63 - Anatomy of the Thoracic Duct and Chylothorax
Editors: Shields, Thomas W.; LoCicero, Joseph; Ponn, Ronald B.; Rusch, Valerie W.
Title: General Thoracic Surgery, 6th Edition
Copyright 2005 Lippincott Williams & Wilkins
> Table of Contents > Volume I - The Lung, Pleura, Diaphragm, and Chest Wall > Section XIII - The Trachea > Chapter 75 - Tracheostomy
function show_scrollbar() {}
Chapter 75
Tracheostomy
Todd L. Demmy
Amgad El Sherif
INTRODUCTION AND HISTORY
Tracheostomy is an operation with a long history, but it has been popular only for the last hundred years. Extrapolating from the work of Dewar and co-workers (1999), U.S. surgeons perform at least 150,000 tracheostomies annually for management of acute and chronic airway problems, as well as planned permanent tracheostomies for the treatment of advanced head and neck malignancies. Despite their frequent use, there are controversies on the timing and usage of tracheostomies because of worldwide practice variations in the evaluation of the management of critically ill patients. This chapter seeks to explore the history, indications, technical considerations, complications, management and outcomes of patients who receive this treatment.
Incisions in the windpipe were documented as early as 1500 bc. Frost (1976) found the indications were airway obstructions usually of a traumatic nature. For instance, Alexander the Great was credited for using the tip of his sword to perform a crude tracheostomy in a soldier, as noted by Beatrous (1968). During the Renaissance, tracheostomy was decried as a futile and irresponsible action for surgeons and was widely discouraged. Then, in the first half of the 19th century, Trousseau saved one of four patients with severe diphtheria by using a tracheostomy. The report of this led to its popularization for other diseases, such as laryngeal malignancy, and its use during wartime, as during the American Civil War. In the early 1900s, Jackson (1923) refined the procedure of tracheostomy, and some of the tools that he designed are still in use today.
The polio epidemic in the 1930s led to further expansion of the use of tracheostomies. Beatrous (1968) and Frost (1976) concluded that the salutary effects of tracheostomy on sputum control and ventilator management promoted its popularity in the second half of the 20th century.
Tracheostomy history is entwined with many interesting and frequently fatal medical diseases that have interested physicians over the ages because of the serious impact these diseases had on the respiratory system. With less invasive, percutaneous methods for inserting tracheostomy tubes, the present era is one with interest in even earlier indications for this common procedure.
INDICATIONS FOR TRACHEOSTOMY
The indications for tracheostomy are grouped loosely into four major categories: (a) conditions associated with upper airway obstruction, (b) conditions that impair alveolar ventilation to require assisted respiration, (c) conditions with excessive airway secretions, and (d) miscellaneous other indications. A list of diseases for each category is provided in Table 75-1.
The indications and results of tracheostomy are diverse and occasionally controversial. Tracheostomy is used frequently in critically ill patients as one part of an overall process for their care. Accordingly, many competing support technologies affect the indications or the resultant outcomes depending on their availability and effectiveness. This is analogous to the difficulty determining the salutary effects of pulmonary artery catheter measurements in critically ill patients. The choice and timing of tracheostomy is influenced highly by (a) the long-term patient prognosis, (b) the anticipated duration of the inciting problem, (c) patient and family concerns regarding its use, (d) the skill sets of individuals who place tracheostomy, and (e) the availability and effectiveness of less invasive respiratory support methods.
Tracheostomies for acute upper airway obstructions too dangerous to manage by standard intubations or other techniques are not controversial. Beatrous (1968) noted that patients in respiratory distress may exhibit restlessness, apprehension, mental confusion, cyanosis, fatigue, and insomnia. Bass (1978) and Cantrell and associates (1978) reported precipitating conditions such as massive facial trauma, epiglottitis, and impacted foreign body. Functional obstruction of the upper airway requires placement of a tracheostomy. Dye (1983) and Mattox and Gates (1983) advocated
P.1018
the use of tracheostomy for sleep apnea, but this has been supplanted largely by the use of nocturnal continuous positive airway pressure (CPAP). Occasionally, tracheostomy is needed for bilateral vocal cord paralysis, as reported by Kanner (1983).
Table 75-1. Indications for Tracheostomy | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
For the difficult airway known preoperatively, Fuhrman and Farina (1995) and Nazari and colleagues (1999) occasionally used tracheostomy prophylactically. They also used it to treat complications of endotracheal intubations. Patients with tracheomalacia, rather than stenosis, may also require tracheostomy. This occurs occasionally in patients with large goiter or other airway malformations that lead to tracheal cartilage loss, as documented by Abdel Rahim (1999) and Palazzo (2000) and their co-workers.
The timing or need for tracheostomy for patients with alveolar hypoventilation is somewhat more controversial. The main issues relate to the anticipated patient survival for long-term chronic illnesses or the speeds acute diseases take to resolve. Frequently, acute respiratory failure from infection superimposed on chronic respiratory insufficiency may be an indication for the procedure. Brook (2000), Rodriguez (1990) and Sugerman (1997) and their co-workers showed conflicting or mixed results when evaluating the use of aggressive early tracheostomies against approaches that wait for signs of patient improvement. The favorable weaning found in some studies of early tracheostomy could be related to other concomitant respiratory interventions. For some conditions, such as infratentorial or other severe neurologic injuries, tracheostomy should be placed by day 8. Qureshi and associates (2000) found that after that time, extubation is unlikely, as is the risk for hospital death from associated traumatic injuries. Also, patients with traumatic injuries who have a Glasgow Coma Scale score of less than or equal to 8 (or injury severity scores greater than or equal to 25) may require tracheostomy, as reported by Gurkin and colleagues (2002). D'Amelio and co-workers (1994) found that early percutaneous endoscopic gastrostomy, combined with tracheostomy, facilitated the care of brain-injured patients.
The proportion of indications and the urgency of the procedures can vary greatly given the proportion of emergencies with which an institution is faced. For instance, Ivatury and co-workers (1992) at one trauma center reported a 33% urgent tracheostomy rate. This is quite a different experience than some intensive care units that do almost all elective tracheostomies for patients with respiratory failure. The contemporary works of Divisi (2002), Ivatury (1992), McHenry (1997) and Mittendorf (2002) and their associates showed that about one-third of tracheostomies are performed for upper airway problems and the rest are for respiratory failure caused by intrinsic pulmonary damage or neurologic compromise.
Tracheostomy is performed in about 10% of patients ventilated over 24 hours. This represents about 1.3% of all intensive care unit patients. The second week of intubation is often
P.1019
the most prevalent time for choosing this option according to Fischler and associates (2000). This may be because Bishop and colleagues (1985), Whited (1984) and Bishop (1989) found that endotracheal tube trauma caused mucosal lesions between 7 and 11 days. Plummer and Gracey (1989) cited a consensus conference that suggested tracheostomy on day 3 to 5 if the probability of weaning is low for the next 21 days.
Flum and co-workers (1997, 1998) reported the controversial role of tracheostomy in patients with acquired immunodeficiency syndrome (AIDS). AIDS patients with typical community-acquired pneumonias may benefit from tracheostomy because there is some chance of recovery with use of antibiotics. On the other hand, AIDS patients with respiratory failure from other causes, such as opportunistic infections, are unlikely to have their survival improved by the placement of a tracheostomy tube (although it may be indicated for better pulmonary toilet and quality of life in patients who have already been intubated).
Patients with respiratory failure from weakness are those with generalized myopathy or neuropathy, including Guillain-Barr syndrome or postpoliomyelitis syndrome. These diseases can also have an obstructive effect by paralyzing the vocal cords, as documented by Lawn and Wijdicks (1999), as well as by Freezer (1990) and Vaz Fragoso (1992) and their associates. Tracheostomy works in these situations by reducing upper airway resistance and limiting the dead space that is proportionally greater in patients with shallow ventilation. Similarly, Ahmed and Mohyuddin (1995) and Pinilla (1982) have used tracheostomy in patients with flail chests for the same reasons and also to facilitate ventilatory support for internal splinting.
Other surgical diseases of the chest influence indications for tracheostomy. Occasionally, early tracheostomy proves beneficial. For instance, Nomori and associates (2000) used early tracheostomy in pediatric burn patients, and Palmieri and co-workers (2002) found that minitracheostomy tubes in lung cancer patients improve outcomes. Izumi and co-workers (1995) advocate the selective use of tracheostomy for esophagectomy patients.
There is considerable interest in the use of tracheostomy after open-heart surgery. Respiratory failure occurs commonly in this population, and there is a credible mechanism by which tracheostomy flora can contaminate a nearby median sternotomy wound. Technologic adaptations, such as percutaneous tracheostomy, cricothyroidotomy, or a longer delay until tracheostomy, address this risk. As such, Curtis (2001) and Stamenkovic (2000) and their colleagues failed to show a definite relation between the timing of median sternotomy infections and tracheostomy.
Excessive airway secretions prompt tracheostomy commonly. This indication is rarely independent of some other failure of pulmonary mechanics or airway protection. Therefore, the studies looking at use of tracheostomy solely for toilet are limited. However, for patients with adequate alveolar ventilation, tracheostomy tubes can be smaller to allow passage of only the suction catheters.
Rarely, tracheostomy is indicated for advanced and unusual conditions. James and co-workers (1980) noted that some patients with benign lower airway constrictions, such as from mediastinal fibrosis, benefit from tracheostomy. This allows easier access for stent replacement and patient salvage in case of abrupt airway obstruction.
Generally, the indications for tracheostomy are similar for the standard or percutaneous methods. On occasion, cricothyroidotomy is indicated over tracheostomy. This is performed uncommonly, such as in situations in which urgent airway access is needed and there is limited time to place a standard tracheostomy. Cricothyroidotomy is also used when a larger distance is desired between the airway wound and wounds in the low neck and mediastinum.
TECHNIQUES OF TRACHEOSTOMY AND CRICOTHYROIDOTOMY
General Considerations
Despite variations in the techniques of surgical airway access with both open and percutaneous methods, there are basic elements common to all. These basic elements relate to safety and preparation. Generally, proper patient selection and a team of care providers prepared to manage usual or unexpected problems obtain the best results, no matter what techniques are used. Anatomic considerations tailored to the patients are important. The need to separate the tracheostomy wound from other surgical areas, tracheostomy timing, and special variations like incision orientation, percutaneous devices, or specific tube types influence the preparation. One of the first considerations is the space for its performance. Many surgeons prefer the operating room because of the proximity of specialized equipment and personnel accustomed to handling difficult airway problems. The intensive care unit has become an increasingly popular place. In any case, there needs to be an experienced team that is able to handle the ventilatory management; this team might include respiratory therapists, anesthesiologists, and other intensive care specialists. Rapid access to flexible fiberoptic bronchoscopy is important and is considered part of the procedure for many who practice percutaneous placement.
After appropriate personnel and equipment are assembled, the next consideration is patient preparation. Generally, patients who require this procedure are already sedated. Otherwise, conscious sedation should be used as a minimum. Pierce and co-workers (1973) found that sealant barriers reduced contamination of nearby recent surgical incisions by tracheal drainage. Additional neck extension may be obtained by placing a roll behind the patient's shoulders. The head should be held in the midline position or supported by small sandbags placed bilaterally. Positioning is even more critical for patients with short necks or obesity that impairs exposure. This is also a good time to
P.1020
review any imaging studies that might predict unfavorable anatomic variations. Distorted or unidentifiable anatomy, known or predicted difficult endotracheal intubation, previous neck operations, cervical irradiation, neck trauma, visible large interposing vessels, morbid obesity, and severe coagulopathy are possible contraindications to percutaneous tracheostomy according to Freeman (2000). Palpation of the neck before prepping the skin alerts the surgeon to the presence of aberrant vessels, indurated tissue, or other anatomic problems. Headlights, in addition to portable overhead lighting, improve the exposure for bedside open tracheostomy.
The entire operating team, including those personnel who will be assisting with the exchange of the airway support tubes, should be familiar with procedural steps the surgeon is planning. Before skin incision, it is important to verify the presence of essential tools such as suction, cautery (or other hemostatic devices), required sutures, securing tapes for the tracheostomy tube, and an appropriate selection of tracheostomy tubes in case the desired one is damaged or has to be abandoned for a different size. Also, nearby resuscitation equipment is important in case oxygen desaturation causes cardiac complications or the need to reestablish an airway by oral endotracheal intubation. Specific tools that many surgeons find useful during open tracheostomy are the tracheal hook to control the airway and the Jackson dilation forceps to expand the incised tracheotomy.
Technique of Open Tracheostomy
After appropriate prepping, draping, sedation, and local anesthetic infiltration, the surgeon verifies the presence of the appropriate equipment and personnel as noted. Frequently, the tracheostomy tube has been opened, and its cuff has been checked for competency. Also, the securing tapes and other sutures that will be necessary should be verified. Although a vertical incision can be performed, a 2- to 3-cm transverse incision 1 finger-breadth above the suprasternal notch is preferred. A horizontal incision has a better late cosmetic appearance. Vertical scars tend to develop widening and depression. The cautery can be used to incise down to the strap muscles that are split in midline. Weitlaner self-retaining retractors are used frequently. Thin, S-type retractors provide useful lateral retraction and exposure. Digital palpation identifies the tracheal prominence and ensures a proper dissection plane. The strap muscles are split in the midline, and dissection is carried through to the pretracheal fascia, which is divided. For surgeons who prefer a higher tracheostomy, the thyroid isthmus can be divided by suture ligation between clamps; cautery has been used safely by Calhoun and co-workers (1994). After the trachea has been exposed, additional lidocaine can be injected into the trachea to provide local anesthesia. Care should be taken to avoid damaging the tracheal balloon. The endotracheal tube should have been freed at this point and ready to be withdrawn slowly. Several choices for creating the tracheostomy access are illustrated in Figure 75-1. Jackson (1923) originally described a vertical midline incision through cartilage 2, 3, and 4. Many others and we prefer flap-tracheostomy. An inferiorly based flap was described by Bjork (1960) and is based on the rationale of a caudal origin of the blood supply of the trachea to maximize flap viability. To accomplish this, a central horizontal tracheotomy is created with a small blade such as a No. 15 scalpel. The incision is extended to about 1 cm and then carried obliquely on each side with a heavy scissors through the tracheal ring in an inferolateral manner. This creates an inferior flap that can be tethered with a small suture, such as a 4-0 polypropylene, to the inferior skin edge. It is tied with a long loop without any traction on the flap. This loop is grasped in the event of early tube dislodgment, allowing trachea control to ease reinsertion. Another alternative is a superiorly placed flap with suturing of inferior skin to the inferior tracheal margin. Miller and co-workers (1995) use a more generous skin incision with muscle transposition (above the upper flap to prevent superior erosion) for cases in which long-term tracheostomy access is anticipated.
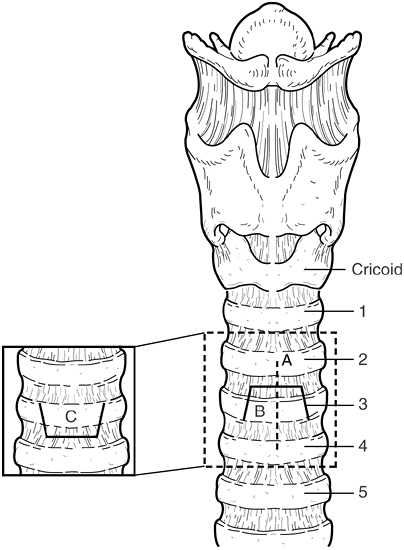 |
Fig. 75-1. Common incisions used for open tracheostomy. A. Vertical (Jackson) incision. B. Inferior-based (Bjork) flap. C. Superior-based flap. |
After the tracheotomy is created, the endotracheal tube is withdrawn so that the tip of the tube is just immediately superior to the opening. Suction is held ready to capture thick mucous secretions that are expelled and contaminate the wound excessively. A large Frazier-tipped or similar suction catheter is useful for this purpose. Then, an appropriately sized tracheostomy tube, dipped in a water-soluble lubricant, is inserted gently into the tracheotomy and directed
P.1021
inferiorly. This is done with an internal obturator that obstructs airflow. The obturator is promptly removed and replaced with a hollow internal cannula with a standard ventilator fitting.
It is important to have had good hemostasis before this point. Hand-held retractors might be better during insertion of the tracheostomy because some self-retaining retractors are tedious to remove after the tracheostomy tube has been inserted. The tracheostomy tube should not be forced into position because this can create a posterior laceration of the trachea that can extend to the carina. Rather, smaller tracheostomy tubes should be available immediately and used. Some expansion of the tracheal stoma can be done with Jackson forceps. However, this is an unusual need when a large enough tracheotomy has been created. Tracheal tapes are prepared with one cut one third the distance of the other to allow convenient lateral tying of the knot. Heavy sutures provide two- or four-point fixation from the skin to the tracheostomy appliance plate, thereby reducing the chance of self-extubation. Concern about airway placement of the tracheostomy tube can be corroborated by the use of a rapid CO2 detection filter placed in the respiratory circuit. In addition, flexible fiberoptic bronchoscopy rapidly diagnoses problems with ventilation that occur at this point. Annoying bleeding that does not respond to mild compression or other conservative means may require small retractors to gain exposure. Rarely, decannulation of the tracheostomy and oral reintubation are indicated to control bleeding. Successful placement of the tracheostomy tube without significant bleeding should be confirmed before withdrawing the endotracheal tube from the larynx completely. Hirota and colleagues (2000) instill lidocaine into the tracheostomy tube cuff to reduce discomfort. In situations of difficult anatomy in which airway loss seems probable during tracheostomy, McGuire and co-workers (2001) advocate placing a jet ventilation catheter prophylactically through the endotracheal tube lumen. This smaller catheter can remain in place during the entire tube placement process.
Special Considerations
If a coagulopathy is mild and the patient has not experienced any evidence of spontaneous bleeding, it may be safe to perform a tracheostomy provided there is good exposure. In patients with severe coagulopathy, the tracheostomy can be performed in two stages, with access to the trachea created first, as described by Turnbull (1991). Later, tracheotomy and tube placement are performed. Variations in the tracheal incision can be made, such as the use of a more laterally placed incision used by Tran and associates (1995) to avoid orthopedic spine stabilization wounds.
Decannulation of Tracheostomy
For many types of tracheostomy, elective decannulation by simply removing the tube generally results in good healing. Occasionally, there can be a persistent cutaneous fistula when tracheal tissue becomes adherent and scars to the skin epithelium. In general, flap-type tracheostomies have had better clinical and experimental preservation of the tracheal lumen, as found by Lulenski (1981). Smith and co-workers (1995) found that vertical tracheostomy wounds healed more consistently. Lulenski and Batsakis (1979) were interested in formally or bluntly dissecting the tracheal flap away from the surrounding tissues after removing the tracheostomy tube in an effort to achieve better coaptation of the tracheal rings. This may have some minor benefit but it is not of sufficient importance to require routine repeat dissection of the tracheostomy region after decannulation. Chest radiographs obtained at tracheostomy completion give a baseline image of tube placement and exclude mediastinal emphysema or other signs of tube malposition.
Technique of cricothyroidotomy
The technique of cricothyroidotomy is based on the technical maneuvers just noted. However, the 3-cm incision is made more superiorly, over the palpable cricothyroid membrane. Intradermal and intermembrane lidocaine reduces discomfort and the cough reflex. Sise and colleagues (1984) made a cruciate incision in the membrane and placed the tube with the same set of maneuvers noted. Although this technique is selected often for more emergent conditions, there is evidence that its sequelae are less than suggested by Jackson (1923), the proponent of modern tracheostomy. Ciaglia and co-workers (1985) suspect that cricothyroidotomy was associated with unacceptable stenosis because of associated inflammatory conditions of the larynx peculiar to Jackson's experience. Therefore, the more favorable later experience by Brantigan and Grow (1976) with cricothyroidotomy led to the use of upper tracheal percutaneous tracheostomy just beneath the cricothyroid cartilage to achieve tracheal access.
Technique of Percutaneous Tracheostomy
Sheldon (1957) and Toye and Weinstein (1986) both described percutaneous tracheostomy using a directed cutting blade technique that resulted in the death of a few patients. The success of more superiorly placed tracheostomy tubes, such as the experience of cricothyroidotomy by Brantigan and Grow (1976), led to percutaneous dilated placement above the thyroid to avoid bleeding. Ciaglia and associates (1985) reported the technique of percutaneous dilational tracheostomy. Griggs and colleagues (1991) also described the technique of percutaneous tracheostomy with antegrade dilational methods. Alternatively, there is a retrograde threaded guidewire option whereby a tracheal tube is pulled down through the mouth and then out the skin, which has been reported by Fantoni and Ripamonti (1997).
P.1022
Antegrade Percutaneous Dilation Technique
After appropriate prepping and patient positioning as in the open tracheostomy, local anesthesia is used to infiltrate the skin and confirm the track by aspirating air from the tracheal lumen. The cannula needle is used to introduce a J wire (0.052). Sometimes accurate positioning is confirmed not only by palpation but also by flexible bronchoscopy viewing down from the larynx. A stiff overguiding sheath is then passed over the J wire to prevent possible migration caused by wire kinking during placement of large dilators. Dilation begins with No. 12F dilator. As a variation, there is a large tapered dilator termed the blue rhino, which can be used instead of individual dilators. Sequential dilations proceed from No. 12F to No. 36F, with overdilation used to make it easier to pass the 6-, 7-, or 8-mm tracheostomy tubes later. Once dilated to 36 mm, the appropriate dilation sheath is used within the lumen of the desired tracheostomy tube. A No. 18F is used for a 6-mm internal diameter tube, the No. 21F for a 7-mm tube, and the No. 24F for an 8-mm tube. The cuff needs to be actively deflated and well lubricated to pass through the tunnel. The head of the bed is elevated 30 to 40 degrees after placing it in the tracheostomy tube to reduce venous bleeding, and antibiotic ointment is placed around the skin next to the site. Ciaglia and Graniero (1992), as well as Ciaglia (1985) and Hazard (1988) and their coinvestigators, described this technique with a subcricoid puncture. Toursarkissian and associates (1994) described the procedure using an entry between the first and third tracheal rings. Byhahn (2000a) and Cothren (2002) and their colleagues believe that a single-step rhino dilator is an easier technique with equivalent complications. Figure 75-2 represents the Ciaglia technique diagrammatically. A variation to the technique is using dilating forceps rather than dilators, as described by Griggs (1991), Anon (2000), Nates (2000) and Van Heerbeek (1999) and their associates. Barba (1995), Fernandez (1996), Hinerman (2000) and Winkler (1994) and their coinvestigators advocate bronchoscope use for the placement of the tracheal wire and dilation catheter to ensure proper site selection. Care needs to be taken because continuous bronchoscopy caused hypercarbia in some cases reported by Reilly and co-workers (1995, 1997). Although endoscopic guidance has not been adopted by all centers, it is interesting that Dexter (1995) found that only 9 of 20 tubes were placed in the desired location using a cadaver percutaneous tracheostomy model. Atweh and colleagues (1999) modified the Ciaglia technique to make a suprasternal incision with penetration of the trachea below the thyroid and the tracheal tube tip. In addition to using standard tracheostomy tubes, Leonard and co-workers (1999) described a commercial tracheostomy tube designed for percutaneous placement. If the trachea lies deep, a special long-shank tube may be needed for percutaneous tracheostomy to avoid conversion to open tracheostomy. This was required in about 2% of percutaneous tracheostomies performed by Muhammad and associates (2000a). Because neck extension for percutaneous tracheostomy can be minimal, Mayberry and co-workers (2000) advocate this technique for some trauma patients without cervical spine clearance. Meyer and colleagues (2002) found that repeat percutaneous dilation tracheostomy can be a safe procedure. Occasionally during placement of a percutaneous tracheostomy, the catheter can hang when a transition ridge of the
P.1023
tracheostomy passes against stiff tracheal cartilage. Frova and Quintel (2002) tested a newer device that uses a rolling motion to help with this problem. Finally, some operators have had difficulty with control of the airway while doing bronchoscopy to ensure proper placement of the wire. This is because the endotracheal tube needs to be pulled back into the larynx. Dosemeci and co-workers (2002) addressed this by the use of a laryngeal mask airway as an alternative for ventilation in some patients.
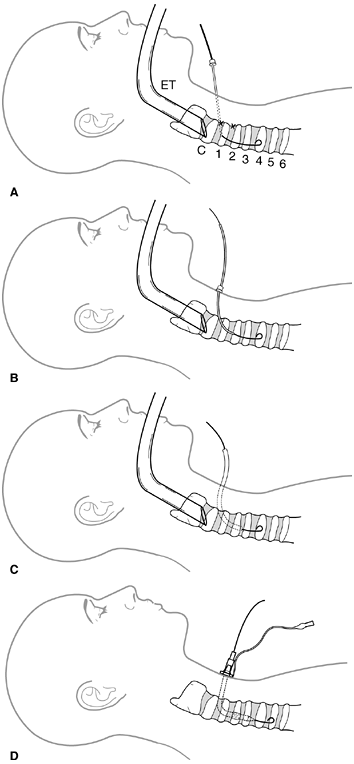 |
Fig. 75-2. Antegrade method of percutaneous tracheostomy. A. Percutaneous puncture and insertion of J wire. X, preferred entry sites; ET, endotracheal tube; C, cricoid cartilage, 1 to 6 tracheal cartilages. B. Placement of oversheath. C. Sequential dilation. D. Insertion of tracheostomy. |
Translaryngeal (Fantoni's) Technique
Fantoni and Ripamonti (1997) described another method of percutaneous tracheostomy. In this technique, the same precautions and preparations are done as with other types of percutaneous tracheostomy. A curved cannula is used to introduce a guidewire under endoscopic vision, and the curve in the cannula directs it in a retrograde fashion toward the pharynx instead of distally. The endotracheal tube, which has been pulled back to allow this maneuver, has the balloon deflated slightly to allow the wire to enter the pharynx where it is grasped. Next, the endotracheal tube is exchanged with a long and thin endotracheal tube, which is passed into the distal airway. The tracheal cannula is connected to the pull-wire and advanced transorally through the pharynx and larynx into the trachea, and then the channel penetrates from inside out through the anterior tracheal wall up to the skin (Fig. 75-3). The skin is held down to provide counterpressure during the penetration. The cannula's cuff is then rotated 180 degrees to be directed toward the carina by means of an obturator. The tube can then be connected to the ventilator after removing the thin ventilating cannula that had been providing ventilation during this process.
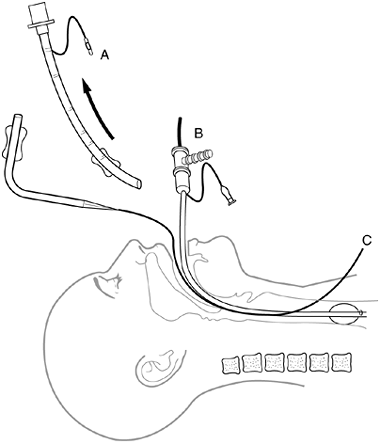 |
Fig. 75-3. Intermediate step in the translaryngeal technique. The endotracheal tube (A) has just been removed, the narrow tube (B) is being used ventilate the patient, and the pull wire (C) has been connected to the tracheostomy catheter. |
An advantage of Fantoni's technique is that less dilation is necessary to achieve passage of the cannula, rather than the overdilation needed by Ciaglia's technique, as contrasted to Fantoni and Ripammonti's (1997) technique as well as techniques reported by Sarpellon (1998) and Westphal (1999) and their co-workers. Also, Fantoni's technique offers the advantage of ventilation during the dilation process, albeit with a smaller tube. Because of the reduced dissection of tissues with this method, Byhahn and associates (2000b) have advocated early percutaneous tracheostomy after median sternotomy.
Mediastinal Tracheostomy
Although physicians other than thoracic surgeons perform many types of tracheostomy, the mediastinal tracheostomy is a more complex procedure often performed in concert with head and neck oncologic surgeons. The history of the anterior mediastinal tracheostomy is described well by Orringer and Sloan (1979). This procedure may be needed for stomal recurrences after laryngectomy and for other complex head and neck malignancies. The operative technique is characterized by preparation that includes the neck, chest, abdomen, and one thigh. The thigh access is the site of a possible skin graft. The operation may be preceded by mobilization of the gastric tube in case this is needed to reconstruct the cervical esophagus. Other conduits can be prepared by laparotomy as well. A common technique is to use a bipedicled advancement flap of upper pectoral skin that serves as the basis for the stoma site. This is accomplished using transverse supraclavicular and inframammary parallel incisions. The trachea is mobilized along the prevertebral fascia, and the neck is supported in a manner so that the oncologic head and neck dissection is performed with optional resection of the strap muscles and required neck structures.
Removing the anterior breast plate allows access to the superior mediastinum, as documented by Orringer and Sloan (1979). This is done by dividing the clavicles lateral to the manubrial clavicular joints, cutting ribs 1 and 2 near the manubrium, and sectioning the body of the sternum just inferior to its joint with the manubrium. Care is taken to avoid lateral tracheal dissection distally because this could interfere with the blood supply. Instead, anterior and posterior blunt dissection is performed. Occasionally, one of the lobes of the thyroid gland and parathyroid tissue can be preserved without compromising the margins of resection. Pharyngogastric or other pharyngoenteric anastomoses are constructed before performing the tracheal stoma suturing.
P.1024
The trachea has been sectioned by this point in an oblique fashion with the posterior flap longer so that it can reach to the skin with less tension. The pectoralis muscle is mobilized to cover the sharp rib edges by rolling it over the bony ridge and suturing it to the interior chest wall. Occasionally, the trachea needs to be transposed beneath the brachiocephalic vessels to have an acceptable length (Fig. 75-4). The trachea can be sutured with 4-0 nonabsorbable sutures. The trachea stoma can be quite short in this type of resection because the skin can drop down to the trachea. Therefore, care is needed to position a ventilating tube without obstructing the airway. During the course of this tracheostomy, a sterile endotracheal tube is used to ventilate the open stoma while the enteric anastomosis is performed. Preparation for this transitional airway needs to be coordinated with the anesthesiologist.
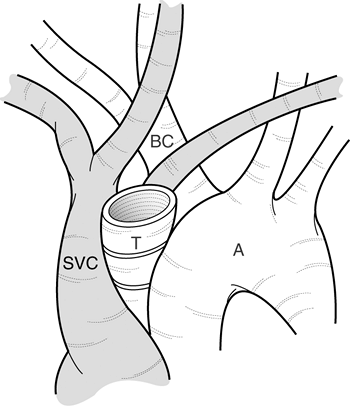 |
Fig. 75-4. Tracheal transposition required for some cases of mediastinal tracheostomy. A, aorta; BC, brachiocephalic artery; SVC, superior vena cava; T, trachea. |
A variation of this technique is the use of a rotational pectoralis flap based on the thoracoacromial vascular distribution, as reported by Orringer and Sloan (1979). Occasionally, patients with impaired healing from radiation or chemotherapy or attenuated mediastinal tissues have a higher risk for complex, life-threatening fistulae. To reduce this risk, Kuwabara and co-workers (2001) used omentum to surround the mediastinal tracheostomy. Gomes and colleagues (1987) described a mediastinal tracheostomy using an island pectoral flap that can be rotated and placed into midline position. For this anastomosis, the circular core of the island flap has the sutures placed through the airway and then to the skin level, similar to the method of heart valve placement. Orringer (1999) has updated his experience for this technique and now prefers a colon interposition graft to restore intestinal continuity and also recommends 5 cm as a minimal optimal length of remaining trachea. About 32% of patients require transposition of the tracheal stump beneath and to the right of the innominate artery to reduce tension (Fig. 75-4).
Tube Selection
The materials used to construct early tracheostomy tubes were relatively crude. Excess pressure on surrounding mucosa caused necrosis of the tracheal wall with later erosion into vital structures. Bernhard and co-workers (1985) noted that if a tracheostomy tube cuff exceeds capillary perfusion pressure (20 to 30 mm Hg), ischemic injury occurs. Grillo and associates (1971) demonstrated the importance of the low-pressure cuff with a clinical trial of 45 patients.
Tracheostomy tubes are made with or without cuffs. Generally, smaller tubes are cuffless because there is less need for a balloon seal in a small trachea. If a small tube is used in a large trachea for weaning purposes, the lack of a cuff reduces airway resistance. Tubes can also be fenestrated. Fenestrated tubes (internal cannulae removed) allow passage of air from the mouth into the upper trachea and then down through the fenestrations in the wall of the tracheostomy tube to reduce airway resistance. Hussey and Bishop (1996) recommend a fenestrated tracheostomy tube during weaning unless the tracheostomy tube is a No. 4 or smaller.
Tracheostomy tubes are constructed with a variety of materials from hard polyvinylchloride (PVC) or stainless steel to soft silicon or latex. Many larger tubes contain an inner cannula to facilitate connection to a positive-pressure ventilator. They also can be removed for easier and rapid cleaning of the tracheostomy. This is safer when patients require positive end-expiratory pressure (PEEP), as described by Heffner and co-workers (1986a).
Some tracheostomy tubes are constructed with self-expanding foam within the tracheal balloon. This foam is collapsed by vacuum during the insertion of the tube and then allowed to expand. The possible advantage of this type of construction is that overpressurization of the cuff is avoided. Harwood and associates (1992) developed a double-lumen tracheostomy tube for unusual cases requiring selective ventilation following single-lung transplantation.
Care should be taken to monitor cuff pressure because it can decrease by valve leakage or, as found by Stanley and Liu (1975), can occasionally increase during anesthesia by absorption of diffusible gases across the tracheostomy cuff. Unique patient anatomy is not always suited for a standard tracheostomy tube. Martin and Shapiro (1981) found it occasionally necessary to fabricate a tracheostomy tube by fusing existing tracheostomy tubes to extend their length. Alternatively, short wire-reinforced tubes designed for use during anesthesia can be inserted and sutured to the skin.
Pediatric Considerations in Tracheostomy
Pediatric tracheostomy traditionally carried a higher morbidity and mortality. Some of this risk is related to the technical and anatomic problems that occur in narrow airways that naturally occlude more easily. Mostly, the risks relate to the diseases that led to tracheostomy placement. Trauma and congenital obstructing lesions are the common indications
P.1025
rather than those for adult tracheostomy. Guillain-Barr syndrome was the predominant neurologic indication in patients who required prolonged ventilatory management in the series of Freezer and Robertson (1990) as well as that of Duncan and colleagues (1992). To some extent, materials used for tracheostomy and better monitoring have reduced complications, as surmised by Wetmore and co-workers (1999). The technique of tracheostomy in children is frequently a midline tracheotomy, although Rhee and associates (1996) prefer a superiorly based flap to reduce long-term complications. Historically, Johnston and co-workers (1967) and others abandoned the classic Bjork flap because it led to more complications in a narrow trachea.
Table 75-2. Pediatric Airway and Corresponding Tube Sizes | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Irving (1991) and Wyatt (1999) and their co-workers described the merits of different types of pediatric tracheostomy tubes and their indications based on patient size. Table 75-2 provides similar useful information pertaining to pediatric airway and tube selections. Guidelines for pediatric tracheostomy care documented by Sherman and colleagues (2000) and care plans reported by Duncan (1992) and Messineo (1995) and their co-workers account for more favorable outcomes in the use of chronic tracheostomy in children managed at home.
COMPLICATIONS
Complications of tracheostomy have been reported at relatively high rates since it became popular. In general, complications are grouped into those that occur early and those that occur late. Those that occur early usually relate to misadventures during the insertion process, and late complications often result from damage of or by the tracheostomy prosthesis.
Early Complications
Some of the early complications associated with tracheostomy are listed in Table 75-3. Bleeding from coagulopathy or damage to various vascular structures of the neck are common problems. Except as noted, most serious complications occur at rates of 1% to 2% or less and are influenced highly by operator experience and the use of preventive measures. Minor early complications, such as transient hypotension, oxygen desaturation, or nonsurgical bleeding, occur at rates of 6% to 10% when reviewing the work of Friedman and Mayer (1993), Nani (2002) and Van Heerbeek (1999) and their associates.
Although it is possible to lacerate an aberrant major vessel like the brachiocephalic artery, bleeding is more common from injuries of veins, the thyroid gland, or the inferior thyroid artery, as reported by Della Puppa and Pittoni (2001) and Tschang and Cramer (1977). In one series by Muhammad and co-workers (2000b), bleeding from unusual venous anatomy in percutaneous tracheostomy was about 5%. Ultrasound identification of vascular structures may reduce the risk for percutaneous bleeding complications.
Another unusual, but serious, early complication is laceration of the posterior wall of the trachea, as noted by Cantais (2002) and Fernandez (1996) and their associates. A forceful insertion of the tracheostomy tube into a friable airway may split the membranous trachea almost to the carina, as described by Jacobs and colleagues (1978) and Lin and co-workers (2000). Trottier and associates (1999) observed this complication at a high rate in patients undergoing
P.1026
percutaneous tracheostomy. Their experimental work suggested that the guidewire and the guiding catheter need to be stabilized firmly to avoid this complication.
Table 75-3. Complications of Tracheostomy | ||||
|---|---|---|---|---|
|
Other complications occur from the trauma of tracheostomy tube insertion. Airway obstructions resulted from tracheal cartilage avulsed during placement of the appliance, particularly during the percutaneous technique as reported by Kumar and co-workers (1997) and Sun (1995); bacteremia is also common, as discussed by Teoh and colleagues (1997).
Poor ventilation manifested by overt hypoxia, occult hypercarbia, or both occurred during placement of the tracheostomy tubes, as reported by Reilly and co-workers (1995). Aspiration of enteric contents may occur. In addition, Rogers and associates (2001) reported airway fires during tracheostomy.
Finally, tube displacement or incision of high-riding pleura caused pneumothorax or pneumomediastinum in the reports of Fernandez and co-workers (1996) and Heuer and Deller (1998). This complication is more common in emphysema patients and approached 5% of cases in the publication of Heffner and associates (1986b).
Although many of these complications are immediate, there are other early problems like delayed bleeding or tracheostomy tube dislodgment. Exploring the wound for bleeding may be difficult with the tube in place; self-extubation can occur and lead to fatal airway loss. A flap tracheotomy may reduce this complication if a tag suture is placed through the flap and the skin and left in place. Damaged or malfunctioning tubes discovered within 1 week of placement require special care. Young and co-workers (1996) placed a small tube (nasogastric or similar) through the tube to be changed to act as a stay catheter to exchange the new tube. It is a good idea to leave the insertion stylet and a replacement tube in an immediately accessible and obvious location so that a displaced tracheostomy tube can be guided back into the wound with reduced trauma.
Although there are different patterns of complications between a standard open tracheostomy and a percutaneous tracheostomy, the cricothyroidotomy also has special concerns. The cricothyroidotomy has a lower rate of incisional hemorrhage and pneumothorax. However, Heffner and co-workers (1986b) believe that because of its proximity to the larynx, there might be a higher rate of early glottic injury.
Variations in complication rates are related to methods used to place the tracheostomy. Therefore, early complications are reduced by improvements in the technique and greater experience of the surgical team. Long-term complications are influenced more by patient anatomy, materials design of the tracheostomy tube, and long-term surveillance by the monitoring staff.
Late Complications
Table 75-3 also lists common late complications. The anatomic relations depicted in Figure 75-5 elucidate the mechanisms for many of these possible complications.
Tracheal Stenosis
As described in a previous section, one of the earliest recognitions of tracheal stenosis was by Jackson (1923), who blamed too high tube placement. Alternatively, later investigators used cricothyroidotomy with good results. As critical care units, ventilators, and tracheostomies grew in popularity, many patients developed ischemia of the trachea from high-pressure cuffs used early in the experience. Many publications described the rationales for managing these complications. Some of these reports were from Johnston (1967), Geffin (1971), Lefemine (1973), Murphy (1966) and their colleagues, as well as Andrews and Pearson (1973) and Pearson and Andrews (1971). Grillo (1971) and Heffner (1986b) and their associates showed the beneficial effects of a low-pressure cuff that reduced this complication at least 10-fold.
However, despite the advent of a low-pressure balloon, chronic pressure on the trachea from forced angulations of a stiff tube or hyperinflation of the cuff can still lead to tracheal damage. Andrews (1971), Dane and King (1975), and
P.1027
Bryant (1971), Dunn (1974) and Eliachar (1987) and their colleagues described the incidence and pathogenesis of tracheal injury both clinically and experimentally. Also, devascularization and chemical erosion can occur near the cuff and lead to damage and long-term stricture formation.
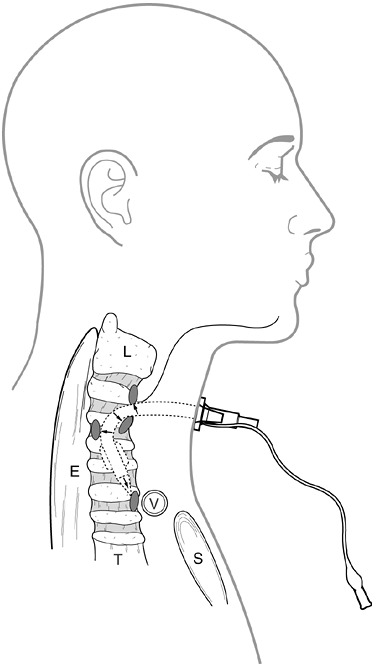 |
Fig. 75-5. Tracheostomy cannula pressure points that lead to erosion complications. E, esophagus; L, larynx; S, sternum; T, trachea; V, brachiocephalic vessel. Adapted from Miller FR, Eliachar I, Tucker HM: Technique, management, and complications of the long-term flap tracheostomy. Laryngoscope 105 :543, 1995. |
In compiled series, Arola (1981) found that tracheal stenoses occur in about 1% of patients who survive extubation. High percutaneous dilational tracheotomies were an extension from uncomplicated series of cricothyroidotomies. However, large recent series from Briche (2001) and Rosenbower (1998) and their co-workers do show symptomatic tracheal stenoses that require therapy after percutaneous tracheotomy. For most of these series, the incidence remains about 1% to 2%, as in the report from Norwood and colleagues (2000).
The best method for avoiding tracheal strictures is prevention. It is best to avoid tube anchoring methods or ventilator equipment connections that cause the prosthesis to press steadily against the wall of the trachea. Also, avoiding especially large tracheostomy tubes and reducing tracheal exposure to other noxious compounds, such as aspirated enteric contents is important. This prevents mucosal injury that leads to stricture, as found by Leverment and Pearson (1977). There may be other unknown or difficult to quantify factors that lead to variations in stenosis rates for both open and percutaneous tracheostomy noted by Dane and King (1975) and Gysin and associates (1999).
Symptoms of tracheal stenosis include dyspnea on exertion and inability to clear secretions once the tracheal lumen has been reduced 75%. Stridor occurs with a dimension of 5 mm according to Heffner and associates (1986b). When tracheal stenosis is suspected, the diagnosis can be confirmed by computed tomography (CT) scanning or direct observation by endoscopy. Callanan and co-workers (1997) found magnetic resonance (MR) imaging to be a very effective tool in the diagnosis of posttracheotomy stenosis. Asymptomatic airway changes may occur in up to 40% of patients, as studied by Gysin and colleagues (1999) and Walz and associates (1998).
The treatment of severe tracheal stenosis may require a segmental tracheal resection up to 50% of its length with primary end-to-end anastomosis. Tracheal dilation can be used for emergency situations or patients with prohibitive risk, but it is not preferred therapy in patients with an anticipated long-term survival. This is because the dilation causes enough reaction around the trachea to complicate later operations. Occasionally, lasers can appropriately ablate limited fibrotic stenoses of the trachea. However, in cases in which there are long circumferential lesions with associated tissue reactions, Heffner and co-workers (1986b) found laser therapies less effective.
Airway Fistulae
Any firm, in-dwelling prosthesis can cause tissue necrosis with fistulization over time. The most dreaded is a vascular fistula most commonly with the brachiocephalic (innominate) artery. Heffner and co-workers (1986b) reported tracheoinnominate fistulae at a rate of 2% with tracheostomy, but this is less common in modern series. The fistula can occur days to months after the placement of the tracheostomy. The etiology is now more likely due to chronic tracheostomy tip erosion through the wall of the airway rather than from balloon necrosis. A sentinel-bleeding event occurs hours to days before massive hemorrhage. First aid for this condition can be as simple as overinflating the tracheostomy balloon if the balloon is what actually caused the fistula. Unfortunately, it is more likely that another part of the airway device will have caused the fistula. The wound may need to be expanded sharply so that a finger can be placed into the upper airway to compress the innominate artery against the back of the sternum for control. It may be necessary to remove the tracheostomy tube and perform a transoral intubation with a small endotracheal tube. Or, a small endotracheal tube placed through the tracheostomy and beside the finger can provide ventilatory support while the vessel is compressed. Overall survival is quite poor and is in the range of 25%. Median sternotomy and division of the brachiocephalic artery accomplish definitive surgical management. For most patients, this does not result in a neurologic defect; thus, vascular reconstruction is not needed. Intravascular surgical options for this complication have not been reported but may need to be considered in the future as first aid or definitive management depending on patient comorbidity.
The tip of the tracheostomy tube may erode anteriorly into a great vessel, and the tube may place pressure posteriorly to create a tracheoesophageal fistula. The usual mechanism is erosion by the tracheostomy cuff, but a right angle of the tube can bow against the posterior wall of the trachea, causing undue pressure. This occurs more often in patients who received irradiation to the region, have poorly fitting tracheostomy appliances, or have other devices like nasogastric tubes that create pressure points for erosion. Diagnosis of a tracheoesophageal fistula should be suspected if there are more copious secretions or the presence of bilious or other enteric secretions in the tracheal aspirate. The demonstration of the fistula can be difficult even with the use of airway or upper esophageal endoscopy. Contrast often has to be used below the upper esophageal sphincter or within the airway at the site of the presumed fistula (if a cuffed endotracheal tube protects the distal airway). Even with this, the diagnosis can be missed, and Arola (1981) found it only at autopsy in three patients in a large series of 794 patients. If the diagnosis is recognized, fistula repair is managed through a cervical incision when the patient is stable.
Another problem is a cutaneous fistula, reported by Hughes and associates (1971), that persists after tracheostomy removal because of skin growth along the tube tract. Tracheostomy tubes formed fistulae, as reported by Mulder and co-workers (1972) into the pleural spaces, by Lotan and co-workers (1977) into the mediastinal tissues, and by Posthumus and Peirce (1978), even into the pericardium. Like other fistulae, removal of the tract, repair of the trachea,
P.1028
and preferably a buttress of intervening healthy tissue such as strap muscle are ideal.
Other Types of Complications
There are reports of many unusual complications with tracheostomy. One example is obstruction for causes other those that have been noted. This can occur from herniation and overinflation of the tracheostomy tube balloon, as described by Sinfield and associates (1989), as well as obstruction by portions of the tracheostomy appliance that occur by dislodgment or by fracture, as noted by Johnson and associates (1977) as well as by Krempl and Otto (1999) and Lawton and Abadee (1987). Rigg and Edmondson (1995) found that malposition caused delayed weaning because the tracheal wall effaced the end of the tracheostomy tube. Percutaneous dilation tracheostomy kits, detailed by Ciaglia (1998) and Pinder and co-workers (2000), contain multiple objects that are introduced into the trachea that could result in a foreign body. Granulomas occur in the airway as a result of foreign body reaction to the tracheostomy tube or other irritants that pool there. Siddharth and Mazzarella (1985) suggested that this may occur even more commonly with fenestrated tracheostomy tubes. Madden and colleagues (2001) treated such granulation tissue with the yttrium-aluminum-garnet (YAG) laser. Finally, 1% to 5% of patients develop delayed pneumothorax or subcutaneous emphysema, according to Heffner and co-workers (1986b).
Infection is another well-recognized complication of tracheostomy, a procedure that opens a space contaminated or colonized with bacteria. For instance, peritracheal abscesses occurring after this operation were found by Cole and Kerr (1983). Staphylococci and hardy gram-negative organisms were cultured commonly from stomas in series by Andrews and Pearson (1973) as well as by Espinoza (1974), Johnston (1967) and Westphal (1999) and their colleagues. Furthermore, Mohammedi and associates (1997) found that cellulitis can be a problem after open or percutaneous tracheostomy.
Occasionally, patients with tracheostomy tubes develop devastating necrotizing infections of the trachea. These require conversion to oral tracheal intubation and wide d bridement until adequate granulation tissue occurs to allow replacement of tracheostomy appliance. Snow and co-workers (1981) believe this complication is due to inadequate stomal hygiene, inadequate treatment of bronchopulmonary infection, and occasionally necrosing suture fixation to the surrounding skin.
Placing a tracheostomy wound near a recent operative space is hazardous. Easy communication with the mediastinum, such as after recent open-heart surgery, is both theoretically possible and certainly has occurred in several well-documented cases, such as that described by Andrews and Pearson (1973). The risk may be as high as 8.6%, but Curtis and co-workers (2001) found it is difficult to predict a safe time interval before placing a tracheostomy. It appears possible for patients to develop mediastinitis even without a recent median sternotomy. This occurred once after percutaneous tracheostomy, leading Maeda and co-workers (2002) to propose extending the skin incision around the cannula to allow the tracheal contents free egress to the skin rather than into the mediastinum.
In contrast, Stamenkovic and colleagues (2000) did not demonstrate a relationship between early tracheostomy and median sternotomy. In addition, Byhahn and associates (2000c) showed there was no cross-contamination of percutaneous tracheostomy contaminants even for those patients that developed mediastinal wound infections.
Vocal cord fusion and obstructive tracheal granulomas are relatively more common in children than in adults, according to Gaudet and co-workers (1978). Finally, Papakostas and colleagues (2000) found that a tracheostomy could cause potentially life-threatening ballooning of the airway over time.
POSTOPERATIVE CARE
Complications from tracheostomy can be reduced with good postoperative care. The considerations and guidelines for tracheostomy management have been outlined by the Society of Otorhinolaryngology and Head-Neck Nurses (1994) and Godwin and Heffner (1991). Many preventive methods involve improved communications with patients and planning for success by using enteral nutrition and weaning as part of an institutional protocol rather than individual practice. Also, preparation for adverse reactions after airway decannulation is a good preventive approach. A useful drill is planning for a dislodged tracheostomy tube. Immediate access to replacement tubes and methods to facilitate transfer are important, such as using the changing tube described by Young and associates (1996). Individuals who are not health care professionals and have to care for patients with home tracheostomy have significant strain. These issues need to be considered before elective tracheostomy and during discharge planning, according to Rossi Ferrario and co-workers (2001).
Physiologic Changes Associated with Tracheotomy
A chronic tracheostomy cuff alters the function of the esophagus and affects swallowing. Leverment and co-workers (1976) showed that the pressures in the esophagus increased at the level of the cuff below the pharyngoesophageal junction and that there was also impaired relaxation of the upper esophageal sphincter.
Typically, there is increased work of breathing as well as airway resistance. Mullins and colleagues (1993) found that tubes that most closely simulate normal upper airway resistance in adults are sizes 8 and 10, and for neonates, size 0.
P.1029
Haberthur and associates (1999) showed that the work of breathing imposed by the tracheostomy tube is related highly to the respiratory flow rate. A rigid, rather than flexible, tracheostomy tube reduces the work of breathing when respiratory rate increases, as identified by the studies of Davis and co-workers (1999). Cowan and co-workers (2001) showed that removing the inner cannula reduces impedance as well as the work of breathing. For patients who are already receiving mechanical ventilation, Lin and co-workers (1999) found that the conversion from a standard endotracheal tube to a tracheostomy affects the respiratory function little, except to reduce peak inspiratory pressure.
Increased iodine 131 (131I) uptake near the tracheostomy site on nuclear medicine imaging was found by Kirk and Schulz (1984). This is possibly from inflammation and can be misleading. Ain and Shih (1994) found that the false uptake caused by tracheostomy can be discriminated by thallium 20 (20Tl) imaging.
Tracheostomy bypasses the normal humidification effects of the upper airway. It is best to use a humidified air mixture for patients who are in intensive care unit settings. Tsuda and associates (1977) found that 100% saturation between the temperatures of 25 and 30 C is optimal. In addition, tracheostomy tubes are placed for assisting with bronchopulmonary toilet. If ventilatory support is not needed, a small tracheostomy tube is sufficient to allow suctioning with soft cannulae. Occasionally, the use of a soft angled-tip catheter is useful for selecting one bronchus or the other. It may also be less traumatic for patients who develop bleeding during suctioning.
Aspiration and Disorders in Swallowing
The presence of a tracheotomy tube almost always disturbs sensitive assessments of swallowing. DeVita and Spierer-Rundback (1990) found that all patients had at least one of the 11 known swallowing defects determined by videofluoroscopy. An intact gag reflex does not ensure protection against the aspiration. In studies of patients with head and neck malignancies, 33% of those with tracheostomy developed tracheal aspiration, as demonstrated by scintigraphic studies performed by Muz and co-workers (1994). Schonhofer and colleagues (1999) noted similar findings in patients receiving prolonged ventilation with tracheostomy. Protection is impaired in that the vocal cords do not close as long after water swallows as compared with that seen in normal volunteers studied by Shaker and co-workers (1995). It is unclear why the tracheostomy, per se, causes these defects; however, Costa (1996) believes it may result from laryngeal fixation to skin.
Attempts to restore normal physiology may reduce clinical aspiration. Investigators have tried speaking valves for patients weaning from the ventilator. In many cases, the speaking valve reduced or limited aspiration during swallowing, as shown by Dettelbach (1995) and Elpern (2000) and their colleagues. Zajac and co-workers (1999) suggested that the moderate increased resistance offered by these speaking valves is primarily physiologic. In addition, the speaking valve restored verbal communication skills, facilitated care, and improved the mood of patients, as observed by Passy and co-workers (1993). In addition to speaking valves, some investigators recreate speech in patients with tracheostomy by using a modified tube that allows humidified compressed air to flow above the tracheostomy balloon past the vocal cords. Also, Heffner and associates (1986b) showed how sound-generating tubes placed into the nasopharynx can create tones modifiable by the patient to produce speech.
Tube Management
Concerns regarding tracheostomy tube construction have been noted previously. Surveillance of older cuff pressures by Ching and colleagues (1971) found some greater than 210 mm Hg. One of the pivotal studies showing the benefits of the low-pressure cuff was by Grillo and co-workers (1971). Before then, others tried to reduce chronic cuff trauma, including Rainer and Sanchez (1970), who inflated the tracheostomy cuffs in synchrony with inspiration.
Chronic tracheal intubation leads to changes in the bacterial flora. Although cross-contamination of airway equipment can cause infection, it appears that infection is more of a host phenomenon. Tracheostomy causes greater adherence of bacteria to upper airway mucosa; however, Niederman and co-workers (1984a, 1984b) showed that poor nutritional status is a more likely cause of lower airway colonization. They and Tano and colleagues (1992) also showed that Pseudomonas species favors colonization of the lower respiratory tract in patients with tracheostomy. The etiology of the lung disease (i.e., whether restrictive or obstructive) does not appear to change the pattern of infecting organisms, according to the work of Lusuardi and co-workers (2000). Klastersky and co-workers (1974) and others tried administering intratracheal antibiotics, but this was not successful enough to warrant broader implementation.
Tracheostomy Weaning Considerations
Patients improving from respiratory failure achieve criteria similar to that associated with successful oral endotracheal extubation. Although the methods of weaning are not standardized and are of some controversy, it is clear by Doerksen and associates' (1994) work that a systematic approach to tracheostomy weaning is better than random or variable methodologies. In addition to systematic weaning approaches, protocols for home tracheostomy care are highly useful. Wilson and Malley (1990) found that competence demonstration by family members and all other caregivers in the proper use of the equipment is highly desirable.
P.1030
When positive-pressure ventilation is no longer needed and the patient is doing a lot of spontaneous upper airway breathing, the patient should be converted to a fenestrated tracheostomy cannula. The fenestrations permit gas flow with less impedance. When the cannula is less than No. 4, then resistance is no longer an issue. For patients difficult to wean because of neuromuscular weakness, the use of cuffless tubes and intermittent positive-pressure breathing is a useful method, according to Bach and Alba (1990). Some practitioners prefer to cap a No. 4 metal or plastic cannula and leave this in place for some time until it is clear that the patient will not require reintubation. Miller (1995) and Heffner (1986a) and their colleagues found that other prostheses (such as cannula buttons) are better because they do not protrude as far into the tracheal lumen.
RESULTS AND PROGNOSES OF PATIENTS WHO REQUIRE TRACHEOSTOMY
One of the first considerations in comparing tracheostomy outcomes is the controversy of whether tracheostomy is really necessary. Stauffer and co-workers (1981) did not show much difference in the airway changes between patients who had endotracheal intubation versus those who had tracheostomy. Whereas, Hazard and co-workers (1988) and others have shown that tracheostomy reduces the duration of mechanical support. In addition, newer noninvasive means of respiratory support, such as external positive-pressure ventilation reported by Bach and associates (1993) or nasally applied bidirectional positive airway pressure (BIPAP), may reduce the need for chronic intubation.
Although open tracheostomy almost always achieves airway access in elective situations, Heuer and Deller (1998), as well as Cantais (2002), Ivatury (1992), Kearney (2000) and Van Heerbeek (1999) and their associates, found that percutaneous tracheostomy failed or required conversion to standard techniques in a range of 0% to 10%. The higher failure rate was observed at an institution that performed more cases in urgent or emergent situations. Translaryngeal percutaneous method may also have a higher failure rate, as noted by Cantais and co-workers (2002).
Death during tracheostomy is relatively uncommon. The contemporary reports of Friedman and Mayer (1993), as well as reports of Beiderlinden (2002), Cantais (2002), Hinerman (2000), Ivatury (1992), Kearney (2000), Lim (2000), Melloni (2002), Toursarkissian (1994), Van Heerbeek (1999) and Walz (1998) and their co-workers, often showed a 0% procedural mortality (0% to 1.6%).
Traditionally, outcomes for pediatric tracheostomy had higher associated complications and mortality rates from clogging because of the smaller airway. However, Wetmore and associates (1982) noted that the long-term mortality rates for both pediatric and adult tracheostomy are related more to the underlying diseases than the procedures. For instance, the mortality rate for AIDS patients is 77% in Flum and co-workers' (1998) series. Mortality rates vary widely (15.4% to 52%) and depend on the patient population, as reported by Divisi (2002), Fernandez (1996), Hinerman (2000), Ivatury (1992) and Mittendorf (2002) and their coinvestigators. In some elderly groups, the use of tracheostomy has been questioned by Dewar (1999) and Kurek (1997) and their associates because many patients die or are placed into chronic health care facilities with a poor quality of life. In one study of intensive care unit (ICU) patients, tracheostomy was used in patients with anticipated good prognoses after the inciting diseases had resolved. Accordingly, Kollef and co-workers (1999) found a higher mortality rate in ICU patients in whom pessimism led to avoidance of tracheostomy (26.4% versus 13.7%).
Table 75-4 shows a comparison of surgical and various percutaneous tracheostomy complication rates. A metaanalysis by Freeman and colleagues (2000) of these and other trials suggests a slight edge for percutaneous tracheostomy because of ease of performance and perhaps less bleeding and infection.
Insertion time comparisons for percutaneous tracheostomy (antegrade dilator, antegrade dilating forceps, and translaryngeal) yield a similar median of 13 minutes with a possible slight speed advantage for the dilating forceps technique. The series reviewed were those by Friedman and Mayer (1993) and Cantais (2002), Cobean (1996), Freeman (2001), Heikkinen (2000), Holdgaard (1998), Kearney (2000), McHenry (1997), Melloni (2002) and Van Heurn (2001) and their associates. The median time for standard open tracheostomy was 31 minutes, but Heikkinen (2000) and Holdgaard (1998) and their colleagues achieved the same time as percutaneous methods.
In addition, the percutaneous treatments may be less expensive. Cobean (1996), Fernandez (1996), Freeman (2001), Heikkinen (2000), McHenry (1997) and Westphal (1999) and their coinvestigators found that the percutaneous method was a median of $277 cheaper (range, $193 to $1,645). Grover and co-workers (2001) were unable to do open tracheostomy with less expense.
Review of the contradictory research leads one to conclude that the difference between these studies is highly dependent on factors such as surgeon expertise and other safety methods employed during the tube placement and postoperative care. For instance, there is considerable variation in outcomes of two types of antegrade percutaneous tracheostomy techniques reported by Anon (2000) and Nates (2000) and their associates. The variations among many of the studies can be explained by the variations in placement time and other resources used.
If tracheostomy is used as part of a process to improve overall care (such as its early use after blunt trauma), there is a net gain and possibly less ICU time, as reported by Armstrong (1998) and Freeman (2001) and their co-workers. Moreover, the early use of percutaneous tracheostomy by Hubner (1998) and Wagner (1998) and their associates for certain cardiac surgical patients also appeared favorable.
Halfpenny and McGurk (2000) suggested that patients who received preoperative radiation therapy are more likely
P.1031
to have tracheostomy-related complications. Furthermore, tracheostomy complications initiate other complications. For patients with active central nervous system lesions in whom tracheostomy is needed, Stocchetti and co-workers (2000) found that all the different tracheostomy techniques are relatively safe, with similar instances of increased intracranial pressure.
Table 75-4. Comparisons of Approaches to Tracheostomy | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
REFERENCES
Abdel Rahim AA, et al: Respiratory complications after thyroidectomy and the need for tracheostomy in patients with a large goitre. Br J Surg 86 :88, 1999.
Ahmed Z, Mohyuddin Z: Management of flail chest injury: internal fixation versus endotracheal intubation and ventilation. J Thorac Cardiovasc Surg 110 :1676, 1995.
P.1032
Ain KB, Shih WJ: False-positive I-131 uptake at a tracheostomy site. discernment with Tl-201 imaging. Clin Nucl Med 19 :619, 1994.
Andrews MJ: The incidence and pathogenesis of tracheal injury following tracheostomy with cuffed tube and assisted ventilation. Analysis of a 3-year prospective study. Br J Surg 58 :749, 1971.
Andrews MJ, Pearson FG: Incidence and pathogenesis of tracheal injury following cuffed tube tracheostomy with assisted ventilation: analysis of a two-year prospective study. Ann Surg 173 :249, 1971.
Andrews MJ, Pearson FG: An analysis of 59 cases of tracheal stenosis following tracheostomy with cuffed tube and assisted ventilation, with special reference to diagnosis and treatment. Br J Surg 60 :208, 1973.
Anon JM, et al: Percutaneous tracheostomy: comparison of Ciaglia and Griggs techniques. Crit Care 4 :124, 2000.
Armstrong PA, McCarthy MC, Peoples JB: Reduced use of resources by early tracheostomy in ventilator-dependent patients with blunt trauma. Surgery 124 :763,1998.
Arola MK: Tracheostomy and its complications. A retrospective study of 794 tracheostomized patients. Ann Chir Gynaecol 70 :96, 1981.
Atweh NA, et al: Dilatational percutaneous tracheostomy: modification of technique. J Trauma 47 :142, 1999.
Bach JR, Alba AS: Tracheostomy ventilation. A study of efficacy with deflated cuffs and cuffless tubes. Chest 97 :679, 1990.
Bach JR, Alba AS, Saporito LR: Intermittent positive pressure ventilation via the mouth as an alternative to tracheostomy for 257 ventilator users. Chest 103 :174, 1993.
Barba CA, et al: Bronchoscopic guidance makes percutaneous tracheostomy a safe, cost-effective, and easy-to-teach procedure. Surgery 118 : 879, 1995.
Bass JW: Tracheostomy for acute epiglottitis. N Engl J Med 298 :342, 1978.
Beatrous WP: Tracheostomy (tracheotomy). Its expanded indications and its present status. Based on an analysis of 1,000 consecutive operations and a review of the recent literature. Laryngoscope 78 :3, 1968.
Beiderlinden M, et al: Complications of bronchoscopically guided percutaneous dilational tracheostomy: beyond the learning curve. Intensive Care Med 28 :59, 2002.
Bernhard WN, et al: Intracuff pressures in endotracheal and tracheostomy tubes: related cuff physical characteristics. Chest 87 :720, 1985.
Bishop MJ: Mechanisms of laryngotracheal injury following prolonged tracheal intubation. Chest 96 :185, 1989.
Bishop MJ, et al: Laryngeal injury in a dog model of prolonged endotracheal intubation. Anesthesiology 62 :770, 1985.
Bjork VO: Partial resection of the only remaining lung with the aid of respiratory treatment. J Thorac Cardiovasc Surg 39 :179, 1960.
Brantigan CO, Grow JB: Cricothyroidotomy: elective use in respiratory problems requiring tracheotomy. J Thorac Cardiovasc Surg 71 :72, 1976.
Briche T, Le Manach Y, Pats B: Complications of percutaneous tracheostomy. Chest 119 :1282, 2001.
Brook AD, et al: Early versus late tracheostomy in patients who require prolonged mechanical ventilation. Am J Crit Care 9 :352, 2000.
Bryant LR, Trinkle JK, Dubilier L: Reappraisal of tracheal injury from cuffed tracheostomy tubes. Experiments in dogs. JAMA 215 :625, 1971.
Byhahn C, et al: Percutaneous tracheostomy: Ciaglia Blue Rhino versus the basic Ciaglia technique of percutaneous dilational tracheostomy. Anesth Analg 91 :882, 2000a.
Byhahn C, et al: Translaryngeal tracheostomy: two modified techniques versus the basic technique early experience in 75 critically ill adults. Intensive Care Med 26 :457, 2000b.
Byhahn C, et al: Early percutaneous tracheostomy after median sternotomy. J Thorac Cardiovasc Surg 120 :329, 2000c.
Calhoun KH, et al: Management of the thyroid isthmus in tracheostomy: a prospective and retrospective study. Otolaryngol Head Neck Surg 111 : 450, 1994.
Callanan V, et al: The use of magnetic resonance imaging to assess tracheal stenosis following percutaneous dilatational tracheostomy. J Laryngol Otol 111 :953, 1997.
Cantais E, et al: Percutaneous tracheostomy: prospective comparison of the translaryngeal technique versus the forceps-dilational technique in 100 critically ill adults. Crit Care Med 30 :815, 2002.
Cantrell RW, Bell RA, Morioka WT: Acute epiglottitis: intubation versus tracheostomy. Laryngoscope 88 :994, 1978.
Ching NP, et al: The contribution of cuff volume and pressure in tracheostomy tube damage. J Thorac Cardiovasc Surg 62 :402, 1971.
Ciaglia P: Airway obstruction with percutaneous tracheostomy. Chest 113 : 849, 1998.
Ciaglia P, Firsching R, Syniec C: Elective percutaneous dilatational tracheostomy. A new simple bedside procedure: preliminary report. Chest 87 :715, 1985.
Ciaglia P, Graniero KD: Percutaneous dilatational tracheostomy. Results and long-term follow-up. Chest 101 :464, 1992.
Cobean R, et al: Percutaneous dilatational tracheostomy. A safe, cost-effective bedside procedure. Arch Surg 131 :265, 1996.
Cole AG, Kerr JH: Paratracheal abscess after tracheostomy. Intensive Care Med 9 :345, 1983.
Costa MM: Swallowing defects determined by tracheostomy. Arq Gastroenterol 33 :124, 1996.
Cothren C, et al: Evaluation of a new technique for bedside percutaneous tracheostomy. Am J Surg 183 :280, 2002.
Cowan T, et al: Effect of inner cannula removal on the work of breathing imposed by tracheostomy tubes: a bench study. Respir Care 46 :460, 2001.
Curtis JJ, et al: Tracheostomy: a risk factor for mediastinitis after cardiac operation. Ann Thorac Surg 72 :731, 2001.
D'Amelio LF, et al: Tracheostomy and percutaneous endoscopic gastrostomy in the management of the head-injured trauma patient. Am Surg 60 :180, 1994.
Dane TE, King EG: A prospective study of complications after tracheostomy for assisted ventilation. Chest 67 :398, 1975.
Davis K Jr, et al: Changes in respiratory mechanics after tracheostomy. Arch Surg 134 :59, 1999.
Della Puppa A, Pittoni G: Inferior thyroid artery bleeding: a life-threatening complication of non-surgical tracheostomy. Minerva Anestesiol 67 : 483, 2001.
Dettelbach MA, et al:. Effect of the Passy-Muir Valve on aspiration in patients with tracheostomy. Head Neck 17 :297, 1995.
DeVita MA, Spierer-Rundback L: Swallowing disorders in patients with prolonged orotracheal intubation or tracheostomy tubes. Crit Care Med 18 :1328, 1990.
Dewar DM, et al: Patterns in costs and outcomes for patients with prolonged mechanical ventilation undergoing tracheostomy: an analysis of discharges under diagnosis-related group 483 in New York State from 1992 to 1996. Crit Care Med 27 :2640, 1999.
Dexter TJ: A cadaver study appraising accuracy of blind placement of percutaneous tracheostomy. Anaesthesia 50 :863, 1995.
Divisi D, et al: Translaryngeal tracheostomy using the Fantoni technique: report of 104 cases. Ann Chir 127 :130, 2002.
Doerksen K, Ladyshewsky A, Stansfield KA: Comparative study of systemized vs. random tracheostomy weaning. Axone 16 :5, 1994.
Dosemeci L, et al: The use of the laryngeal mask airway as an alternative to the endotracheal tube during percutaneous dilatational tracheostomy. Intensive Care Med 28 :63, 2002.
Duncan BW, et al: Tracheostomy in children with emphasis on home care. J Pediatr Surg 27 :432, 1992.
Dunn CR, Dunn DL, Moser KM: Determinants of tracheal injury by cuffed tracheostomy tubes. Chest 65 :128, 1974.
Dye JP: Living with a tracheostomy for sleep apnea. N Engl J Med 308 : 1167, 1983.
Eliachar I, et al: Planning and management of long-standing tracheostomy. Otolaryngol Head Neck Surg 97 :385, 1987.
Elpern EH, et al: Effect of the Passy-Muir tracheostomy speaking valve on pulmonary aspiration in adults. Heart Lung 29 :287, 2000.
Espinoza H, et al: Clinical and immunologic response to bacteria isolated from tracheal secretions following tracheostomy. J Thorac Cardiovasc Surg 68 :432, 1974.
Fantoni A, Ripamonti DA: Non-derivative, non-surgical tracheostomy: the translaryngeal method. Intensive Care Med 23 :386, 1997.
Fernandez L, et al: Bedside percutaneous tracheostomy with bronchoscopic guidance in critically ill patients. Arch Surg 131 :129, 1996.
Fischler L, et al: Prevalence of tracheostomy in ICU patients: a nation-wide survey in Switzerland. Intensive Care Med 26 :1428, 2000.
Flum DR, Bholat OS, Wallack MK: The role of tracheostomy in acquired immunodeficiency syndrome. Ann Thorac Surg 64 :982, 1997.
Flum DR, et al: Bedside percutaneous tracheostomy in acquired immunodeficiency syndrome. Am Surg 64 :444, 1998.
Freeman BD, et al: A meta-analysis of prospective trials comparing percutaneous and surgical tracheostomy in critically ill patients. Chest 118 : 1412, 2000.
Freeman BD, et al: A prospective, randomized study comparing percutaneous with surgical tracheostomy in critically ill patients. Crit Care Med 29 :926, 2001.
P.1033
Freezer NJ, Beasley SW, Robertson CF: Tracheostomy. Arch Dis Child 65 :123, 1990.
Freezer NJ, Robertson CF: Tracheostomy in children with Guillain Barr syndrome. Crit Care Med 18 :1236, 1990.
Friedman Y, Mayer AD: Bedside percutaneous tracheostomy in critically ill patients. Chest 104 :532, 1993.
Frost EA: Tracing the tracheostomy. Ann Otol Rhinol Laryngol 85 :618, 1976.
Frova G, Quintel MA: New simple method for percutaneous tracheostomy: controlled rotating dilation. A preliminary report. Intensive Care Med 28 :299, 2002.
Fuhrman TM, Farina RA: Elective tracheostomy for a patient with a history of difficult intubation. J Clin Anesth 7 :250, 1995.
Gaudet PT, et al: Pediatric tracheostomy and associated complications. Laryngoscope 88 :1633, 1978.
Geffin B, et al: Stenosis following tracheostomy for respiratory care. JAMA 216 :1984. 1971.
Godwin JE, Heffner JE: Special critical care considerations in tracheostomy management. Clin Chest Med 12 :573, 1991.
Gomes MN, Kroll S, Spear SL: Mediastinal tracheostomy. Ann Thorac Surg 43 :539, 1987.
Griggs WM, Myburgh JA, Worthley LI: A prospective comparison of a percutaneous tracheostomy technique with standard surgical tracheostomy. Intensive Care Med 17 :261, 1991.
Grillo HC, et al: Low-pressure cuff for tracheostomy tubes to minimize tracheal injury. A comparative clinical trial. J Thorac Cardiovasc Surg 62 :898, 1971.
Grover A, et al: Open versus percutaneous dilatational tracheostomy: efficacy and cost analysis. Am Surg 67 :297, 2001.
Gurkin SA, et al: Indicators for tracheostomy in patients with traumatic brain injury. Am Surg 68 :324, 2002.
Gysin C, et al: Percutaneous versus surgical tracheostomy: a double-blind randomized trial. Ann Surg 230 :708, 1999.
Haberthur C, et al: Additional inspiratory work of breathing imposed by tracheostomy tubes and non-ideal ventilator properties in critically ill patients. Intensive Care Med 25 :514, 1999.
Halfpenny W, McGurk M: Analysis of tracheostomy-associated morbidity after operations for head and neck cancer. Br J Oral Maxillofac Surg 38 :509, 2000.
Harwood RJ, et al: Use of a double-lumen tracheostomy tube after single lung transplantation. J Thorac Cardiovasc Surg 103 :1224, 1992.
Hazard P, Jones C, Benitone J: Comparative clinical trial of standard operative tracheostomy with percutaneous tracheostomy. Crit Care Med 19 :1018, 1991.
Hazard PB, et al: Bedside percutaneous tracheostomy: experience with 55 elective procedures. Ann Thorac Surg 46 :63, 1988.
Heffner JE, Miller KS, Sahn SA: Tracheostomy in the intensive care unit. Part 1: indications, technique, management. Chest 9 0:269, 1986a.
Heffner JE, Miller KS, Sahn SA: Tracheostomy in the intensive care unit. Part 2: complications. Chest 90 :430, 1986b.
Heikkinen M, Aarnio P, Hannukainen J: Percutaneous dilational tracheostomy or conventional surgical tracheostomy? Crit Care Med 28 :1399, 2000.
Heuer B, Deller A: Early and long-term results of percutaneous dilatation tracheostomy (PDT Ciaglia) in 195 intensive care patients. Anasthesiol Intensivmed Notfallmed Schmerzther 33 :306, 1998.
Hinerman R, Alvarez F, Keller CA: Outcome of bedside percutaneous tracheostomy with bronchoscopic guidance. Intensive Care Med 26 :1850, 2000.
Hirota W, et al: Lidocaine added to a tracheostomy tube cuff reduces tube discomfort. Can J Anaesth 47 :412, 2000.
Holdgaard HO, et al: Percutaneous dilatational tracheostomy versus conventional surgical tracheostomy: a clinical randomised study. Acta Anaesthesiol Scand 42 :545, 1998.
Hubner N, et al: Percutaneous dilatational tracheostomy done early after cardiac surgery: outcome and incidence of mediastinitis. Thorac Cardiovasc Surg 46 :89, 1998.
Hughes M, Kirchner JA, Branson RJ: A skin-lined tube as a complication of tracheostomy. Arch Otolaryngol 94 :568, 1971.
Hussey JD Bishop MJ: Pressures required to move gas through the native airway in the presence of a fenestrated vs a nonfenestrated tracheostomy tube. Chest 110 :494, 1996.
Irving RM, et al: A guide to the selection of paediatric tracheostomy tubes. J Laryngol Otol 105 :1046, 1991.
Ivatury R, et al: Percutaneous tracheostomy after trauma and critical illness. J Trauma 32 :133, 1992.
Izumi K, et al: Analysis of tracheostomy for patients after thoracic esophageal cancer resection. Kyobu Geka 48 :811, 1995.
Jackson C: High tracheotomy and other errors: the chief causes of chronic laryngeal stenosis. Surg Gynecol Obstet 32 :1923, 1923.
Jacobs JR, et al: Posterior tracheal laceration: a rare complication of tracheostomy. Laryngoscope 88 :1942, 1978.
James EC, Harris SS, Dillenburg CJ: Tracheal stenosis: an unusual presenting complication of idiopathic fibrosing mediastinitis. J Thorac Cardiovasc Surg 80 :410, 1980.
Johnson JT, Maloney RW, Cummings CW: Tracheostomy tube: cuff obstruction. JAMA 238 :211, 1977.
Johnston JB, Wright JS, Hercus V: Tracheal stenosis following tracheostomy. A conservative approach to treatment. J Thorac Cardiovasc Surg 53 :206, 1967.
Kanner RE: Bilateral vocal cord paralysis for 26 years with respiratory failure. Timing of restoration of tidal volume and serum electrolytes after tracheostomy. Chest 84 :304, 1983.
Kearney PA, et al: A single-center 8-year experience with percutaneous dilational tracheostomy. Ann Surg 231 :701, 2000.
Kirk GA, Schulz EE: Post-laryngectomy localization of I-131 at tracheostomy site on a total body scan. Clin Nucl Med 9 :409, 1984.
Klastersky J, et al: Endotracheally administered gentamicin for the prevention of infections of the respiratory tract in patients with tracheostomy: a double-blind study. Chest 65 :650, 1974.
Kollef MH, Ahrens TS, Shannon W: Clinical predictors and outcomes for patients requiring tracheostomy in the intensive care unit. Crit Care Med 27 :1714, 1999.
Krempl GA, Otto RA: Fracture at fenestration of synthetic tracheostomy tube resulting in a tracheobronchial airway foreign body. South Med J 92 :526, 1999.
Kumar BN, Walsh RM, Courteney-Harris RG: Laryngeal foreign body: an unusual complication of percutaneous tracheostomy. J Laryngol Otol 111 :652, 1997.
Kurek CJ, et al: Clinical and economic outcome of patients undergoing tracheostomy for prolonged mechanical ventilation in New York State during 1993: analysis of 6,353 cases under diagnosis-related group 483. Crit Care Med 25 :983, 1997.
Kuwabara Y, et al: Use of omentum for mediastinal tracheostomy after total laryngoesophagectomy. Ann Thorac Surg 71 :409, 2001.
Lawn ND, Wijdicks EF: Tracheostomy in Guillain-Barr syndrome. Muscle Nerve 22 :1058, 1999.
Lawton MB, Abadee P: Aspiration of a tracheostomy plug. Arch Phys Med Rehabil 68 :318, 1987.
Lefemine AA, MacDonnell K, Moon HS: Tracheal stenosis following cuffed tube tracheostomy. Anatomical variation and selected treatment. Ann Thorac Surg 15 :456, 1973.
Leonard RC, et al: Late outcome from percutaneous tracheostomy using the Portex kit. Chest 115 :1070, 1999.
Leverment JN, Pearson FG: Tracheal damage associated with cuffed tracheostomy tubes. Aspiration of gastric content as a cause of local damage in tracheotomised dogs. Anaesthesia 32 :603, 1977.
Leverment JN, Pearson FG, Rae SA: Manometric study of the upper oesophagus in the dog following cuffed-tube tracheostomy. Br J Anaesth 48 :83, 1976.
Lim JW, et al: Experience with percutaneous dilational tracheostomy. Ann Otol Rhinol Laryngol 109 :791, 2000.
Lin JC, Maley RH Jr, Landreneau RJ: Extensive posterior-lateral tracheal laceration complicating percutaneous dilational tracheostomy. Ann Thorac Surg 70 :1194, 2000.
Lin MC, et al: Pulmonary mechanics in patients with prolonged mechanical ventilation requiring tracheostomy. Anaesth Intensive Care 27 :581, 1999.
Lotan AN, Eliachar I, Joachims HZ: Pretracheal air cyst: late complication of tracheostomy. Arch Otolaryngol 103 :596, 1977.
Lulenski GC: Long-term tracheal dimensions after flap tracheostomy. Arch Otolaryngol 107 :114, 1981.
Lulenski GC, Batsakis JG: Management of the flap tracheostomy. An experimental study. Arch Otolaryngol 105 :260, 1979.
Lusuardi M. et al: Influence of clinical history on airways bacterial colonization in subjects with chronic tracheostomy. Respir Med 94 :436, 2000.
Madden BP, Datta S, McAnulty G: Tracheal granulation tissue after percutaneous tracheostomy treated with Nd:YAG laser: three cases. J Laryngol Otol 115 :743, 2001.
P.1034
Maeda K, et al: Mediastinitis after percutaneous dilatational tracheostomy. Thorac Cardiovasc Surg 50 :123, 2002.
Martin WM, Shapiro RS: Long custom-made plastic tracheostomy tube in severe tracheomalacia. Laryngoscope 91 :355, 1981.
Massick DD, et al: Bedside tracheostomy in the intensive care unit: a prospective randomized trial comparing open surgical tracheostomy with endoscopically guided percutaneous dilational tracheotomy. Laryngoscope 111 :494, 2001.
Mattox DE, Gates GA: Alternatives to tracheostomy in sleep apnea. N Engl J Med 308 :656, 1983.
Mayberry JC, et al: Cervical spine clearance and neck extension during percutaneous tracheostomy in trauma patients. Crit Care Med 28 :3436, 2000.
McGuire G, El Beheiry H, Brown D: Loss of the airway during tracheostomy: rescue oxygenation and re-establishment of the airway. Can J Anaesth 48 :697, 2001.
McHenry CR, et al: Percutaneous tracheostomy: a cost-effective alternative to standard open tracheostomy. Am Surg 63 :646, 1997.
Melloni G, et al: Surgical tracheostomy versus percutaneous dilatational tracheostomy: a prospective-randomized study with long-term follow-up. J Cardiovasc Surg (Torino) 43 :113, 2002.
Messineo A, et al: The safety of home tracheostomy care for children. J Pediatr Surg 30 :1246, 1995.
Meyer M, et al: Repeat bedside percutaneous dilational tracheostomy is a safe procedure. Crit Care Med 30 :986, 2002.
Miller FR, Eliachar I, Tucker HM: Technique, management, and complications of the long-term flap tracheostomy. Laryngoscope 105 :543, 1995.
Mittendorf EA, et al: Early and late outcome of bedside percutaneous tracheostomy in the intensive care unit. Am Surg 68 :342, 2002.
Mohammedi I, et al: Major cellulitis following percutaneous tracheostomy. Intensive Care Med 23 :443, 1997.
Muhammad JK, Major E, Patton DW: Evaluating the neck for percutaneous dilatational tracheostomy. J Maxillofac Surg 28 :336, 2000a.
Muhammad JK, et al: Percutaneous dilatational tracheostomy: haemorrhagic complications and the vascular anatomy of the anterior neck. a review based on 497 cases. Int J Oral Maxillofac Surg 29 :217, 2000b.
Mulder DS, et al: Tracheopleural fistula. A complication of the cuffed tracheostomy tube. J Thorac Cardiovasc Surg 63 :416, 1972.
Mullins JB, et al: Airway resistance and work of breathing in tracheostomy tubes. Laryngoscope 103 :1367, 1993.
Murphy DA, MacLean LD, Dobell AR: Tracheal stenosis as a complication of tracheostomy. Ann Thorac Surg 2 :44, 1966.
Muz J, et al: Scintigraphic assessment of aspiration in head and neck cancer patients with tracheostomy. Head Neck 16 :17, 1994.
Nani R, et al: Fantoni translaryngeal tracheostomy: perioperative complications on a 220 consecutive patients series. Minerva Anestesiol 68 :89, 2002.
Nates NL, et al: Percutaneous tracheostomy in critically ill patients: a prospective, randomized comparison of two techniques. Crit Care Med 28 :3734, 2000.
Nazari S, et al: Decompressing tracheostomy for the treatment of postintubation tracheal rupture. Ann Thorac Surg 68 :1122, 1999.
Niederman MS, et al: Nutritional status and bacterial binding in the lower respiratory tract in patients with chronic tracheostomy. Ann Intern Med 100 :795, 1984a.
Niederman MS, et al: Respiratory infection complicating long-term tracheostomy. The implication of persistent gram-negative tracheobronchial colonization. Chest 85 :39, 1984b.
Nomori H, Horio H, Suemasu K: Assisted pressure control ventilation via a mini-tracheostomy tube for postoperative respiratory management of lung cancer patients. Respir Med 94 :214, 2000.
Norwood S, et al: Incidence of tracheal stenosis and other late complications after percutaneous tracheostomy. Ann Surg 232 :233, 2000.
Orringer MB: As originally published in 1992: anterior mediastinal tracheostomy with and without cervical exenteration. Updated in 1998. Ann Thorac Surg 67 :591, 1999.
Orringer MB, Sloan H: Anterior mediastinal tracheostomy: indications, techniques, and clinical experience. J Thorac Cardiovasc Surg 78 :850, 1979.
Palazzo FF, Allen JG, Greatorex RA: Laryngeal mask airway and fibre-optic tracheal inspection in thyroid surgery: a method for timely identification of tracheomalacia requiring tracheostomy. Ann R Coll Surg Engl 82 :141, 2000.
Palmieri TL, Jackson W, Greenhalgh DG: Benefits of early tracheostomy in severely burned children. Crit Care Med 30 :922, 2002.
Papakostas K, Morar P, Fenton JE: Ballooned trachea caused by cuffed tracheostomy tube. J Laryngol Otol 114 :724, 2000.
Passy V, et al: Passy-Muir tracheostomy speaking valve on ventilator-dependent patients. Laryngoscope 103 :653, 1993.
Pearson FG, Andrews MJ: Detection and management of tracheal stenosis following cuffed tube tracheostomy. Ann Thorac Surg 12 :359, 1971.
Pierce WS, Tyers GF, Waldhausen JA: Effective isolation of a tracheostomy from a median sternotomy wound. J Thorac Cardiovasc Surg 66 : 841, 1973.
Pinder M, Cameron PD, Lovegrove A: Tracheal foreign body following tube change during percutaneous dilational tracheostomy: a cautionary tale. Anaesth Intensive Care 28 :443, 2000.
Pinilla JC: Acute respiratory failure in severe blunt chest trauma. J Trauma 22 :221, 1982.
Plummer AL, Gracey DR: Consensus conference on artificial airways in patients receiving mechanical ventilation. Chest 96 :178, 1989.
Posthumus DL, Peirce TH: Fatal tension pneumopericardium complicating tracheostomy. Chest 73 :107, 1978.
Qureshi AI, et al: Prediction and timing of tracheostomy in patients with infratentorial lesions requiring mechanical ventilatory support. Crit Care Med 28 :1383, 2000.
Rainer WG, Sanchez M: Tracheostomy cuff ilation synchronously timed with inspiration. Ann Thorac Surg 9 :384, 1970.
Reilly PM, et al: Occult hypercarbia. An unrecognized phenomenon during percutaneous endoscopic tracheostomy. Chest 107 :1760, 1995.
Reilly PM, et al: Hypercarbia during tracheostomy: a comparison of percutaneous endoscopic, percutaneous Doppler, and standard surgical tracheostomy. Intensive Care Med 23 :859, 1997.
Rhee CK, et al: The superiorly based flap long-term tracheostomy in pediatric patients. Am J Otolaryngol 17 :251, 1996.
Rigg CD, Edmondson L: Percutaneous dilational tracheostomy: malposition leading to delayed weaning. Anaesthesia 50 :724, 1995.
Rodriguez JL, et al: Early tracheostomy for primary airway management in the surgical critical care setting. Surgery 108 :655, 1990.
Rogers ML, et al: Airway fire during tracheostomy: prevention strategies for surgeons and anaesthetists. Ann R Coll Surg Engl 83 :376, 2001.
Rosenbower TJ, et al: The long-term complications of percutaneous dilatational tracheostomy. Am Surg 64 :82, 1998.
Rossi Ferrario S, et al: Caregiver strain associated with tracheostomy in chronic respiratory failure. Chest 119 :1498, 2001.
Sarpellon M, et al: Translarnygeal tracheostomy (TLT): a variant technique for use in hypoxemic conditions and in the difficult airway. Minerva Anestesiol 64 :393, 1998.
Schonhofer B, et al: Scintigraphy for evaluating early aspiration after oral feeding in patients receiving prolonged ventilation via tracheostomy. Intensive Care Med 25 :311, 1999.
Shaker R, et al: Deglutitive aspiration in patients with tracheostomy: effect of tracheostomy on the duration of vocal cord closure. Gastroenterology 108 :1357, 1995.
Sheldon CH: Percutaneous tracheostomy. JAMA 165 :2068, 1957.
Sherman JM, et al: Care of the child with a chronic tracheostomy. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med 161 :297, 2000.
Siddharth P, Mazzarella L: Granuloma associated with fenestrated tracheostomy tubes. Am J Surg 150 :279, 1985.
Sinfield A, DiVito J Jr, Brandstetter RD: Airway obstruction from overinflation and herniation of tracheostomy tube balloon. Heart Lung 18 :260, 1989.
Sise MJ, et al: Cricothyroidotomy for long-term tracheal access. A prospective analysis of morbidity and mortality in 76 patients. Ann Surg 200 :13, 1984.
Smith MM, et al: Evaluation of horizontal and vertical tracheotomy healing after short-duration tracheostomy in dogs. J Oral Maxillofac Surg 53 :289, 1995.
Snow N, Richardson JD, Flint L: Management of necrotizing tracheostomy infections. J Thorac Cardiovasc Surg 82 :341, 1981.
Society of Otorhinolaryngology and Head-Neck Nurses: Practice Guidelines. Tracheostomy. ORL Head Neck Nurs 12 :26, 1994.
Stamenkovic SA, et al: Is early tracheostomy safe in cardiac patients with median sternotomy incisions? Ann Thorac Surg 69 :1152, 2000.
Stanley TH, Liu WS: Tracheostomy and endotracheal tube cuff volume and pressure changes during thoracic operations. Ann Thorac Surg 20 : 144, 1975.
Stauffer JL, Olson DE, Petty TL: Complications and consequences of endotracheal intubation and tracheotomy. A prospective study of 150 critically ill adult patients. Am J Med 70 :65, 1981.
P.1035
Stocchetti N, et al: Neurophysiological consequences of three tracheostomy techniques: a randomized study in neurosurgical patients. J Neurosurg Anesthesiol 12 :307, 2000.
Stoeckli SJ, Breitbach T, Schmid SA: Clinical and histologic comparison of percutaneous dilational versus conventional surgical tracheostomy. Laryngoscope 107 :1643, 1997.
Sugerman HJ, et al: Multicenter, randomized, prospective trial of early tracheostomy. J Trauma 43 :741, 1997.
Sun KO: Fracture and dislodgement of tracheal cartilage during percutaneous tracheostomy. Anaesthesia 50 :370, 1995.
Tano Y, et al: Relation of bacterial flora between upper and lower respiratory tracts in patients with long-term tracheostomy. Kansenshogaku Zasshi 66 :592, 1992.
Teoh N, Parr MJ, Finfer SR: Bacteraemia following percutaneous dilational tracheostomy. Anaesth Intensive Care 25 :354, 1997.
Toursarkissian B, et al: Percutaneous dilational tracheostomy: report of 141 cases. Ann Thorac Surg 57 :862, 1994.
Toye FJ, Weinstein JD: Clinical experience with percutaneous tracheostomy and cricothyroidotomy in 100 patients. J Trauma 26 :1034, 1986.
Tran N, et al: Lateral tracheostomy in patients with cervical spinal cord injury. Br J Surg 82 :412, 1995.
Trottier SJ, et al: Posterior tracheal wall perforation during percutaneous dilational tracheostomy: an investigation into its mechanism and prevention. Chest 115 :1383, 1999.
Tschang TP, Cramer S: Massive hemorrhage from perforated thyroid complicating tracheostomy. Report of two cases. Arch Otolaryngol 103 :557, 1977.
Tsuda T, et al: Optimum humidification of air administered to a tracheostomy in dogs. Scanning electron microscopy and surfactant studies. Br J Anaesth 49 :965, 1977.
Turnbull AD: The two stage tracheostomy as a safe technique in instances of severe coagulopathy. Surg Gynecol Obstet 172 :315, 1991.
Van Heerbeek N, et al: The guide wire dilating forceps technique of percutaneous tracheostomy. Am J Surg 177 :311, 1999.
Van Heurn LW, et al: Comparative clinical trial of progressive dilatational and forceps dilatational tracheostomy. Intensive Care Med 27 :292, 2001.
Vaz Fragoso CA, Kacmarek RM, Systrom DM: Improvement in exercise capacity after nocturnal positive pressure ventilation and tracheostomy in a postpoliomyelitis patient. Chest 101 :254, 1992.
Wagner F, et al: Percutaneous dilatational tracheostomy: results and long-term outcome of critically ill patients following cardiac surgery. Thorac Cardiovasc Surg 46 :352, 1998.
Walz MK, et al: Percutaneous dilatational tracheostomy: early results and long-term outcome of 326 critically ill patients. Intensive Care Med 24 : 685, 1998.
Westphal K, et al: Tracheostomy in cardiosurgical patients: surgical tracheostomy versus Ciaglia and Fantoni methods. Ann Thorac Surg 68 : 486, 1999.
Wetmore RF, Handler SD, Potsic WP: Pediatric tracheostomy. Experience during the past decade. Ann Otol Rhinol Laryngol 91 :628, 1982.
Wetmore RF, et al: Pediatric tracheostomy: a changing procedure? Ann Otol Rhinol Laryngol 108 :695, 1999.
Whited RE: A prospective study of laryngotracheal sequelae in long-term intubation. Laryngoscope 94 :367, 1984.
Wilson EB, Malley N: Discharge planning for the patient with a new tracheostomy. Crit Care Nurse 10 :73, 1990.
Winkler WB, et al: Bedside percutaneous dilational tracheostomy with endoscopic guidance: experience with 71 ICU patients. Intensive Care Med 20 :476, 1994.
Wyatt ME, Bailey CM, Whiteside JC: Update on paediatric tracheostomy tubes. J Laryngol Otol 113 :35, 1999.
Young JS, et al: A novel method for replacement of the dislodged tracheostomy tube: the nasogastric tube guidewire technique. J Emerg Med 14 :205, 1996.
Zajac DJ, Fornataro-Clerici L, Roop TA: Aerodynamic characteristics of tracheostomy speaking valves: an updated report. J Speech Lang Hear Res 42 :92, 1999.
EAN: 2147483647
Pages: 203