35 - Vesicoureteral Reflux
Authors: Macfarlane, Michael T.
Title: Urology, 4th Edition
Copyright 2006 Lippincott Williams & Wilkins
> Table of Contents > Part Two - Selected Topics > Chapter 35 - Vesicoureteral Reflux
Chapter 35
Vesicoureteral Reflux
Vesicoureteral reflux (VUR) is the backward flow of urine from the bladder into the upper urinary tract. It is an abnormality that is associated with recurrent urinary tract infections and a particular form of renal damage known as reflux nephropathy. Because of its pathogenic role in reflux nephropathy, early recognition and eradication are essential. Primary reflux is the result of a congenital anomaly of the ureterovesical junction, whereas secondary reflux is the result of bladder-outlet obstruction and high intravesical pressures.
Pathophysiology
The most distal 13 mm of the ureter in adults lies intravesically (5 mm in neonates), including an intramural segment within the muscular wall of the bladder and a submucosal segment lying just beneath the bladder mucosa. This intravesical segment acts as a passive flap-valve mechanism to prevent reflux. The ratio between the length of the submucosal segment and the diameter of the ureter (normal, 4:1 or 5:1) is believed to be an important factor for normal function of the antireflux mechanism. Active peristalsis of the ureter also acts to prevent reflux.
Factors associated with VUR include the following:
A short submucosal tunnel
Lateral placement of the ureteral orifice
Abnormal configuration of ureteral orifice (e.g., stadium, horseshoe, and golf-hole orifices)
Infection
Severe bladder-outlet obstruction
Young age
Duplicated collecting systems (particularly from the more laterally placed orifice draining the lower pole)
P.258
Consequences of Reflux
Persistent VUR has been associated with renal damage, pyelonephritic scarring, and eventually impaired renal function, hypertension, and proteinuria. Reflux nephropathy refers to the radiologic changes of reflux including dilated calyces, renal parenchymal thinning, and scarring. Experimental and clinical data suggest that the combination of VUR and intrarenal reflux of infected urine into the collecting tubules of the nephron is necessary for renal damage to occur. In addition, the risk of renal scarring is greatest in children younger than 1 year and is uncommon after age 5 years. Early diagnosis and antibiotic treatment are important to prevent reflux nephropathy.
Megacystis Megaureter Syndrome
The megacystis megaureter syndrome is a condition characterized by a large-capacity, smooth, thin-walled bladder and massive vesicoureteral reflux in children. The massively dilated ureters and large-capacity bladder are a result of the constant recycling of large volumes of refluxed urine. The syndrome is not a problem of bladder-outlet obstruction or neurogenic bladder but is caused by massive primary vesicoureteral reflux. Therapy should be directed toward correction of the reflux.
Incidence
The incidence of VUR in the general population is estimated to be less than 2%. However, in children investigated because of urinary tract infection, the incidence is between 30% and 50% and decreases with advancing age. Siblings of patients with reflux are at a much greater risk of also having reflux.
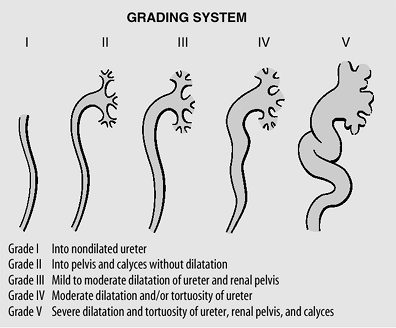
Grading System
The international grading system for reflux is based primarily on the radiographic appearance of the calyces on voiding cystourethrography (VCUG).
P.259
 |
No Caption Available |
Diagnosis
Urinalysis and culture should be performed early in the workup to exclude infection. The principal diagnostic test for evaluating VUR is the voiding cystourethrogram (VCUG). A nuclear cystogram is a good alternative and is more sensitive for picking up low-grade reflux; however, it does not give the anatomic detail of a VCUG and makes grading the reflux more difficult. A renal ultrasound has replaced the intravenous urography (IVU) for initial evaluation of the upper tracts in children. Dimethylsulfoxide (DMSO) renal scan is the study of choice for detecting pyelonephritis and cortical renal scarring. Cystoscopy should be performed at the time of a planned surgical repair only if indicated. Indications for cystoscopy include nonvisualization of the urethra on VCUG, uncertain ureteral location or anomaly, or localization of a paraureteral diverticulum. Urodynamic evaluation is indicated in children with secondary reflux.
Management
The management of patients is based on the observation that VUR has a natural tendency for spontaneous resolution. Surgical
P.260
correction can often be avoided by maintaining the patient on careful medical surveillance and continuous antibiotic prophylaxis to prevent secondary renal damage. The decision for medical versus surgical management is made after a careful diagnostic evaluation, with particular focus on the grade of reflux and age of the patient. Most grade I to III refluxes resolve spontaneously, as do some in grade IV. Grade V refluxes seldom resolve on their own. Reflux is more likely to resolve spontaneously in younger children regardless of grade.
Medical
Medical management consists of continuous low-dose antibiotic prophylaxis, regular urine cultures (every 3 months), and a yearly nuclear cystogram and renal ultrasound. Medical surveillance is appropriate for young children with mild-to-moderate grades of reflux (I III) and very young children with grade IV reflux. Ampicillin or amoxicillin is appropriate for children younger than 6 weeks, whereas trimethoprim sulfamethoxazole can be used after 6 weeks (mature biliary system). Grade V reflux also is managed medically in newborns until the child is old enough for surgical management.
Surgical
The success rate for antireflux procedures is greater than 90% in experienced hands. Indications for early surgical intervention follow.
Breakthrough infection despite antibiotic prophylaxis
Poor compliance with medical regimen
Progressive renal scarring with antibiotic prophylaxis
A refluxing orifice within a diverticulum
Severe reflux (grade IV or V)
EAN: 2147483647
Pages: 44