5 - Hypertension
Editors: Norris, John W.; Hachinski, Vladimir
Title: Stroke Prevention, 1st Edition
Copyright 2001 Oxford University Press
> Table of Contents > I - Primary Prevention > 5 - Hypertension
5
Hypertension
Philip A. Wolf
In 1973, Sir George Pickering wrote, It has been known for over a century that high arterial pressure lessens life expectancy and for half that time that in most patients the raised pressure and its consequences constitute disease (essential hypertension) .1 The prevalence of hypertension in the United States, defined by the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure as 2:140 mm Hg systolic or >90 diastolic, is high.2 Hypertension is present in 38% of persons aged 50 to 59 and 71% of those aged 80 and above, and it is a potent risk factor for the development of cardiovascular disease, particularly stroke.3 The relationship of hypertension to cardiovascular disease and specifically to apoplexy has long been known.4 While hypertension, cerebral hemorrhage, and the miliary aneurysms of Charcot and Bouchard have been closely related for more than 50 years, the link to ischemic stroke was made more recently.5,6 In fact, it has only been in the past 30 years that epidemiologic study has confirmed the role of elevated blood pressure in stroke.7 Hypertension is now known to be the most prevalent and powerful risk factor for stroke. It is also one of the most treatable conditions predisposing to stroke. What had been accepted as normal or average blood pressure (at a given age) is now considered to be much higher than ideal or optimal as far as stroke or cardiovascular disease risk is concerned. In older adults, particularly in persons above aged 65, in whom stroke occurs most frequently, the systolic component
P.94
of blood pressure has been shown to be no less important than the diastolic. Both systolic and diastolic pressures increase with age from childhood into middle adult years. By age 60, while the systolic pressure continues to rise, diastolic pressure has already reached a plateau and has begun to fall. With advancing age the diastolic continues to decline. In these older persons, aged 60 years and above, the level of risk cardiovascular disease, particularly stroke, is directly related to the level of systolic component, even in presence normal diastolic pressure.
The availability of a large number potent antihypertensive agents makes it possible to control virtually all hypertension. At the same time, a host of randomized clinical trials has shown such treatment is safe and effective. In the past, physicians were cautioned not to reduce blood pressure to normal levels for fear of precipitating stroke. Although some still advocate only moderate reduction of elevated pressure, most experts favor vigorous control of elevated blood pressure. With accumulating data, the target level has been gradually lowered. Now, a normal blood pressure of systolic < 140 mm Hg and diastolic <90 mm Hg (or lower) is considered to be the optimal blood pressure level for stroke prevention.2
Etiology Of Stroke
Unlike myocardial infarction, in which atherosclerosis of the coronary arteries is the underlying disease process, stroke is heterogenous; approximately 85% is due to infarction and the remainder to hemorrhage (half intracerebral half subarachnoid). With the exception of embolism from a cardiac source, most brain infarctions result from occlusion of large and small arteries to the brain. Hypertension is the most common potent risk factor for noncardioembolic ischemic stroke, and reduction of elevated blood pressure clearly prevents stroke regardless of infarct subtype. Much the observational data presented is based on the study of stroke in the general population sample at Framingham, Massachusetts. After 40 years of follow-up, stroke occurred in 718 persons 312 men and 406 in women. Incidence increased with age, approximately doubling in each successive decade above age 55. The most common type, accounting for approximately 60% of all stroke cases, has been called atherothrombotic brain infarction (ABI) and includes infarction resulting from large vessel atherothrombosis, lacunar infarction, and infarct of undetermined cause; embolic stroke from a known cardiac source was excluded.
Hypertension and Risk of Stroke
Among stroke risk factors, hypertension is clearly preeminent and is of importance for all stroke types, infarction as well hemorrhage. Using the systolic blood pressure levels in the most recent classification of hypertension (sixth report
P.95
of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure), the incidence nonembolic ischerm'c stroke in Framingham (ABI) was approximately 3 times greater in persons with definite hypertension ( 160/ 95 mm Hg) than in normotensives.7 Hypertension made a powerful and significant independent contribution to the incidence of ABI, even after age and other pertinent risk factors had been taken into account.
While the incidence of stroke is increased in hypertensives, dichotomy hypertensive and normotensive obscures the powerful, graded, direct relationship that exists between increasing level of blood pressure and increasing incidence of stroke. Using the systolic blood pressure categories of the JNC VI, stroke incidence increased with increasing levels of systolic pressure from normal (<130 mm Hg systolic) through high normal (130 139 systolic), mild hypertension (140 159 mm Hg systolic), moderate hypertension (160 179 Hg systolic), to severe hypertension ( 180 mm Hg systolic) (Figure 5.1).8 This was true in both sexes and in all age categories, including the elderly, aged 75 to 84 years. There was no evidence women tolerated hypertension better than men or that hypertension was unimportant in the elderly.
Furthermore, although the incidence rate of stroke was greatest at the upper levels of blood pressure, most stroke events occurred in persons with moderate
P.96
and normotensive diastolic blood pressure levels (Figure 5.2).9 Similarly, for systolic blood pressure, most stroke events occurred in persons at high normal, mild, and moderate hypertension levels. Among subjects aged 65 to 84 years, after 40 years of follow-up in Framingham, only 19% of strokes occurred those with severe hypertension (Figure 5.3).8 This was true for stroke due to hemorrhage or ischemia. More than two-thirds (69%) of all strokes occurred at systolic blood pressure levels between 130 mm Hg and 179 mm Hg.
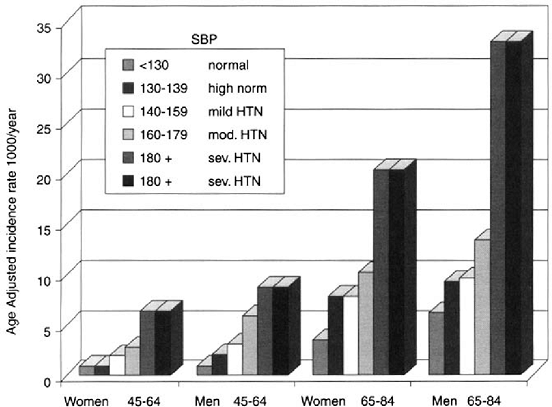 |
FIGURE 5.1. Stroke incidence by systolic blood pressure. Source: Joseph LN, Kase CS, Beiser AS, Wolf PA. Mild Blood Pressure Elevation and Stroke: The Framingham Study. Stroke 1998;29(1):277 . |
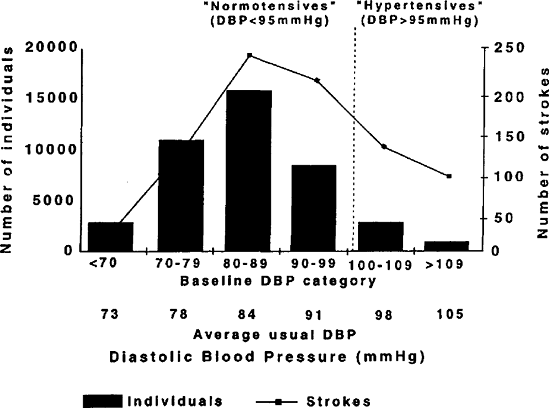 |
FIGURE 5.2. Absolute numbers of individuals and numbers strokes in seven prospective observational studies, subdivided by baseline diastolic blood pressure (DBF) category (405,000 individuals and 843 strokes in total). Approximately 80% of all occurred among the 95% of individuals classified as normotensive (usual DBF <95 mm Hg). Reprinted from MacMahon S, Rodgers A. The epidemiological association between blood pressure and stroke: implications for primary secondary prevention. Hyperten Res 1994;17(suppl l):523 532. Used by permission. |
Control of Hypertension and Stroke Prevention
Following clinical observation of patients with treated and untreated hypertension with prospective epidemiologic study, it is apparent that level of blood pressure is related to incidence of stroke, and this true for severe, moderate, mild hypertensives.10 Analysis of nine major prospective studies that included 420,000 individuals with a mean 10-year follow-up, the evidence clearly showed
P.97
a graded relationship between diastolic pressure and stroke coronary heart disease (CHD) incidence. There was no threshold level below which risk gradients were flat. For every 7.5 mm Hg diastolic pressure increase, there was a 46% increase in stroke incidence and a 29% increase CHD.10 Matching these findings derived from observational studies, an analysis of 14 treatment trials with a total of 37,000 hypertensive subjects showed reduction blood pressure in hypertensives reduced stroke incidence.11 The average diastolic blood pressure was reduced by 5.8 mm Hg and was associated with a corresponding reduction in stroke incidence of 42%. This observed reduction in stroke closely approximated what had been expected from the prospective observational studies. These findings should put to rest the concern that reduction of blood pressure in hypertensives precipitates stroke.
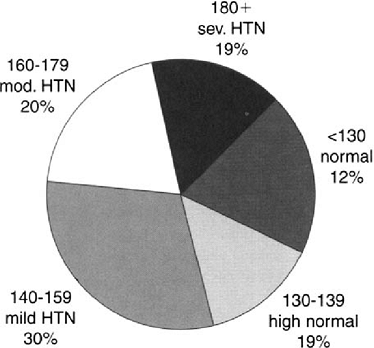 |
FIGURE 5.3. Percent of stroke by systolic blood pressure in subjects aged 65 84 years. Source: Joseph LN, Kase CS, Beiser AS, Wolf PA. Mild blood pressure elevation and stroke: The Framingham Study. Stroke 1998;29(1):277 . |
The 14% decrease in CHD rates was, however, considerably less than what might be expected. The explanation for the lesser effect on CHD incidence may relate to the adverse influence on electrolyte, glucose, and lipid metabolism of the thiazide diuretics that were the mainstay of treatment in most the trials and on the relatively lesser importance of hypertension to CHD (where blood lipid levels are key) than stroke. It is important to note that these substantial and significant reductions in stroke incidence occurred during the course of the trials. In these studies, the duration of blood pressure reduction was brief, from two to five years, suggesting interruption of a precipitating factor rather than interfering
P.98
with atherogenesis.11 Presumably, more prolonged blood pressure control would have both effects.
These trials were conducted in younger individuals, generally below the age of 65, and physicians were hesitant to reduce the blood pressures of elderly hypertensives. In the Swedish Trial in Old Patients with Hypertension (STOP), 1627 patients, aged 65 to 84 years (mean age 78 years), with elevated systolic (180 230 mm Hg) and diastolic (>90 mm Hg) blood pressure levels were randomized to treatment (thiazide diuretic and beta-blockers) placebo groups.12 Blood pressure was reduced, on average, 20/8 mm Hg. The trial stopped after 2.1 years, with a 47% reduction in stroke incidence. Cardiovascular events were 40% lower and deaths 43% lower in the treatment group. A number of other trials antihypertensives in elderly persons with mild diastolic hypertension also demonstrated the benefit and safety of this treatment in elderly persons.13,14,15
Isolated Systolic Hypertension
Traditionally, greater importance has been ascribed to the diastolic than the systolic blood pressure level, and while most clinical trials of hypertension treatment have classified subjects by the diastolic level, evidence for the ascendancy of the diastolic component of the blood pressure over systolic is lacking.16 With advancing age, systolic blood pressure continues to rise into the 70s, while diastolic pressures peak in the early 50s, then decline. In elderly, isolated systolic hypertension, that is, blood pressure levels >160 mm Hg systolic and <90 mm Hg diastolic, becomes highly prevalent: approximately 25% of persons above age 80 are affected.17 Although common, it is not innocuous. In Framingham, men 65 to 84 years of age with isolated systolic hypertension had approximately a 2-fold increased risk of stroke and women had a 1.5-fold increase in risk.18 Since isolated systolic hypertension is a consequence of reduced elasticity of the great arteries, it has been suggested that the arterial rigidity per se, rather than the systolic blood pressure, was responsible for the increased stroke rate. However, data from Framingham showed the risk of stroke was increased in persons with isolated systolic hypertension, even after the arterial rigidity was taken into account, and incidence of stroke rose in direct relation to the level systolic pressure.18 Furthermore, in two large clinical trials, reduction of increased systolic blood pressure levels was followed by a 40% to 50% reduction in stroke incidence rates.19,20 It had been assumed that reduction of blood pressure would be difficult to achieve, hazardous in terms of side effects, and unwarranted on the basis of available data. The Systolic Hypertension in the Elderly Program (SHEP) was a double-blind, placebo-controlled trial involving 4736 persons of an average age of 72 years with systolic blood pressure levels of 160 mm Hg. or greater and diastolic pressures below 90 mm Hg.19 In the treatment group, where blood pressure reduction averaged 11/4 mm Hg, there was a 37% reduction in
P.99
stroke and a 27% reduction in MI and coronary death after 4.6 years of followup. The magnitude of the benefit was probably an underestimate impact of treatment on disease outcomes since, by the end of the SHEP trial, 44% of patients assigned to the placebo group were no longer receiving randomized treatment. These findings have enormous importance because two-thirds of all individuals with hypertension above the age of 65 years have isolated systolic hypertension. Of course, the majority of strokes occur in this age group.
It is clear from the SHEP trial and European Working Party on Hypertension in the Elderly (EWPHE) study that antihypertensive medication was well tolerated by the elderly.13 SHEP demonstrated that reduction of pressure was accomplished with relative ease. Approximately half were controlled with chlorthalidone (a thiazide diuretic) alone, which was well tolerated, as evidenced by a 90% compliance rate in the active treatment group at five years. Contrary to the fears of clinicians, the treatment group did not experience greater syncope, confusion, falls, or depression.19
More recently, the Systolic Hypertension in Europe (Syst-Eur) trial, a doubleblind, randomized trial in 4695 elderly persons with systolic hypertension, compared the antihypertensive agent nitrendipine to placebo. After a median two years of follow-up, a 42%, (95% CI -60 to -17), p = 0.003 reduction in stroke incidence was found.20 Nitrendipine, a dihydropyridine calcium channel blocker, the antihypertensive drug used (an angiotensin-converting enzyme, then a thiazide diuretic could be added) and was quite effective in stroke prevention. Total coronary events declined by 26% (p = 0.03), but cardiovascular mortality and all causes of mortality were not significantly reduced. However, concerns have been raised that certain calcium channel blockers increase rates of myocardial infarction.21,22 The treatment of choice for control hypertension is generally considered to be a diuretic, a beta-blocker, or both.2 Because increased blood pressure is the most powerful risk factor for stroke, and because the benefits of treatment occur so promptly, control of increased blood pressure, systolic as well as diastolic, is the cornerstone of stroke prevention.
Optimal Blood Pressure
The optimal level to which elevated blood pressure should be reduced for stroke prevention remains unknown, but it is clearly lower than had been previously thought. Fears that overzealous blood pressure reduction would reduce cerebral blood flow in persons with cerebral atherosclerosis and precipitate stroke have not been borne out. Despite the evidence that careful and sustained reduction of elevated blood pressure prevents stroke, less than vigorous control has been advocated by some.23 In a highly regarded textbook of geriatric medicine, the author states Although advocated as a possible ideal, there is therefore no need to normalize the blood pressure to a diastolic below 90 or a systolic below 160
P.100
mm Hg in order to produce at least some benefit. A more modest reduction of pressure may constitute a desirable compromise between benefit and adverse effects of treatment for some patients. 23 The major concern expressed is that vigorous treatment of hypertension in the elderly might precipitate stroke or produce serious adverse effects. These specific effects of treatment include hypokalemia, hyponatremia, and increased rates of dementia, depression, faints, falls, fractures. The occurrence of these adverse effects was systematically monitored in the treated groups and did not occur in these large trials of isolated systolic hypertension in the elderly.19,20
On the basis of an analysis a number clinical trials and meta-analyses, for stroke prevention, the recommended target for systolic pressure is less than 125 mm Hg. and the diastolic pressure less than 85 mm Hg (Figure 5.4).24 To address this question, the Hypertension Optimal Treatment (HOT) trial randomly
P.101
assigned 18,790 patients, aged 50 80 years (mean 61.5 years) with diastolic blood pressures between 100 mm Hg and 115 mm Hg (mean 105 Hg), to goals of one of three diastolic pressure ranges.25 One-third was allocated to the target pressure <90 mm Hg, one-third to 85 and 80 Hg. Diastolic pressure was reduced by 20.3 mm Hg, 22.3 and 24.3 Hg in these target groups, respectively. The lowest incidence of major cardiovascular events occurred at a mean achieved diastolic level of 82.6 mm Hg and at a systolic pressure of 138.5 mm Hg. For stroke, the lowest risk was below 80 mm Hg diastolic and 142.2 mm Hg systolic. However, the small differences in blood pressure reduction in the three target groups made it difficult to recognize significant differences in event rates the three groups, and for stroke these differences were not statistically significant. Statistical significance was reached only for the end point all myocardial infarction (p trend = 0.05, relative risk = 1.37, 95% CI 0.99 1.91) comparing the group whose target was 90 mm Hg vs. 80 mm Hg. In the subgroup of 1501 patients with diabetes mellitus, greater reduction in the diastolic pressure was associated with an approximately 30% relative risk reduction in stroke, although these effects also were not statistically significant. This issue of target blood pressure levels has yet to be definitively resolved and is still under study.
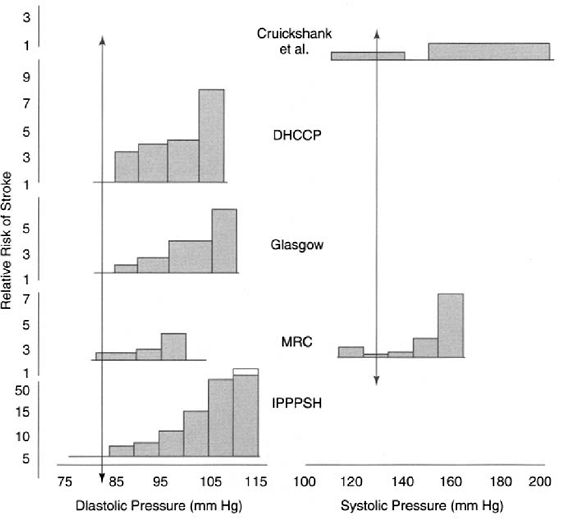 |
FIGURE 5.4. Relative risks of stroke according to blood pressure during treatment for hypertension in eight studies and meta-analyses. The arrows indicate the levels of treated systolic and diastolic blood pressure associated with the lowest risks of stroke. Reprinted from Fletcher AE, Bulpitt CJ. How far should blood pressure be lowered? N Engl J Med. 1992;326:251 254 . Used by permission. |
Choice of Antihypertensive Drugs
Concern about the expense of antihypertensive medication is real, but for stroke, most trials have demonstrated approximately a 40% relative risk reductions with inexpensive agents thiazide diuretics, beta-blockers, and hydralazine. The optimal drugs and combinations of drugs for specific patients is currently being intensively studied in many large scale trials, with more than 100,000 patients already randomized.21
Subgroups of Hypertensive Patients Including Stroke Risk Profile
Type 2 diabetics experience an increase in microvascular and macrovascular disease incidence, including stroke.26 To determine if tight control of blood pressure could reduce these cardiovascular complications, 1148 hypertensive type 2 diabetics were recruited. They were randomized to either an angiotensin converting enzyme inhibitor (captopril) or a beta-blocker (atenolol) and to two levels of blood pressure control. Of the patients, 758 were allocated to a tight control of blood pressure group (goal <150/<85 mm Hg) and 390 to a less-tight control group (< 180/105 mm Hg).27 Reductions in all the cardiovascular endpoints occurred in the tight control group compared to less-tight control group. A 44% relative risk reduction of stroke was seen after 8.4 years median follow-up.
P.102
Neither antihypertensive agent was superior, either in terms of the benefit or absence of harm. It thus seems likely the marked increase in stroke and other microand macrovascular complications of type 2 diabetes mellitus may be significantly reduced by tight control of the frequently associated elevated blood pressures.28
Among asymptomatic persons with elevated blood pressure, it would be helpful to be able identify those at greatly increased risk of stroke. At any given blood pressure level, the presence of associated risk factor abnormalities exerts a powerful influence on stroke risk. For example, a 70-year-old man with systolic blood pressure of 120 mm Hg may have several times the risk of stroke someone with a systolic pressure of 180 mm Hg who is free other risk factor abnormalities.29 In persons with high normal blood pressure or mild systolic hypertension and few associated stroke risk factors, control might be accomplished with hygienic measures, such as weight loss, increase in dietary potassium, reduction in dietary sodium, moderation of alcohol consumption, and promotion of moderate physical activity. Of course, these measures can also be advocated for most people. Persons with higher blood pressure levels and those with associated cardiovascular disease, cigarette smoking, or, particularly, diabetes mellitus will undoubtedly require medication to achieve blood pressure control.
In order to select those persons at greatest risk of developing cardiovascular disease and stroke, a risk profile was developed based on 36 years of follow-up data from Framingham.29 Using information collected during a complete history and physical examination, including an electrocardiogram (ECG), probability of stroke may be determined. Using a separate table for men and women, stroke probability is determined by a point system based on age, systolic blood pressure, antihypertensive therapy use, presence of diabetes, cigarette smoking, history of cardiovascular disease [coronary heart disease (CHD) or heart failure (CHF)], and electrocardiogram (ECG) abnormalities [left ventricular hypertrophy (LVH) or atrial fibrillation (AF)]. It is apparent that in persons at varying levels of blood pressure, the probability stroke varies across a wide range. Probability rises with increased systolic blood pressure (120 mm Hg and 180 mm Hg are shown) depending on the presence of other abnormalities in the risk profile (Figure 5.5).29 This risk provides a quantitative determination of probability of stroke relative to what is average for a man of this age. The realization that the probability of stroke is increased several-fold may help patient and physician to more fully appreciate the need for serious risk factor management.
Preventive Implications
The recent demonstration of the benefits treatment and control hypertension in stroke prevention the elderly with diastolic or isolated systolic hypertension
P.103
suggests that considerable progress remains to be achieved. Recently, it has been estimated that of the 50 million hypertensives in United States, only 32.5 million were aware of its presence and 24.5 million were being treated. Unfortunately, only 10.5 million hypertensives had their blood pressure controlled, leaving nearly 40 million either unaware, untreated, or treated but uncontrolled. Because clinical trial data suggest an approximately 40% reduction in stroke incidence, even with short-term treatment trials (i.e., less than 5 years), a great deal of stroke prevention could be achieved by blood pressure control. It has been estimated that nearly 250,000 new strokes could be prevented each year by such efforts. In light of the end of the decline in stroke mortality, it is imperative that such preventive efforts be redoubled. Effective programs to detect, treat, and control hypertension, particularly in those at greatest risk of stroke, those above age 65 years, hold promise that stroke incidence and mortality may be reduced still further. When these measures are combined with a long-term, sustained program of risk factor modification, such as cigarette smoking cessation, the tools for
P.104
achieving further substantial reduction in death and disability from stroke are already available.
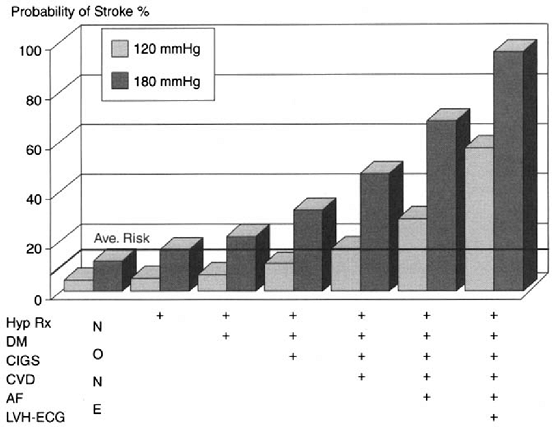 |
FIGURE 5.5. Probability of stroke during 10 years in men aged 70 years at two systolic blood pressure levels: impact of other risk factors. Hyp Rx = antihypertensive therapy; DM = diabetes mellitus; Cigs cigarette smoking; CVD = previously diagnosed coronary heart disease, cardiac failure, or intermittent claudication; AF = atrial fibrillation; LVH-ECG = left ventricular hypertrophy by electrocardiogram. Source: Wolf PA, D'Agostino RB, Belanger AJ, Kannel WB. Probability of stroke: A risk profile from the Framingham Study. Stroke 1991;22:312 318 . |
References
1. Pickering G. In: Laragh JH, ed. Hypertension Manual: Mechanisms, Methods, Management, New York: Yorke Medical Books, 1973.
2. JNC-VI: The sixth report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Arch Intern Med. 1997;157: 2413 2446.
3. Morbidity & Mortality: 1998 Chartbook on Cardiovascular, Lung and Blood Diseases. National Institutes of Health, National Heart, Lung, and Blood Institute. October, 1998.
4. Janeway TC. A clinical study of hypertensive cardiovascular disease. Arch Intern Med. 1913;12:755.
5. Russell RWR. Observations on intracerebral aneurysms. Brain 1963;86:425.
6. Cole FM, Yates PO: The occurrence and significance of intracerebral microaneurysms. J Pathol Bacterial 1967;93:393.
7. Kannel WB, Wolf PA, Verier J, McNamara PM. Epidemiologic assessment of the role of blood pressure in stroke. The Framingham Study. JAMA. 1970;214(2):301 310.
8. Joseph LN, Kase CS, Beiser AS, Wolf PA. Mild blood pressure elevation and stroke: The Framingham Study. Stroke 1998;29(1):277.
9. MacMahon S, Rodgers A. The epidemiological association between blood pressure and stroke: Implications for primary and secondary prevention. Hypertens Res. 1994; 17(suppl I):S23-S32.
10. MacMahon S, Peto R, Cutler J, Collins Sorlie P, Neaton Abbott Godwin Dyer A, Stamler J. Blood pressure, stroke, and coronary heart disease. Part 1: Prolonged differences in blood pressure: Prospective observational studies corrected for the regression dilution bias. Lancet 1990;335(8692):765 774.
11. Collins R, Peto MacMahon S, Hebert P, Fiebach NH, Eberlein KA, Godwin J, Qizilbash N, Taylor JO, Hennekens CH. Blood pressure, stroke, and coronary heart disease. Part 2: Short-term reductions in blood pressure: Overview of randomised drug trials in their epidemiological context. Lancet 1990;335(8693):827 838.
12. Dahlof B, Lindholm LH, Hansson L, Schersten Ekbom T, Wester PO. Morbidity and mortality in the Swedish Trial Old Patients with Hypertension (STOP-Hypertension. Lancet 1991;338(8778):1281 1285.
13. Amery A, Birkenhager W, Brixko P, Bulpitt C, Clement D, Deruyttere M, De Schaepdryver A, Dollery C, Fagard R, Forette F, et al. Mortality and morbidity results from the European Working Party on High Blood Pressure in the Elderly trial. Lancet 1985; 1(8442): 1349 1354.
14. Coope J, Warrender TS. Randomised trial of treatment hypertension in elderly patients in primary care. Brit Med J Clin Res Ed 1986;293(6555):1145 1151.
15. MRC Working Party. Medical Research Council trial of treatment hypertension in older adults: principal results. BMJ 1992;304(6824):405 412.
16. Rutan GH, McDonald RH, Kuller LH: A historical perspective of elevated systolic vs diastolic blood pressure from an epidemiological and clinical trial viewpoint. J Clin Epidemiol 1989;42:663 673.
17. Wilking SV, Belanger A, Kannel WB, D'Agostino RB, Steel K: Determinants of isolated systolic hypertension. JAMA 1988;260:3451 3455.
P.105
18. Kannel WB, Wolf PA, McGee DL, Dawber TR, McNamara P, Castelli WP. Systolic blood pressure, arterial rigidity, and risk of stroke: The Framingham Study. JAMA 1981;245(12):1225 1229.
19. SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP. JAMA 1991;265(24):3255 3264.
20. Staessen JA, Fagard R, Thijs L, Celis H, Arabidze GG, Birkenhager WH, Bulpitt CJ, de Leeuw PW, Dollery CT, Fletcher AE, Forette F, Leonetti G, Nachev C, O'Brien ET, Rosenfeld J, Rodicio JL, Tuomilehto Zanchetti A. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension: The Systolic Hypertension in Europe (Syst-Eur. Trial Investigators. Lancet 1997;350(9080):757 764.
21. Fletcher AE, Bulpitt CJ. How far should blood pressure be lowered? N Engl J Med 1992;326(4):251 254.
22. Estacio RO, Jeffers BW, Hiatt WR, Biggerstaff SL, Gifford N, Schrier RW. The effect of nisoldipine as compared with enalapril on cardiovascular outcomes in patients with non-insulin-dependent diabetes and hypertension. N Engl J Med 1998;338(10): 645 652.
23. Cutler JA. Calcium-channel blockers for hypertension uncertainty continues. NEngl J Med 1998;338(10):679 681.
24. Evans JG. The prevention of stroke. In: Evans JG, Williams TF, eds. Oxford Textbook of Geriatric Medicine. New York: Oxford University Press, 1992:329 334.
25. Hansson L, Zanchetti A, Carruthers SG, Dahlof B, Elmfeldt D, Julius S, Menard J, Rahn KH, Wedel H, Westerling S. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: Principal results of the Hypertension Optimal Treatment (HOT. randomised trial. HOT Study Group. Lancet 1998; 351(9118):1755 1762.
26. Manson JE, Colditz GA, Stampfer MJ, Willett WC, Krolewski AS, Rosner B, Arky RA, Speizer FE, Hennekens CH. A prospective study of maturity-onset diabetes mellitus and risk of coronary heart disease and stroke in women. Arch Int Med 1991; 151(6):1141 1147.
27. Turner R, Holman Stratton I, et al. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ 1998;317(7160):703 713.
28. Orchard T. Diabetes: A time for excitement and concern. Hopeful signs exist that the ravages of diabetes can be tamed. BMJ 1998;317(7160):691 692.
29. Wolf PA, D' Agostino RB, Belanger AJ, Kannel WB. Probability of stroke: A risk profile from the Framingham Study. Stroke 1991;22(3):312 338.
EAN: 2147483647
Pages: 23
- ERP Systems Impact on Organizations
- ERP System Acquisition: A Process Model and Results From an Austrian Survey
- Intrinsic and Contextual Data Quality: The Effect of Media and Personal Involvement
- A Hybrid Clustering Technique to Improve Patient Data Quality
- Development of Interactive Web Sites to Enhance Police/Community Relations