29 - Pneumonectomy and Its Modifications
Editors: Shields, Thomas W.; LoCicero, Joseph; Ponn, Ronald B.; Rusch, Valerie W.
Title: General Thoracic Surgery, 6th Edition
Copyright 2005 Lippincott Williams & Wilkins
> Table of Contents > Volume I - The Lung, Pleura, Diaphragm, and Chest Wall > Section VII - Pulmonary Resections > Chapter 37 - Complications of Pulmonary Resection
function show_scrollbar() {}
Chapter 37
Complications of Pulmonary Resection
Ronald B. Ponn
Operations for lung resection vary widely, from a small pneumonotomy for enucleation of a peripheral hamartoma to a radical pneumonectomy. Although most procedures are unilateral, synchronous bilateral resections are not uncommon. In addition, the procedures may be extended to include removal of portions of the chest wall, diaphragm, pericardium, and other adjacent structures. Large airways and pulmonary arteries may be reconstructed to preserve lung parenchyma in order to avoid pneumonectomy. Another variable is the method of exposure (various types of thoracotomy and video-assisted thoracic surgery). The technical aspects and some of the problems associated with specific operations and incisions are discussed in Chapters 25,26,27,28,29,30,31,32,33,34,35 and 36. Despite marked improvement in the morbidity and mortality of pulmonary resection over the years, complications will occur, as in all areas of medical treatment. Some may be anticipated, whereas others are purely random. The goal is to minimize the complication rate by optimizing preoperative assessment and preparation, intraoperative management, and postoperative care and by reviewing individual, institutional, national, and international experience.
INTRAOPERATIVE COMPLICATIONS
The three major life-threatening complications during the operation, other than those associated with the anesthetic management of the patient (Chapters 22, 23 to 24), are injury to a major vessel with massive hemorrhage, cardiac arrhythmias and myocardial ischemia, and the development of a contralateral pneumothorax. Intraoperative complications that do not present an immediate threat to life but often cause significant morbidity and sometimes mortality postoperatively include injuries to an intrathoracic nerve, the thoracic duct, the esophagus, the spinal cord, or the dura. Because the consequences of these injuries are usually not detected during the operation, they are discussed as early postoperative complications. Similarly, tumor embolization is a rare occurrence that may be potentially lethal during lung resection but is more often diagnosed postoperatively.
Injury to a Major Pulmonary Vessel
The avoidance and management of an injury to a major pulmonary vessel are discussed in Chapter 26. It should be stressed that at times, in order to obtain proximal control, the vessel must be exposed intrapericardially. Digital control of bleeding is almost always possible while blood is made available and proximal dissection carried out.
Intraoperative Cardiac Complications
Intraoperative cardiac arrhythmias and myocardial ischemia occur most often in patients with underlying cardiac disease, but may also be caused by temporary physiologic derangements in patients without clinical heart disease. The former problem is best avoided by the preoperative identification of high-risk cases and, when indicated, the use of a Swan-Ganz catheter and appropriate prophylactic preoperative and intraoperative medications to minimize ischemia. In all cases, factors that may produce cardiac dysfunction (most often hypoxemia, hypokalemia, hypervolemia or hypovolemia, tachycardia, and acidosis) must be rapidly identified and corrected. Excessive manipulation of the heart can cause both arrhythmias and myocardial ischemia, due to direct effects and hypotension. If retraction or compression of the heart cannot be avoided, manipulation should be limited to short intervals, with predetermined hemodynamic end points and ample time for recovery between attempts.
Although the appropriate preoperative medical treatment of coronary artery disease reduces the risk of myocardial ischemia during operation, the use of prophylactic digitalization has no effect on reducing the occurrence of intraoperative arrhythmias, according to Ritchie and associates (1990, 1992). The efficacy of prophylactic calcium channel blockers such as diltiazem, which has been shown by Amar and co-workers (1997)
P.555
to be effective in reducing the incidence of postoperative supraventricular arrhythmias, is unknown.
Contralateral Pneumothorax
Contralateral tension pneumothorax is rare, Vogt-Moykopf (1990) reporting an incidence of 0.8%. It is thought to be a greater threat in patients undergoing operation for bullous or bleb disease of the lung. It may occur, however, during any thoracotomy. Vogt-Moykopf (1990) stated that it may occur during an ultraradical lymph node dissection with perforation of the mediastinal pleura, but the few I have seen have occurred as a result of the spontaneous rupture of an unsuspected contralateral bleb. As a result of positive-pressure ventilation, air accumulates in the contralateral pleural space, the lung on the affected side becomes increasingly difficult to ventilate, and the effects of insufficient gas exchange become evident. With recognition of this complication, prompt evacuation of the air from the contralateral pleural space is mandatory and is accomplished by opening the mediastinal pleura from the operative side and placing a thoracostomy tube via the mediastinum or a transcutaneous route.
POSTOPERATIVE COMPLICATIONS
Predictors of Morbidity and Mortality After Pulmonary Resection
Multiple factors influence the incidence and type of complications, both fatal and nonfatal, after pulmonary resection. These include the age and physical status of the patient (i.e., the cardiorespiratory functional status, comorbidity, and the nature of the pathologic process), the type and extent of the procedure, and the use of various neoadjuvant therapies for cancer. It is obvious that older, sicker patients undergoing more major procedures will have the highest risk. Current work, however, must focus on refinements that will allow an individualized risk assessment for a given patient that yields a reliable acute and long-term prognosis and that indicates whether operation is or is not the optimal approach. The factors discussed here are nononcologic. The advisability of primary surgery or combined approaches based on cancer-related factors is discussed in Chapters 99 and 106. Both sets of data must be synthesized in deciding whether operation is in the patient's best interest.
Although standard pulmonary function tests have long been regarded as the major predictors of pulmonary complications, the simple formulas for predicting postresection function, and therefore morbidity and mortality, appear to be no longer sufficient as sole indicators (see also Chapters 19 and 20). Melendez and Carlon (1998) found that even combining cardiac and pulmonary risk factors was not predictive of outcome for resections less than pneumonectomy. Likewise, the reports of Miller (1993) and those of Putnam (1990), Cerfolio (1996a), Morice (1992), Kearney (1994), Lewis (1994), and Wang (1999) and their associates stress more exacting preoperative functional evaluation. Wang and associates (1999) believe the diffusing capacity of the lung for carbon dioxide (Dlco) to be the most valuable single study, whereas Bolliger and colleagues (1995) believe that exercise testing with determination of maximum oxygen consumption (Vo2 max) is the single best predictor of postoperative complications. In a study by Mitsudomi and colleagues (1996) in patients who underwent pneumonectomy, elevated serum lactic dehydrogenase (LDH) level or a low predicted postoperative forced expiratory volume in 1 second (FEV1) were significantly associated with complications. Duque and co-workers (1997) reported that the presence of insulin-dependent diabetes mellitus or peripheral vascular disease increased the incidence of postoperative complications and mortality.
Rather than relying on a single or a few preoperative factors to predict complications, other authors have employed multifactorial profiles. Pierce and colleagues (1994) described the predicted postoperative product (PPP) index, and Melendez and Barrera (1998) constructed the predictive respiratory complication quotient (PRQ). Each appears to be superior to any single factor in predicting postoperative mortality and morbidity.
More recently, Harpole and associates (1999) examined major pulmonary resection using a model similar to the earlier cardiac and other major surgical studies of the Veterans Administration (VA) Surgical Quality Improvement Program. Their report included 3,516 patients who underwent lobectomy or pneumonectomy between 1991 and 1995 at a number of VA centers. The results are summarized in Table 37-1. Among other factors, older age, blood transfusion, prolonged operative time, weight loss, low serum albumin, and smoking predicted higher morbidity. As an aside comment, although we all try to influence our patients who smoke to stop or decrease their use based on general principles, a study by Nakagawa and colleagues (2001) focused on the duration of smoking cessation in relation to postresection pulmonary complications. Pulmonary morbidity occurred in 44% and 53% of recent and current smokers, respectively, as opposed to 24% of nonsmokers. Patients who stopped smoking 4 to 8 weeks preoperatively had fewer complications than those who stopped for a shorter period or not at all.
Brunelli and co-workers (1999) adapted the physiologic and operative severity score for the enumeration of mortality and morbidity (POSSUM), a profile designed for general and vascular surgery, to lung resection. These authors found a very high predictive value using this system. In two recent reports, Licker and associates (1999) and Stephan and colleagues (2000) assessed American Society of Anesthesiology (ASA) score in addition to standard preoperative factors. Both found that an ASA score of 3 or higher was an independent negative prognostic indicator. The latter authors also confirmed that standard pulmonary function testing was not valuable and that longer duration of the operative
P.556
procedure correlated with increased complications. As pointed out by Harpole and associates (1999), multifactorial predictive profiles are superior to lesser systems, but require further refinement and validation in the area of lung resection.
Table 37-1. Thirty-day Mortality and Morbidity Rates After Lobectomy and Pneumonectomy: Veterans Administration System | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Overall Mortality and Morbidity by Procedure
When reviewing the literature relevant to the mortality and morbidity of any surgical operation, attention to definitions is important. To be meaningful, operative mortality should include, at a minimum, all deaths within 30 days of operation or during the same hospitalization. Ideally any late death related to the operation should also be included, but tracking discharged patients may be a problem in some systems. Unfortunately, many reports limit mortality to the 30-day definition. It is clear that with modern intensive care; cardiac, ventilatory, and renal support; and newer antimicrobials, many (most) patients who ultimately succumb to complications can be maintained longer than 30 days. Although this chapter does not limit citations to papers with a fuller definition, readers are cautioned to be aware of this important limitation. Likewise, with respect to morbidity, one must decide what is major and what minor, what is avoidable and what not, and which complications are severe enough that, if predictable, they would lead one to advise against operation.
When thinking of pneumonectomy, two clinical adages come to mind. First, in contrast to the laws of physics, pneumonectomy is greater than the sum of its parts. This implies that resection of an equal but bilateral amount of lung tissue is associated with less morbidity than the emptying of an entire pleural space. Second, pneumonectomy itself is a disease. This implies that the life of some pneumonectomy patients is saved by the procedure, but often changed in its quality forever. Pneumonectomy patients remain at risk for life for certain late complications. These are personal observations. More important, since the prior edition of General Thoracic Surgery, several excellent studies of pneumonectomy have been published. Deslauriers and Faber (1999) edited a two-volume series of Chest Surgery Clinics of North America devoted to pneumonectomy. These two monographs are must read material for anyone
P.557
performing lung surgery. With respect to mortality, Klemperer and Ginsberg (1999) reported that there has clearly been improvement over time, citing a 4-decade (1931 to 1970) experience at the Massachusetts General Hospital with operative mortality declining by decade from 56% to 15% to 14% to 11%.
After pneumonectomy, mortality rates vary widely, from as low as 3% to as high as 30% in some settings. In patients with carcinoma of the lung undergoing standard pneumonectomy, current mortality is between 3% and 12% (Table 37-2). Ginsberg and associates (1983) in the Lung Cancer Study Group reported an overall 30-day postoperative mortality rate of 6%, as did Nagasaki and colleagues (1982). In a review of 586 pneumonectomies for lung cancer in one year in Japan, the incidence of postoperative mortality was reported by Wada and associates (1998) to be only 3.2%. In patients 70 years of age or older, the mortality rate may be as high as 30%. However, with proper preoperative selection and meticulous postoperative care, the mortality rate in patients older than 70 years may be kept as low as 6%, as reported by Ginsberg and associates (1983). Wahi (1989) and Patel (1992) and their co-workers reported a mortality rate of 13% in this older group, whereas Ishida and associates (1990) recorded no deaths after pneumonectomy in a small series of 11 patients in this age group. Roxburgh and associates (1991) noted a higher mortality rate after pneumonectomy in the elderly, but the difference was not significant. In contrast, Dyszkiewicz and co-workers (2000) experienced an operative mortality rate of 17% in 42 pneumonectomy patients older than 70 years, compared with no deaths in a similar group undergoing lobectomy or wedge resection.
Table 37-2. Mortality Rates After Pneumonectomy | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
Numerous reports, including those of Nagasaki (1982) and Cybulsky (1992) and their associates, have documented a significantly higher mortality rate for right versus left pneumonectomy, due mainly to a higher incidence of bronchopleural fistula, empyema, and pulmonary edema. In a recent report from Memorial Sloan-Kettering Cancer Center focusing on resection after induction therapy, Martin and colleagues (2001) found a striking operative mortality of 24% for right pneumonectomy versus no deaths for an approximately equal number of left pneumonectomies and only 2.4% for the entire series.
In addition to older age, right pneumonectomy, and induction therapy, other factors that may increase the risks of pneumonectomy include completion pneumonectomy, extended procedures such as carinal and extrapleural pneumonectomy, and resection for infectious and inflammatory diseases, including those that occur after prior lobectomy or lesser resection. Patients undergoing a completion pneumonectomy for a second lung cancer have a slightly higher, but not prohibitive, mortality rate than first-time pneumonectomy patients. However, as pointed out by McGovern and colleagues (1988), when the procedure is carried out for removal of a persistent or superimposed inflammatory process, the mortality rate may be three times as high. Muysoms and associates (1998) reported a mortality rate of 37.5% in patients undergoing a completion pneumonectomy for the correction of early complications of a prior operation (especially for control of a bronchopleural fistula). Terzi and colleagues (1995) experienced even a higher mortality (57%) if the procedure was done for an early complication of a sleeve resection. In a series including 66 more chronic benign cases and recurrent neoplasms, Fujimoto and co-workers (2001) reported a 7.6% operative mortality for completion pneumonectomy, despite a high complication rate of 53%. The mortality rates for extrapleural pneumonectomy for malignant mesothelioma have declined from about 30% two decades ago to 5% and 6%, as reported by Sugarbaker (1996) and Pass (1997) and their associates, as well as by Rusch (1999). Brown and Pomerantz (1995) achieved an enviable rate of only 1.6% in 62 pleuropneumonectomies (including some completion pneumonectomies) for multiple drug-resistant tuberculosis (TB). Likewise, Blyth (2000) reported an operative mortality rate of 1.2% in 155 patients undergoing pneumonectomy for inflammatory lung disease. Shiraishi and associates (2000) had a mortality rate of only 8.5% in the difficult setting of extrapleural pneumonectomy for empyema. Similarly, although the risk of carinal pneumonectomy in the past has been very high, experience in several centers has markedly improved the results. Dartevelle and Macchiarini (1999), Mathisen and Grillo (1991), and Tsuchiya (1990) and Roviaro (1994) and their colleagues have recorded operative mortality rates after sleeve pneumonectomy of 7%, 15%, 8%, and 4%, respectively (see Chapters 29 and 30). In summary,
P.558
although complex pneumonectomy remains a high-risk operation overall, it is clear it can be performed safely in centers and by surgeons with experience in this area.
Significant morbidity is also higher after pneumonectomy than following lesser pulmonary resections. Overall complication rates range from 15% to as high as 75%. As alluded to earlier, some complications are minor. Major complications that occur in a significant number of cases include respiratory failure, pneumonia, bronchopleural fistula, empyema, difficult arrhythmias, myocardial infarction, and pulmonary emboli. Less common but often lethal complications include cardiac torsion or herniation and postpneumonectomy pulmonary edema. Most of these are discussed in subsequent sections.
Mortality rates associated with lobectomy are lower than those following pneumonectomy (Table 37-3). In the Lung Cancer Study Group experience reported by Ginsberg and collaborators (1983), operative mortality for lobectomy was 2.9%. More recently, Harpole and associates (1999) reported an operative mortality for lobectomy of 4% versus 11.5% for pneumonectomy. Wada and colleagues (1998) noted an operative mortality of only 1.2% in 5,609 lobectomies performed for lung cancer. Our group, as reported by Pagni and associates (1997, 1998), noted a mortality of 2.4% for 293 lobectomies in patients aged 70 and older, as contrasted with 12.5% for 24 pneumonectomies during the same period, and a 4.2% mortality rate in octogenarians undergoing standard or extended lobectomy for lung cancer. In a series of 500 pulmonary resections for lung cancer in patients over 70 years old, Thomas and colleagues (1998) reported mortality rates of 8%, 11.8%, 7.6%, and 0% for pneumonectomy, bilobectomy, lobectomy, and lesser resections, respectively. Recent series of bronchoplastic resections, including those of Tronc (2000), Rendina (2000), Lausberg (2000), and Okada (2000) and their associates, have documented a very low mortality (0% to 3%) in these technically demanding procedures, often associated with vascular as well as airway reconstruction (see Chapter 28).
The reported morbidity rate following lobectomy varies with definitions, but may be as high as that seen with pneumonectomy. Most significant problems are pulmonary, including atelectasis and pneumonia; cardiac; or are related to a residual space. Bronchial stump fistulae are less common and less ominous than those that occur after pneumonectomy. The problem of prolonged air leak from sutured or stapled lung parenchyma, however, is unique to resections less than pneumonectomy. Although most leaks resolve and do not cause significant clinical problems, they are often a source of prolonged hospitalization, increased use of inpatient and outpatient resources, and patient inconvenience. These complications are discussed in subsequent sections.
Table 37-3. Mortality Rates After Lobectomy | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
After a segmentectomy, the mortality rate is generally less than 1% when the procedure is done electively in patients with satisfactory pulmonary function. Jensik (1986) and Martini and associates (1986), however, reported that it may be as high as 4% to 6% in patients with poor pulmonary function, when more extensive tumor is present, or in those patients with a previous pulmonary resection. The nonfatal complications are similar to those occurring after a lobectomy.
The morbidity and mortality rates after a wedge resection are generally low. As with segmentectomy, however, when wedge excision is performed as a compromise for anatomic resection in patients with impaired cardiopulmonary status, complications and operative mortality increase. Complications in this setting are most commonly due to retention of secretions, ventilatory insufficiency, prolonged air leaks, cardiac failure, and arrhythmias. Persistent air spaces occur, but with an incidence of less than 10%. Wada and colleagues (1998) reported a 30-day mortality rate of 0.8% for lesser resection in 904 patients with lung cancer.
The specific complications occurring after lung volume reduction procedures, bronchoplastic and tracheoplastic operations, and video-assisted thoracoscopic pulmonary resections are discussed in their respective chapters.
EARLY COMPLICATIONS AFTER PULMONARY RESECTION
Hemorrhagic Complications
Postoperative Hemorrhage
Major hemorrhage after lung resection is most commonly the result of bleeding from a bronchial artery or an intercostal or other systemic vessel in the chest wall. Less frequently, slippage of a ligature or failure of a staple line on a major pulmonary vessel or an unrecognized injury to a systemic vein (vena cava, azygous) is the cause. If the pulmonary ligament has been dissected, local vessels may be the culprit sites. If adhesions were taken down, especially dense apical adhesions, vessels in these areas may result in significant bleeding. Bleeding related to a coagulopathy, as in all types of operations, is usually associated with prolonged complex cases and multiple transfusions.
When chest tubes are in place, an output of blood of more than 200 mL per hour for 4 to 6 hours suggests significant
P.559
bleeding, but lesser output may occur because of clot formation within the pleural space or in the drainage system. Complete reliance on the amount of drainage to determine blood loss can be misleading. It is critical to ensure patency of the drains at all times. When bleeding is suspected, serial radiographs are indicated to determine if there is undrained blood in the hemithorax. In addition, the dressings should be removed to assess bleeding around the chest tube entry sites. Any one of the following is an indication for reexploration in most cases: (a) failure to respond to presumed adequate blood replacement, (b) a large amount of blood in the hemithorax, or (c) continued excessive bleeding from the chest tubes. Determining the hematocrit of the chest tube drainage may be helpful in deciding whether to return to the operating room, especially if done serially, since visual assessment is not accurate in the early postoperative period.
In a series of 1,428 resections, Peterffy and Henze (1983) reported 113 hemorrhagic episodes (30% occurred after a pneumonectomy, 66% after a lobectomy, and 4% after a segmentectomy). Emergency thoracotomy was required in 37 patients (an incidence of 2.6%). Six of the patients died (4 as the result of hemorrhage and 2 because of a subsequent bronchopleural fistula). In another 3 patients, massive bleeding (2 from the pulmonary artery and 1 from a systemic vessel) was found to be the cause of death at autopsy. Thus, the overall incidence of mortality related to bleeding was less than 0.1%. Most reports find a reoperation rate for control of hemorrhage of about 3%. At operation, unless the major source of bleeding is immediately identified, a systematic examination of all the previously noted areas is carried out. Even after a major source is controlled, a similar assessment of all other areas is warranted. If no definite site is found, packing dissected areas with oxidized cellulose or other hemostatic agent or applying fibrin glue or other sealant should be considered before closure.
Sudden Massive Hemorrhage
On rare occasions, the ligature on the stump of the pulmonary artery will slip off, as noted in the aforementioned report of Peterffy and Henze (1983). Less commonly, a ligature slips from a pulmonary vein closure, especially when the pericardial reflection is included in the ligature. Massive blood loss occurs rapidly into the ipsilateral hemithorax. If the patient is still unconscious and there is no chest drain, sudden hypotension will be the only indication of its occurrence. If the patient is awake, sudden syncope with accompanying loss of pulse and blood pressure occurs. Massive fluid infusion and ventilation with 100% O2 may restore some degree of cardiac output and oxygenation. Further bleeding from the vessel may temporarily cease due to a low or near-absent cardiac output as well as the result of the tamponading effect of the large amount of blood in the hemithorax. If time permits, an electrocardiogram (ECG) should rule out a myocardial infarction.
The patient should be returned to the operating room as expeditiously as possible and the incision reopened, the clotted blood removed (bleeding from the vessel may recur at this time), and the vessel identified and controlled. Secure closure of the vessel is best obtained by suture of the stump or by the use of a vascular stapler. A successful outcome may be anticipated if the bleeding has been recognized promptly, the fluid replacement is adequate, and control of the vessel is obtained without further major loss of blood. Use of a suture ligature placed sufficiently distal to the simple ligature or of a vascular stapler for primary closure should minimize this tragic complication.
The possibility of significant or sudden massive bleeding is one of the arguments favoring chest tube balanced drainage of pneumonectomy cases. If hypotension occurs, the presence of this system helps rule in or rule out hemorrhage as a cause. In addition, mediastinal shift is prevented by this approach, and thus serial radiographs, intrapleural pressure measurements, and other delays can usually be eliminated in assessing the etiology of hemodynamic instability or collapse. Cardiac herniation or torsion is an exception, since tube drainage neither prevents nor helps diagnose this rare catastrophe.
Bronchovascular Fistula
The occurrence of a bronchovascular fistula with fatal hemorrhage is a rare event after a standard pulmonary resection, but it may develop in approximately 3% of patients who have undergone a bronchoplastic procedure, according to the review of Tedder and associates (1992). In most instances, the fistula is the result of a small, clinically asymptomatic abscess from a minor leak of the bronchial suture line that erodes into an adjacent ligated pulmonary artery or one of its branches or through the suture line of an adjacent angioplastic repair. It is best avoided by interposition of a viable tissue flap between the bronchial and vascular suture lines at the time of operation.
Cardiac Complications
Perioperative cardiac events are discussed in detail in Chapter 38, but will be reviewed briefly here for the sake of continuity in the discussion of the complications of lung resection.
Cardiac Herniation
When pulmonary resection involves opening the pericardium, cardiac herniation can occur. This rare complication follows pneumonectomy, but Ohri and colleagues (1992) reported a case after extended lobectomy. The incidence is equal on the right and left sides. Opening of the pericardial sac on the left down to the diaphragm will prevent left-sided herniation, but opening the pericardium completely on the right will not do so. Although globally classified as herniation, the mechanism of hemodynamic failure differs between the two sides. When a defect exists on the left, the left ventricular
P.560
apex can herniate through the foramen and become strangulated, as in other types of hernias. The problem involves both mechanical filling and emptying of the chamber as well as impairment of coronary blood flow. On the right side, in contrast, the problem is mainly torsion. The heart can rotate through the pericardial defect, with the left ventricle apex shifting anteriorly and to the right. The result is that both the inferior and superior venae cavae are occluded, and cardiac inflow ceases. In either case, the result is rapid catastrophic hemodynamic failure.
Cardiac herniation usually occurs in the early postoperative period and is often brought about by a change in the position of the patient, but has been reported as late as 72 hours following resection. Increased venous pressure is observed, associated with hypotension, tachycardia, displaced cardiac impulse, and cardiovascular collapse. The displacement of the heart through a right-sided defect is readily identified on a radiograph of the chest. Herniation and strangulation on the left side is not usually identified on an anteroposterior or posteroanterior film, but can sometimes be appreciated on a lateral radiograph. The ECG may show ischemia and thereby be misleading by suggesting a primary myocardial etiology.
If the operation was a right pneumonectomy, the patient should immediately be positioned left side down. In all cases, prompt surgical repair, involving reduction of the cardiac displacement and repair (usually with a patch of synthetic material) of the pericardial defect, is essential. A high index of suspicion is required for patient salvage, since there is little time for multiple diagnostic tests. The mortality rate is about 50%. Although most cases have been reported in situations in which the pericardial defect was not closed, this diagnosis cannot be eliminated in those with pericardial patches, since torsion can occur with apparent adequate closure by experienced surgeons, as stressed by Veronesi and associates (2001). Methods to prevent this problem are discussed in Chapter 29.
Cardiac Tamponade
When the pericardium has been opened and subsequently closed to prevent the occurrence of cardiac herniation, there is the rare possibility, as noted by Harvey and associates w(1995), that undetected bleeding may occur from the pericardial incision into the pericardial space. The amount of blood that may accumulate may be sufficient to result in a degree of tamponade. Hypotension, increased central venous pressure, a paradoxical pulse, and slowly developing cardiac failure may be seen. Diagnosis is established by determination of right-sided and wedge pressures, radiography, and ultrasonography. The treatment is prompt, adequate drainage of the accumulated blood by a transthoracic or subxiphoid incision or a percutaneous catheter approach.
Hypotension in the Absence of Bleeding
Hypotension associated with an elevated central venous pressure may occur with cardiac tamponade, cardiac herniation, myocardial infarction, and cardiac failure. Although heart failure can occur after any operation, right-sided heart failure is more common after pneumonectomy, since pulmonary artery pressure generally rises acutely to some degree. More surprising than the occasional occurrence of this problem is its rarity and rapid resolution, despite the sudden occlusion of about half of the pulmonary vascular bed inherent in pneumonectomy.
Heart failure due to underlying cardiac disease is suggested by the patient's preoperative cardiac status and is managed medically with inotropic agents, afterload reduction, diuretics, and other modalities as necessary. An additional factor in lung surgery is the dictum that we keep the patients dry, that is, minimize fluid infusion. Although there are little data to support this approach with respect to avoiding such complications as postpneumonectomy pulmonary edema, for example, a syndrome in which logic would dictate fluid restriction, it is generally accepted and appears innocuous in most cases. Third space loss in pulmonary resection is not generally the major issue it is in abdominal surgery, for example. Most patients are able to take oral fluids on the day of surgery. The result is that most thoracic surgeons accept a degree of hypotension or hypovolemia, as long as the patient's mental status, urine output, and peripheral perfusion appear acceptable. The threshold to pursue cardiac evaluation should be low, however, when the degree of hypotension is more than can be explained by mild hypovolemia and is not readily reversed by fluid infusion.
Cardiac Dysrhythmias
Cardiac dysrhythmias following thoracic surgery occur in about 18% of cases, as reported by Amar and associates (1995). Mitsudomi and colleagues (1996) reported the incidence of cardiac rhythm problems to be as high as 34% and to constitute the most common complication after pneumonectomy for lung cancer. The dysrhythmias occur most often in patients aged 60 years or older. Generally, the incidence in the older age group is between 20% and 30% after pneumonectomy, between 15% and 20% after lobectomy, and less frequently after lesser resections. Most dysrhythmias are atrial, the most common being atrial fibrillation. Sinus tachycardia, atrial flutter, paroxysmal atrial tachycardia, and frequent premature atrial contractions can also occur. Premature ventricular contractions, nodal rhythm, and bradyarrhythmias are less often encountered. Because of their common occurrence, and the prolongation of hospitalization, utilization of resources, and postdischarge follow-up that they engender, arrhythmias have received much attention. The focus has been on predicting the event, prophylaxis to prevent or lessen problems, and treatment once the complication has occurred.
With respect to the mortality associated with cardiac rhythm problems, the reported experience varies widely. Krowka and associates (1987) cited a 25% incidence of mortality associated with these complications. In contrast, neither Asamura (1993) nor Mitsudomi (1996) and their associates
P.561
noted any association of early mortality with atrial dysrhythmias. Cardinale and co-workers (1999) likewise not only confirmed a lack of association between atrial fibrillation and early mortality, but also found no difference in the length of postoperative hospitalization in patients with and without this problem. This latter finding appears incongruent with most experience and may be related to a long length of stay in both groups (13 and 14 days). With current methods of rapid detection and treatment, death due directly to a primary atrial arrhythmia (i.e., one not associated with ischemia, hypoxia, or other complications) should be very uncommon.
Abnormal rhythms usually arise during the first postoperative week. Ritchie and associates (1990, 1992) showed that with continuous monitoring initiated at the induction of anesthesia, over one half of the arrhythmias are recognized within the first 24 hours. In their experience, this was more often the case after pneumonectomy than after lobectomy. In the majority of reports, however, the complication is recognized on the second or third day postoperatively. The duration is variable, and often the heart reverts spontaneously to a normal rhythm. This occurs most often in patients who develop atrial fibrillation, but many patients require a period of medical therapy.
The cause of the abnormal rhythms is unknown, although mediastinal shift, hypoxia, abnormal serum pH, electrolyte derangements, and atrial distension, as well as other factors, have been implicated but unproved. The role of vagal nerve irritation in increased right ventricular preload and afterload, as suggested by Nakamura and colleagues (1997), is yet to be determined. What is known is that the occurrence of an arrhythmia is more common with advanced age, coronary artery disease, and a more extensive operative procedure, the incidence being highest after intrapericardial ligation of the pulmonary vessels. Krowka and colleagues (1987) also noted that arrhythmias occurred frequently in the postpneumonectomy patient who develops interstitial pulmonary edema or perihilar edema. Previous cardiac arrhythmia, frequent premature atrial or ventricular contractions preoperatively, and a complete or incomplete right bundle branch block on preoperative electrocardiogram also have been associated with an increased incidence of this complication. Von Knorring and associates (1992) reported that intraoperative hypotension was also a predictor of postoperative cardiac arrhythmias. Asamura and colleagues (1993), in a retrospective study of 267 resections, found an incidence of 23.6% for cardiac dysrhythmias and noted that extensive operation and older age were the only reliable predictors among the 16 variables analyzed. Similarly, Curtis and colleagues (1998) found that among 30 variables only age and pneumonectomy predicted atrial fibrillation.
Because of the high incidence of postoperative arrhythmias, many clinicians have used prophylactic digitalization in the older patient undergoing pneumonectomy or, less commonly, lobectomy. Early trials with digoxin prophylaxis, such as those of Wheat and Burford (1961) and of Shields and Ujiki (1968), suggested efficacy, but were not randomized. Two randomized series by Ritchie and associates (1990, 1992) showed no benefit of digoxin over controls. In a later nonrandomized study, Patel and colleagues (1992) also found prophylactic digitalization to be of no benefit in the reduction of postpneumonectomy arrhythmias. Many surgeons, therefore, no longer routinely use digoxin. Agents that appear to be more effective include flecainide, amiodarone, verapamil, diltiazem, and -blockers.
Borgeat and associates (1991) used a continuous infusion of flecainide starting postoperatively and continuing for 72 hours. A significant reduction in the incidence of arrhythmias was observed in the flecainide-treated group (7%) as compared with untreated patients or those receiving digoxin (47%). The disadvantages of this regimen include the use of a continuous infusion, the need to measure serum drug levels, and the potential ventricular proarrhythmic effect of flecainide. In addition, intravenous flecainide is not available in the United States, although an oral preparation is approved.
Van Mieghem and co-workers (1994) used amiodarone to prevent sinoventricular tachyarrhythmia (SVT), but stopped their trial due to the pulmonary toxicity of this drug. Recent interest in amiodarone prophylaxis in cardiac surgery, such as the favorable report by White and colleagues (2002), as well as a meta-analysis by Crystal and associates (2002), is likely to generate a reevaluation of this agent for pulmonary resection patients. Although Ciriaco and co-workers (2000) found that amiodarone was safe and effective for treating atrial tachyarrhythmias that developed after lung resection, there is currently only one study on its prophylactic use after lung resection. In a nonrandomized retrospective study of the use of prophylactic low-dose amiodarone (200 mg by mouth every 8 hours after recovery from anesthesia, continued to the time of discharge), Lanza and associates (2003) at the Mayo Clinic in Scottsdale, Arizona, found that in 83 patients 60 years of age or older undergoing pulmonary resection of various types, 3 (9.7%) of 31 patients receiving prophylactic low-dose amiodarone and 17 (33%) of 52 patients in the nonprophylactic group developed atrial fibrillation (P = 0.0253). The duration of the event was shorter in the prophylactic group, and no pulmonary toxicity due to amiodarone was noted. Obviously, a prospective randomized study is indicated. Although most instances of pulmonary toxicity have been associated with high-dose, prolonged treatment, short-duration therapy can also result in lung injury, as noted by Kaushik and associates (2001). It is possible that lung resection patients respond differently than cardiac patients, but this remains to be elucidated.
Although -blockers have traditionally been avoided in pulmonary resection patients because of the potential induction of bronchospasm, experience with prophylactic therapy in noncardiac surgery, as summarized by Auerbach and Goldman (2002) and by Fleischer and Eagle (2001), has been favorable. Jakobsen and colleagues (1997) published favorable results regarding the perioperative use of metoprolol to reduce the incidence of atrial fibrillation after
P.562
lung resection. At the present time, many institutions are using prophylactic -blockers in the perioperative management of the thoracic surgical patient. However, Bayliff and associates (1998), in a double-blinded study, found that propranolol when used as a prophylactic agent did not significantly reduce postoperative arrhythmias but did result in a high incidence of hypotension (49%) and bradycardia (25%). The use of -blockers in pulmonary resection cases, aside from severely bronchospastic patients, deserves future study.
Prophylactic calcium channel blockers appear to decrease the incidence of SVT. Van Mieghem and associates (1996) noted a 50% decrease in atrial fibrillation when a constant infusion of verapamil was begun postoperatively and continued for 72 hours. There was, however, a significant incidence of bradycardia and hypotension. Diltiazem, in contrast, appears to be an effective agent without the side effects of verapamil. In a prospective, randomized study of 70 patients undergoing standard or extrapleural pneumonectomy, Amar and colleagues (1997) found an incidence of supraventricular arrhythmia in the control placebo group, in the group of patients who received digoxin, and in the diltiazem group of 28%, 31%, and 14%, respectively. The regimen consisted of an initial loading dose of 20 mg IV immediately postoperatively, followed by 10 mg IV every 4 hours for 24 to 36 hours. On day 2, 180 to 240 mg was given as a single daily oral dose and continued for 30 days. In the diltiazem group, all the dysrhythmias were in patients who had undergone an extrapleural pneumonectomy; none were observed in patients who had undergone a standard pneumonectomy. Of interest was the observation that the incidence of dysrhythmias following extrapleural pneumonectomy was essentially the same in the control, the digoxin, and the diltiazem groups (30% to 38%). In a subsequent randomized, double-blinded study, Amar and colleagues (2000) compared placebo and diltiazem in 330 patients having lobectomy or pneumonectomy. The dosing was simplified in that intravenous diltiazem was given for only 18 to 24 hours, followed by oral agent for 14 days. The incidence of atrial fibrillation in the treated group was about half that in the placebo patients (10% vs. 19%). Lastly, the use of magnesium sulfate to prevent postoperative atrial tachyarrhythmias was reported by Terzi and coinvestigators (1996). Excellent results were obtained, but the possibility of further harm to the kidney in the presence of renal failure must always be considered in selecting this agent. Nonetheless, De Decker and colleagues (2003) believe that its use in the noncardiac surgical patient should be further investigated.
The treatment of postoperative rhythm complications is addressed in Chapter 38. In summary, many effective algorithms exist that include pharmacologic management and cardioversion when needed. For all but the most transient arrhythmias, it is prudent to involve a cardiologist in the in-hospital and subsequent outpatient care of the patient.
Persistence or frequent recurrence of atrial fibrillation in the postoperative patient always raises the issue of anticoagulation to prevent thromboembolism. Unfortunately, there are no reliable guidelines to decide this risk benefit question; that is, whether the risk of embolism is higher than the risk of bleeding in the postsurgical patient, and when in the postoperative period the ratio changes. If the operation has been complicated by bleeding, anticoagulation is generally not used early. In many cases, a low-dose approach is used initially, either with heparin followed by coumadin, or with coumadin alone. Aspirin may be adequate and less prone to cause hemorrhagic problems. The ideal approach in the specific setting of noncardiac thoracic surgery must await clinical trials.
When an immediate inciting factor is eliminated, ventricular dysrhythmias, especially when not present preoperatively, may reflect myocardial ischemia or damage. Bradyarrhythmia is managed acutely by the use of atropine or intravenous isoproterenol. Cardiac pacing may be required when a third-degree atrioventricular block or a sick sinus syndrome is present. Appropriate testing and treatment should be instituted quickly. Persistent problems require cardiology consultation and possibly electrophysiologic testing.
Myocardial Ischemia and Myocardial Infarction
Myocardial ischemia is uncommon, but von Knorring and associates (1992) reported this finding in 3.8% of 598 patients undergoing resection for lung cancer. Patients with coronary artery disease and previous myocardial infarction are more prone to develop this complication. Silent ischemia may be identified by postoperative monitoring and usually is seen on the second to fourth postoperative day. Khan (1993) suggested that such patients receive enteric-coated aspirin, 160 to 325 mg daily, as well as an appropriate -blocker to protect the patient from infarction and death, although this therapy has not been proven in clinical trials.
Myocardial infarction was recorded in 1.2% of patients reported by the aforementioned authors. Of more significance is that the event was fatal in 50% to 75% of the patients. It is probable that this high mortality rate has been lessened by advancements in rapid diagnosis, pharmacologic management, coronary angioplasty, and stenting, mechanical support, and surgical bypass, but data specifically relevant to the pulmonary resection patient are not available. The appropriate cardiac evaluation for a prospective thoracic surgical patient is discussed in Chapter 20.
Right-to-Left Shunt
Rarely, a patient will develop platypnea and orthodeoxia after a pneumonectomy, very rarely after a lobectomy (usually a right upper lobectomy or a right upper and middle bilobectomy). The patient may or may not be dyspneic in the supine position but becomes so, or the degree of dyspnea worsens, upon assuming an upright or sitting position. Oxygen saturation is found to be less than normal in the
P.563
supine position but is rapidly corrected by oxygen administration. The desaturation is exaggerated when the patient sits up or stands. When the problem occurs early and acutely, it is most often due to increased pulmonary vascular resistance, leading to elevated right ventricular and atrial pressure, often with tricuspid insufficiency. Because of the elevated right atrial pressure, a shunt may occur across a patent foramen ovale.
Although pulmonary artery pressure and vascular resistance may be normal at rest following pulmonary resection, studies by Reed (1996) and Okada (1994) and their colleagues have shown elevations in these parameters with exercise and have delineated their effects on right ventricular function. A shunt can also occur in the presence of normal right atrial pressure or equal atrial pressures, as shown by Smeenk and Postmus (1993). In this setting, the presentation is usually delayed and less acute. It is postulated that the shunt occurs as a result of a change in the position of the heart after a right pneumonectomy that causes direct streaming of blood from the inferior vena cava to the foramen ovale, despite the absence of a pressure gradient. Mercho and colleagues (1994) demonstrated this phenomenon in two patients after a right pneumonectomy with patent foramen ovale and normal atrial pressures by dynamic magnetic resonance imaging. At least 24 cases have been described in the literature since the original report of Schnable (1956). Four patients were recorded by Bakris and associates (1997), and Zueger and colleagues (1997) reported one patient with a true septum secundum defect.
The diagnosis is confirmed by echocardiography with a bubble study, dynamic magnetic resonance (MR) imaging, shunt measurements by catheterization, or cardiac angiography. Closure of the defect is curative. This most often has been by direct repair, but Godart and co-workers (1997) successfully used a modified button device described by Rao and colleagues (1994) to close secundum defects by a percutaneous route.
Pulmonary Complications
Postpneumonectomy Pulmonary Edema
Postpneumonectomy pulmonary edema (PPE) is an exceedingly frustrating complication for general thoracic surgeons, mainly because it defies all of our clinical skills, since it is nearly impossible to predict, to prevent, or to treat successfully. Deslauriers and associates (1998, 1999) presented two superb discussions of PPE. This complication occurs in 2% to 5% of cases of pneumonectomy. PPE is lethal when unrecognized and carries a mortality rate of 60% to 90% even with early diagnosis. Although PPE is clinically and histologically essentially the same syndrome as noncardiogenic pulmonary edema [adult respiratory distress syndrome (ARDS)], its devastating consequences in the pneumonectomy patient, its refractoriness to standard therapies, and the possibility that some of the etiologic factors for PPE are unique make it reasonable to view PPE as a specific syndrome.
Peters (1987) reported that it usually follows a right pneumonectomy in a patient whose preoperative pulmonary function was good and whose first 12 to 24 hours postoperatively were uneventful. The patient develops rapidly progressive dyspnea, hypoxemia, and radiographic signs of pulmonary edema in the remaining lung. Peters postulated from clinical observations and studies in the laboratory by Zeldin and associates (1984) that perioperative excessive fluid administration is the etiologic factor. According to this explanation, the remaining lung must remove a large fluid load, and the fluid filtered in the lung exceeds the capacity of its lymphatics. Fluid accumulates in the peribronchial spaces initially, which makes the lung less compliant, thereby increasing the work of breathing. When the peribronchial space is filled, the alveoli fill rapidly with fluid, hypoxemia worsens, and death ensues.
PPE is a diagnosis of exclusion. It is imperative to be sure that the cause of respiratory failure is not cardiogenic, aspiration or infectious pneumonitis, pulmonary embolism, sepsis, or bronchopleural fistula. Most patients should rapidly undergo invasive right-heart monitoring, pancultures, computed tomography (CT) or other pulmonary embolus study, and bronchoscopy to exclude these diagnoses.
Verheijen-Breemhaar and associates (1988) reported 11 cases of severe PPE in 243 patients (4.5% incidence). The majority occurred after right pneumonectomy [8 (7%) in 113 patients and only 3 (2%) after a left pneumonectomy]. Overhydration again was thought to be the common denominator, and of note was that PPE was found in 3 of 7 patients who required reoperation and multiple transfusions for postoperative hemorrhage. Patel and associates (1992) recorded 30 PPE cases of varying magnitude among 197 patients. Thirteen of these 30 patients died, a mortality rate of 43%. Postpneumonectomy pulmonary edema also occurs as one of the major fatal complications after carinal pneumonectomy. In this setting, Mathisen and Grillo (1991) suggest that the extensive interruption of major lymphatic channels to the remaining lung may play a role.
Turnage and Lunn (1993) showed that the histologic changes seen in PPE are those of ARDS, that is, diffuse alveolar damage. Shapira and Shahian (1993) suggest that the chain of events leading to postpneumonectomy pulmonary edema results from an increased filtration gradient across the pulmonary microcirculation acting in concert with hyperpermeability. Abnormal capillary permeability in the patient with pulmonary edema was noted by Mathru and associates (1990). Waller and colleagues (1996) suggested that increased pulmonary endothelial permeability may be the result of increased microvascular flow rate, since the linear velocity of the blood in the microcirculation is increased when a reduced vascular bed is subjected to a constant cardiac output. The increase in flow may result in injury to the endothelium. In addition, Rocker and co-workers (1988) noted a possible role of neutrophil-related enzymes in producing endothelial injury, with resultant increase
P.564
in endothelial permeability. Furthermore, van der Werf and associates (1997) noted that multiple transfusions of fresh frozen plasma were associated with postpneumonectomy pulmonary edema, possibly due to an immunologic reaction to these blood products.
Deslauriers and co-workers (1998, 1999) found an incidence of PPE of 4.5% and mortality rate of 80% in 291 pneumonectomies. Like Waller and colleagues (1993) and Turnage and Lunn (1993), they did not find a correlation between PPE and fluid balance. It could occur despite meticulous attention to minimization of perioperative fluid infusion. They found that PPE was associated with increasing extent and duration of operation and with the use of an underwater seal drainage system versus a balanced system. These authors' extensive analysis also suggested that other, purely mechanical, factors (hyperinflation and air-block syndrome) may play a role in PPE (Fig. 37-1). They base this idea on their finding that PPE was more common in their patients whose pneumonectomy spaces were drained with an underwater seal device than in those with a balanced system or no drain. This allows some degree of mediastinal shift and hyperinflation of the remaining lung, leading to volotrauma and fluid accumulation. Hyperinflation can also result in interstitial air leakage into the perivascular sheaths, causing extrinsic compression of the pulmonary microcirculation, similar to the air-block syndrome seen following repair of congenital diaphragmatic hernias. This theory fits well with the timing of PPE on the third or fourth postoperative day, its refractoriness to standard treatment methods, and its more common occurrence after right pneumonectomy (since mediastinal anatomy favors left lung hyperinflation more than right). The increased frequency after right pneumonectomy has also been attributed to greater interference with left lung lymphatic drainage at the bifurcation and subcarinal area as compared with standard left pneumonectomy, in which the proximal extent of bronchial dissection is usually more distal and therefore less likely to damage right-sided lymphatic channels.
Nonetheless, whatever the cause of PPE, current information dictates that fluid infusion should be minimized in the operative and early postoperative period, diuretics should be used early, and pressors should not be avoided if volume replacement appears adequate but blood pressure is low. It also has been suggested that prolonged high-pressure ventilation be minimized during the operation. When the process is unrecognized until it is in a full-blown state, the accompanying ventilatory dysfunction progresses relentlessly, despite aggressive therapeutic intervention to reverse the process, and often results in death. When the possibility of PPE is suspected, other causes of hypoxemia and radiographic infiltrates (cardiogenic pulmonary edema, bronchopleural fistula, aspiration, infection, pulmonary embolus, and other pathologic states) must be rapidly assessed and often empirically treated until reliably eliminated from the diagnostic possibilities. When early therapy is instituted, consisting of fluid restriction, optimal pain control, diuretics, and mechanical ventilation, the mortality rate remains high, but may be reduced. Because barotrauma and mediastinal shift may be etiologic factors, limiting airway pressure is prudent. This may be accomplished by lowering tidal volume, minimizing end-expiratory pressure, and accepting higher inspired oxygen levels. Mathisen and associates (1998) found that inhaled nitric oxide at a concentration of 10 to 20 parts per million, in addition to standard measures, improved oxygenation and decreased mortality.
The role of steroids in PPE and many other forms of postoperative and posttraumatic pulmonary and systemic impairment remains a complex and controversial subject, beyond the scope of this chapter. Many surgeons, the author included, believe that they do have a beneficial effect in many cases and that fears of adverse effects of early
P.565
and brief administration are unproved. For information about innovative, cutting-edge approaches to severe respiratory failure, refer to Chapter 40 for a detailed presentation of the current status of extracorporeal membrane oxygenation, intravascular oxygenation, extracorporeal CO2 removal, and partial liquid ventilation.
 |
Fig. 37-1. Pathophysiology of postpneumonectomy pulmonary edema. From Deslauriers J et al: Postpneumonectomy edema. Chest Surg Clin N Am 9:565, 1999. With permission. |
Other Types of Respiratory Insufficiency
Respiratory failure is discussed in detail in Chapters 40 and 72. The incidence of respiratory insufficiency requiring more than 48 hours of mechanical ventilation either immediately after pulmonary resection or after later reintubation is between 5% and 15%. The relevant issues are prediction, prevention, diagnosis, etiology, and treatment. With respect to risk, patients with poor lung function, especially those who retain CO2, are chronic sputum producers, continue to wheeze despite a good medical regimen, and continue to smoke, are at highest risk. Likewise, the extent of resection and predicted postoperative parameters need to be considered. Preventive measures include preoperative optimization of lung function and smoking cessation or reduction for as long as possible, avoidance of overhydration, adequate pain control, and optimal pulmonary therapy. Diagnosis is based on clinical, radiographic, and blood gas parameters (see Chapters 40 and 72).
Effective treatment requires determination of etiology. Among the many possibilities are nonprimary pulmonary processes such as heart failure, fluid overload, sepsis, inadequate pain control, and oversedation. Primary pulmonary causes include inadequate reserve following resection (a dreaded, usually predictable, and often long-term problem), excessive secretions, significant atelectasis, pneumonia, pneumonitis or infection from aspiration, pneumonitis from prior or current treatment (e.g., preoperative radiation, chemotherapy agents, reaction to perioperative drugs), suboptimal management of underlying bronchospasm/emphysema, bronchopleural fistula, and pulmonary embolus. Appropriate treatment depends on ruling in or out these uncommon etiologies, some of which may occur simultaneously. Rare complications that must occasionally be considered include tumor emboli or main pulmonary artery stenosis following pneumonectomy for central tumors, as described by Flores and associates (2001).
Noncardiogenic, noninfectious pulmonary edema (ARDS), such as that seen in PPE as discussed previously, can occur after lobectomy, lesser resections, and indeed any surgical procedure, trauma, or acute illness. It remains a diagnosis of exclusion, and the principles for its treatment are similar to those noted for PPE. Fortunately, the mortality rate is about half that of PPE. Although one may postulate that the lower mortality is due simply to the presence of more lung parenchyma in the nonpneumonectomy patient, it is also possible that the etiology, or at least some of the etiology, of PPE is unique. In a recent report examining the incidence of acute lung injury (ALI) and ARDS in 1,221 patients undergoing lung resection, including pneumonectomy, for cancer, Ruffini and associates (2001) found no reliable preoperative predictors. They confirmed that the highest incidence follows right pneumonectomy (4.5%) and, interestingly, noted that sublobar resection was associated with a higher risk (3.2%) than left pneumonectomy (3%), bilobectomy (2.4%), or lobectomy (2%). Mortality was 40% for ALI and 59% for ARDS. Although the definitions of ALI versus ARDS may be arbitrary in general, this large series reemphasizes the clear association of right pneumonectomy with this complication, its unpredictability otherwise, and its lethal nature despite aggressive treatment. In a similar large series, Kutlu and co-workers (2000) found an incidence of 3.9% for ALI/ARDS in 1,139 resections. An age of over 60, male gender, and a diagnosis of lung cancer correlated with this complication. Of note is that ALI/ARDS caused 72.5% of the total operative mortality in this series.
An important point is that respiratory failure may have more than one etiology at any given time and at different times in the postoperative course. Thus, what begins as ARDS is often later compounded or replaced by bacterial or other infectious pneumonia, aspiration, drug reaction, suboptimal nutrition, a cardiogenic source or a combination of problems. New infections may develop after treatment of a prior organism. The possible synchronous and metachronous permutations of multiple problems are myriad. Thus, careful attention to the synthesis of frequent radiographic, laboratory, clinical, and culture data is mandatory, and one must be ever mindful that today's primary problem in these critically ill patients may not be the same as tomorrow's pathophysiology.
Massive Atelectasis
Severe or massive atelectasis after lobectomy was reported to have an incidence of 7.8% and constituted about 25% of the complications after lobectomy in 218 patients reported by Korst and Humphrey (1997). Severe atelectasis was more common after a right upper or a right upper middle bilobectomy than after a right lower or either left lobectomies. The difference (15.5% vs. 6%) was statistically significant. These authors also noted that there were no obvious predisposing factors in those in whom the complication developed as compared with those in whom it did not occur. Although in some patients the large airways are clear at the time of bronchoscopy, in others there are copious, often thick secretions, some congealed enough to form plugs. In rare instances, there is a physical abnormality of a major bronchus, such as stenosis of the left bronchus due to vigorous retraction while stapling the left upper lobe bronchus. This problem is prevented during a right upper lobectomy by the presence of the middle lobe bronchus. Van Leuven and associates (1999) also reported two cases of atelectasis due to abnormal upward displacement causing twisting of lower lobe bronchi, one following right upper and middle bilobectomy and one after left upper
P.566
lobectomy. Both patients were treated successfully with stents.
Clinically, when massive atelectasis does develop, most patients become short of breath. Associated with the tachypnea, a rapid pulse and sharp temperature elevation may be observed. Some patients, however, appear surprisingly asymptomatic, even with significant volumes of unaerated lung. The physical findings and radiographic examination are usually diagnostic. Mediastinal shift, usually a sign of atelectasis, may be misleading in the postresection patient. If there is doubt on plain film whether the problem is atelectasis, pleural fluid, or both, a CT scan is determinative. Treatment is prompt and effective tracheobronchial toilet, including bronchoscopy if needed. If the problem is an iatrogenic anatomic abnormality of the bronchus, as just noted, reoperation, dilation, or stenting may be required.
Lobar Torsion and Gangrene
A 180-degree rotation of a lobe on its bronchovascular pedicle occasionally is observed intraoperatively. It also may occur spontaneously postoperatively. Rotation is seen most commonly with a freely mobile (complete major and minor fissures) right middle lobe, as recorded in a survey by Wong and Goldstraw (1992), but it may occur with either the remaining upper or lower lobe of the left lung as well. If unrecognized and not corrected, vascular occlusion with resultant infarction and gangrene of the involved lobe occurs.
Obviously, the remaining lung after a lobectomy should be inspected to ensure its proper position and lack of torsion before closure of the chest. Also, after a right upper lobectomy, the middle lobe should be stabilized by securing it to the lower lobe by ligature, suturing, or stapling. To assess the optimal position for this pexy, the lobes are temporarily reinflated and the best position is assessed, with careful attention to preventing kinking of the middle lobe vein, which is often small. This maneuver can be avoided after right upper lobectomy only if it is clear that the remaining fissure will prevent torsion. Such fixation or stabilization is rarely, if ever, warranted on the left side despite reports of a few isolated cases by M. V. Kelly (1977), Livaudais (1980), and Kucich (1989) and their associates.
When this rare event does occur, failure of complete expansion and opacification of the lobe (often in an unusual anatomic position) can be observed on the postoperative radiographs. Failure of expansion after tracheobronchial suction requires prompt bronchoscopy. Piccione and Faber (1991) report that bronchoscopy will reveal a compressed bronchus that has a fishmouth appearance. Although the bronchoscope may be passed through the obstruction, the involved bronchus will collapse as the scope is withdrawn. Although the features of torsion on radionuclide perfusion scan, pulmonary angiography, and CT have been well described by Spizarny and associates (1998), among others, these studies are generally not required for diagnosis.
When torsion of the lobe is suggested by the radiographic and bronchoscopic findings, immediate reoperation is indicated to release the torsion and to stabilize the involved lobe, if viable, in the correct anatomic position. If the lobe is not viable, a lobectomy of the involved middle lobe on the right or a completion pneumonectomy on the left side becomes necessary.
When the torsion remains unrecognized, infarction and gangrene of the involved lobe will occur, with the resultant local thoracic and systemic findings of infection. Gangrene of a lobe also may occur in the absence of torsion, as noted by Piccione and Faber (1991), the underlying cause being an unrecognized ligation or other compromise of either the venous outflow or, less commonly, the pulmonary arterial supply of the lobe. Sugimoto and colleagues (1998) point out that the middle lobe vein may originate from the inferior pulmonary vein and be inadvertently ligated during lower lobectomy. Hovaguimian and co-authors (1991) described a case and referred to one other report of right upper lobe venous thrombosis after right lower and middle bilobectomy. In both instances some degree of necrosis occurred based on imaging and the presence of hemoptysis, but over time collateral bronchial and pulmonary channels enlarged sufficiently to permit salvage of the lobe, although observed function remained less than predicted. In most cases of torsion or other cause of necrosis, however, reoperation and lobar resection is required. The author's only personal case was a left lower lobe torsion after upper lobectomy and take-down of the pulmonary ligament. The diagnosis was made by radiograph and bronchoscopy immediately postoperatively. The lobe was detorsed and secured to the pleura. Although the patient required several days of ventilatory support and had infiltrates confined to the involved lobe, he survived and had no residual radiographic abnormalities and a normal-size lobe.
The rarity of lobar gangrene is supported by the data reported by Keagy and associates (1985), in which only one instance of this complication was noted in 224 complications (0.4%) in 369 patients (0.27%) who had undergone a lobectomy. More recently, a Mayo Clinic review by Cable and co-workers (2001) reported that only 7 (0.089%) of 7,889 lobectomy or segmentectomy patients developed lobar torsion. This series is interesting in that the middle lobe alone was involved in only 2 of the 7 cases, the right middle and upper in 1, right lower in 2, and left upper in 2. Thus, the common assumption that the right middle lobe is most at risk for this rare complication may be incorrect.
Pulmonary Infarction After Angioplasty
After pulmonary artery angioplasty accompanying a lobectomy or a bronchoplastic procedure, thrombosis may occur secondary either to kinking of the vessel or the presence of a stenosis at the site of the repair. With rare exception, this leads to infarction of the supplied pulmonary parenchyma. A low-grade fever and opacification of the
P.567
lung are present in the absence of a bronchial obstruction. According to Warren (1995), initially the bronchial mucosa may appear normal on bronchoscopy but soon becomes cyanotic, edematous, and hemorrhagic. The diagnosis is confirmed by a pulmonary angiogram or a perfusion scan. Once the diagnosis is made, a completion pneumonectomy is usually indicated.
Postoperative Pneumonia
In some patients, infection may be superimposed on unresolved atelectatic areas or also may result from unrecognized episodes of aspiration. The true incidence of postoperative pneumonia is difficult to establish; in most reviews, this complication is considered together with atelectasis and major problems associated with retention of secretions. Keagy and associates (1985) noted this conglomerate group of complications in 7% of 369 patients who had undergone lobectomy, and Wahi and colleagues (1989) reported an incidence of 6.6% in 197 patients who had undergone a pneumonectomy. Although the overall incidence of pneumonia was not recorded, von Knorring and associates (1992) reported it was the cause of death in 1.3% of 598 patients undergoing resection for lung cancer. Tedder and associates (1992), in a review of bronchoplastic procedures, noted that postoperative pneumonia per se occurred in 6.6% of the reported patients and was responsible for 15.4% of the postoperative deaths observed. Hollaus and colleagues (1997) reported that aspiration pneumonia is common in patients with a bronchopleural fistula. In these patients, the aspiration often is associated with the development of ARDS. Approximately 40% of patients will die as the result of the development of this complication.
Although data are sparse, it is likely that postoperative pneumonia most often is seen in patients who require prolonged ventilatory support or who have continued inordinate difficulty in clearing their tracheobronchial secretions. Aerobic, anaerobic, and mixed infections occur, and proper collection (bronchoscopic aspiration, protected brush) and culture for identification of the offending organism(s) are mandatory (see Chapter 14). Although most postresection pneumonias are due to bacteria, the possibility of viral or fungal causes, legionella, and mycoplasma should always be kept in mind, especially in patients immunosuppressed by cancer and its treatment and those with complicated postoperative courses. Camazine and associates (1995) stress the need for a high index of suspicion of atypical infections in debilitated patients after finding that three of six patients with pneumonia and respiratory failure in a series of 54 consecutive thoracotomies for cancer had herpes simplex virus pneumonia. All three patients responded to acyclovir. In all cases, appropriate antibiotics, nutritional support, and good tracheobronchial toilet are essential for recovery. Pseudomonas, serratia, and, increasingly, resistant staphylococcal infections are the most difficult to treat successfully, as in other clinical settings.
Prolonged Air Leak
After pulmonary resections of lesser magnitude than a pneumonectomy, an air leak from a residual raw or stapled parenchymal surface is a common occurrence. With complete reexpansion of the lung and obliteration of the pleural space, the leak usually stops in 2 to 3 days. The persistence of a leak beyond 7 days is considered abnormal and is generally used to define a prolonged air leak. Various maneuvers (increasing or decreasing the suction applied to the water-seal system, conversion to water-seal drainage only, placement of additional chest tubes) may be tried empirically. In most instances, the air leak will stop even if the space persists.
Prolonged air leaks are a very frequent problem in volume reduction surgery for emphysema, occurring in 30% to 50% of cases. The various methods that have been suggested to reduce the incidence of persistent air leak from the stapled excision lines through the emphysematous parenchyma in this setting are discussed in Chapter 85. With respect to standard lung resection, Rice and Kirby (1992) reported peripheral air leaks lasting over 7 days in 35 (15.2%) of 197 patients. Only 3 leaks (1.5%), however, persisted beyond 2 weeks. Although there were no complications directly related to the leaks, the mean postoperative length of stay was 5.6 days longer in this group. Several studies conducted by and recently summarized by Cerfolio and associates (2002) have focused on this common problem that previously received little detailed analysis. Among commonly accepted risk factors for prolonged air leak are severe emphysema, upper lobectomy, lung volume reduction operations, steroid use, and active infection.
The reason for the previous sparsity of literature on air leaks is likely due to their generally benign course and the absence of a single correct way to reduce their incidence and to manage them. The ingenuity, training, experience, and habitual practice of the surgeon greatly affect the approach to the individual patient in whom infection of any accompanying air space is absent. If a lobectomy or segmentectomy has been performed and there is a prolonged, large air leak, it is generally prudent to assess the bronchial stump for the presence and size of a fistula early in the patient's course, since a significant bronchial fistula may require reoperation or endobronchial methods of control. Most often, the stump will be normal and the problem is a peripheral or alveolar air leak (AAL). If there is no sepsis, respiratory insufficiency, or significant residual space, in most instances it is best to be patient and allow the leak to seal itself. Usually this approach does not require prolonged hospitalization. As shown by McKenna (1996) and the author (1997) and their associates, most cases can be managed on an outpatient basis with one-way valves (Heimlich valve, Becton Dickinson Co., Franklin Lakes, NJ, U.S.A.; Pneumostat valve, Atrium Medical Corp., Nashua, NH, U.S.A.). Early conversion from suction to water seal in the presence of an AAL is tolerated well by most patients and, more importantly, has been shown by Cerfolio (2002a) to decrease the duration of air leak. An occasional patient will not be able to maintain sufficient lung expansion
P.568
to avoid respiratory distress. Others will develop significant subcutaneous emphysema. In these cases, suction is resumed and decisions about when to try water seal again are made on the basis of clinical, radiographic, and AAL monitoring.
When an AAL persists despite appropriate tube management, either inpatient or outpatient, a decision must be made regarding treatment. While there is no universally agreed-upon time limit, in most cases plans should be formulated at 2 to 3 weeks. Kirschner (1992) and later Cerfolio and associates (2002) confirmed that in many cases chest tubes can be removed safely after 2 to 3 weeks despite an ongoing air leak. Prior to removal, a period of provocative clamping is done to ensure that clinically significant lung collapse or subcutaneous emphysema does not occur. In many cases this can all be accomplished on an outpatient basis. The reason this approach may be successful is that sufficient adhesions have developed over time to prevent lung collapse.
When an AAL persists and tube removal is not possible, several methods of control have been described. The identification and occlusion by vascular embolization coils and fibrin glue of the subsegmental bronchi supplying the leaking site, as described by the author and associates (1993), may be successful, but is time-consuming and requires CT scan and fluoroscopic guidance, as well the involvement of a skilled thoracic radiologist. Fibrin glue, autologous blood, and other sealants have been applied to the parenchymal leak by thoracoscopy, percutaneously, or under image guidance, as described by Samuels (1996), Suter (1997), Thistlewaite (1999), O'Neill (2000), and Rivas de Andres (2000) and their colleagues. If there is a significant residual space, thoracoscopic take-down of adhesions in order to allow lung reexpansion without application of sealants has also been successful. Some recommend that the presence of a prolonged air leak in patients without evidence of a pneumothorax be managed by the instillation of talc or other sclerosing agent via the indwelling chest tube. Since complications of peripheral air leaks are uncommon, reoperation is very rarely required, unless pleural infection occurs.
Intraoperative methods to minimize AAL include meticulous control of fissures; use of staple-line buttressing material such as Gore-Tex (W.L. Gore & Associates, Flagstaff, AZ, U.S.A.) or bovine pericardium; application of fibrin glue, synthetic polymers, or other sealants; and coverage of dissected parenchyma with easily available tissue such as the pericardial fat pad, pleura, or intercostal or diaphragmatic flaps. This topic has recently been discussed by Toloza and Harpole (2002). Take-down of the pulmonary ligament after upper lobectomy is believed to help avoid significant residual spaces. If it still appears that a residual space may contribute to the persistence of AAL, the most common and simplest adjuvant technique is the construction of an apical pleural tent. The necessity at the time of primary resection for other measures, such as phrenic nerve injection or crush, diaphragmatic relocation, induced pneumoperitoneum, major muscle flaps, and thoracoplasty, should be uncommon, generally predictable, and planned in advance on the basis of the individual case.
Bronchopleural Fistula
The clinical effects of failure of healing of a bronchial stump after anatomic lung resection can vary from a minor problem, culminating in spontaneous or simple endoscopic closure, to a life-threatening septic and ventilatory catastrophe. The reported incidence of bronchopleural fistula (BPF) also varies greatly, but is in the range of 1% to 10% overall. Three important points are indisputable, however. First, BPF is more common after pneumonectomy than following lesser resections. Second, BPF is more common after right than left pneumonectomy. Third, BPF following pneumonectomy is clinically more devastating than after lobectomy or segmentectomy. Vester and associates (1991) reported an incidence of 3.9% after 503 pneumonectomies (3.7% after stapled closure of the bronchus and 12.5% after suture closure), 1.1% after 1,083 lobectomies, and 0.3% after 650 segmentectomies. Asamura and associates (1992) reported an overall incidence of 2.1% after 2,359 pulmonary resections for lung cancer and found a higher incidence for right-sided operations, especially pneumonectomy (Table 37-4). Al-Kattan and colleagues (1994) reported an incidence of only 1.3% in 530 consecutive pneumonectomies. The bronchial stump was closed manually with nonabsorbable monofilament 2 0 polypropylene sutures. Of interest is the report of Sarsam and Moussali (1989), who recorded no fistulae after the use of a bronchoplastic method of closure using a membranous flap from the posterior bronchial wall originally described by Jack (1965) in a series of 332 pneumonectomies, despite the use of the now-antiquated chromic catgut as the suture material. Wright and colleagues (1996) experienced a 3.1% BPF rate in 256 pneumonectomy cases in which the bronchus was closed by sutures. Deschamps and associates (2001) reported an overall incidence of postpneumonectomy BPF of 4.5% in 713 cases, 8% for right pneumonectomy and 1.1% for left. In their series, stapled closures were less likely to fail than sutured closures.
Much has been written and many dogmas are held about the optimal means of avoiding this problem. Clearly, prevention is the key. Less clear, however, is the optimal
P.569
means of prevention. The broad scope of the present chapter prevents a detailed analysis of decades-old and ongoing claims in this area. The reader is referred to the chapters in this text dealing with the technical aspects of bronchial closure and to the vast literature on this subject. Rather, this section focuses on risk factors, diagnosis, and treatment.
Table 37-4. Prevalence of Bronchopleural Fistula According to Side of Resection | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||
Table 37-5 lists commonly accepted risk factors for BPF. A bronchopleural fistula is more common after resections for inflammatory disease of the lung, especially in patients with active tuberculosis and positive sputum. Pomerantz and colleagues (1991) noted a 10.5% incidence after resection in 85 patients with resistant mycobacterial infections; almost all were after a right pneumonectomy in patients with multiple-drug-resistant Mycobacterium avium-intracellulare infections, despite a transposed muscle flap to cover the bronchial stump. In contrast, in a subsequent report Brown and Pomerantz (1995) reported only one fistula in 62 pneumonectomies (the vast majority were extrapleural pneumonectomies and a few were completion pneumonectomies) in patients with multidrug-resistant Mycobacterium tuberculosis infections. In patients who received a full course of preoperative mediastinal and hilar irradiation, Yashar and associates (1992) reported an incidence of 9.6%.
In a multivariate analysis of 1,360 recent lung cancer resections, Asamura and associates (1992) noted that the significant risk factors for a bronchopleural fistula were pneumonectomy, residual tumor at the bronchial stump, preoperative irradiation, and the presence of diabetes. The aforementioned large series by Deschamps and co-workers (2001) surprisingly found that bronchial stump coverage with other tissue was associated with a higher incidence of BPF than seen with nonreinforced stumps. One may postulate that only the highest-risk cases were treated with reinforcement, but this is not made clear in the paper. Other factors that have been mentioned include mediastinal lymphadenectomy, older age, steroid use, preoperative chemotherapy, and partial-dose radiation. With the exception of preoperative induction treatment followed by right pneumonectomy, as noted by Martin and colleagues (2001), these factors alone have not consistently been shown to be predictive of BPF.
Early (1 to 2 days, even up to 7 days) after a resection, a bronchopleural fistula may occur because of a technically poor closure of the bronchial stump. After a pneumonectomy, an early large bronchopleural fistula manifests by a massive air leak with the development of a progressive increase in clinically evident subcutaneous emphysema. A small amount of subcutaneous emphysema is normally seen, as some of the air in the postpneumonectomy space at the time of closure is expelled into the tissue of the chest wall with coughing or is forced out with a rapid accumulation of fluid within the space. Along with the development of subcutaneous emphysema, the patient may exhibit varying degrees of respiratory insufficiency because the fistula physiologically represents a modified open pneumothorax. Ventilatory support, often best accomplished by the use of selective bronchial intubation or jet ventilation, may be necessary at this stage in severe cases.
Table 37-5. Risk Factors for Bronchopleural Fistula | |
|---|---|
|
When the bronchial leak occurs later in the postoperative course, it may be caused by failure of healing because of inadequate viable tissue coverage of the stump or as the result of infection of the fluid within the space and rupture of the empyema through the bronchial stump. At this stage, the patient expectorates variable quantities of serosanguineous, frothy fluid. Danger of flooding of the remaining lung is present. Whenever there is clinically significant deterioration that may be due to a BPF, the patient should be placed with the operated side down and the head elevated. Prompt drainage of the affected pleural space with a chest tube or even by urgently opening a prior tube site or a portion of the incision is indicated to prevent further soiling of the remaining lung and relieve any intrapleural tension.
When a bronchopleural fistula occurs later than 2 weeks after pneumonectomy, it is most likely the result of rupture of an empyema through the bronchial stump, although at times failure of healing of the bronchial stump may be the underlying cause. Clinically, the patient is most likely febrile and has a cough productive of purulent sputum. Hemoptysis may occur.
Small fistulae present with more subtle findings. In some cases the fistula may be asymptomatic or minimally symptomatic. An occult bronchopleural fistula (without expectoration of pleural fluid) occasionally occurs (Fig. 37-2). A fall in the fluid level on a chest radiograph should arouse suspicion. Whether the fluid escapes through the bronchus and is swallowed, unnoticed, by the patient or is lost by absorption through the parietal pleura as the result of increased intrapleural pressure, which becomes potentially greater than atmospheric pressure, is unresolved. Nonetheless, confirmation of the diagnosis is most often by simple bronchoscopy. Other methods include instillation of methylene blue into the pneumonectomy space and watching for its appearance in the sputum or by bronchoscopy, and the use of radionuclide inhalation to determine if the material appears in the pneumonectomy space. In cases of tiny fistulae, one or more of these tests may be diagnostic. Failure to document a fistula by any of these studies, despite its obvious presence, defines the true occult fistula.
The management of an occult bronchopleural fistula poses a vexing clinical problem. When the patient remains asymptomatic and no signs of clinical infection are present, close observation alone is warranted, as suggested by O'Meara and Slade (1974). Antibiotics are not needed.
P.570
More often than not, there will be no further difficulty. Despite much worry on the part of the thoracic surgeon, most patients eventually return with radiographs showing a normal fluid-filled pneumonectomy space months or even years after presentation. If any finding of clinical infection occurs, however, prompt drainage of the pleural space is mandatory.
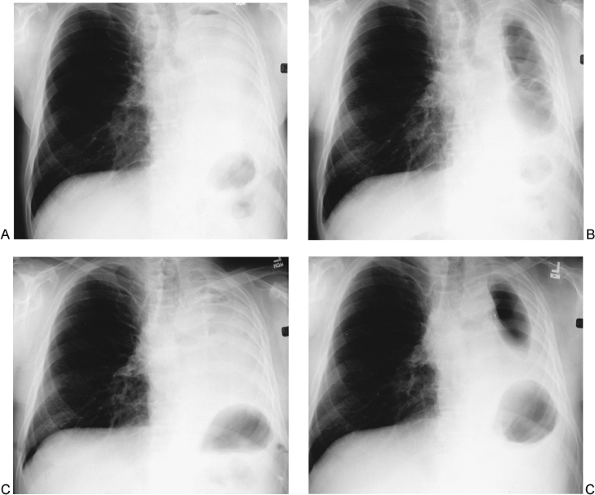 |
Fig. 37-2. Occult postpneumonectomy bronchopleural fistula. A. Chest radiograph 1 month after left pneumonectomy shows space almost completely filled with fluid. B. Film 2 months later at routine follow-up shows a large volume of air in the hemithorax. The patient was entirely well and had not noted cough, sputum, or symptoms of infection. Bronchoscopy at this time was negative. C. Fourteen months later the hemithorax is filled with fluid and a few air pockets (1.5 years postpneumonectomy and 6 months after the hemithorax was filled with antibiotic-saline solution at the time of thoracoscopy and repeat bronchoscopy, both of which failed to demonstrate a fistula or recurrent tumor). D. Six months afterward (2 years following pneumonectomy), a large volume of air is again seen in the pleural space. The patient remains asymptomatic and without evidence of recurrent cancer, 7.5 years after diagnosis of an occult bronchopleural fistula. |
The management of a clinically evident bronchopleural fistula depends on the time of its development postoperatively and its underlying cause. Early in the postoperative period, up to 7 or even 14 days according to Brutel de la Riviere and associates (1997), reoperation and repair of the bronchial stump may be indicated. With operative repair, coverage of the new bronchial suture line is mandatory. A transposed muscle flap, the pericardial fat pad, or an omental pedicle flap may be used (see Chapter 59). In some early cases associated with severe empyema it is prudent to create an open flap for drainage rather than using a simple chest tube. Nonoperative control has been achieved in a few instances.
P.571
Jessen and Sharma (1985) suggested using fibrin glue to occlude the opening when the fistula is small. Glover and associates (1987) also reported successful use of fibrin glue for the closure of small fistulae. Hollaus and co-workers (1998) reported that the endoscopic application of fibrin glue was most successful in the treatment of fistulae under 3 mm in size; endoscopic techniques alone were less satisfactory in patients with larger fistulae.
In most situations when a major bronchopleural fistula is present, more aggressive measures to achieve closure of the fistula and to control the associated empyema are necessary. Puskas and colleagues (1995) at the Massachusetts General Hospital recommend initial drainage and the subsequent direct closure of the bronchus by a manual suture technique and support of the suture line with an omental flap. Eventual obliteration of the pleural space may be necessary. At the Mayo Clinic, Pairolero and colleagues (1990), as well as Trastek (1997), advocate that after stabilization of the patient, open drainage be accomplished by establishing an Eloesser flap or modification thereof or reopening a portion of the original thoracotomy. After cleansing of the pleural space, the bronchial stump is reclosed and reinforced with vascularized tissue (a transposed muscle or omental flap). Subsequent sterilization of the pleural space is accomplished by the Clagett maneuver. Gharagozloo and associates (1998) reported success with 22 early postpneumonectomy fistulae by reoperation for d bridement and bronchial stump closure, continuous pleural irrigation with 0.1% povidone-iodine (40 mL/h for 7 days) followed by saline irrigation for 24 hours. If a Gram's stain of the pleural effluent was negative at that point, the hemithorax was filled with 2 liters of a solution containing gentamicin, neomycin, and polymyxin B. If the Gram's stain was positive, povidone-iodine irrigation was resumed and the cycle repeated. There were no recurrent fistulae or empyemas, and the mean hospitalization after repair was only 13 days. The use of muscle or omental flaps to close bronchopleural fistulae and to obliterate the pleural space, as described by Miller (1984, 1996) and by Deschamps and colleagues (1999), is usually a two-stage procedure, has a high success rate, and is discussed in detail in Chapter 59. The approach is similar to the treatment of any postsurgical empyema, with modifications based on the presence of a BPF, the size of the residual space, and the clinical status of the patient, including oncologic prognosis.
Transsternal transpericardial exposure and division of a long bronchial stump associated with a bronchopleural fistula has also been used. When the distal stump cannot be removed, a tissue flap, preferably muscle, should be transposed between the divided ends. Simple stapling of the stump proximal to the leak is ineffective, since refistulization inevitably occurs. Abruzzini (1961) was one of the first to report the importance of division of the stump to control a fistula. Maassen (1975), Bruni (1987), Perelman (1987), and Perelman and Ambatiello (1970) also recorded the use of this procedure in Europe. In the United States, Baldwin and Mark (1985) and Cosgrove (1985) and in Canada, Ginsberg and associates (1989), have reported its use. The technique and indications for transsternal closure of a bronchopleural fistula are presented in Chapter 34. Perelman and associates (1987) described a right thoracotomy approach to close left bronchial stump fistulae, with initial good results in 20 of 25 patients (Fig. 37-3). Four late
P.572
deaths occurred, two related to bronchial recanalization and two related to progressive empyema. Brutel de la Riviere and associates (1997), in addition to their experience with the transsternal transpericardial closure of a long stump, reported the use of a carinal resection to eradicate a fistula in patients with a short bronchial stump. Unfortunately, a high failure rate was incurred with this approach. Azorin and colleagues (1996) reported a transcervical mediastinal video-thoracoscopic approach to staple the left main-stem bronchial stump for control of a postpneumonectomy BPF. The pleural space was then cleaned and drained through a thoracic approach. Although this technique appeared to be successful, the stump was not divided and late recanalization remains a possibility.
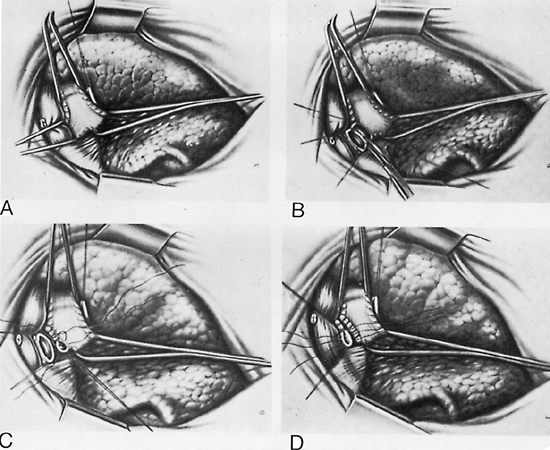 |
Fig. 37-3. Right posterior approach to the left main-stem bronchus. A. The trachea and both main-stem bronchi have been isolated and tape placed around them. B. The left main-stem bronchial stump is dissected off the trachea. C. The trachea is closed with interrupted sutures. D. The remaining distal stump is closed in a similar manner. From Perelman MI, Rynko LP, Ambatiellom GP: Bronchopleural fistula: surgery after pneumonectomy. In Eschepasse H, Grillo HC (eds): International Trends in General Thoracic Surgery. Major Challenges. Vol. 2. Philadelphia: WB Saunders, 1987. With permission. |
Bronchopleural fistula rarely occurs after a lobectomy. The management of the open bronchial stump and the usually associated empyema space is similar to that following a pneumonectomy except that the presence of pulmonary tissue in the hemithorax modifies the management to a variable extent (see Chapter 59). Occasionally, it is advisable to perform a completion pneumonectomy, although as noted by McGovern and colleagues (1988), the complication rate is high (over 50%). Deslauriers (1988) emphasized the hazard of previous irradiation when a completion pneumonectomy is contemplated. He also noted that when a bronchial dehiscence is the indication for completion pneumonectomy accompanying a benign inflammatory process, other therapeutic options deserve serious consideration before resorting to this procedure. Bronchial dehiscence and fistula formation also occur after bronchoplastic or tracheoplastic procedures. In a survey of 1,562 such procedures performed in Japan, Maeda and associates (1989) reported this complication in 5.6% of cases, with death in 47.7% of the patients in whom it occurred, for an overall mortality rate of 2.7%.
The reported mortality rate after the development of a bronchopleural fistula is variable. Rates as low as 16% to as high as 72% have been recorded. Most deaths are due to sepsis, respiratory insufficiency, and malnutrition. Rarely, an inflammatory erosion of the pulmonary artery stump will occur, with resulting fatal hemorrhage. Khargi and associates (1993) recorded a 4% incidence of this event, with a 50% mortality rate. Most series have not been composed of comparable patients, disease states, or operations, so that it is difficult to state categorically which patients are most likely to succumb as a result of a BPF. However, those who have undergone an extensive peribronchial dissection or a right-sided pneumonectomy or who received preoperative irradiation appear to be at greatest risk. Others at high risk are those who have undergone a tracheoplastic or bronchoplastic procedure, have borderline pulmonary function, have a serious comorbid disease, or are elderly.
An excellent summation on the subject of bronchopleural fistula by several of the authors cited earlier is presented in a review edited by Miller (2001).
Pleural Complications
Persistent Residual Spaces
There is little literature that specifically addresses postresection spaces, probably because they are essentially an expected finding after lobectomy. There is no standard definition of persistent (in contrast to air leaks), and they are rarely clinically significant unless infected (in which case the definition becomes empyema rather than space ) or large enough to cause symptoms. Following most lobectomies, a variable volume of the pleural space is initially unfilled by expansion of the remaining lung tissue. This is a common finding on plain radiographs and can almost always be seen by CT scan. Most spaces resolve rapidly.
Persistent residual air spaces are more common in resections for inflammatory or infectious diseases, lung volume reduction surgery, and resections of any type performed in patients with emphysema or diffuse fibrotic processes. In these disease processes the rarified or poorly compliant ( stiff ) remaining lobes fail to readily fill the void left in the hemithorax. By virtue of leaving a larger space and less parenchyma, bilobectomy is also a risk factor. In addition, if allowed to persist, large undrained postresection fluid collections may result in trapping of the remaining lobe(s), preventing adequate reexpansion and resulting in a fixed space even when drainage is ultimately attempted. Apical spaces are more often encountered than basilar spaces. When resection was common for the management of persistent negative cavitary M. tuberculosis, Shields and colleagues (1959) reported an incidence of persistent residual air space as high as 21%. Persistent pleural air space after a segmentectomy is as high as 33% in patients with pulmonary tuberculosis (Fig. 37-4), but it is much less common after similar resections for neoplasm. Persistent air spaces after a wedge resection occur infrequently. The incidence is less than 10%. Since sublobar resection results in removal of minimal volumes of lung tissue, space problems in this setting are most often related to diffuse restrictive or emphysematous lung disease associated with air leaks, rather than to a primary volumetric parenchymal/pleural mismatch. Presently, most residual spaces are seen after lobectomy for carcinoma, usually upper lobectomy, and most are therefore apical rather than basilar (Fig. 37-5).
Fortunately, as discussed by Miller (1996), the great majority of spaces do not cause problems, and the clinical course of the patient is unaffected or minimally affected by their presence. Most asymptomatic spaces disappear over a period of time by absorption of the gases within the space, further expansion of the remaining lung, mediastinal shift, chest wall adjustment, diaphragmatic elevation, and the deposition of a pleural peel in the area. Some spaces, however, require intervention of varying magnitude for their eventual control. The problems may consist of pain, dyspnea, hemoptysis, sepsis, or continued air leak. Most resolve with simple open flap or open ( empyema )
P.573
tube drainage. Drains can be placed under image guidance, if necessary. If a larger drain is needed, the surgeon may follow the tract of the percutaneous drain. Almost all of this treatment can be accomplished on an outpatient basis, with brief admission for creation of an open flap, if needed. When adequately vented, most spaces will resolve by the mechanisms noted previously. Soft mushroom catheters are reliable and easy to manage as an alternative to open drainage in many cases.
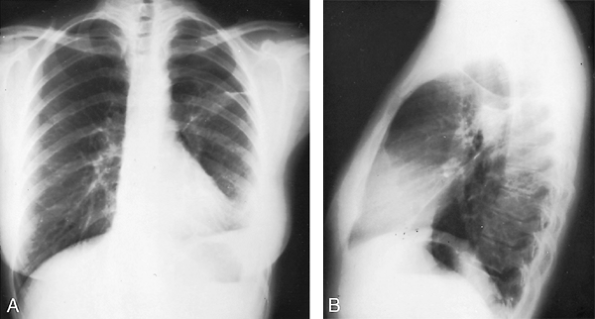 |
Fig. 37-4. Posteroanterior (A) and lateral (B) radiographs reveal an asymptomatic air space 6 weeks after a left apical posterior segmentectomy was performed for treatment of pulmonary tuberculosis. |
In the minority of cases that fail to resolve over a period of time, most of which are associated with persistence or development of a BPF with or without empyema, surgical space reduction or filling by muscle flaps, thoracoplasty, or combination approaches is indicated, as described in Chapters 59 and 62.
P.574
Although some have proposed chronologic indices for proceeding to surgical intervention, the decision should be individualized based on the patient's clinical and radiographic status, including whether the process and its sequelae are worsening, slowly improving, or static and on the oncologic and general prognosis aside from the space issue. In a young, working person with a good prognosis it would often be better to proceed sooner, whereas in an elderly person who is not deteriorating and is tolerating outpatient treatment, waiting a few weeks may often be wiser than proceeding to a major operation based on arbitrary time frames.
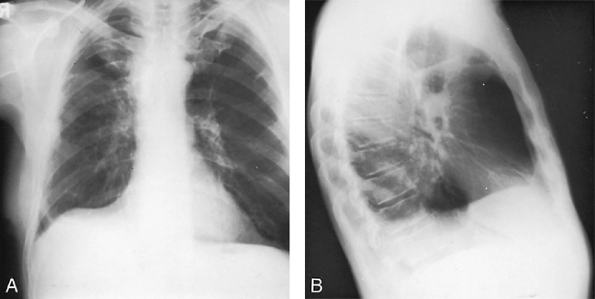 |
Fig. 37-5. Posteroanterior (A) and lateral (B) radiographs of the chest show an asymptomatic residual air space 4 weeks after a right upper lobectomy for carcinoma of the lung. |
Pleural Effusion
A small collection of pleural effusion at the base of the hemithorax is common after lobectomy or a lesser resection, but major collections are uncommon if satisfactory pleural drainage has been maintained. Although most small to moderate effusions are resorbed over time, when a significant amount of fluid persists, drainage by thoracentesis should be the first step. Tube drainage should be considered for recurrence. Drainage is indicated if the effusion is felt to be causing symptoms. In the absence of dyspnea, there are no clear guidelines for intervention. As noted earlier, however, a large chronic effusion may result in trapped lung, thus potentially leading to a difficult, long-term space problem. In addition, multiple thoracenteses may also cause visceral pleural reaction and fibrosis resulting in trapped lung. Fear of infection is not an indication to drain a small, asymptomatic effusion, since the spontaneous development of infection in the absence of a fistula or pneumonia is exceedingly rare. On the contrary, multiple interventions are likely to increase the possibility of conversion of a sterile collection to an empyema.
Empyema
As noted in a comprehensive review by Vallieres (2002), empyema following pulmonary resection currently occurs less frequently than in the early years of thoracic surgery. The reported incidence of empyema after pneumonectomy ranges from 2% to 16%, and is about 5% to 7% in most series. A review by Deschamps and colleagues (2001), for example, of 713 pneumonectomies at the Mayo Clinic showed that 53 patients (7.5%) developed an empyema. The majority following pneumonectomy are associated with a BPF. Empyema is much less common after lobectomy, segmentectomy, or wedge resection, reportedly occurring in 0.01% to 2% of cases. These cases are less often associated with a BPF, and more often idiopathic or related to alveolar air leak, persistent spaces, or resection for infectious processes. Multiple additional risk factors have been implicated in the development of postresection empyema, many of which are concordant with those for BPF and for prolonged air leaks and significant residual spaces, since these problems may result in empyema. Among these are advanced age, cardiopulmonary impairment, malnutrition, induction radiation or chemotherapy, steroid use, diabetes, right pneumonectomy, completion pneumonectomy, prolonged complex operation, emergency resection for trauma, postoperative pneumonia, and postoperative mechanical ventilation. Porte and associates (2001) found an unexpectedly high number of empyemas following the use of synthetic sealants employed to minimize air leaks and described drainage of infected sealant along with pleural contents. Because intraoperative measures to reduce alveolar air leaks are receiving considerable current attention, it is important to note that no other studies have found empyema to be a problem with the use of these various materials, although the issue remains unresolved.
When a postresection empyema occurs, the patient shows a greater or lesser degree of systemic toxicity, the white blood cell count is elevated with a shift to the left, the appetite is poor, and general deterioration occurs. At times, it is difficult to establish a definitive diagnosis of the presence of a frank empyema. The threshold should be low for a diagnostic sampling for culture of the pleural fluid. Once the diagnosis is established, immediate tube drainage of the space is indicated. Broad-spectrum antibiotics are given and adjusted once cultures and sensitivity results are available. The therapeutic route from this point on depends on multiple factors, including the presence or absence of a bronchopleural fistula, the chronicity of the empyema, the adequacy of drainage as determined radiographically and by the patient's response, the size of any remaining space, and the patient's prognosis unrelated to the infection. In some cases following lobectomy or lesser resection, a short period of closed-tube drainage alone may be sufficient. In other instances, conversion to an open empyema tube and outpatient management may over time result in resolution. If the problem is diagnosed soon after operation and associated with a BPF, early fistula repair and space elimination may be the most expeditious maneuver. If the space is large and more chronic, open flap drainage may be a superior approach. If the sepsis is treated, the patient remains stable, and the space diminishes over time, this approach alone may result in cure and be followed by simple closure of the open chest wall window. Most large infected spaces and essentially all postpneumonectomy empyemas will require open drainage followed at the appropriate clinical point (determined by patient status, including nutrition, space volume, and the appearance of the lining granulation tissue) by a Clagett procedure or a modification thereof, or by space obliteration using muscle flaps, omental transposition, thoracoplasty, or combination operations. In addition to imaging to assess the volume of the remaining space over time, a simple office method entails filling the space with saline via an indwelling tube or open window and noting the volume. This method, of course, cannot be used in the presence of a BPF.
P.575
As with BPF and prolonged air leaks, although basic rules apply, an individualized approach is optimal. Algorithms exist, but none is either absolute or comprehensive. These issues are addressed in Chapters 59 and 62 and in the reviews of Vallieres (2002), Miller (1996), Pezzella and associates (2000), and De Hoyos and Sundaresan (2002). The assessment and management of these not uncommon postresection complications are challenging problems that should be dealt with only by experienced general thoracic surgeons.
Postresection Chylothorax
The anatomy of the thoracic duct and the problem of chylothorax are discussed in detail in Chapter 63. Chylothorax is rare after pulmonary resection. Simpson (1990) stated that the incidence of such injury was less than 0.05%. However, Brie (1990), Sarsam (1994), and Terzi (1994) and their associates report rates of 0.3%, 0.5%, and 0.74%, respectively, in their experience. Cerfolio and colleagues (1996b) reported that only 13 of the 47 chylothoraces occurring in 11,000 thoracic operations at the Mayo Clinic followed lung resection, despite the great preponderance of pulmonary over esophageal resections. Several decades ago most injuries followed resections for benign diseases, mainly tuberculosis, but at present they are more common after resections for the treatment of lung cancers that require pneumonectomy and extensive hilar and mediastinal dissection. Chylothorax may also occur after lobectomy. Injury to the duct may occur anywhere along its course, or the injury may be to lymphatic channels from the lung or lymph nodes that enter directly into the thoracic duct, which were demonstrated by the anatomic study of Riquet and associates (1989).
Because most lung resection patients resume oral alimentation on the day of or the day after operation, the diagnosis of chylothorax is usually made early. In the postlobectomy patient, the chylothorax is manifest by a change in the character of the drainage to a cloudy or milky fluid and an increase in the amount of drainage. In pneumonectomy cases treated without a chest tube or whose tubes are removed on the first postoperative morning, the diagnosis is more elusive. In nine pneumonectomy patients with chylothorax, Sarsam and colleagues (1994) noted a rapid accumulation of fluid in the pleural space without symptoms in five cases and respiratory problems in four patients. The development of a tension chylothorax also was noted by Karwande (1986) and Brie (1990) and their colleagues. Emergency thoracentesis will reveal the characteristic milky fluid, and immediate closed-tube thoracostomy is indicated. An elevated amylase level in the pleural fluid is a common finding.
Ngan (1988) and Vallieres (1993) and their colleagues suggested that lymphangiography be performed soon after the diagnosis is made. Standard lipoidal lymphangiography, despite the risk of an occasional pulmonary complication, may demonstrate the site of the leak or the lack of one at best. Le Pimpec-Barthes and associates (2002) suggest that lymphangiography need be performed only when reoperation is being contemplated based on other factors. Nuclear lymphangiography, although used by Rice and associates (1987), may not be successful in this regard. Lipoidal lymphangiography is both diagnostic and prognostic. When no major leak is seen, or only a leak from a small pulmonary or nodal lymphatic, and the contrast material appears at the venous terminus of the thoracic duct, most investigators believe that conservative management is more likely to be successful.
Treatment consists of an initial period of expectant therapy with continued drainage and total parenteral nutrition or a low-fat diet and medium-chain triglycerides. With reexpansion of the remaining lung in the lobectomy patient, the leak frequently seals (approximately 50% or more of patients), but spontaneous closure is less likely in the pneumonectomy patient. In a pneumonectomy patient, a continued leak of more than 300 mL per day is an indication for surgical intervention with ligation of the thoracic duct or local control as described in Chapter 63. In the series reported by Brie and associates (1990), this step was necessary in all four patients who had undergone a pneumonectomy. In the lobectomy patient, a persistent leak of 500 mL per day is an indication of failure of conservative management. Operative intervention is then required. In the series of Le Pimpec-Barthes and colleagues (2002), reoperation was required overall in 6 of 26 patients. The negative effect of pneumonectomy in this experience is demonstrated by the fact that 5 of 8 such patients underwent reoperation versus only 1 of 18 lobectomy or bilobectomy cases. The method of repair depends on the findings. In addition to open ligation of the thoracic duct or control of the actual leaking sites, Morita (1990) and Landreneau (1992) and their colleagues have used a video-thoracoscopic surgical approach to control the chylous leaks. Stenzl (1983) and Akaogi (1989) and their associates reported successful closure of leaks with the use of fibrin glue applied through tube thoracostomies. Options for control of this complication, as well as a discussion of the problem in general, are reviewed by Johnstone (2002).
Esophageal Injury
As noted by Trastek and associates (1992) and by Massard and Wihlm (1999), injury to the esophagus is a rare complication of pulmonary resection that occurs more often during pneumonectomy than other operations and more often on the right (70% among pneumonectomy cases) because of the location of the esophagus in relation to the hilar and mediastinal nodes and to the trachea and carina. The usual setting is a difficult dissection during a pneumonectomy performed for either an inflammatory process or extensive neoplastic disease. Shama and Odell (1985) reported an incidence of 0.5% in a series of 869 pneumonectomies for inflammatory disease. Van den Bosch and associates (1980)
P.576
confirmed that most (92%) occurred on the right. Benjamin and colleagues (1969) reported its occurrence during resection for carcinoma. Massard and colleagues (1994) recorded seven esophageal injuries that occurred during lung resections: six during removal of a carcinoma and only one during operation for an inflammatory process.
In contrast to Evans's (1972) belief that most esophageal fistulae resulted from erosion of a peribronchial abscess into the esophagus, most surgeons now consider that the injury to the esophagus occurs at the time of surgery and that only the manifestation of the resultant empyema is recognized late. Massard and Wihlm (1999) divide esophagopleural fistulae into early and late groups. The etiology of the problem in the former group is direct tearing of the esophagus, entry into a diverticulum, or devascularization/necrosis due to extensive dissection or electrocautery. Late cases (beyond 3 months) are caused by tumor recurrence, postoperative infection or inflammation, or radiation necrosis.
When a difficult mediastinal dissection is encountered intraoperatively, peroral placement of a large bougie may aid in identifying and protecting the esophagus. If an injury is suspected, injection of air or methylene blue may locate the site. When recognized at operation, immediate repair, often buttressed by a pleural, intercostal muscle or other viable tissue flap, usually is successful. If the injury is not recognized intraoperatively, mediastinitis and empyema occur. Recognition of the source of the infection may be elusive until oral feedings are observed in the thoracic drainage. Less conclusive signs include dysphagia, odynophagia, and dysgeusia. Any empyema following pneumonectomy in the absence of BPF, especially if new air appears in the pleural space on radiographs, should arouse a suspicion of esophageal leakage. The diagnosis is usually confirmed by a contrast esophagogram. As in the case of suspected perforation from any cause or routine postesophagectomy study, the study begins with soluble contrast or dilute barium and proceeds to full barium if results are negative using these contrast agents.
Initial treatment requires pleural drainage, cessation of oral intake, and establishment of an alternate means of nutrition. Definitive surgical treatment basically parallels that for any esophageal injury and depends mostly on the chronicity of the process and the state of the local tissues, as discussed in Chapter 138. For late presentations it is imperative to assess the patient for cancer recurrence before embarking on extensive operative interventions. Unfortunately, the overall results, as noted by Massard and co-workers (1994), are poor, with prolonged morbidity and a high incidence of eventual mortality.
Wound Complications
Wound Infections
Infection of a thoracotomy or sternotomy incision after a pulmonary resection is rare. When present, the usual signs and symptoms of infection are observed. Open drainage and antibiotics are indicated in its management.
Wound Dehiscence
Complete breakdown of a thoracic incision after a pulmonary resection is even less common than a wound infection. Early dehiscence requires prompt reclosure, but late dehiscence, most often the result of wound infection, may be managed initially by local d bridement and pleural drainage, with subsequent reclosure when the infection has been controlled.
Subcutaneous Emphysema
Air trapped within the pleural space after a pneumonectomy, or air from a leak that is not being removed effectively by a chest tube drainage system after a lobectomy or lesser resection, may be forced out through the intercostal incision into the soft tissues of the chest wall on change of position or coughing. This subcutaneous air may be localized only to the wound area, but when excessive amounts of air are forced into the adjacent tissue planes, it may extend up into the neck and face and down to the groin and into the scrotum. The eyelids may become so swollen as to be closed and immobile. Although the patient's appearance may be grotesque and alarming to family members, the incidence of clinical problems is vanishingly low. In the vast majority of cases, no specific therapy other than to ensure patency of the drainage system or to place additional drains is required. If additional chest tubes are required, computed tomography may be useful in deciding where to place them by delineating any pockets of retained intrapleural air. In addition, percutaneous drains may be placed under image guidance. In most cases, however, the lung is largely or fully expanded. On occasion, the sudden appearance of massive subcutaneous emphysema may indicate the occurrence of a bronchopleural fistula, but in most instances, subcutaneous emphysema is a benign, self-limiting process. Upper airway obstruction as a result of subcutaneous emphysema is a rare complication, and the use of cervical incisions to decompress the area is not indicated. If airway obstruction is suggested clinically, endotracheal intubation is indicated until the compression resolves.
Neurologic Complications
Injury to Intrathoracic Nerves
Phrenic Nerve
Unsuspected injury to the phrenic nerve rarely occurs during pulmonary resection. Unintentional injury is most often due to mechanical or electrocautery attempts to control bleeding from the vein that accompanies the nerve or when dense mediastinal adhesions need to be divided for hilar exposure. More often a segment of the nerve is intentionally
P.577
resected in the removal of a tumor invading the mediastinum or in the excision of metastatic nodes anterior to the superior pulmonary vein. Although most patients clinically tolerate unilateral loss of diaphragmatic function, paralysis does lessen ventilatory capacity, even when present on the side of a pneumonectomy. The consequences to people with marginal pulmonary function may be significant. Purposeful injury or division of the nerve to paralyze the hemidiaphragm in order to reduce the volume of the ipsilateral hemithorax ( phrenic crush ) is to be avoided, except in unusual circumstances.
Recurrent Laryngeal Nerves
Recurrent nerve injury occurs far more often on the left and results from mechanical or cautery dissection of mediastinal lymph nodes or invasive tumor in the aortopulmonary window at the ligamentum arteriosum. Exposure of the nerve at this time may be helpful in avoiding its injury. Right-sided injury is rare in cases of pulmonary resection, being seen only with extensive high node dissections. Unilateral damage results in hoarseness and in some cases can also cause serious problems with aspiration and clearance of secretions. The consequences of impaired cough are usually more dangerous in pneumonectomy patients than in those who have undergone lesser resections. In a series of complete mediastinal lymph node dissections in patients with lung cancer, unintentional injury was observed in 3 of 62 patients by Bollen and associates (1993). The number of left-sided dissections was not recorded, so the actual incidence of this injury remains unknown. It should be noted that the incidence of this injury is often not specified by the many advocates of routine complete lymph node dissection in lung cancer patients.
In patients who have received neoadjuvant therapy for locally advanced lesions, injury to or the necessary removal of either the vagus or phrenic nerves because of the extent of the disease process, as noted by Yashar and colleagues (1992), may increase the number of these injuries. Fortunately, there are currently relatively simple and effective methods to achieve medialization of the affected vocal cord, as described by Carew and co-workers (1999). It is common to wait several months before recommending medialization when the exact technical cause of the injury is unknown and the patient is asymptomatic aside from hoarseness, based on the fact that many patients improve over time. When it is clear, however, that the nerve has been divided or the patient is having significant secretion problems, early repair is indicated.
Spinal Cord Injury
Injury to the spinal cord with resultant paraplegia usually results from attempts to control persistent bleeding from intercostal vessels, or to stop continued oozing at the posterior angle of the intercostal incision or at the site of removal of a portion of a vertebra. Thrombosis of the anterior spinal artery is an infrequent cause.
The use of unipolar cautery is to be avoided in these areas, as is packing of the area with hemostatic substances such as oxidized cellulose. Either continued bleeding with egress of blood into the spinal canal or migration and swelling of the hemostatic material within the canal, as reported by Short (1990), may compromise the space and result in pressure on the spinal cord.
Attar and colleagues (1995) reported five instances of paraplegia from their own institution and reviewed 35 cases reported in the literature. They confirm that the major intraoperative factors contributing to this devastating complication were bleeding at the costovertebral angle and the use of oxidized cellulose to control this bleeding, with subsequent migration and swelling of the material in the spinal canal. Thrombosis of the anterior spinal artery, epidural hematoma, epidural narcotic, metastatic carcinoma, and intraoperative hypotension were infrequent causes. If bleeding in the costovertebral angle appears significant and persistent, the thoracic surgeon should seek neurosurgical assistance for widening of the foramen, bipolar cautery control, and other specialized techniques. The avoidance, prophylactic management, and early recognition of this complication during the operative procedure were discussed by Walker (1990) and Benfield (1990). Unfortunately, even early postoperative diagnosis and prompt neurosurgical decompression of the spinal cord frequently fails to reverse the process.
Dural Laceration: Subarachnoid-Pleural Fistula
Laceration of the dura without damage to the spinal cord may occur during pulmonary resection and result in a subarachnoid-pleural fistula, commonly called a cerebrospinal fluid (CSF) leak. Most often, this complication occurs during resection of lung neoplasms that invade the posterior chest wall in the region of the costovertebral angle, such as Pancoast's tumors. However, nerve root avulsion and CSF leak can result from rib retraction during any thoracotomy, as reported by Frantz and Battaglini (1980) and Da Silva and associates (1987), among others. If the diagnosis is made intraoperatively, usually by the identification of clear CSF draining into the operative field from the posterior aspect of the intercostal incision, closure should usually be carried out at that time. Although pleural and muscle flaps placed into the foramen have been successful, it is generally prudent to seek intraoperative neurosurgical consultation for consideration of foraminal widening, direct dural suture or patching, or a planned immediate or staged approach to the problem by posterior laminectomy.
Because of small volumes of drainage and mixing with blood during the operation, a CSF leak is more often recognized in the postoperative period. With decreasing proportions of blood over time, the chest tube output becomes clear and persists in higher volumes than expected. A clinical diagnosis of CSF leak can be made by this finding following an operation requiring dissection in the costovertebral region. Plain radiographs of the skull or cranial CT may show pneumocephalus in some cases. Bilsky and associates (2001)
P.578
reported three cases of tension pneumocephalus, two of which followed pulmonary and posterior chest wall resection and the third of which appeared after resection of a posterior mediastinal tumor. This finding is due to the entry of pleural air via sufficiently large fistulae into the subarachnoid space during the positive-pressure phases of mechanical or spontaneous ventilation and coughing. If the diagnosis remains in doubt, radionuclide myelography, as reported by Pollack and co-workers (1990), may demonstrate the fistula. Many patients are asymptomatic, but others develop headache, seizures, mental status changes, focal neurologic findings, or signs of meningeal irritation. Death has been reported. Although often discussed, bacterial meningitis is rare. Although some fistulae close spontaneously, early neurosurgical consultation is warranted. If the diagnosis is suspected, chest tubes should be converted from suction to water seal in order to lessen CSF drainage since the pressure gradient favoring air entry from the pleura into the subarachnoid space is increased in the presence of less CSF in this space. Closure of the fistula can be performed by the aforementioned techniques. A posterior hemilaminectomy approach is generally preferable to reopening the thoracotomy.
Peripheral Tumor Emboli
Embolization of tumor fragments is a very rare complication of lung resection. A tumor embolus may be dislodged from a pulmonary vein involved by tumor during the isolation and ligation of the vessel. Taber (1961) and Senderoff and Kirschner (1962) were the first to report the occurrence of a massive tumor embolism during pulmonary resection, although Till and Fairburn (1947) previously reported a spontaneous, nonoperative massive embolism in a patient with a far-advanced lung cancer. Whyte and associates (1992) reported 2 cases and reviewed an additional 18 cases in patients with lung cancer or metastatic sarcomas. Spencer and colleagues (1993) reported a patient with multiple tumor emboli occurring during a pneumonectomy. Gomez and colleagues (1995) described an additional case and noted that a total of 31 cases had been reported in the literature. Eighty-four percent of these occurred during a pulmonary resection, and the remainder were spontaneous. In the review of Whyte and associates (1992), the site of embolization was the aortic bifurcation or femoral vessels in 50% of patients. Other sites included vessels of the upper extremities, the cerebral circulation, and the mesenteric arteries. Fifty percent of the patients died.
Removal of the embolus is indicated when possible. Those who survive the acute episode, according to Heitmiller (1992), ultimately die from metastatic spread of the original tumor and not of the effects of the embolic episode per se. Prevention of embolization when a major pulmonary vein is involved is primarily by proximal intrapericardial ligation or stapling of the vessel, including excision of a portion of the adjacent atrium, if necessary. Current imaging modalities should alert the surgeon to the possibility of central vascular invasion prior to operation, and in many cases suggest that primary resection may not be the optimal therapy. The use of cardiopulmonary bypass to remove tumor from the atrium, as suggested by Mansour and colleagues (1988), is inappropriate in patients with lung cancer, except in patients with a low-grade sarcoma.
Complications Not Unique to Pulmonary Resection
Pulmonary Embolism
Pulmonary embolism may occur in 1% to as many as 5% of individuals undergoing a pulmonary resection. This high percentage was recorded in a prospective evaluation of 77 patients by Ziomek and colleagues (1993). The site of origin of the embolus was in the lower extremities. Occasionally, the site may be in the veins of the pelvis. Sudden death may occur, but most patients survive long enough to permit diagnosis and treatment. Nonetheless, in the postresection patient, the overall mortality rate is 50%, according to Nagasaki and associates (1982).
An unusual site of origin of the embolus in postpneumonectomy patients is a thrombus in the pulmonary arterial stump. Chuang and colleagues (1966) reported that thrombosis occurred in 1% of postpneumonectomy patients. It is said to occur twice as often after a right than after a left pneumonectomy. This may be the result of the longer length of the right arterial stump. Takahashi and associates (1993) noted that the right pulmonary artery stump is 42 to 43 mm long, whereas the left stump is usually less than 10 mm in length. The thrombosis may be due to lack of effective flow in the stump or, theoretically, could develop due to puckering and infolding of the vessel by the ligature, which could increase the likelihood of thrombosis within the vessel. A vascular suture closure or stapling of the vessel may lessen the already minimal risk of this complication. In the report of Harpole and colleagues (1999), pulmonary embolism, although uncommon overall, occurred twice as often after pneumonectomy (1.4%) than following lobectomy (0.7%).
Deep Venous Thrombosis
In the aforementioned prospective study of Ziomek and colleagues (1993), 4 of the 77 patients had evidence of deep venous thrombosis preoperatively, and an additional 11 cases developed postoperatively, for an overall incidence of 19%. As noted, 4 pulmonary emboli occurred in the 77 patients. Of interest was the observation that none of these complications occurred in 17 patients who were taking aspirin or ibuprofen preoperatively (a controlled study relative to this certainly is indicated). Lastly, these authors noted that the thromboembolic events occurred more commonly
P.579
in patients who had adenocarcinoma, a large tumor, a major resection, and a higher TNM stage.
Renal Failure
In most series, renal failure is a rare complication. However, Patel and associates (1992) documented this event in 15% of 197 patients undergoing a pneumonectomy. The renal failure occurred most often in patients whose age was greater than 70 years. These authors, among many others, also found renal failure to be a strong predictor for operative mortality. Harpole and colleagues (1999) noted a doubling of the incidence of renal failure in pneumonectomy cases (1.4%) versus lobectomy patients (0.7%).
Cerebrovascular Accident
Data relative to the frequency of this complication are lacking, but an occasional stroke is observed postoperatively. In cancer patients, it is imperative that a true cerebrovascular event be differentiated from the postoperative manifestation of a previously occult cerebral metastasis. The use of magnetic resonance imaging and positron emission tomography may promptly resolve the issue.
Massive Gastrointestinal Hemorrhage
Massive gastrointestinal hemorrhage likewise is an uncommon complication. It is rarely seen as a single event but more often is observed in association with other life-threatening complications in the setting of sepsis and multiple organ failure and is often a terminal event.
READMISSION FOLLOWING PULMONARY RESECTION
Despite the fact that early postoperative readmission to the hospital is often due to a surgical complication, little data exist on rates of readmission following lung resection. Since, as shown by several studies of readmission following cardiac surgery, a high proportion of patients are treated at hospitals other than the site of the primary operation, rates of complications may actually be higher than usually reported.
Handy and colleagues (2001) reported on readmissions among 366 lung resection patients. The rate of readmission was 19%, with some patients having more than one hospitalization. Sixteen percent were admitted to other hospitals on their first readmission, a figure that climbed to 36% by the third readmission. Analysis of multiple factors showed that only pneumonectomy was a reliable predictor of readmission, with a rate of 36%. Overall, the major causes for readmission were pulmonary (27%), surgical infection (14%), cardiac (7%), and other causes (16%). It is important that the authors included a postdischarge period of 90 days in their definition, since the mean time to readmission was 32 days. Thus, using a 30-day definition would have missed many cases. McKenna and associates w(1998) reported a readmission rate of only 0.9% during a follow-up period of over 2 years of 212 patients who had undergone video-assisted lobectomy. Wright and co-workers (1997) noted a readmission rate of 1.8% among 277 lobectomies performed after institution of a clinical pathway, but limited their definition to a 7-day postdischarge period. Clearly, the paucity of data on this issue and the vastly different figures just noted suggest that this issue be studied further and among larger groups.
LATE COMPLICATIONS
Most late complications that are the result of the surgical procedure and are not related to residual or recurrent cancer occur in pneumonectomy patients or in patients who have residual spaces following lobectomy or lesser resections. Although they are important clinical issues, chronic pain syndromes, respiratory insufficiency due to progression of emphysema, heart disease, recurrent pulmonary infections, and complications resulting from adjuvant chemotherapy or radiation will not be discussed because they are not directly related to pulmonary resection, but rather to the incisional approach or to underlying disease states. In addition, postresection left-to-right shunt, which may occur or become increasingly symptomatic late after operation, has been discussed previously.
Postpneumonectomy Syndrome
In infants and children, and less frequently in young or middle-aged adults, progressive mediastinal shift after a pneumonectomy will gradually occur to an extreme degree with the passage of time. In their comprehensive discussion of this problem, Mehran and Deslauriers (1999) noted that the etiology of excessive shift is multifactorial and related not only to hyperinflation of the remaining lung but also to hyperplasia (especially in children) and to the size of the pneumonectomy space, chest wall and diaphragmatic changes, and elasticity of the mediastinal tissues. The resultant stretching and compression of the trachea or remaining bronchus or both over the pulmonary artery, aorta, or vertebral column can lead to severe respiratory compromise, tracheobronchial malacia, repeated infections, bronchiectasis, and parenchymal destruction. The syndrome is far more common after a right pneumonectomy, is infrequently seen after a left pneumonectomy in patients with a right-sided aortic arch, and is observed very rarely after a left pneumonectomy in patients with normal aortic anatomy.
Right Postpneumonectomy Syndrome
After a right pneumonectomy, excessive displacement of the heart with a counterclockwise rotation of the great vessels
P.580
and of the trachea leads to a stretching and narrowing of the left main-stem bronchus between the aorta and the pulmonary artery, as well as compression of the left pulmonary vessels. The narrowing of the bronchus results in severe respiratory insufficiency. Adams (1972), Szarnicki (1978), and Wasserman (1979) and their associates were among the first to describe this syndrome, although Maier and Gould (1953) were the first to describe the pathophysiology resulting in the syndrome in a young patient following pneumonectomy for agenesis of the right lung.
Although children may become symptomatic early after operation, the clinical presentation in adults is usually delayed for a variable and often very long period of time. Typical symptoms include dyspnea, stridor, recurrent pulmonary infections, and occasionally orthopnea and dysphagia. In some instances symptoms do not become apparent until tracheomalacia occurs many years after operation. Bronchoscopic examination and the findings on CT examination of the chest, as described by Shepard and colleagues (1986), are diagnostic (Fig. 37-6). Of note is that the case described by these authors was diagnosed 37 years after pneumonectomy. Bronchoscopy documents airway compression and may suggest malacia. CT scan shows an astounding counterclockwise rotation of the heart and compression and stretching of the airway. Boiselle and colleagues (1997) note that inspiratory and expiratory CT may be useful for identifying tracheomalacia in postpneumonectomy syndrome. Because pneumonectomy patients often have dyspnea and progression of emphysema, especially if they continue to smoke, a high index of suspicion is needed to diagnose this syndrome on purely clinical grounds. A plain radiograph showing excessive mediastinal shift, however, should alert the clinician to this possibility.
The most successful treatment has been dissection of adhesions and the placement of prosthetic devices in the ipsilateral hemithorax to restore the heart and lung to a more normal position and thus relieve the obstruction of the bronchus. Such procedures have been described by Wasserman (1979), Powell (1979), Riveron (1990), Rasch (1990), Grillo (1992), Jansen (1992), and Audry (1993) and their associates. A variety of devices have been used, as summarized by Mehran and Deslauriers (1999), including lucite balls, individually constructed plastic prostheses, silicone breast or testicular implants, and standard or inflatable saline breast implants. Silicone devices have been abandoned
P.581
because of their possible causation of immunologic diseases. Expandable saline prostheses appear to be effective, as noted by Grillo (1992), Audry (1993), and Shamji (1996) and their colleagues. Correction of malacia, if present, using various posterior supports, resection and reanastomosis, or silastic stents, as reported by Nissen (1954), Herzog (1987), Moser (1994), and Grillo (1992) and their colleagues, has been mainly unsuccessful. Although experience is limited, newer expandable metallic mesh stents appear to be superior, as described by Evans and Clark (1995), and by Shah (1995) and R. F. Kelly (2001) and their colleagues.
 |
Fig. 37-6. The right postpneumonectomy syndrome. A. Posteroanterior chest radiograph with shift of the left lung into the right hemithorax. Computed tomographic scans reveal compression of the left main-stem bronchus by the adjacent vessels. Soft tissue windows at the level of the aortic arch (B) and the left pulmonary artery (C) demonstrate a small postpneumonectomy space (PPS). The aortic arch (Arch) and pulmonary artery are rotated counterclockwise. The trachea (T) is to the right of the spine (Sp), and the left main bronchus (arrow) crosses anterior to the thoracic spine and posterior to the left pulmonary artery (LPA). From Grillo HC, et al: Postpneumonectomy syndrome: diagnosis, management and results. Ann Thorac Surg 54:638, 1992. With permission. |
Left Postpneumonectomy Syndrome
Quillin and Shackelford (1991), as well as Shephard (1986) and Grillo (1992) and their associates, described the same obstructive syndrome after left pneumonectomy in patients who had a right-sided aortic arch. It was believed that the syndrome could not occur with a normally situated left aortic arch. However, Shamji and colleagues (1996) described four patients with a normally located aortic arch in whom the syndrome developed after left pneumonectomy. The bronchial obstruction was believed due to a clockwise rotation of the pulmonary vessels and trachea, with compression of the right main bronchus between the right pulmonary artery and the spine (Fig. 37-7). Three of the four were successfully treated with the placement of a saline-filled prosthesis into the left pleural space to reposition the heart and right lung in a more normal anatomic position. The fourth patient was managed by removal of a portion of the offending thoracic vertebra. R. F. Kelly and co-workers (2001) reported a successful outcome in a patient with the syndrome and a normal aortic arch who was initially treated with saline implants, but required deployment of an expandable stent several months later.
 |
Fig. 37-7. Contrast-enhanced computed tomographic scan at the level of the right pulmonary artery and bronchus intermedius demonstrates narrowing of the airway caused by compression between the right pulmonary artery and spine (arrow). Marked mediastinal shift and clockwise rotation exist. From Shamji FM, et al: Postpneumonectomy syndrome with ipsilateral aortic arch after left pneumonectomy. Ann Thorac Surg 62:1627, 1996. With permission. |
Superimposed Late Infection
Late Empyema
Pyogenic Empyema
Daly (1999) has recently discussed empyema occurring late after pneumonectomy. Although more common after pneumonectomy, late empyema may occur in any residual pleural space as a result of a hematogenous spread of an organism from another site in the body, from an adjacent pneumonia, or from the late occurrence of a bronchopleural fistula, often the result of recurrent tumor. The course is often indolent and may become manifest only by the occurrence of an empyema necessitans. Drainage and subsequent management is that of any other empyema, with variations based on the presence or absence of a fistula or of recurrent cancer.
Hemorrhagic Empyema
Shimada and colleagues (1991) reported the rare occurrence of a chronic expanding hematoma in a postpneumonectomy space many years after the original procedure. The origin of the bleeding was from granulation tissue within the space. Clinical symptomatology was the result of pressure and distortion of the mediastinal structures and the remaining lung. Surgical evacuation of the chronic hematoma was successful. The term hemorrhagic empyema was applied to this very uncommon late complication.
Superimposed Fungal Infection
The most commonly reported fungal infection that becomes clinically apparent late after a pulmonary resection is due to Aspergillus organisms. Massard and associates (1992) reported 10 cases of aspergillosis that developed in a persistent pleural space after a lobectomy; the initial lobectomy was performed for the treatment of lung cancer in 6, for pulmonary tuberculosis in 3, and for an aspergilloma in 1. The most effective treatment was a thoracoplasty. Open drainage, as suggested by Shirakusa and colleagues (1989), is not advocated by Massard and associates (1992) because it requires a second procedure, either a muscle transfer or an eventual thoracoplasty.
Retained Foreign Body
On rare occasions, a foreign body, most often a surgical sponge, is unintentionally left within the pleural space after
P.582
a lung resection. Patel and colleagues (1994) have coined the term gossypiboma to describe retained cotton material within a body cavity. These authors removed by a lobectomy a retained sponge that had caused a severe pulmonary infection after a cardiac procedure. Preoperatively, the infection was thought to be due to an echinococcal cyst. Nomori and associates (1996) reported one case that occurred after a pulmonary resection and reviewed four additional cases in the Japanese literature. In their case, the retained sponge in the pleural space resulted in the development of a foreign body granuloma that years later eroded into a bronchus, with subsequent episodes of hemoptysis. Radiologic examination including MR imaging revealed a cavitary mass containing an air crescent that resembled an aspergilloma. Resection was successfully carried out and revealed the offending foreign body. Foreign bodies that are placed intentionally, such as pericardial or chest wall patches or saline implants, may also become infected late after the original operation. Treatment may be complex and require several operative procedures.
REFERENCES
Abruzzini P: Trattenento chirurgico della fistule del broncho principale consecutive a pneumonectomia per tubercolosi. Chir Torac 14:165, 1961.
Adams HD, et al: Severe airway obstruction caused by mediastinal displacement after right pneumonectomy in a child. A case report. J Thorac Cardiovasc Surg 63:534, 1972.
Akaogi E, et al: Treatment of postoperative chylothorax with intrapleural fibrin glue. Ann Thorac Surg 48:116, 1989.
Alexiou C, et al: Pneumonectomy for non small cell lung cancer: predictors of operative mortality and survival. Eur J Cardiothorac Surg 20: 476, 2001.
Al-Kattan K, Cattalani L, Goldstraw P: Bronchopleural fistula after pneumonectomy with a hand suture technique. Ann Thorac Surg 58:1433, 1994.
Amar D, et al: Clinical and echocardiographic correlates of symptomatic tachydysrhythmias and noncardiac thoracic surgery. Chest 108:349, 1995.
Amar D, et al: Effects of diltiazem versus digoxin on dysrhythmias and cardiac function after pneumonectomy. Ann Thorac Surg 63:1374, 1997.
Amar D, et al: Effects of diltiazem prophylaxis on the incidence and clinical outcome of atrial arrhythmias after thoracic surgery. J Thorac Cardiovasc Surg 120:790, 2000.
Asamura H, et al: Bronchopleural fistulas associated with lung cancer operations. Univariate and multivariate analysis of risk factors, management and outcome. J Thorac Cardiovasc Surg 104:1456, 1992.
Asamura H, et al: What are the risk factors for arrhythmias after thoracic operations? A retrospective multivariate analysis of 267 consecutive thoracic operations. J Thorac Cardiovasc Surg 106:1104, 1993.
Attar S, et al: Paraplegia after thoracotomy: report of five cases and review of the literature. Ann Thorac Surg 59:1410, 1995.
Audry G, et al: Expandable prosthesis in right postpneumonectomy syndrome in childhood and adolescence. Ann Thorac Surg 56:323, 1993.
Auerbach AD, Goldman L: Beta-blockers and reduction of cardiac events in noncardiac surgery: scientific review and clinical application. JAMA 287:1435, 2002.
Azorin JF, et al: Closure of a postpneumonectomy main bronchus fistula using video-assisted mediastinal surgery. Chest 109:1097, 1996.
Bakris NC, et al: Right to left shunt after pneumonectomy. Ann Thorac Surg 63:198, 1997.
Baldwin JC, Mark JBD: Treatment of bronchopleural fistula after pneumonectomy. J Thorac Cardiovasc Surg 90:813, 1985.
Bayliff CD, et al: Propranolol in the prevention of postoperative arrhythmias in patients undergoing thoracic surgery. Abstract 59. Presented at the 34th Annual Meeting of the Society of Thoracic Surgeons, New Orleans, LA, January 26, 1998.
Benfield JR: Invited commentary of Short HD: Paraplegia associated with the use of oxidized cellulose in posterolateral thoracotomy incisions. Ann Thorac Surg 50:290, 1990.
Benjamin I, Olsen AM, Ellis FH Jr: Esophagopleural fistula: a rare postpneumonectomy complication. Ann Thorac Surg 7:139, 1969.
Bernard A, et al: Pneumonectomy for malignant disease: factors affecting early morbidity and mortality. J Thorac Cardiovasc Surg 121:1076, 2001.
Bilsky MH, et al: Tension pneumocephalus resulting from iatrogenic subarachnoid pleural fistulae: report of three cases. Ann Thorac Surg 71: 455, 2001.
Blyth DF: Pneumonectomy for inflammatory lung disease. Eur J Cardiothorac Surg 18:429, 2000.
Boiselle PM, et al: Postpneumonectomy syndrome: another twist. J Thorac Imaging 12:209, 1997.
Bollen ECM, et al: Mediastinal lymph node dissection in resected lung cancer. Morbidity and accuracy of staging. Ann Thorac Surg 55:961, 1993.
Bolliger CT, et al: Lung scanning and exercise testing for prediction of postoperative performance in lung resection candidates at increased risk for complications. Chest 108:341, 1995.
Borgeat A, et al: Prevention of arrhythmias after noncardiac thoracic surgery: flecainide versus digoxin. Ann Thorac Surg 51:964, 1991.
Brie M, et al: Chylothorax complicating pulmonary resection. In Deslauriers J, Lacquet LK (eds): Thoracic Surgery: Surgical Management of Pleural Diseases. St. Louis: CV Mosby, 1990.
Brown J, Pomerantz M: Extrapleural pneumonectomy for tuberculosis. Chest Surg Clin N Am 5:289, 1995.
Brunelli A, et al: POSSUM scoring system as an instrument of audit in lung resection surgery. Physiological and operative severity score for the enumeration of mortality and morbidity. Ann Thorac Surg 67:329, 1999.
Bruni F: Bronchopleural fistula: treatment of long stump after pneumonectomy. In Eschapasse H, Grillo H (eds): International Trends in General Thoracic Surgery. Vol. 2. Philadelphia: WB Saunders, 1987.
Brutel de la Riviere A, et al: Transsternal closure of bronchopleural fistula after pneumonectomy. Ann Thorac Surg 64:954, 1997.
Cable DG, et al: Lobar torsion after pulmonary resection: presentation and outcome. J Thorac Cardiovasc Surg 122:1091, 2001.
Camazine B, et al: Herpes simplex viral pneumonia in the post-thoracotomy patient. Chest 108:876, 1995.
Cardinale D, et al: Atrial fibrillation after operation for lung cancer: clinical and prognostic significance. Ann Thorac Surg 68:1827, 1999.
Carew JF, Kraus DH, Ginsberg RJ: Early complications: recurrent nerve palsy. Chest Surg Clin N Am 9:597, 1999.
Cerfolio RJ: Advances in thoracostomy tube management. Surg Clin N Am 82:833, 2002a.
Cerfolio RJ: Air leaks and the pleural space. Chest Surg Clin N Am 12:3, 2002b.
Cerfolio RJ, et al: Lung resection in patients with compromised pulmonary function. Ann Thorac Surg 62:348, 1996a.
Cerfolio RJ, et al: Postoperative chylothorax. J Thorac Cardiovasc Surg 112:1361, 1996b.
Cerfolio RJ, et al: Predictors and treatment of persistent air leaks. Ann Thorac Surg 73:1727, 2002.
Chuang TH, et al: Pulmonary embolization from vascular stump thrombosis following pneumonectomy. Ann Thorac Surg 2:290, 1966.
Ciriaco P, et al: Supraventricular arrhythmia following lung resection for non small cell lung cancer and its treatment with amiodarone. Eur J Cardiothorac Surg 18:12, 2000.
Cosgrove DM III: Closure of postpneumonectomy bronchopleural fistula. Presented at the Clinical Congress, American College of Surgeons, Thoracic Surgery Postgraduate Course, Chicago, IL, October 15, 1985.
Crystal E, et al: Interventions on prevention of postoperative atrial fibrillation in patients undergoing heart surgery: a meta-analysis. Circulation 106:75, 2002.
Curtis JJ, et al: Incidence and predictors of supraventricular dysrhythmias after pulmonary resection. Ann Thorac Surg 66:1766, 1998.
Cybulsky IJ, et al: Prognostic significance of computed tomography in resected N2 lung cancer. Ann Thorac Surg 54:533, 1992.
Daly BDT: Late results. Chest Surg Clin N Am 9:675, 1999.
Dartevelle P, Macchiarini P: Techniques of pneumonectomy. Sleeve pneumonectomy. Chest Surg Clin N Am 9:407, 1999.
Da Silva VF, et al: Subarachnoid-pleural fistula complicating thoracotomy: case report and review of the literature. Neurosurgery 20:806, 1987.
P.583
De Decker K, Jorens PG, Van Schil P: Cardiac complications after noncardiac thoracic surgery: an evidence-based current review. Ann Thorac Surg 75:1340, 2003.
De Hoyos A, Sundaresan S: Thoracic empyema. Surg Clin North Am 82: 643, 2002.
Deneffe G, et al: Surgical treatment of bronchogenic carcinoma: a retrospective study of 720 thoracotomies. Ann Thorac Surg 45:380, 1988.
Deschamps C, et al: Early complications: bronchopleural fistula and empyema. Chest Surg Clin N Am 9:587, 1999.
Deschamps C, et al: Empyema and bronchopleural fistula after pneumonectomy: factors affecting incidence. Ann Thorac Surg 72:243, 2001.
Deslauriers J: Indications for completion pneumonectomy. Ann Thorac Surg 46:133, 1988.
Deslauriers J, Faber LP (eds): Pneumonectomy, Parts I and II. Chest Surg Clin N Am 9(2 3), 1999.
Deslauriers J, Aucoin A, Gregoire J: Postpneumonectomy pulmonary edema. Chest Surg Clin N Am 8:611, 1998.
Deslauriers J, Aucoin A, Gregoire J: Early complications: postpneumonectomy edema. Chest Surg Clin N Am 9:565, 1999.
Deslauriers J, et al: Current operative morbidity associated with elective surgical resection for lung cancer. Can J Surg 32:335, 1989.
Duque JL, et al: Early complications in the surgical treatment of lung cancer: a prospective, multicenter study. Grupo Cooperativo de Carcinoma Broncogenico de la Sociedad Espanola de Neumologia y Cirugia Toraica. Ann Thorac Surg 63:944, 1997.
Dyszkiewicz W, Pawlak K, Gasiorowski L: Early post-pneumonectomy complications in the elderly. Eur J Cardiothorac Surg 17:246, 2000.
Evans GH, Clark RJ: Management of life-threatening adult postpneumonectomy syndrome. Anaesthesia 50:148, 1995.
Evans JP: Post-pneumonectomy oesophageal fistula. Thorax 27:674, 1972.
Ferguson MK, Reeder LB, Mick R: Optimizing selection of patients for major lung resection. J Thorac Cardiovasc Surg 109:275, 1995.
Fleisher LA, Eagle KA: Lowering cardiac risk in noncardiac surgery. N Engl J Med 345:1677, 2001.
Flores RM, Murthy S, DeCamp MM Jr: Contralateral pulmonary artery stenosis after left pneumonectomy. Ann Thorac Surg 72:274, 2001.
Frantz PT, Battaglini JW: Subarachnoid-pleural fistula: unusual complication of thoracotomy. J Thorac Cardiovasc Surg 79:873, 1980.
Fujimoto T, et al: Completion pneumonectomy: current indications, complications and results. J Thorac Cardiovasc Surg 121:484, 2001.
Gharagozloo F, et al: Pleural space irrigation and modified Clagett procedure for the treatment of early postpneumonectomy empyema. J Thorac Cardiovasc Surg 116:943, 1998.
Ginsberg RJ, et al: Modern thirty-day operative mortality for surgical resections in lung cancer. J Thorac Cardiovasc Surg 86:654, 1983.
Ginsberg RJ, et al: Closure of chronic postpneumonectomy bronchopleural fistula using the transsternal transpericardial approach. Ann Thorac Surg 47:231, 1989.
Glover W, et al: Fibrin glue application through the fiberoptic bronchoscope: closure of bronchopleural fistulas. J Thorac Cardiovasc Surg 93:470, 1987.
Godart F, et al: Postpneumonectomy interatrial right-to-left shunt: successful percutaneous treatment. Ann Thorac Surg 64:834, 1997.
Gomez JR, et al: Tumor embolism after pneumonectomy for primary pulmonary neoplasia. Ann Vasc Surg 9:199, 1995.
Grillo HC, et al: Postpneumonectomy syndrome: diagnosis, management and results. Ann Thorac Surg 54:638, 1992.
Handy JR Jr, et al: Hospital readmission after pulmonary resection: prevalence, patterns and predisposing factors. Ann Thorac Surg 72:1855, 2001.
Harpole DH, et al: Prospective analysis of pneumonectomy: risk factors for major morbidity and cardiac dysrhythmias. Ann Thorac Surg 61: 977, 1996.
Harpole DH Jr, et al: Prognostic models of thirty-day mortality and morbidity after major pulmonary resection. J Thorac Cardiovasc Surg 117: 969, 1999.
Harvey JC, Erdman C, Beattie EJ: Pneumonectomy. Chest Surg Clin N Am 5:253, 1995.
Heitmiller RF: Prognostic significance of massive bronchogenic tumor embolus. Ann Thorac Surg 53:153, 1992.
Herzog H, et al: Surgical therapy for expiratory collapse of the trachea and large bronchi. In Grillo HC, Eschapasse H (eds): International Trends in General Thoracic Surgery. Vol. 2. Philadelphia: WB Saunders, 1987, p. 74.
Hollaus PH, et al: Natural history of bronchopleural fistula after pneumonectomy: a review of 96 cases. Ann Thorac Surg 63:1391, 1997.
Hollaus PH, et al: Endoscopic treatment of postoperative bronchopleural fistula: experience with 45 cases. Ann Thorac Surg 66:923, 1998.
Hovaguimian H, et al: Pulmonary venous thrombosis following bilobectomy. Chest 99:1515, 1991.
Ishida T, et al: Long-term results of operation for non small cell lung cancer in the elderly. Ann Thorac Surg 50:919, 1990.
Jack GD: Bronchial closure. Thorax 20:8, 1965.
Jakobsen CJ, et al: Perioperative metoprolol reduces the frequency of atrial fibrillation after thoracotomy for lung resection. J Cardiothorac Vasc Anesthesia 11:746, 1997.
Jansen JP, et al: Postpneumonectomy syndrome in adulthood. Surgical correction using an expandable prosthesis. Chest 101:1167, 1992.
Jensik RJ: The extent of resection for localized lung cancer: segmental resection. In Kittle CF (ed): Current Controversies in Thoracic Surgery. Philadelphia, WB Saunders, 1986.
Jessen C, Sharma P: Use of fibrin glue in thoracic surgery. Ann Thorac Surg 39:521, 1985.
Johnstone DW: Postoperative chylothorax. Chest Surg Clin N Am 12:597, 2002.
Kadri MA, Dussek JE: Survival and prognosis following resection of primary non small cell bronchogenic carcinoma. Eur J Cardiothorac Surg 5:132, 1991.
Karwande SV, Wolcott MW, Gay WA: Postpneumonectomy tension chylothorax. Ann Thorac Surg 42:585, 1986.
Kaushik S, et al: Acute pulmonary toxicity after low-dose amiodarone therapy. Ann Thorac Surg 72:1760, 2001.
Keagy BA, et al: Elective pulmonary lobectomy: factors associated with morbidity and operative mortality. Ann Thorac Surg 40:349, 1985.
Kearney DJ, et al: Assessment of operative risk in patients undergoing lung resection. Importance of predicted pulmonary function. Chest 105: 753, 1994.
Kelly MV 2nd, Kyger R, Miller WC: Postoperative lobar torsion and gangrene. Thorax 32:501, 1977.
Kelly RF, Hunter DW, Maddaus MA: Postpneumonectomy syndrome after left pneumonectomy. Ann Thorac Surg 71:701, 2001.
Khan MG: Angina. In Khan MG, Lynch JP III (eds): Cardiac and Pulmonary Management. Philadelphia: Lea & Febiger, 1993, p. 57.
Khargi K, et al: Hemorrhage due to inflammatory erosion of the pulmonary artery stump in postpneumonectomy bronchopleural fistula. Ann Thorac Surg 56:357, 1993.
Kirschner PA: Provocative clamping and removal of chest tubes despite persistent air leak [Letter]. Ann Thorac Surg 53:740, 1992.
Klemperer J, Ginsberg RJ: Morbidity and mortality after pneumonectomy. Chest Surg Clin N Am 9:515, 1999.
Knott-Craig CJ, et al: Improved results in the management of surgical candidates with lung cancer. Ann Thorac Surg 63:1405, 1997.
Korst RJ, Humphrey CB: Complete lobar collapse following pulmonary lobectomy. Its incidence, predisposing factors and clinical ramifications. Chest 111:1285, 1997.
Krowka MJ, et al: Cardiac dysrhythmia following pneumonectomy. Clinical correlates and prognostic significance. Chest 91:490, 1987.
Kucich VA, Villarreal JR, Schwartz DB: Left upper lobe torsion following lower lobe resection. Early recognition of a rare complication. Chest 95: 1146, 1989.
Kutlu CA, et al: Acute lung injury and acute respiratory distress syndrome after pulmonary resection. Ann Thorac Surg 69:376, 2000.
Landreneau RJ, et al: Video-assisted thoracoscopic surgery: basic technical concepts and intercostal approach strategies. Ann Thorac Surg 54: 800, 1992.
Lanza LA, et al: Low-dose oral amiodarone prophylaxis reduces atrial fibrillation after pulmonary resection. Ann Thorac Surg 75:223, 2003.
Lausberg HF, et al: Bronchial and bronchovascular sleeve resection for treatment of central lung tumors. Ann Thorac Surg 70:367, 2000.
Le Pimpec-Barthes F, et al: Chylothorax complicating pulmonary resection. Ann Thorac Surg 73:1714, 2002.
Lewis JW Jr, et al: Right heart function and prediction of respiratory morbidity in patients undergoing pneumonectomy with moderately severe cardiopulmonary dysfunction. J Thorac Cardiovasc Surg 108: 169, 1994.
Licker M, et al: Perioperative mortality and major cardio-pulmonary complications after lung surgery for non small cell carcinoma. Eur J Cardiothorac Surg 15:314, 1999.
Livaudais W Jr, Cavanaugh DG, Geer TM: Rapid postoperative thoracotomy for torsion of the left lower lobe: case report. Mil Med 145:698, 1980.
P.584
Maassen W: The transsternal and transpericardial approach for surgical treatment of fistulas of the main bronchus after pneumonectomy. Thorax Chir Vask Chir 23:257, 1975.
Maeda M, et al: Statistical survey of tracheobronchoplasty in Japan. J Thorac Cardiovasc Surg 97:402, 1989.
Maier HC, Gould WI: Agenesis of the lung with vascular compression of the tracheobronchial tree. J Pediatr 43:38, 1953.
Mansour KA, Malone CE, Craver JM: Left atrial tumor embolization during pulmonary resection: review of the literature and report of two cases. Ann Thorac Surg 46:455, 1988.
Martin J, et al: Morbidity and mortality after neoadjuvant therapy for lung cancer: the risks of right pneumonectomy. Ann Thorac Surg 72:1149, 2001.
Martini N, et al: The extent of resection for localized lung cancer: lobectomy. In Kittle CF (ed): Current Controversies in Thoracic Surgery. Philadelphia: WB Saunders, 1986.
Massard G, Wihlm J: Early complications: esophagopleural fistula. Chest Surg Clin N Am 9:617, 1999.
Massard G, et al: Pleuropulmonary aspergilloma: clinical spectrum and results of surgical treatment. Ann Thorac Surg 54:1159, 1992.
Massard G, et al: Esophagopleural fistula: an early and long-term complication after pneumonectomy. Ann Thorac Surg 58:1437, 1994.
Mathisen DJ, Grillo HC: Carinal resection for bronchogenic carcinoma. J Thorac Cardiovasc Surg 102:16, 1991.
Mathisen DJ, et al: Inhaled nitric oxide for adult respiratory distress syndrome following pulmonary resection. Ann Thorac Surg 66:1894, 1998.
Mathru M, et al: Permeability pulmonary edema following lung resection. Chest 98:1216, 1990.
McGovern EM, et al: Completion pneumonectomy: indications, complications, and results. Ann Thorac Surg 46:141, 1988.
McKenna RJ Jr, et al: Use of the Heimlich valve to shorten hospital stay after lung reduction surgery for emphysema. Ann Thorac Surg 61:1115, 1996.
McKenna RJ Jr, et al: Video-assisted thoracic surgery (VATS) lobectomy for bronchogenic carcinoma. Semin Thorac Cardiovasc Surg 10:321, 1998.
Mehran RJ, Deslauriers J: Late complications: postpneumonectomy syndrome. Chest Surg Clin N Am 9:655, 1999.
Melendez JA, Barrera R: Predictive respiratory complication quotient predicts pulmonary complications in thoracic surgical patients. Ann Thorac Surg 66:220, 1998.
Melendez JA, Carlon VA: Cardiopulmonary risk index does not predict complications after thoracic surgery. Chest 114:69, 1998.
Mercho N, et al: Right-to-left interatrial shunt causing platypnea after pneumonectomy. Chest 105:931, 1994.
Miller JI: Single-stage complete muscle flap closure of the postpneumonectomy empyema space: a new method and possible solution to a disturbing complication. Ann Thorac Surg 38:227, 1984.
Miller JI Jr: Physiologic evaluation of pulmonary function in the candidate for lung resection. J Thorac Cardiovasc Surg 105:347, 1993.
Miller JI Jr: Acute and delayed space problems following pulmonary resection. Chest Surg Clin N Am 6:615, 1996.
Miller JI Jr: Introduction: management of bronchopleural fistula. Semin Thorac Cardiovasc Surg 13:2, 2001.
Mitsudomi T, et al: Postoperative complications after pneumonectomy for treatment of lung cancer: multivariate analysis. J Surg Oncol 61:218, 1996.
Mizushima Y, et al: Survival and prognosis after pneumonectomy for lung cancer in the elderly. Ann Thorac Surg 64:193, 1997.
Morice RC, et al: Exercise testing in the evaluation of patients at high risk for complications from lung resection. Chest 101:356, 1992.
Morita R, et al: A case of postoperative chylothorax successfully treated by thoracoscopic fibrin gluing. Nippon Kyobu Geka Gakkai Zasshi 38: 2465, 1990.
Moser NJ, et al: Management of postpneumonectomy syndrome with a bronchoscopically placed endobronchial stent. South Med J 87:1156, 1994.
Muysoms FE, et al: Completion pneumonectomy: analysis of operative mortality and survival. Ann Thorac Surg 66:1165, 1998.
Nagasaki F, Flehinger BJ, Martini N: Complications of surgery in the treatment of carcinoma of the lung. Chest 82:25, 1982.
Nakagawa M, et al: Relationship between the duration of the preoperative smoke-free period and the incidence of postoperative pulmonary complications after pulmonary surgery. Chest 120:705, 2001.
Nakamura T, et al: Cardiac arrhythmias following lobectomy in elderly patients. J Jpn Assoc Chest Surg 11:500, 1997.
Ngan H, Fok M, Wong J: The role of lymphography in chylothorax following thoracic surgery. Br J Radiol 61:1032, 1988.
Nissen R: Tracheoplastie zur Beseitigung der Erschalffung des membranosen Teils der Intrathorakalen. Luftrohre Schweiz Med Wochenschr 84:219, 1954.
Nomori H, et al: Retained sponge after thoracotomy that mimicked aspergilloma. Ann Thorac Surg 61:1535, 1996.
Ohri S, Siddiqui AA, Townsend ER: Cardiac torsion after lobectomy with partial pericardiectomy. Ann Thorac Surg 53:703, 1992.
Okada M, et al: Right ventricular dysfunction after major pulmonary resection. J Thorac Cardiovasc Surg 108:503, 1994.
Okada M, et al: Survival related to lymph node involvement in lung cancer after sleeve lobectomy compared with pneumonectomy. J Thorac Cardiovasc Surg 119:814, 2000.
O'Meara JB, Slade PR: Disappearance of fluid from the postpneumonectomy space. J Thorac Cardiovasc Surg 67:621, 1974.
O'Neill PJ, et al: Intrathoracic fibrin sealant application using computed tomography fluoroscopy. Ann Thorac Surg 70:301, 2000.
Pagni S, Federico JA, Ponn RB: Pulmonary resection for lung cancer in octogenarians. Ann Thorac Surg 63:785, 1997.
Pagni S, et al: Pulmonary resection for malignancy in the elderly: is age still a risk factor? Eur J Cardiothorac Surg 14:40, 1998.
Pairolero PC, et al: Postpneumonectomy empyema: the role of intrathoracic muscle transposition. J Thorac Cardiovasc Surg 99:958, 1990.
Pass HI, et al: Surgically debulked malignant pleural mesothelioma: results and prognostic factors. Ann Surg Oncol 4:215, 1997.
Patel RL, Townsend ER, Fountain SW: Elective pneumonectomy: factors associated with morbidity and operative mortality. Ann Thorac Surg 54: 84, 1992.
Patel AM, Trastek VF, Coles DT: Gossypibomas mimicking echinococcal cyst disease of the lung. Chest 105:284, 1994.
Perelman MI: Late treatment of chronic bronchopleural fistula with long stump after pneumonectomy. In Eschapasse H, Grillo H (eds): International Trends in General Thoracic Surgery. Vol. 2. Philadelphia: WB Saunders, 1987.
Perelman MI, Ambatiello GP: Transpleuraler, transsternaler und kontralateraler Zugang bei Operationen wegen Bronchial fistel nach Pneumonectomie. Thorax Chir Vaskul Chir 18:45, 1970.
Perelman MI, Rymko LP, Ambatiello GP: Bronchopleural fistula: surgery after pneumonectomy. In Eschapasse H, Grillo H (eds): International Trends in General Thoracic Surgery. Vol. 2. Philadelphia: WB Saunders, 1987.
Peterffy A, Henze A: Haemorrhagic complications during pulmonary resection. A retrospective review of 1428 resections with 113 haemorrhagic episodes. Scand J Thorac Cardiovasc Surg 17:283, 1983.
Peters RM: Postpneumonectomy pulmonary edema. In Eschapasse H, Grillo H (eds): International Trends in General Thoracic Surgery. Vol. 2. Philadelphia: WB Saunders, 1987.
Pezzella AT, et al: Complications of general thoracic surgery. Curr Probl Surg 37:773, 2000.
Piccione W Jr, Faber LP: Management of complications related to pulmonary resection. In Waldhausen JA, Orringer MB (eds): Complications in Cardiothoracic Surgery. St. Louis: Mosby-Year Book, 1991, p. 336.
Pierce RJ, et al: Preoperative risk evaluation for lung cancer resection: predicted postoperative product as a predictor of surgical mortality. Am J Respir Crit Care Med 150:947, 1994.
Pollack IF, Pang P, Hall WA: Subarachnoid-pleural fistula and subarachnoid-mediastinal fistula. Neurosurgery 26:519, 1990.
Pomerantz M, et al: Surgical management of resistant mycobacterial tuberculosis and other mycobacterial pulmonary infections. Ann Thorac Surg 52:1108, 1991.
Ponn RB, Silverman HJ, Federico JA: Outpatient chest tube management. Ann Thorac Surg 64:1437, 1997.
Ponn RB, et al: Treatment of peripheral bronchopleural fistulas with endobronchial occlusion coils. Ann Thorac Surg 56:1343, 1993.
Porte HL, et al: Randomized controlled trial of a synthetic sealant for preventing alveolar air leaks after lobectomy. Ann Thorac Surg 71:1618, 2001.
Powell RW, Luck SR, Raffensperger JG: Pneumonectomy in infants and children: the use of a prosthesis to prevent mediastinal shift and its complications. J Pediatr Surg 14:231, 1979.
Puskas JD, et al: Treatment strategies for bronchopleural fistula. J Thorac Cardiovasc Surg 109:989, 1995.
P.585
Putnam JB Jr, et al: Predicted pulmonary function and survival after pneumonectomy for primary lung carcinoma. Ann Thorac Surg 49:909, 1990.
Quillin SP, Shackelford GD: Postpneumonectomy syndrome after left lung resection. Radiology 179:100, 1991.
Rao PS, et al: International experience with secundum atrial septal defect occlusion by the buttoned device. Am Heart J 128:1022, 1994.
Rasch DK, et al: Right pneumonectomy syndrome in infancy treated with an expandable prosthesis. Ann Thorac Surg 50:127, 1990.
Reed CE, Dorman BH, Spinale FG: Mechanisms of right ventricular dysfunction after pulmonary resection. Ann Thorac Surg 62:225, 1996.
Rendina EA, et al: Lung conservation techniques: bronchial sleeve resection and reconstruction of the pulmonary artery. Semin Surg Oncol 18:165, 2000.
Rice TW, Kirby T: Prolonged air leak. Chest Surg Clin N Am 2:803, 1992.
Rice TW, et al: Simultaneous occurrence of chylothorax and subarachnoid pleural fistula after thoracotomy. Can J Surg 30:256, 1987.
Riquet M, Hidden G, Debesse B: Les collaterales dur canal thoracique d'origine ganglio-pulmonaire etude anatomique et chylothorax apres chirurgie pulmonaire. Ann Chir Thorac Cardiovasc 43:646, 1989.
Ritchie AJ, Bowe P, Gibbons JRP: Prophylactic digitalization for thoracotomy: a reassessment. Ann Thorac Surg 50:86, 1990.
Ritchie AJ, Danton M, Gibbons JRP: Prophylactic digitalisation in pulmonary surgery. Thorax 47:41, 1992.
Rivas de Andres JJ, et al: Postsurgical pleurodesis with autologous blood in patients with persistent air leak. Ann Thorac Surg 70:270, 2000.
Riveron FA, et al: Silastic prosthesis plombage for right postpneumonectomy syndrome. Ann Thorac Surg 50:465, 1990.
Rocker GM, et al: Neutrophil degranulation and increased pulmonary capillary permeability following oesophagectomy: a model of early lung injury in man. Br J Surg 75:883, 1988.
Romano PS, Mark DH: Patient and hospital characteristics related to in-hospital mortality after lung cancer resection. Chest 101:1332, 1992.
Roviaro GC, et al: Tracheal sleeve pneumonectomy for bronchogenic carcinoma. J Thorac Cardiovasc Surg 107:13, 1994.
Roxburgh JC, Thompson J, Goldstraw P: Hospital mortality and long-term survival after pulmonary resection in the elderly. Ann Thorac Surg 51: 800, 1991.
Ruffini E, et al: Frequency and mortality of acute lung injury and acute respiratory distress syndrome after pulmonary resection for bronchogenic carcinoma. Eur J Cardiothorac Surg 20:30, 2001.
Rusch VW: Indications for pneumonectomy: extrapleural pneumonectomy. Chest Surg Clin N Am 9:327, 1999.
Samuels LE, Shaw PM, Blaum LC: Percutaneous technique for management of persistent airspace with prolonged air leak using fibrin glue. Chest 109:1653, 1996.
Sarsam MA, Moussali H: Technique of bronchial closure after pneumonectomy. J Thorac Cardiovasc Surg 98:220, 1989.
Sarsam MA, Rahman AN, Deiraniya AK: Postpneumonectomy chylothorax. Ann Thorac Surg 57:689, 1994.
Schnabel TG: Postural cyanosis and angina pectoris following pneumonectomy: relief by closure of an interatrial septal defect. J Thorac Surg 32:246, 1956.
Senderoff E, Kirschner A: Massive tumor embolism during pulmonary surgery. J Thorac Cardiovasc Surg 44:528, 1962.
Shah R, et al: Self-expanding tracheobronchial stents in the management of major airway problems. J Cardiovasc Surg (Torino) 36:343,1995.
Shama DM, Odell JA: Esophagopleural fistula after pneumonectomy for inflammatory disease. J Thorac Cardiovasc Surg 89:77, 1985.
Shamji FM, et al: Postpneumonectomy syndrome with ipsilateral aortic arch after left pneumonectomy. Ann Thorac Surg 62:1627, 1996.
Shapira OM, Shahian DM: Postpneumonectomy pulmonary edema. Ann Thorac Surg 56:190, 1993.
Shephard JA, et al: Right-pneumonectomy syndrome: radiographic findings, and CT correlation. Radiology 161:661, 1986.
Shields TW, Ujiki GT: Digitalization for prevention of arrhythmias following pulmonary surgery. Surg Gynecol Obstet 126:743, 1968.
Shields TW, et al: Persistent pleural air space following resection for pulmonary tuberculosis. J Thorac Cardiovasc Surg 38:523, 1959.
Shimada J, et al: Chronic hemorrhagic empyema developing thirty-three years after right pneumonectomy. A case report. J Jpn Assoc Thorac Surg 39:1204, 1991.
Shiraishi Y, et al: Morbidity and mortality after 94 extrapleural pneumonectomies for empyema. Ann Thorac Surg 70:1202, 2000.
Shirakusa T, et al: Surgical treatment of pulmonary aspergilloma and Aspergillus empyema. Ann Thorac Surg 48:779, 1989.
Short HD: Paraplegia associated with the use of oxidized cellulose in posterolateral thoracotomy incisions. Ann Thorac Surg 50:288, 1990.
Simpson L: Chylothorax in adults: pathophysiology and management. In Deslauriers J, Lacquet LK (eds): Thoracic Surgery: Surgical Management of Pleural Diseases. St. Louis: CV Mosby, 1990.
Smeenk FW, Postmus PE: Interatrial right to left shunting developing after pulmonary resection in the absence of elevated right sided heart pressures. Review of the literature. Chest 103:528, 1993.
Spencer DD, de la Garza LJ, Walker WA: Multiple tumor emboli after pneumonectomy. Ann Thorac Surg 55:169, 1993.
Spizarny DL, Shetty PC, Lewis JW Jr: Lung torsion: preoperative diagnosis with angiography and computed tomography. J Thorac Imaging 13:42, 1998.
Stenzl W, et al: Treatment of postsurgical chylothorax with fibrin glue. Thorac Cardiovasc Surg 31:35, 1983.
Stephan F, et al: Pulmonary complications following lung resection. A comprehensive analysis of incidence and possible risk factors. Chest 118:1263, 2000.
Sugarbaker DJ, et al: Extrapleural pneumonectomy in the multimodality therapy of malignant pleural mesothelioma: results in 120 consecutive patients. Ann Surg 224:288, 1996.
Sugimoto S, et al: Anatomy of inferior pulmonary vein should be clarified in lower lobectomy. Ann Thorac Surg 66:1799, 1998.
Suter M, et al: Thoracoscopic pleurodesis for prolonged (or intractable) air leak after lung resection. Eur J Cardiothorac Surg 12:160, 1997.
Swartz DE, et al: Perioperative mortality after pneumonectomy: analysis of risk factors and review of the literature. Can J Surg 40:437, 1997.
Szarnicki R, et al: Tracheal compression by the aortic arch following right pneumonectomy in infancy. Ann Thorac Surg 25:231, 1978.
Taber RE: Massive systemic tumor embolism during pulmonary surgery. Ann Surg 44:528, 1961.
Takahashi T, et al: Clot in the pulmonary artery after pneumonectomy [Letter]. AJR Am J Roentgenol 161:1110, 1993.
Tedder M, et al: Current morbidity, mortality, and survival after bronchoplastic procedures for malignancy. Ann Thorac Surg 54:387, 1992.
Terzi A, et al: Chylothorax after pleuro-pulmonary surgery: a rare but unavoidable complication. Thorac Cardiovasc Surgeon 42:81, 1994.
Terzi A, et al: Completion pneumonectomy: experience with 47 cases. Thorac Cardiovasc Surg 43:52, 1995.
Terzi A, et al: Prevention of atrial tachyarrhythmias after non-cardiac surgery by infusion of magnesium sulfate. Thorac Cardiovasc Surg 44:300, 1996.
Thistlewaite PA, et al: Ablation of persistent air leaks after thoracic procedures with fibrin sealant. Ann Thorac Surg 67:575, 1999.
Thomas P, et al: Clinical patterns and trends of outcome of elderly patients with bronchogenic carcinoma. Eur J Cardiothorac Surg 13:266, 1998.
Till AS, Fairburn EA: Massive neoplastic embolism. Br J Surg 35:86, 1947.
Toloza EM, Harpole DH Jr: Intraoperative techniques to prevent air leaks. Chest Surg Clin N Am 12:489, 2002.
Trastek VF: Invited commentary on Hollaus PH, et al: Natural history of bronchopleural fistula after pneumonectomy: a review of 96 cases. Ann Thorac Surg 63:1391, 1997.
Trastek VF, et al: Unusual complications of pulmonary resection. Chest Surg Clin N Am 2:853, 1992.
Tronc F, et al: Long term results of sleeve lobectomy for lung cancer. Eur J Cardiothorac Surg 17:550, 2000.
Tsuchiya R, et al: Resection of tracheal carina for lung cancer: procedure, complications, and mortality. J Thorac Cardiovasc Surg 99:779, 1990.
Turnage WS, Lunn JJ: Postpneumonectomy pulmonary edema. A retrospective analysis of associated variables. Chest 103:1646, 1993.
Vallieres E: Management of empyema after lung resections. Chest Surg Clin N Am 12:571, 2002.
Vallieres E, Shamji FM, Todd TR: Postpneumonectomy chylothorax. Ann Thorac Surg 55:1006, 1993.
Van den Bosch JM, et al: Postpneumonectomy oesophagopleural fistula. Thorax 35:865, 1980.
van der Werf YD, et al: Postpneumonectomy pulmonary edema. A retrospective analysis of incidence and possible risk factors. Chest 111:1278, 1997.
Van Leuven M, Clayman JA, Snow N: Bronchial obstruction after upper lobectomy: kinked bronchus relieved by stenting. Ann Thorac Surg 68: 235, 1999.
P.586
Van Mieghem W, et al: Amiodarone and the development of ARDS after lung surgery. Chest 105:1642, 1994.
Van Mieghem W, et al: Verapamil as prophylactic treatment of atrial fibrillation after lung operations. Ann Thorac Surg 61:1083, 1996.
Verheijen-Breemhaar L, et al: Postpneumonectomy pulmonary oedema. Thorax 45:323, 1988.
Veronesi G, et al: Cardiac dislocation after extended pneumonectomy with pericardioplasty. Eur J Cardiothorac Surg 19:89, 2001.
Vester SR, et al: Bronchopleural fistula after stapled closure of the bronchus. Ann Thorac Surg 52:1253, 1991.
Vogt-Moykopf I: Contralateral pneumothorax occurring after pulmonary surgery. In Deslauriers J, Lacquet LK (eds): Thoracic Surgery: Surgical Management of Pleural Diseases. St. Louis: CV Mosby, 1990, p. 158.
von Knorring J, et al: Cardiac arrhythmias and myocardial ischemia after thoracotomy for lung cancer. Ann Thorac Surg 53:642, 1992.
Wada H, et al: Thirty-day operative mortality for thoracotomy in lung cancer. J Thorac Cardiovasc Surg 115:70, 1998.
Wahi R, et al: Determinants of perioperative morbidity and mortality after pneumonectomy. Ann Thorac Surg 48:33, 1989.
Walker WE: Paraplegia associated with thoracotomy. Ann Thorac Surg 50: 178, 1990.
Waller DA, et al: Noncardiogenic pulmonary edema complicating lung resection. Ann Thorac Surg 55:140, 1993.
Waller DA, et al: Pulmonary endothelial permeability changes after major lung resections. Ann Thorac Surg 61:1435, 1996.
Wang J, et al: Assessment of pulmonary complications after lung resection. Ann Thorac Surg 67:1444, 1999.
Warren WH: Surgical techniques in the dissection and reconstruction of the pulmonary artery. Chest Surg Clin N Am 5:333, 1995.
Wasserman K, et al: Post-pneumonectomy syndrome. Surgical correction using silastic implants. Chest 75:78, 1979.
Wheat MW Jr, Burford TH: Digitalis in surgery. J Thorac Cardiovasc Surg 41:162, 1961.
White CM, et al: A comparison of two individual amiodarone regimens to placebo in open heart surgery patients. Ann Thorac Surg 74:69, 2002.
Whyte RI, Starkey TD, Orringer MB: Tumor emboli from lung neoplasms involving the pulmonary vein. J Thorac Cardiovasc Surg 104:421, 1992.
Wong PS, Goldstraw P: Pulmonary torsion: a questionnaire survey and a survey of the literature. Ann Thorac Surg 54:286, 1992.
Wright CD, et al: Postpneumonectomy bronchopleural fistula after sutured closure: incidence, risk factors and management. J Thorac Cardiovasc Surg 112:1367, 1996.
Wright CD, et al: Pulmonary lobectomy patient care pathway: a model to contain cost and maintain quality. Ann Thorac Surg 64:299, 1997.
Yashar J, et al: Preoperative chemotherapy and radiation therapy for stage IIIa carcinoma of the lung. Ann Thorac Surg 53:445, 1992.
Zeldin RA, et al: Postpneumonectomy pulmonary edema. J Thorac Cardiovasc Surg 87:359, 1984.
Ziomek S, et al: Thromboembolism in patients undergoing thoracotomy. Ann Thorac Surg 56:223, 1993.
Zueger O, et al: Dyspnea after pneumonectomy: the result of an atrial septal defect. Ann Thorac Surg 63:1451, 1997.
Reading References
Amar D, et al: Relationship of early postoperative dysrhythmias and long-term outcome after resection of non small cell lung cancer. Chest 110:437, 1996.
Pairolero PC, Payne WS: Postoperative care and complications in the thoracic surgical patient. In Glenn WWL, et al. (eds): Thoracic and Cardiovascular Surgery. 4th Ed. Norwalk, CT: Appleton-Century-Crofts, 1983, p. 338.
EAN: 2147483647
Pages: 203