112 - Multimodality Therapy for Non-Small-Cell Lung Cancer
Editors: Shields, Thomas W.; LoCicero, Joseph; Ponn, Ronald B.; Rusch, Valerie W.
Title: General Thoracic Surgery, 6th Edition
Copyright 2005 Lippincott Williams & Wilkins
> Table of Contents > Volume II > The Esophagus > Section XXI - Operative Procedures in the Management of Esophageal Disease > Chapter 129 - Exposure of the Cervical Esophagus
Chapter 129
Exposure of the Cervical Esophagus
Jeffrey A. Hagen
Tom R. DeMeester
The first operations on the esophagus were performed on the cervical portion of the organ. In 1738, Goursand of France removed a foreign body from the cervical esophagus. In 1877, Billroth and Czerny first successfully reconstructed the cervical esophagus after resection of a malignant tumor. Today, exposure of the cervical esophagus is commonly required for closure of endoscopic perforations, cricopharyngeal myotomy for motility disorders, suspension or resection of pharyngeal diverticula, and esophagoenteric anastomosis after esophageal resections.
SURGICAL APPROACH
The cervical esophagus is best approached through an oblique incision in the left side of the neck, along the anterior border of the sternocleidomastoid muscle. The left side is chosen for three reasons. First, dissection in the neck is facilitated by the course of the esophagus, which extends slightly to the left side of the trachea. Second, the right recurrent laryngeal nerve lies farther from the esophageal wall than the left nerve and is thus less likely to be injured when encircling the esophagus from the left. Third, if there is an aberrant (nonrecurrent) nerve, it more commonly occurs on the right side. The anatomic relationships of the esophagus and other structures in the neck are discussed in Chapter 123.
Patients who are at risk for vocal cord paralysis should have the function of their cords evaluated before surgery. This includes patients with a history of previous thyroid or parathyroid surgery and those with esophageal cancer. This evaluation is accomplished easily by passing a fiberoptic bronchoscope through the anesthetized nose and into the nasopharynx, observing cord movement during speech.
The operation is performed with the patient in the supine position on the operating table. Once the patient is anesthetized, a rolled towel is placed transversely under the scapula to provide slight hyperextension of the neck. The patient's neck is kept straight. The table is placed in a reversed Trendelenburg's position to decrease venous congestion and soft tissue edema, which may interfere with postoperative ventilation. The upper chest is incorporated into the operative field because enlargement of the thoracic inlet may be required (Fig. 129-1).
The incision along the anterior border of the sternocleidomastoid muscle extends from the superior aspect of the thyroid cartilage to the suprasternal notch. The platysma is sharply incised, and hemostasis is obtained. The sternocleidomastoid muscle is retracted laterally, and the omohyoid muscle divided inferiorly as it courses anterior to the carotid sheath. The sternohyoid and sternothyroid muscles are divided at their sternal attachments. The middle thyroid vein is ligated as it enters the jugular vein. The carotid sheath and its contents are gently retracted laterally and the thyroid gland and trachea medially (Fig. 129-2). This step exposes the deeper structures of the neck. The inferior thyroid artery is ligated as it enters the field posterior to the common carotid artery.
The cervical esophagus lies along the vertebral bodies and longus colli muscle. The exposure, as seen by the surgeon, is shown in Fig. 129-3. Blunt dissection easily separates the posterior esophagus from the prevertebral fascia. The esophagus is mobilized anteriorly by identifying the left recurrent laryngeal nerve as it courses horizontally along the posterolateral wall of the trachea just above the tracheoesophageal groove (Fig. 129-3). The esophagus is separated from the trachea by sharp dissection in the tracheoesophageal groove just posterior to the recurrent nerve. Grasping the esophagus with broad-tipped (Russian) forceps and pulling it toward the surgeon can facilitate this dissection. Fine-tipped forceps should be avoided because they can damage the esophageal wall. With this maneuver, the right border of the esophagus can be visualized, and a right-angled clamp is passed around it (Fig. 129-4). Normally, there is sufficient space between the right recurrent laryngeal nerve and the right border of the esophagus to allow circumferential dissection without injury to this nerve. Not exposing the right border of the esophagus by
P.1972
lateral traction as described can result in damage to the esophageal wall or the right recurrent nerve when passing the clamp. The esophagus is encircled with a Penrose drain at a level just above the thoracic inlet to aid in its retraction (Fig. 129-5). The fibroareolar tissue between the esophagus and trachea is bluntly dissected down into the thoracic inlet as far as the finger can reach.
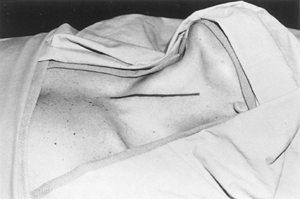 |
Fig. 129-1. Patient position for the left neck approach. |
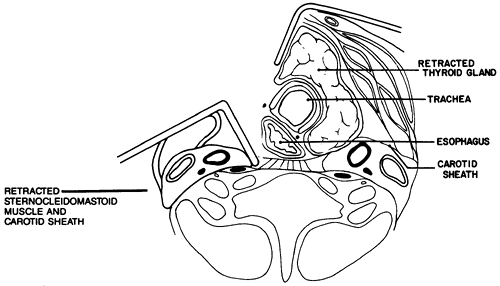 |
Fig. 129-2. Retraction to visualize the deep structures of the neck. |
 |
Fig. 129-3. Exposure as seen by the surgeon: thyroid gland (a), trachea (b), left recurrent laryngeal nerve (c), and esophagus (d). |
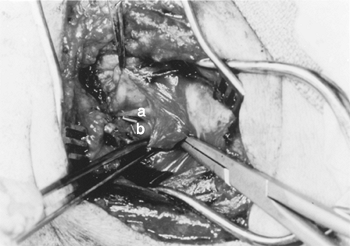 |
Fig. 129-4. Dissection of the right border of the esophagus: left recurrent laryngeal nerve (a), right-angled clamp around esophagus (b). |
The cervical esophagus is lifted from its bed between the levels of the cricopharyngeus muscle and the thoracic inlet and retracted into the wound. Injury to the thoracic
P.1973
duct can occur where it courses along the left posterolateral esophageal wall. It arches laterally behind the carotid sheath, below the inferior thyroid artery, before it enters the venous system; if necessary, ligation at this level may be performed without sequelae. Anterolateral retraction of the esophagus brings the posterior junction between the cricopharyngeus and inferior pharyngeal constrictor muscles into view to perform a cricomyotomy, pharyngoesophageal suspension or diverticulectomy, esophagoenteric anastomosis, or esophagostomy.
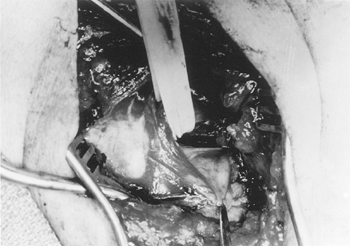 |
Fig. 129-5. Retraction of the esophagus into the wound with a Penrose drain. |
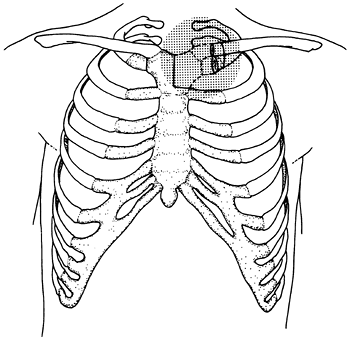 |
Fig. 129-6. Schematic diagram of the thoracic inlet area to be resected. |
EXPOSURE OF THE THORACIC INLET
The bony thoracic inlet measures 5 cm in the anteroposterior plane and 10 cm in the lateral plane. This size can compromise the passage of an esophageal substitute into the neck and may necessitate widening of the thoracic inlet. To do so requires resection of half of the manubrium, the head of the clavicle, and the medial segment of the first rib (Fig. 129-6).
The cervical skin incision is extended inferiorly over the sternal midline to the sternal angle, and the left pectoralis major muscle is reflected laterally to provide the necessary exposure. In this resection, the sternocleidomastoid and remnants of the strap muscles are reflected laterally, using the cautery to divide the muscular attachments at the bone. The clavicle is encircled with a right-angled clamp just lateral to its junction with the first rib, and a Gigli saw is passed to divide the clavicle. This maneuver must be carefully executed to avoid damaging the subclavian vein, which lies just beneath the head of the clavicle. The intercostal muscles in the first interspace are divided along the superior border of the second rib, again with the cautery, from the manubrium to the point of transection of the first rib. The surgeon must avoid damaging the internal mammary vessels, which lie on the pleural surface underneath the first rib. An L-shaped cut is made in the manubrium using the sternal saw along the line shown in Fig. 129-6. The manubrium is then retracted laterally along with the attached medial segment of the clavicle. The first rib is divided through the costal cartilage with a rib shear, completing the removal of the left manubrioclavicular joint.
In addition to widening the thoracic inlet, removal of the manubrioclavicular joint allows greater exposure of the esophagus in patients with an unusually short neck (Fig. 129-7).
P.1974
Before closure, the medial end of the remaining clavicle can be wired to the first rib if a cosmetic deformity appears likely. For most procedures, this approach to the cervical esophagus affords adequate exposure and permits safe dissection while avoiding injury to the recurrent laryngeal nerves and related structures.
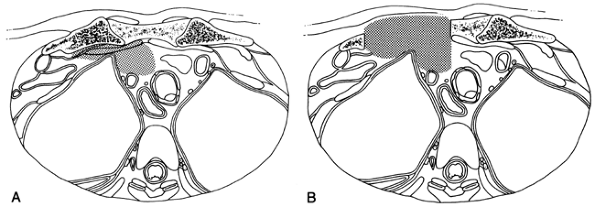 |
Fig. 129-7. Schematic diagram of the thoracic inlet as seen from above. |
REFERENCES
Czerny J: Neue Operationen: Vorl ufige Mitteilung. Zentralbl Chir 4:443, 1877.
Goursand. Cited by Meade RH: A History of Thoracic Surgery. Springfield, IL: Charles C Thomas, 1961, p. 567.
EAN: 2147483647
Pages: 203