31 - Renovascular Hypertension
Authors: Macfarlane, Michael T.
Title: Urology, 4th Edition
Copyright 2006 Lippincott Williams & Wilkins
> Table of Contents > Part Two - Selected Topics > Chapter 31 - Renovascular Hypertension
Chapter 31
Renovascular Hypertension
In approximately 5% to 10% of patients with hypertension, the disorder has a curable etiology, of which renovascular disease is the most common. It is important to identify this small group because these are often the most difficult hypertensive patients to manage medically and because their renal lesions are usually progressive and can lead to significant renal damage.
Mechanisms of Renovascular Hypertension
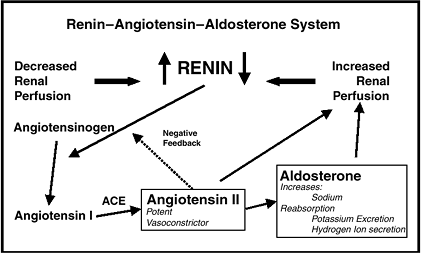
The preponderance of experimental data suggests that the mechanism of hypertension in renovascular disease is produced by stimulation of the renin angiotensin system.
 |
No Caption Available |
Only renal artery stenosis of a critical degree (>70%) will result in a functionally significant reduction in renal blood flow, thereby stimulating increased renin secretion. Hypertension results from the direct vasoconstrictor effect of angiotensin II and the increased vascular volume secondary to sodium retention by aldosterone.
P.226
Pathology
The major pathologic lesions producing renal artery narrowing are atherosclerosis (70%) and fibromuscular disease (30%).
Atherosclerosis
Atherosclerotic lesions cause most cases of renovascular hypertension (RVH) and usually involve the orifice and proximal 2 cm of the renal artery (i.e., near the aorta). Manifestations of generalized atherosclerosis involving the abdominal aorta and coronary, cerebral, and peripheral vasculature are usually evident.
Medial Fibroplasia
Medial fibroplasia is the second most common cause of RVH. It occurs characteristically in females aged 20 to 50 years and produces a typical multifocal string of beads pattern on angiography that starts in the midrenal artery and often extends into peripheral branches. Hemorrhage and dissection are rare. Correction is indicated in younger individuals.
Perimedial Fibroplasia
Perimedial fibroplasia is a progressive fibrous disease of young female patients that occurs only in the renal artery. It results in an irregular, severely stenotic lesion that often appears beaded on angiography. Surgical correction is indicated.
Intimal Fibroplasia
Intimal fibroplasia is a progressive disease that generally occurs in children or young adults, involves the proximal or middle portion of the artery, and often dissects. These lesions should be surgically corrected.
Workup
History
Disease onset before age 30 years and no family history of hypertension should suggest a renovascular etiology. A history of severe
P.227
hypertension, headaches, or difficult medical management also is common. Patients may give a history of angina, congestive heart failure, cerebrovascular accidents, or intermittent claudication.
Factors that suggest a renovascular etiology include the following:
Onset before age 30 years
Sudden development or worsening of hypertension at any age
Accelerated or malignant hypertension
Hypertension refractory to appropriate three-drug regimen
Extensive atherosclerotic disease
Impaired renal function associated with hypertension or use of an angiotensin-converting enzyme inhibitor (ACEI)
A continuous (systolic/diastolic) abdominal bruit
A unilaterally small kidney
Hypokalemia suggesting aldosterone hypersecretion
Physical Examination
Hypertension is defined as blood pressure of greater than 160/90 mm Hg in patients younger than 40 years and greater than 160/95 mm Hg in patients older than 40 years on three separate determinations. Check for retinopathy and abdominal or carotid bruits. Hypokalemia in the absence of diuretic therapy is highly suggestive; however, it occurs in fewer than 20% of patients.
Peripheral Plasma Renin Activity
A plasma renin activity (PRA) screening test must be performed in a highly standardized fashion because it is otherwise subject to many uncontrolled variables. Antihypertensive agents (except for -blockers) should be discontinued at least 2 weeks before PRA screening.
![]() Screening Plasma Renin Activity
Screening Plasma Renin Activity
Measurement of peripheral PRA indexed to sodium excretion in a 24-hour urine sample is useful for identifying abnormally high renin secretion. The blood sample for PRA should be taken at 12 noon after 4 hours of ambulation. A low peripheral PRA is strong evidence against renal arterial disease.
![]() Captopril Plasma Renin Activity Test (Captopril Challenge)
Captopril Plasma Renin Activity Test (Captopril Challenge)
Captopril is an ACE inhibitor, blocking the conversion of AI to AII. In the captopril-PRA test, peripheral PRA is measured before and 1 hour after taking 25 mg captopril orally (onset of action is
P.228
10 15 minutes). Angiotensin blockade results in a marked increase in PRA and decrease in blood pressure in patients with RVH.
Rapid-Sequence Intravenous Urography
A delayed calyceal appearance time on the side with a lesion during a rapid-sequence intravenous urogram has been used to screen for patients with potential renovascular disease. However, this has been shown to have a 10% false-positive rate among patients with essential hypertension and would therefore result in incorrectly identifying an unacceptably high number of patients.
Radionuclide Renography with Angiotensin-Converting Enzyme Inhibitor
The captopril renogram has improved sensitivity and specificity over a standard renogram in identifying RVH. The patient is given 25 mg captopril PO; 1 hour later, the patient is scanned for 20 to 30 minutes after intravenous (IV) MAG3. A delay to peak activity of the scan is consistent with RVH. A repeated MAG3 scan should be performed if the ACEI renogram is abnormal.
Doppler Ultrasound
The use of Doppler ultrasound to detect renal artery stenosis has been gaining acceptance. Measurement of peak systolic velocity and the renal/aortic ratio can correctly identify high-grade renal artery stenosis. The test is technically difficult.
Renal Vein Renin Sampling
Renal vein renin (RVR) sampling is now rarely used to diagnose RVH but can be useful in localizing the more ischemic kidney in bilateral disease. RVR can demonstrate three different abnormalities.
![]() Renal Vein/Renin Ratios
Renal Vein/Renin Ratios
A renal vein/renin ratio of greater than 1.5:1 (i.e., renal vein PRA from stenotic side divided by renal vein PRA from normal side) generally predicts a correctable renal vascular lesion. This test has a false-negative rate of at least 15% and is subject to sampling error.
P.229
![]() Renin Suppression
Renin Suppression
Renin is suppressed in the contralateral, noninvolved renal vein (VPRA). The IVCPRA can substitute for the arterial PRA (APRA).
VPRA - IVCPRA = 0
![]() 50% Renin Increment
50% Renin Increment
A renal vein PRA (VPRA) increment of more than 50% on the involved side over arterial PRA (may substitute IVCPRA) indicates significant RVH (assuming unilateral disease).
![]()
Selective Arteriography
Selective renal arteriography is the gold standard for diagnosing renal artery disease. It is performed before surgical renal revascularization for a more detailed anatomic image. If percutaneous transluminal renal angioplasty is performed, angiography can be conducted at the same time.
Diagnosis
Criteria for Diagnosis of Renovascular Hypertension
Documented sustained, fixed, diastolic hypertension
Demonstration of renin hypersecretion (if possible)
Peripheral PRA indexed to sodium excretion or a captopril-PRA test
Captopril renography
Demonstration of a significant vascular lesion by angiography
Treatment
If a curable, functional renal artery lesion is found in younger patients, surgical management is the preferred choice. Medical management is unlikely to halt progression of the disease or the potential renal damage. Vigorous medical management should be attempted in older patients with atherosclerotic RVH. Medical management of hypertension is the preferred initial treatment for
P.230
a patient with medial fibroplasia. Percutaneous transluminal renal angioplasty and open surgical revascularization have both been shown to be highly successful forms of therapy. Angioplasty of the main renal artery has had excellent results in fibrous dysplasia. However, percutaneous transluminal renal angioplasty is generally unsuccessful in treating atheromatous lesions involving the ostium. Preoperative treatment of significant existing coronary or cerebrovascular occlusive disease should be considered.
EAN: 2147483647
Pages: 44