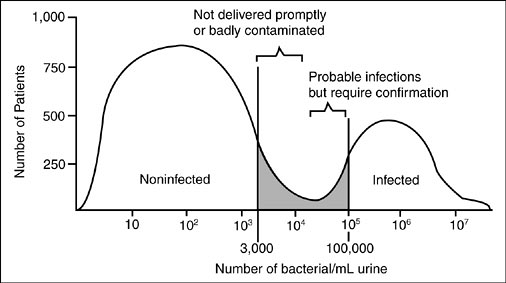
Figure 7-2. Results of quantitative bacterial counts from cultures of urine specimens. (From Brumfitt W, Percival A. Pathogenesis and laboratory diagnosis of nontuberculous urinary tract infection: a review. J Clin Pathol 1964; 17:482. Reprinted with permission.)
Suprapubic needle aspiration. Any growth from urine obtained by suprapubic needle aspiration may be important. Use of a 0.01-mL quantitative loop for culturing aspirated urine permits the detection of as few as 100 CFU per mL. Two or more colonies (less than or equal to 200 CFU per mL) of the same microorganism ensure the purity of growth from such specimens and permit standardized antimicrobial susceptibility testing. Similar criteria should be used for patients who are receiving antimicrobials at the time of culture. Except in unusual circumstances, the isolation of diphtheroids, alpha-hemolytic streptococci, and lactobacilli indicates contamination of the urine specimen with vaginal or periurethral flora.
Prostatic secretions. In men, the distinction between a urinary source and a prostatic focus of infection must be made. The procedure for obtaining voided urine and expressed prostatic secretions in partitioned segments that enable proper interpretation is diagrammed in Figure 7-3. Leukocytes (greater than 10 to 15 white blood cells per high-power field) and lipid-laden macrophages are seldom observed in the expressed
P.100
prostatic secretion of healthy men. These agents signify prostatic inflammation. Therefore, a prostatic focus of infection should be considered when a significant step-up of pyuria or colony counts occurs in the prostate specimens. A UTI of prostatic origin is indicated by colony counts of 105 or more CFU per mL of the same microorganism in all four specimens. Both urologists and primary care physicians underuse this procedure. In one study, a two-step procedure involving microscopical examination and culture of pre- and post prostate massage urine specimens compared favorably to this four-step procedure. This simplified approach was able to arrive at a similar diagnosis in 91% of patients. Further trials are needed to evaluate this approach, which may improve physician use.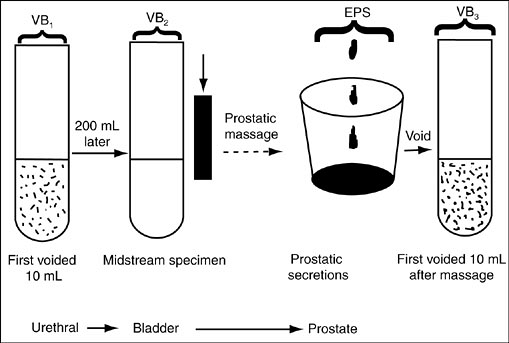
Figure 7-3. Localization of infection with segmented cultures of the lower urinary tract in men. VBl is the first 10 mL of voided urine, and VB2 is the midstream specimen of urine obtained before prostatic massage. Subsequently, the expressed prostatic secretions (EPS) are collected before the final voided urine specimen (VB3). When the bacterial colony counts in the urethral culture exceed by tenfold or more those of the midstream and prostatic cultures, the urethra is the source of the infection. The diagnosis is bacterial prostatitis if the quantitative counts of the prostatic specimens exceed those of the urethral and midstream samples. (From Meares EM, Stamey TA. Bacteriologic localization patterns in bacterial prostatitis and urethritis. Invest Urol 1968; 5:492. Reprinted with permission.)
Microscopic examination of urine. Procedures for the microscopical examination of urine are poorly standardized; nonetheless, visualization of bacteria leukocytes and epithelial cells in urine can provide some useful information and enable the clinician to make a presumptive diagnosis of UTI. The advantages of microscopical analysis are immediate availability and low cost. The disadvantages, depending on the method, are lack of sensitivity, specificity, or both. Only properly collected and processed specimens for quantitative urine cultures can provide definitive diagnosis. The microscopical examination can be done on either unspun urine or the centrifuged sediment. A critical comparison of these two techniques is not available. The presence of squamous epithelial cells and mixed bacterial flora indicates contamination and the need for a repeat specimen.
Unspun urine. When fresh, unspun urine from patients with significant bacteriuria (greater than 105 CFU per mL) is examined microscopically (X1,000), 90% of specimens show one or more bacteria, and 75% of specimens show one or more white blood cells per oil-immersion field. The best assessment of pyuria is the finding of approximately 10 white blood cells per mm3 of unspun urine examined in a counting chamber.
Centrifuged sediment. After 10 mL of urine is centrifuged in a standard 15-mL conical tube for 5 minutes at 2,500 revolutions per minute in a clinical centrifuge, three or four drops of the sediment are examined under a coverslip at high power (X400) in diminished light. Patients with significant bacteriuria usually show bacilli in the urinary sediment, whereas only approximately 10% of patients with fewer than 105 CFU per mL show bacteria. Approximately 60% to 85% of patients with significant bacteriuria have ten or more white blood cells per high-power field in the sediment of midstream voided urine; however, approximately 25% of patients with negative urine cultures also have pyuria (ten or more white blood cells per high-power field), and only approximately 40% of patients with pyuria have 105 or more bacteria per mL of urine by quantitative culture. The principal pitfall is false-positive pyuria owing to leukocytes from a contaminating vaginal discharge.
Gram's stain. A simple Gram-stained smear of unspun urine or spun sediment can enhance the specificity of the test, because morphology and stain characteristics aid in identifying the likely pathogen and in targeting empiric therapy.
Pyuria. Although the presence of pyuria in a midstream specimen has low predictive value for significant bacteriuria, pyuria is a sensitive indicator of inflammation. Thus, pyuria may be more accurate than bacteriuria in distinguishing a true infection from contamination: 95% of patients with pyuria have a genitourinary tract infection; however, pyuria cannot distinguish a bacterial UTI from acute urethral syndrome. In addition to a UTI, any of the causes of acute urethral syndrome (see section IV.A) can result in pyuria. For example, tuberculosis is a cause of pyuria with negative routine urine cultures, although mycobacterial cultures are positive in 90% of instances. Analgesic nephropathy, interstitial nephritis, perinephric abscess, renal cortical abscess, disseminated fungal infection, and appendicitis may also result in pyuria.
Biochemical tests for bacteriuria. Two metabolic capabilities shared by most bacterial pathogens of the urinary tract are use of glucose and reduction of nitrate to nitrite; these are properties of all enterobacteriaceae. Because small amounts of glucose and nitrate are normally present in urine, the presence of significant numbers of bacteria in urine results in the absence of glucose and presence of nitrite. Dipstick devices are commercially available for both types of testing. Studies with nitrite-indicator strips show that 85% of women and children with culture-confirmed significant bacteriuria show positive results if three consecutive morning urine specimens are tested. A morning urine specimen is preferred for the nitrite test, because most bacteria take 4 to 6 hours to convert nitrate to nitrite. A negative nitrite test may be observed in patients taking diuretics or with organisms that do not produce nitrate reductase (Staphylococcus species, Enterococcus species, and P. aeruginosa). The sensitivity of the glucose-use test is about 90% to 95% in patients without diabetes mellitus. Both biochemical tests have fewer than 5% false-positive results. Therefore, these biochemical tests can be used by patients or parents, after proper instruction, to determine when quantitative cultures are needed in the management of recurrent episodes of UTI. Spectrum bias in the use of dipsticks must be avoided. Dipsticks should only be used for patients with symptoms suggestive of UTI (i.e., high pretest probability of UTI), and not for asymptomatic screening, as in pregnancy.
Localization of the site of infection. The site of infection within the urinary tract has great therapeutic and prognostic importance. Upper UTI (pyelonephritis) indicates a much greater likelihood of underlying uropathy (e.g., congenital anomalies, renal stones, ureteral occlusion, vesicoureteral reflux, neurogenic bladder, or prostatic hypertrophy) or previous instrumentation (see section III.B). Relapses with the same, often multiple-antibiotic-resistant bacteria are common with pyelonephritis or chronic bacterial prostatitis. Treatment is long (minimum, 10 to 14 days) and may be arduous. On the other hand, cystitis rarely is complicated, and treatment can be short (single-dose or 3-day) and usually is easy. No ready way to distinguish between upper and lower UTIs by simple laboratory tests exists. The difficulty in making this distinction reliably on clinical grounds alone has been discussed (see section IV.B). Older, indirect methods (e.g., serum antibodies, urine concentration test, and urinary beta-glucuronidase activity) are neither sensitive nor specific. Direct methods for localization (e.g., ureteral catheterization, renal biopsy, and the bladder washout technique) are hazardous, expensive, or both. Eradication of bacteriuria with single-dose or short-course (3-day) antibiotic therapy in symptomatic patients with uncomplicated disease is a practical method for presumptive localization of infection to the bladder or urethra.
Radiography and other diagnostic procedures: indications. The principal role of radiographic and urologic studies for patients with UTIs is to detect vesicoureteral reflux, renal calculi, and potentially correctable lesions that obstruct urine flow and cause stasis. Uncomplicated reinfections (cystitis and urethritis) in women who respond to short-course antimicrobial therapy are not an indication for radiographic and cystoscopic investigation of the urinary tract. Radiologic and urologic evaluation should be considered in all children with a first episode of UTIs (except for school-aged girls). Special emphasis should be on the early detection of urologic abnormalities in all young children and boys with a first infection, as well as any child with pyelonephritis or a complicated course. A review of studies evaluating diagnostic imaging in children with UTIs expressed the need for better outcome-based research in this area. Radiologic and urologic evaluation should be considered in adults with UTIs. In the past, all UTIs in males were considered complicated. The conventional recommendation that all males presenting with initial UTIs undergo urologic evaluation to identify predisposing anatomic or functional
P.102
abnormalities is still followed. However, several studies have indicated that only approximately 20% of men have previously unidentified abnormalities. Some sexually active males are at a higher risk for cystitis (homosexual males, males with a partner who harbors a uropathogen, uncircumcised males). The value of urologic evaluation in this high-risk group, with a single episode of cystitis and an uncomplicated course, is not known. In general, urologic evaluations are recommended in the following situations: (a) males with first episode, (b) all patients with a complicated infection or bacteremia, (c) suspected obstruction or renal stones, (d) hematuria following infection, (e) failure to respond to appropriate antibiotic therapy, and (f) patients with recurrent infections.Some experts recommend the evaluation of all patients with pyelonephritis. The radiologic evaluation of a subgroup of patients with pyelonephritis (young and otherwise healthy women who respond well to therapy) may have a low diagnostic yield. In one study, only 1 of 25 young women with uncomplicated pyelonephritis had a surgically correctable etiology, and 2 of 25 had focal abnormalities that resolved on a follow-up ultrasound. This has led others to recommend a diagnostic evaluation in young women with uncomplicated pyelonephritis after the second recurrence, or at any time, if a complicating course is present. The ease in obtaining a noninvasive test (ultrasound) has increased radiologic evaluations for most patients admitted with pyelonephritis.
Ultrasound with a plain film of the abdomen has replaced the intravenous pyelogram as the initial radiologic studies for most adults. For a detailed evaluation of the ureterovesical junction, bladder, and urethra, a voiding cystourethrogram and measurement of the residual urine after voiding may be necessary. If vesicoureteral reflux is present after acute infection has been treated, a urologist should be consulted. Cystoscopy may be warranted. Renal calculi can usually be detected on a plain radiograph of the abdomen. An IVP confirms the presence and the location of calculi, detects radiolucent stones (fewer than 10% of renal calculi), and discloses the degree of obstruction and dilation. Ordinarily, radiographic studies should not be performed within 6 weeks of acute infections.
Gram-negative bacilli have the ability to impede ureteral peristalsis, and transient abnormalities of the IVP are common with acute pyelonephritis. These include hydroureter, vesicoureteral reflux, diminished pyelogram, loss of renal outline, and renal enlargement. Acute pyelonephritis with an obstructed ureter is a surgical emergency, and a perinephric abscess also requires surgical drainage. These complications, however, are best detected initially by ultrasound and by computed tomography (CT), respectively. To avoid radiocontrast-induced acute renal failure, excretory urography and other radiocontrast studies should be avoided whenever possible in patients with a serum creatinine above 1.5 mg per dL, diabetes mellitus, dehydration, or advanced age.
P.101
Treatment of UTI
Principles of underlying therapy and follow-up. To successfully treat a UTI, the clinician must have knowledge of microbial susceptibility and mechanisms of resistance, pharmacokinetics and pharmacodynamics, and status of host defenses. First, most uropathogens are susceptible to a wide range of antibiotics; however, resistant gram-negative bacteria frequently are seen with indwelling catheters, in immunocompromised patients, and in patients with relapsing bacteriuria. Second, the majority of antibiotics are filtered by the kidney and thus achieve a urinary concentration that is many times higher than the minimum inhibitory concentration. Third, although most antibiotics achieve adequate concentration in renal tissue, only tetracyclines, trimethoprim-sulfamethoxazole, and fluoroquinolones achieve any reasonable concentration in the prostate. Finally, patients with systemic or local abnormalities in host defenses usually develop a renal
P.103
infection that is refractory to therapy. In this case, antibiotics that achieve adequate serum concentrations and are bactericidal are preferable to bacterial static agents. The basic caveats for the effective management of UTIs are outlined here.Asymptomatic patients should have colony counts greater than or equal to 100,000 per mL on at least two occasions before treatment is considered.
Unless symptoms are present, no attempt should be made to eradicate bacteriuria until catheters, stones, or obstructions are removed.
Selected patients with chronic bacteriuria may benefit from suppressive therapy.
A patient who develops bacteriuria as a result of catheterization should have treatment to reestablish a sterile urine.
Antimicrobial agents used for treatment should be the safest and least expensive agents to which the causative microorganisms are susceptible.
Efficacy of treatment should be evaluated by urine culture 1 week after completion of therapy, except in nonpregnant adult women who respond to therapy for uncomplicated cystitis and uncomplicated pyelonephritis.
Antimicrobial agents
Beta-lactams. The increasing antimicrobial resistance observed in E. coli makes amoxicillin and ampicillin less attractive choices for empiric therapy in the patient with a complicated UTI, unless enterococcus is strongly considered to be the etiologic agent. Amoxicillin has replaced oral ampicillin due to improved bioavailability and less frequent dosing. Amoxicillin is effective for uncomplicated cystitis, but short-course therapy (single-dose and 3-day regimens) has generally been less effective than trimethoprim-sulfamethoxazole or fluoroquinolones given for a similar duration. Cefixime and cefpodoxime are oral third-generation cephalosporins with enhanced activity against enteric gram-negative bacteria, longer serum half-life, and less frequent dosing than first-generation cephalosporins. Parenteral beta-lactams are generally reserved for more complicated infections. Ceftriaxone is a third-generation cephalosporin with good activity against most community-acquired gram-negative enteric bacteria (except P. aeruginosa). Ceftazidime and cefepime are examples of cephalosporins with good activity against many gram-negative bacteria, including P. aeruginosa.
Nitrofurantoin is active against many uropathogens, including E. coli, Staphylococcus saprophyticus, and Enterococcus faecalis. Some gram-negative bacteria are resistant to nitrofurantoin (Klebsiella, Enterobacter, and Pseudomonas species), making it a less than ideal agent for the empiric therapy of complicated UTIs. No clinically significant increase in resistance has been observed. However, this drug is significantly less active than fluoroquinolones and trimethoprim-sulfamethoxazole against non-E. coli aerobic gram-negative rods and is inactive against Proteus and Pseudomonas species. The major role of nitrofurantoin in therapy includes the treatment of uncomplicated cystitis and as an alternative agent for cystitis caused by E. faecalis. The oral adult dose for both crystalline and macrocrystalline preparations is 50 to 100 mg every 6 hours for 7 days. Although a 3-day regimen is successful in many patients with uncomplicated cystitis, one clinical trial found nitrofurantoin to be less effective than a 3-day regimen of trimethoprim-sulfamethoxazole. Patients with renal insufficiency (creatinine clearance less than 60 mL per minute) should not receive this agent. Nitrofurantoin has been used in pregnancy [U.S. Food and Drug Administration (FDA) category B], although it is contraindicated in nursing mothers, pregnant women near term, and newborns (in whom it is associated with hemolytic anemia). Suppressive
P.104
therapy has been successful in some patients, although concern for less common reactions (e.g., peripheral neuropathy, pneumonitis, and hepatitis) may limit long-term use.Trimethoprim-sulfamethoxazole and trimethoprim. Trimethoprim-sulfamethoxazole has a wide spectrum of activity against many uropathogens. However, lack of clinical activity against enterococci and P. aeruginosa, as well as increased resistance by some enteric gram-negative bacteria (Klebsiella species, Enterobacter species), makes trimethoprim-sulfamethoxazole a less than ideal agent for the treatment of complicated UTIs. In addition, resistance patterns tabulated by microbiology laboratories show trimethoprim-sulfamethoxazole resistance variability depending on locale; an 18% incidence of resistance is present in the southeastern and western United States for women with acute cystitis who have had a UTI in the last 6 months. Therefore, some authorities recommend the use of trimethoprim-sulfamethoxazole only if (a) the local resistance pattern is less than 20%, (b) no sulfa allergy exists, and (c) no recent antibiotic use is present. Of interest, despite a 30% resistance prevalence in some locales, at least half of women treated with trimethoprim-sulfamethoxazole have 80% to 85% clinical and microbiologic cures.
Trimethoprim-sulfamethoxazole is well tolerated in most patients. Adverse effects due to sulfonamides are well described and include gastrointestinal symptoms, transient elevation in the serum creatinine, and hematologic and dermatologic reactions. Sulfonamides displace warfarin and hypoglycemic agents from albumin, thus potentiating these drug effects. Trimethoprim-sulfamethoxazole is highly effective for the prophylaxis and therapy of uncomplicated cystitis and for therapy of uncomplicated pyelonephritis. A randomized trial with four different 3-day drug regimens in women with uncomplicated acute cystitis found a 3-day regimen of trimethoprim-sulfamethoxazole was the most cost-effective. Complicated UTIs, especially catheter-associated infections and nosocomial UTIs, should have in vitro susceptibility testing performed. Trimethoprim-sulfamethoxazole has been used in pregnancy, but it is not FDA-approved for pregnant women. Other agents, such as amoxicillin, nitrofurantoin, and cephalosporins, are preferred.
Trimethoprim alone is preferred over trimethoprim-sulfamethoxazole by some experts for the prophylaxis and treatment of uncomplicated cystitis, because its efficacy is similar and the side effects fewer (because of the absence of sulfamethoxazole). This agent should not be used alone for the therapy of complicated UTIs.
Trimethoprim monotherapy also achieves good prostate concentrations and is an alternative to fluoroquinolones depending on the susceptibility pattern of the bacteria.
Multiple fluoroquinolones are now available for clinical use (Tables 7-2 and 7-3). These agents achieve very high concentrations in the urine and renal tissue, easily exceeding the minimal inhibitory concentration of most uropathogens. Fluoroquinolones should not be used as first-line agents for the therapy of uncomplicated cystitis because of concern for the development of resistance and because of the cost. However, their antimicrobial spectrum and generally low side-effect profile make them excellent choices for empiric therapy of complicated UTIs. Among current agents within this antimicrobial class, no particular drug has demonstrated superior clinical efficacy for the therapy of patients with UTIs. An exception is moxifloxacin, which does not achieve adequate urinary concentrations and should be avoided in the treatment of UTIs. Fluoroquinolones should not be used for enterococcal UTIs (only 60% to 70% susceptible), during pregnancy or in children (until further information is available). Aluminum- and magnesium-containing antacids and iron-,
P.105
calcium-, and zinc-containing preparations should not be administered with oral fluoroquinolones due to a significant decrease in absorption. In general, these agents are well tolerated by most patients. The most common adverse effects are gastrointestinal and on the central nervous system, but these infrequently lead to drug discontinuation. Photosensitivity may limit the use of some of these agents (e.g., lomefloxacin, sparfloxacin). Many of these agents are available for both parenteral and oral administration. Conversion from parenteral to oral therapy (step-down therapy) should be considered for patients who are clinically stable and tolerating oral medications. The excellent bioavailability of these drugs, good clinical success with oral therapy, and the high cost of parenteral therapy due to intravenous catheter related complications and cost of intravenous preparations are all good reasons for considering oral therapy.Table 7-2. Oral Antimicrobial Agents Commonly Used for Treatment of Urinary Tract Infections
Adult dose Comment Miscellaneous agents Trimethoprim 100 mg every 12 hr Prophylaxis, uncomplicated cystitis Trimethoprim-sulfamethoxazole 160 mg/800 mg every 12 hr Uncomplicated cystitis; cost-effective Nitrofurantoin 50 100 mg every 6 hr Prophylaxis, uncomplicated cystitis Tetracycline 250 500 mg every 6 hr Prophylaxis Beta-lactamsa Amoxicillin 250 500 mg every 8 hr During pregnancy, enterococcal infections Cephalexin or cephradine 250 mg every 6 hr During pregnancy, uncomplicated cystitis Cefixime 200 mg every 12 h/400 mg every 24 hr Step-down therapya Cefpodoxime 100 200 mg every 12 hr Step-down therapya Fluoroquinolones Norfloxacin 400 mg every 12 hr Low serum drug levels Ciprofloxacin 250 500 mg every 12 hr First systemic fluoroquinolone Lomefloxacin 400 mg every 24 hr Skin photosensitivity reactions Enoxacin 400 mg every 12 hr P-450 drug interactionsb Ofloxacin 200 400 mg every 12 hr Generally replaced by levofloxacin Levofloxacin 250 500 mg every 24 hr L-isomer of ofloxacin Note: Comments for miscellaneous agents and beta-lactams relate to role in therapy. The role of fluoroquinolones has been for treatment of complicated UTIs and as an alternative agent for uncomplicated cystitis. Because these agents have not been rigorously compared, comments are related to general spectrum of activity, side-effect profile, and drug interactions. aShort-course therapy for uncomplicated cystitis has generally been less effective than the use of trimethoprim-sulfamethoxazole or fluoroquinolones for a similar duration. The general role of extended-spectrum oral cephalosporins (cefixime, cefpodoxime) has been for the treatment of complicated UTIs (alternative agent) and for intravenous to oral step-down therapy. bEnoxacin is a potent inhibitor of P-450 hepatic isoenzymes. (Inhibition of hepatic isoenzymes causes an elevation of serum levels of theophylline and caffeine.) Table 7-3. Intravenous Antimicrobial Agents Commonly Used for Treatment of Urinary Tract Infections (UTIs)
Adult dose Comment Beta-lactams Ampicillin 1 2 g every 4 hr Enterococcus faecalis; usually combined with gentamicin Ceftriaxone 1 g every 12 24 hr Pyelonephritis Ceftazidime 1 2 g every 8 12 hr Complicated UTI, including Pseudomonas aeruginosa Cefepime 1 2 g every 12 hr Complicated UTI, including Pseudomonas aeruginosa Aztreonam 1 g every 8-12 hr Penicillin-allergic patient Fluoroquinolonesa Ciprofloxacin 200 400 mg every 12 hr Ofloxacin 200 400 mg every 12 hr Generally changed to levofloxacin Levofloxacin 500 mg every 24 h Miscellaneous agents Trimethoprim-sulfamethoxazole 160 mg/800 mg every 12 hr Prophylaxis, uncomplicated cystitis Vancomycin 1 g every 12 hr Methicillin-resistant Staphylococcus aureus; serious enterococcal infection in the penicillin-allergic patient Gentamicin 4 7 mg/kg every 24 hr Serious gram-negative infection 1.5 2.0 mg/kg every 8 hr Older dosing schedule; for enterococcus combined with ampicillin aBecause oral fluoroquinolones have excellent bioavailability and cost approximately 20% as much as parenteral fluoroquinolones, conversion from intravenous to oral therapy should be done when the patient is clinically stable.
Treatment of asymptomatic bacteriuria
Pregnancy increases the risk of UTI complications. The rate of prematurity in children born to women who have bacteriuria during pregnancy is increased, and 20% to 40% of these patients develop pyelonephritis. Successful therapy of these patients with bacteriuria decreases the risk of symptomatic infection by 80% to 90%. Therefore, all women should be screened twice during gestation for asymptomatic bacteriuria. All bacteriuria patients should be treated for 7 days, with follow-up cultures to identify relapses. Long-term prophylaxis offers no advantage over close surveillance. In selecting therapy, the risk to the fetus should be considered. Short-acting sulfonamides or amoxicillin for 7 days usually suffices, because almost all these infections are caused by susceptible E. coli. Tetracyclines (FDA category D), trimethoprim (FDA category C), and fluoroquinolones (FDA category C) should be avoided.
Children. Asymptomatic bacteriuria in preschool- and school-aged girls may signify underlying vesicoureteral reflux. Moreover, vesicoureteral reflux, when combined with recurring bacteriuria, can result in progressive renal scarring. Therefore, in this at-risk population, asymptomatic bacteriuria should routinely be detected and treated, with follow-up urologic evaluations after 6 weeks.
General population. Asymptomatic bacteriuria in men and nonpregnant women, a common condition in the elderly, does not appear to cause renal damage in the absence of obstructive uropathy or vesical ureteral reflux. Prospective randomized studies of therapy for asymptomatic bacteriuria in the elderly have been recently reviewed. Of five clinical trials reviewed, three studies had very small sample sizes, and one non-blinded study displayed a nonstatistical significant decrease in symptomatic infections. The largest randomized trial failed to demonstrate any significant difference in mortality between treated and untreated patients. Therefore, repeated attempts to clear the bacteriuria with antimicrobial agents seem unwarranted; they may only select for more resistant microorganisms and create a need for more toxic and costly antibiotics should the patient subsequently develop symptoms.
Miscellaneous. Instrumentation of the genitourinary tract should be avoided in patients with asymptomatic bacteriuria or, if necessary, done under the cover of prophylactic antimicrobial therapy. Selected high-risk patients (e.g., with renal transplantation or neutropenia) may benefit from therapy for asymptomatic bacteriuria.
P.107
Treatment of uncomplicated cystitis. Acute cystitis and low-colony-count coliform urethritis are almost exclusively diseases of women, mostly sexually active women between the ages of 15 and 45 years. Although reinfection is common, complications are rare.
Short-course therapy. Appreciable evidence exists that infections truly confined to the bladder or urethra respond as well to single-dose or short-course (3-day) therapy as to conventional therapy for 10 to 14 days. Indeed, response to single-dose or short-course therapy implies a lower UTI. Reviews of short-course therapy have concluded that 3-day regimens are more effective than single-dose therapy. One randomized trial evaluated four different 3-day drug regimens in women with uncomplicated acute cystitis. A 3-day regimen of trimethoprim-sulfamethoxazole was more effective than a 3-day regimen of nitrofurantoin. Cure rates for cefadroxil (66%) and amoxicillin (67%) were not statistically different from the cure rate for trimethoprim-sulfamethoxazole (82%). The 3-day regimen of trimethoprim-sulfamethoxazole was the most cost-effective regimen. Further clinical trials are needed to evaluate other patients with uncomplicated cystitis and to measure the impact of newer agents (fluoroquinolones) on outcomes and cost effectiveness. Recommended oral 3-day regimens include trimethoprim-sulfamethoxazole, trimethoprim, and a fluoroquinolone. This variety of treatments is an important breakthrough in the management of uncomplicated cystitis and coliform urethritis, because all patients were treated formerly with the standard 10 to 14 days of therapy. Diabetic women with uncomplicated infections (i.e., with normal urinary tracts) may also be treated with a 3-day course of antibiotic therapy. Post-treatment urine cultures are not required unless symptoms persist. Formal urologic imagings, such as ultrasound, intravenous pyelography, and CT, are not needed in most cases, as correctable abnormalities are rarely found.
Seven-day regimen. A longer course of therapy for cystitis should be considered in patients with complicating factors that lead to a lower success rate and a higher risk of relapse. These complicating factors include a history of prolonged symptoms (more than 7 days), recent UTI, diabetic patients with abnormal urinary tracts, age older than 65 years, and use of a diaphragm. Importantly, the elderly frequently have concurrent renal bacteriuria; thus, short-course therapy should not be used.
Symptomatic pyuria without bacteriuria in an otherwise healthy young person suggests chlamydial or gonococcal urethritis. The importance of documenting these infections as well as screening for other STDs (e.g., human immunodeficiency virus infection, syphilis), and the necessity of counseling about STD risk reduction cannot be understated.
P.108
Recent guidelines suggest that either a single dose of azithromycin or a 7-day course of doxycycline is effective for chlamydial urethritis. Therapy for gonococcal urethritis includes a single dose of ceftriaxone or cefixime, or a fluoroquinolone combined with therapy for chlamydial infection.
Management of recurrent cystitis (reinfections). Ten to twenty percent of women develop recurrent UTIs within several months. Some infections are related to inadequate antimicrobial therapy. It is common, however for women whose periurethral and vaginal epithelial cells avidly support attachment of coliform bacteria to suffer from recurrent episodes of cystitis in the absence of recognized structural abnormalities of the urinary tract. A recent prospective study of UTIs in young women identified recent use of a diaphragm and spermicide such as Nonoxynol-9, recent sexual intercourse, and a history of recurrent infection as risk factors for infection.
Antimicrobial strategies. Strategies for managing the disease of women with frequent episodes of cystitis include (a) postcoital prophylaxis, (b) continuous low-dose prophylaxis, (c) patient self-administered therapy, and (d) consideration of contraception or barrier methods against STDs without the use of vaginal spermicides. Postcoital prophylaxis is most helpful for patients who associate recurrent UTIs with sexual intercourse. In these women, a single dose of an antimicrobial after sexual intercourse or thrice weekly at bedtime has been shown to significantly reduce the frequency of episodes of cystitis from an average of three per patient-year to 0.1 per patient-year. Women with frequent recurrent infections (more than three UTIs per year) are offered these prophylactic regimens. Women with fewer than three UTIs per year can be offered self-administered treatment. Multiple antimicrobial agents have demonstrated efficacy in prophylaxis and self-administered therapy. Some of these regimens include nitrofurantoin, 50 or 100 mg; trimethoprim, 100 mg; trimethoprim-sulfamethoxazole, 40 mg per 200 mg; and cephalexin, 250 mg. Fluoroquinolones and cephalosporins are also effective but are more expensive. Although antimicrobial prophylaxis is effective and usually safely tolerated for months to years, single-dose therapy for acute cystitis makes prophylaxis more expensive and possibly more hazardous for most patients because of alterations in fecal and vaginal bacterial flora. Indeed, self-administration of a single-dose regimen at the onset of symptoms has proved to be as cost-effective as prophylaxis.
Nonantimicrobial prophylaxis issues. Encouraging women to practice regular and complete emptying of the bladder may help prevent recurrent cystitis. Postcoital emptying of the bladder has also been widely recommended, although one prospective study failed to demonstrate any relationship with recurrent infections. Moreover, several theoretical preventive measures relate to the use of an alternative contraceptive method: to use a properly fitted diaphragm, to void frequently when wearing a diaphragm, and to limit diaphragm use to the recommended 6 to 8 hours after intercourse. In postmenopausal women, intravaginal administration of estriol can reduce recurrent UTIs by modifying the milieu for vaginal flora. Cranberry juice (300 mL per day) was effective in decreasing asymptomatic bacteriuria with pyuria in postmenopausal women. The small difference in symptomatic UTIs was not statistically significant.
Treatment of acute bacterial pyelonephritis. The occurrence of flank pain, chills and fever, and nausea and vomiting with or without dysuria suggests acute bacterial pyelonephritis. In this clinical setting, blood cultures and quantitative cultures of urine should be obtained. Whether ambulatory patients should be admitted to the hospital for treatment depends in part on a subjective assessment of toxicity, likely compliance with therapy, and the home situation. When the assessment is doubtful, the patient should be treated in the hospital, at least until a clear response to therapy
P.109
has occurred. This policy also applies to patients with known underlying uropathies, because complications are more common in these patients.Outpatient therapy. Recommendations for therapy of uncomplicated pyelonephritis are outlined in Table 7-4. Fluoroquinolone or trimethoprim-sulfamethoxazole is the drug of choice for initial therapy of pyelonephritis in outpatients. Local susceptibility patterns will influence
P.110
the choice for initial therapy. After culture results and susceptibility tests are available, a full 10- to 14-day course of antimicrobial therapy may be completed with the least expensive drug to which the patient's microorganism is susceptible.Table 7-4. Recommendations for Therapy for Urinary Tract Infections
Infection Group Medication Duration Uncomplicated cystitis Young women Trimethoprim-sulfamethoxazole, trimethoprim, fluoroquinolonea 3 d Cystitis Women with risk factors including recent UTI, symptoms >7 d, diaphragm use, age >65 yr, diabetics with abnormal GU structures Trimethoprim-sulfamethoxazole, trimethoprim, fluoroquinolone, nitrofurantoin, cephalosporins 7 d Pregnant women Amoxicillin, cephalosporinsb, nitro-furantoin, sulfonamides, trimethoprim-sulfamethoxazolec 7 d Acute uncomplicated pyelonephritis Women (outpatient) Fluoroquinolone, trimethoprim-sulfamethoxazole, oral cephalosporind 10 14 d Women (inpatient) Fluoroquinolonee, ceftriaxone, ampicillin plus gentamicinf, trimethoprim-sulfamethoxazole 14 d Complicated infection Outpatient Fluoroquinolone 10 14 d Inpatient Fluoroquinolonee, cephalosporinsg, ampicillin plus gentamicinf 14 d UTI, urinary tract infection. aOral fluoroquinolones are listed in Table 7-2; they offer no significant advantage over trimethoprim-sulfamethoxazole in women with uncomplicated cystitis. bOral cephalosporins: cephradine, cephalexin. cTrimethoprim-sulfamethoxazole has been used in pregnancy, but it has not been approved by the U.S. Food and Drug Administration for pregnant patients. dOral cephalosporins with an extended spectrum: cefpodoxime, loracarbef. eFluoroquinolones available for intravenous administration are listed in Table 7-3. fIncreasing ampicillin resistance among many enteric bacteria, including Escherichia coli, limits ampicillin as a single agent for complicated UTIs. If enterococcus is not likely, then a fluoroquinolone or a parenteral third- or fourth-generation cephalosporin is recommended. gSome examples of parenteral cephalosporins are listed in Table 7-3. Adapted from Falagas ME. Practice guidelines: urinary tract infections. Infect Dis Clin Pract 1995;4:241 257; Kunin CM. Detection, prevention, and management of urinary tract infections, 5th ed. Philadelphia: Lea & Febiger, 1997; Stamm WE. Urinary tract infections. In: Root RK, ed. Clinical infectious diseases: a practical approach, 1st ed. New York: Oxford University Press, 1999. Inpatient therapy. Patients who require admission to the hospital should be treated initially with a third-generation cephalosporin or a fluoroquinolone (intramuscular or intravenous), or gentamicin or tobramycin (1.5 to 2.0 mg per kg every 8 hours or 4.0 to 7.0 mg per kg every 24 hours, with appropriate alteration of the dose interval if the serum creatinine exceeds 1 mg per dL) if the urine shows gram-negative bacilli on microscopical examination. If gram-positive cocci are seen in the urine, intravenous ampicillin (l g every 4 hours) should be given in addition to the aminoglycoside, to cover the possibility of enterococcal infection while the results of urine and blood cultures and antimicrobial susceptibility tests are pending. If no complications ensue and the patient becomes afebrile, the remaining days of a 10- to 14-day course can be completed with oral therapy. However, persistent fever, persistent bacteriuria in 48 to 72 hours, or continual signs of toxicity beyond 3 days of therapy suggest the need for an evaluation to exclude obstruction, metastatic focus, or the formation of a perinephric abscess. The urinary tract is a common source of sepsis and bacteremic shock in patients with underlying uropathies. As with other patients in septic shock, intravenous fluids must be given to maintain adequate arterial perfusion, which usually results in a urinary output in excess of 50 mL per hour. Failure to respond to seemingly appropriate therapy suggests the possibility of undrained pus. Examination by ultrasound or CT may disclose an obstructed ureter or perinephric abscess, both of which require surgical drainage.
Management of recurrent renal infections (relapses). Chronic bacterial pyelonephritis is one of the most refractory problems in clinical medicine; relapse rates are as high as 90%. The entity is a heterogeneous one with multiple underlying factors.
Risk factors. To improve the success rate, it is of utmost importance that any correctable lesion be repaired, that obstructions to urine flow be relieved, and that foreign bodies (e.g., indwelling urinary catheters or renal staghorn calculi) be removed if possible. If the risk factors cannot be corrected, long-term eradication of bacteriuria is almost impossible. To attempt eradication in such instances leads only to the emergence of more resistant strains of bacteria or fungi; consequently, the physician must be resigned to treating symptomatic episodes of infection and suppressing bacteriuria in selected patients.
Acute symptomatic infection. The treatment of the acute symptoms and signs of UTI in a patient with chronic renal bacteriuria is the same as for patients with acute bacterial pyelonephritis. Urine cultures to detect a possible change in antimicrobial susceptibility of the infecting microorganism are important. Toxic patients also should have blood cultures.
Prolonged treatment. Some patients with relapsing bacteriuria after 2 weeks of therapy respond to 6 weeks of antimicrobial therapy. This is especially true of patients with no underlying structural abnormalities. Men may require 6 to 12 weeks of antibiotic therapy for febrile UTIs, since over 90% have associated asymptomatic prostatitis. Patients who fail the longer therapy, who have repeated episodes of symptomatic infection, or who have progressive renal disease despite corrective measures are candidates for suppressive chemotherapy.
Suppressive therapy. To reduce the colony counts in their urine, patients selected for suppressive therapy should have 2 to 3 days of specific high-dose antimicrobial therapy, to which their infecting bacteria are susceptible. The preferred agent for long-term suppression is methenamine mandelate, 1 g four times daily in adults. To be most effective, the pH of the urine should be maintained below 5.5; this can be accomplished
P.111
with ascorbic acid, 500 mg two to four times daily. Alternatively, the dosage of methenamine mandelate alone can be increased to 8 g or even 12 g per day. The dosage should be adjusted to the minimum amount required to keep the urine free of bacteria. To avoid metabolic acidosis, the dosage of methenamine mandelate must be reduced in patients with renal insufficiency, in whom 2 g per day may suffice. In these patients, methenamine mandelate should not be used at all unless the creatinine clearance exceeds 10 mL per minute. Alternative therapy is trimethoprim-sulfamethoxazole (160 mg/800 mg tablets twice daily) or nitrofurantoin (50 to 100 mg once or twice daily).Prognosis. Although a common cause of appreciable morbidity, UTIs do not play a major role in the pathogenesis of end-stage renal disease. Patients who come to renal dialysis or transplantation because of chronic bacterial pyelonephritis almost always have an underlying structural defect. Most often, the lesion is chronic atrophic pyelonephritis associated with vesicoureteral reflux that started in infancy. The role of surgical correction of vesicoureteral reflux is not clear despite years of debate; what is certain, however, is the importance of meticulous control of infection in children to prevent progressive renal scarring and renal failure by early adulthood.
Treatment of prostatitis
Acute bacterial prostatitis is commonly accompanied by acute cystitis, which enables the recovery of its causative pathogen by culture of voided urine. Massage of an acutely inflamed prostate gland often results in bacteremia; therefore, this procedure should be avoided unless the patient is already receiving effective antibiotic therapy. Antimicrobial selection depends on (a) the susceptibility pattern of the causative bacteria and (b) the ability of the drug to achieve concentrations in the prostate that exceed the minimum inhibitory concentrations of the bacteria. The drug of choice most commonly is either the combination of trimethoprim-sulfamethoxazole (cotrimoxazole) or a fluoroquinolone; treatment, however, must be based ultimately on an accurate microbiological diagnosis. Beta-lactam antibiotics should be avoided because of the low concentrations achieved in prostatic tissue and lower cure rates. Treatment should be given for 30 days to prevent chronic bacterial prostatitis. After acute symptoms subside, a suitable oral antibiotic can be given in full dose for at least 30 days. Urethral catheterization should be avoided. If acute urinary retention develops, drainage should be by suprapubic needle aspiration or, if prolonged bladder drainage is required, by a suprapubic cystostomy tube, placed while the patient is under local anesthesia.
Chronic bacterial prostatitis. The hallmark of chronic bacterial prostatitis is relapsing UTI. It is most refractory to treatment. Although erythromycin with alkalinization of the urine has been effective against susceptible gram-positive pathogens, most instances of chronic bacterial prostatitis are caused by gram-negative enteric bacilli. Cotrimoxazole or a fluoroquinolone is the drug of choice. Approximately 75% of patients improve, and 33% are cured with 12 weeks of cotrimoxazole therapy (160 mg/800 mg twice daily). For patients who cannot tolerate cotrimoxazole or a fluoroquinolone, nitrofurantoin, 50 or 100 mg once or twice daily, can be used for long-term (6 to 12 months) suppressive therapy.
The therapy for nonbacterial chronic prostatitis is difficult because an exact etiology has not been identified. Due to a concern for C. trachomatis, Ureaplasma urealyticum, and other fastidious and difficult to culture organisms, many experts recommend a 6-week trial of a tetracycline or erythromycin. Symptomatic therapy with nonsteroidal anti-inflammatory drugs (NSAIDs) and alpha-receptor blockers has also been used.
Recommendations for the care of urinary catheters. Urinary catheters are valuable devices for enabling drainage of the bladder, but their use is
P.112
associated with an appreciable risk of infection in the urinary tract. For a single (in-and-out) catheterization, the risk is small (12%), though this prevalence is much higher in diabetic and elderly women. However, bacteriuria occurs in virtually all patients with indwelling urinary catheters within 3 to 4 days unless placement is done under sterile conditions and a sterile, closed drainage system is maintained (Fig. 7-4). The use of a neomycin-polymyxin irrigant does not prevent catheter-associated infections. Urinary catheters are the single most common cause of nosocomial infections and are responsible for more than 5,000 deaths from gram-negative sepsis each year in the United States. Explicit recommendations for the prevention of catheter-associated UTIs, formulated by the Centers for Disease Control and Prevention, are as follows: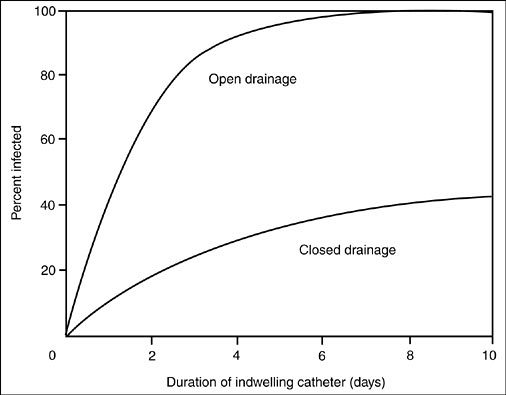
Figure 7-4. Prevalence of bacteriuria in catheterized patients according to duration of catheterization and type of drainage system. (From Fass RJ, Klainer AS, Perkins RL. Urinary tract infection: practical aspects of diagnosis and treatment. JAMA 1973;225:1509. Reprinted with permission.)
Indwelling urinary catheters should be used only when absolutely necessary. They should never be used solely for nurse or physician convenience, and they should be removed as soon as possible.
Catheters should be inserted only by adequately trained personnel. If practical, a team of individuals should be given responsibility for catheter insertion and maintenance.
Urinary catheters should be aseptically inserted using proper sterile technique and the following sterile equipment: gloves, a fenestrated drape, sterile sponges and an iodophor solution for periurethral cleansing, a lubricant jelly, and an appropriately sized urinary catheter. After insertion, catheters should be properly secured to prevent movement and urethral traction.
Once- or twice-daily perineal care for catheterized patients should include cleansing of the meatal-catheter junction with an antiseptic soap; subsequently, an antimicrobial ointment may be applied.
A sterile closed drainage system should always be used. The urinary catheter and the proximal portion of the drainage tube should not be disconnected (thus opening the closed system) unless it is required for irrigation of an obstructed catheter. Sterile technique must be observed whenever the collecting system is opened and catheter irrigation is done. A large-volume sterile syringe and sterile irrigant fluid should be used and then discarded. If frequent irrigations are necessary to ensure catheter patency, a triple-lumen catheter that permits continuous irrigation within a closed system is preferable.
Small volumes of urine for culture can be aspirated from the distal end of the catheter with a sterile syringe and 21-gauge needle. The catheter must first be prepared with tincture of iodine or alcohol. Urine for chemical analyses can be obtained from the drainage bag in a sterile manner.
Nonobstructed gravity flow must be maintained at all times. This requires emptying the collecting bag regularly, replacing poorly functioning or obstructed catheters, and ensuring that collection bags always remain below the level of the bladder.
All closed collecting systems contaminated by inappropriate technique, accidental disconnection, leaks, or other means should be immediately replaced.
Routine catheter change is not necessary in patients with urinary catheterization of less than 2 weeks' duration, except when obstruction, contamination, or other malfunction occurs. In patients with chronic indwelling catheters, replacement is necessary when concretions can be palpated in the catheter or when malfunction or obstruction occurs.
Catheterized patients should be separated from each other whenever possible and should not share the same room or adjacent beds if other arrangements are available. Separation of bacteriuric and nonbacteriuric patients is particularly important.
These guidelines should be adhered to meticulously, and the use of indwelling urinary catheters should be kept to a responsible minimum.
P.113
Catheter-associated infections. Catheter-associated bacteriuria should only be treated in the symptomatic patient. When the decision to treat a patient with a catheter-associated infection is made, removal of the catheter is an important aspect of therapy. If an infected catheter remains in place, relapsing infection is very common. The interaction between the organisms and catheter (foreign body) cause the organism to form a biofilm or area in which antibiotics are unable to completely eradicate these organisms. Recommendations for empiric therapy are similar to recommendations for complicated UTIs (see Table 7-4). The choice of empiric therapy is based on an initial Gram's stain of the urine, local susceptibility patterns, host factors, and the patient's recent antibiotic use. The final choice of an antibiotic and duration of therapy should be based on the identification and susceptibility of the etiologic agent and the host's response to therapy. Patients who respond rapidly to therapy may be treated for 7 days, although making firm conclusions about duration of therapy is very difficult.
Patients with candiduria may fall into several different clinical categories. Otherwise healthy patients with asymptomatic candiduria often require only a urinary catheter change and may not require antifungal therapy. On the other end of the spectrum is the immunocompromised host, in whom candiduria may represent disseminated infection. The patient with disseminated candidiasis requires systemic therapy with either fluconazole or amphotericin B or a liposomal preparation of amphotericin. General recommendations for treating patients with candiduria and without evidence of disseminated infection include the removal of the urinary catheter
P.114
and discontinuation of antibiotics. Antifungal options include either fluconazole (200 mg the first day, then 100 mg for 4 days), continuous bladder irrigation with amphotericin B (50 mg per 1,000 mL of sterile water via a three-way catheter for 5 days), or low-dose intravenous therapy with amphotericin (0.3 mg per kg in a single dose). Occasionally, longer systemic therapy with oral 5-fluorocytosine, intravenous amphotericin B, or both is required.
P.106
REFERENCES
1. Stamm WE, Hooton TM. Management of urinary tract infections in adults. N Engl J Med 1993;329:1328 1334.
2. Hooton TM, Scholes D, Hughes JP, et al. A prospective study of risk factors for symptomatic urinary tract infection in young women. N Engl J Med 1996;335:468 474.
Suggested readings
Ang BSP, Telenti A, King B, Steckelberg JM, Wilson WR. Candidemia from a urinary source: microbiological aspects and clinical significance. Clin Infect Dis 1993;17:662 666.
Domingue GJ, Hellstrom WJG. Prostatitis. Clin Microbiol Rev 1998;11:604 613.
Edelstein H, McCabe RE. Perinephric abscess: modern diagnosis and treatment in 47 cases. Medicine (Baltimore) 1988;67:118 131.
Fihn SD. Acute uncomplicated urinary tract infection in women. N Engl J Med 2003:349:259 266.
Fisher JF, Newman CL, Sobel JD. Yeast in the urine: solutions for a budding problem. Clin Infect Diseases 1995;20:183 189.
Fowler JE Jr., Pulaski ET. Excretory urography, cystography, and cystoscopy in the evaluation of women with urinary-tract infection. N Engl J Med 1981;304:462 465.
Godfrey KM, Harding MD, Zhanel GG, et al. Antimicrobial treatment in diabetic women with asymptomatic bacteriuria. N Engl J Med 2002;347:1576 1583.
Hooton TM, Fihn SD, Johnson C, Roberts PL, Stamm WE. Association between bacterial vaginosis and acute cystitis in women using diaphragms. Arch Intern Med 1989;149:1932 1936.
Hooton TM, Stamm WE. Diagnosis and treatment of uncomplicated urinary tract infections. Infect Dis Clin North Am 1997;11:551 582.
Hooton TM, Winter C, Tiu F, Stamm WE. Randomized comparative trial and cost analysis of 3-day antimicrobial regimens for treatment of acute cystitis in women. JAMA 1995;273:41 45.
Kincaid-Smith P, Becker G. Reflux nephropathy and chronic atrophic pyelonephritis: a review. J Infect Dis 1978;138:774 780.
Krieger JN. Complications and treatment of urinary tract infections during pregnancy. Urol Clin North Am 1986;13:685 693.
Kunin CM. Detection, prevention, and management of urinary tract infections, 5th ed. Philadelphia: Lea & Febiger, 1997.
Kunin CM, Chin QF, Chambers S. Indwelling urinary catheters in the elderly: relation of catheter life to formation of encrustations in patients with and without blocked catheters. Am J Med 1987;82:405 411.
Kunin CM, Van Arsdale White L, Hua TH. A reassessment of the importance of low-count bacteriuria in young women with acute urinary symptoms. Ann Intern Med 1993;119:454 460.
Lachs MS, Nachamkin I, Edelstein PH, Goldman J, Feinstein AR, Schwartz JS. Spectrum bias in the evaluation of diagnostic tests: lessons from the rapid dipstick test for urinary tract infection. Ann Intern Med 1992;117:135 140.
Lipsky BA, Baker CA. Fluoroquinolone toxicity profiles: a review focusing on new agents. Clin Infect Dis 1999;28:352 364.
Nickel JC. The Pre and Post Massage Test (PPMT): a simple screen for prostatitis. Tech Urol 1997;3:38 43.
P.115
Nicolle LE. Asymptomatic bacteriuria in the elderly. Infect Dis Clin North Am 1997;11:647 662.
Nicolle LE, Bjornson J, Harding GK, MacDonell JA. Bacteriuria in elderly institutionalized men. N Engl J Med 1983;309:1420 1425.
Nicolle LE, Harding GK, Preiksaitis J, Ronald AR. The association of urinary tract infection with sexual intercourse. J Infect Dis 1982;146:579 583.
Silverman DE, Stamey TA. Management of infection stones: the Stanford experience. Medicine (Baltimore) 1983;62:44 51.
Stamm WE. Guidelines for prevention of catheter-associated urinary tract infections. Ann Intern Med 1975;82:386 390.
Stamm WE, Counts GW, Wagner KF, et al. Antimicrobial prophylaxis of recurrent urinary tract infections: a double-blind, placebo-controlled trial. Ann Intern Med 1980;92:770 775.
Stapleton A, Latham R, Johnson C, Stamm WE. Postcoital antimicrobial prophylaxis for recurrent urinary tract infection: a randomized, double-blind, placebo-controlled trial. JAMA 1990;264:703 706.
Stapleton A, Stamm WE. Prevention of urinary tract infection. Infect Dis Clin North Am 1997;11:719 733.
Strom BL, Collins M, West SL, Kreisberg J, Weller S. Sexual activity, contraceptive use and other risk factors for symptomatic and asymptomatic bacteriuria: a case-control study. Ann Intern Med 1987;107:816 823.
Talan DA, Klimberg IW, Nicolle LE, Song J, Kowalsky SF, Church DA. Once daily, extended release ciprofloxacin for complicated urinary tract infections and acute uncomplicated pyelonephritis. J Urol 2004 Feb;171(2):734 739.
Ulleryd P. Febrile urinary tract infection in men. Intnl J Antimicrobial Agents 2003;22:S89 S93.
Velasco M, Martinez JA, Moreno-Martinez A, et al. Blood cultures for women with uncomplicated acute pyelonephritis: are they necessary? Clin Infect Dis 2003;37:1127 1130.
Warren JW. Catheter-associated urinary tract infections. Infect Dis Clin North Am 1997;11(3):609 622.