40 - Mechanical Ventilation of the Surgical Patient
Editors: Shields, Thomas W.; LoCicero, Joseph; Ponn, Ronald B.; Rusch, Valerie W.
Title: General Thoracic Surgery, 6th Edition
Copyright 2005 Lippincott Williams & Wilkins
> Table of Contents > Volume I - The Lung, Pleura, Diaphragm, and Chest Wall > Section X - The Diaphragm > Chapter 49 - Diaphragmatic Function, Diaphragmatic Paralysis, and Eventration of the Diaphragm
Chapter 49
Diaphragmatic Function, Diaphragmatic Paralysis, and Eventration of the Diaphragm
Thomas W. Shields
Although the major anatomic function of the diaphragm is the separation of the thoracic and abdominal cavities, its major physiologic function is its role in ventilation. The movement of this musculotendinous structure is responsible for the largest fraction of air moved during inspiration. With quiet breathing, this accounts for about 75% to 80% of the total amount of air brought into the lungs. In the supine position, it contributes 60% of the minute volume.
Primarily, the diaphragm is a muscle of inspiration, and the downward descent of the central tendon results from a coordinated contraction of all its muscle fibers. The resultant vertical movement is about 1 to 2 cm during quiet breathing but may be as much as 6 to 7 cm with deep, forced breathing. Each centimeter of vertical movement is estimated to contribute an intake of about 300 to 400 mL of air during normal breathing.
As noted by De Troyer and associates (1982) and Rochester (1985), however, the muscle mass of the diaphragm is considered to comprise two functionally distinct parts: costal and crural portions. The fiber composition of each is different: The costal muscle is thin, and the crural portion is thicker. Both groups of fibers are innervated by the phrenic nerves, but stimulation by phrenic activity results in two different actions on the chest wall. Contraction of the costal portion causes the diaphragm to flatten and the lower ribs to lift; both activities enlarge the thoracic cavity. The crural portion only causes some downward displacement of the diaphragm and is thus less effective in overall ventilatory activity of the structure.
Some muscular activity of the diaphragm occurs during exhalation. Contraction of the diaphragmatic muscle fibers does not cease abruptly at the onset of expiration but gradually declines during the initial portion of expiration and reaches zero at about the midpoint of expiration. Persistent diaphragmatic activity during the early phase of expiration provides precise regulation of the shift in airflow from inspiration to expiration. During vigorous breathing efforts, activity of the diaphragm also occurs toward the end of maximum expiratory efforts. The muscular activity at this time, as Agostoni and Torri (1962) reported, limits the degree to which the lungs collapse.
PARALYSIS OF THE DIAPHRAGM
Either the right or left hemidiaphragm may be paralyzed without significant respiratory embarrassment in the adult. Although ventilation on the paralyzed side is maintained by transmission of the cyclic pressure changes produced by the functioning hemidiaphragm across the mediastinum, a 20% to 30% reduction initially occurs in the vital capacity and the total lung capacity. Fackler and colleagues (1967) reported the return of these lung volumes to normal after 6 months. Clinically, in an adult, respiratory distress is minimal, although the patient may complain of chest pain and a nonproductive cough. The patient may spontaneously sleep in a semirecumbent position or in the lateral decubitus position with the side of the paralyzed hemidiaphragm down. Bilateral diaphragmatic paralysis may be tolerated by normal adults, but as McCredie and associates (1962) noted, a marked reduction of vital capacity and expiratory flow rates results, particularly while the individual is supine. In a patient with bilateral paralysis, excessive movement of the accessory muscles of respiration may be seen. Rochester (1985) has noted that such individuals are prone to chronic respiratory failure.
In infants and young children, unilateral paralysis may cause severe respiratory embarrassment, and mechanical ventilation is necessary. Bilateral paralysis is even more life-threatening and is fatal unless the infant or child receives prompt ventilatory support.
In the infant or child, the lower rib cage, as noted by Hagan and colleagues (1977), may move paradoxically, even with quiet respiration. When the infant is in the lateral decubitus position, Robotham (1979) has reported that, with the paralyzed diaphragmatic leaf up, the inward paradoxic motion
P.741
of the subcostal area of the upper abdomen can be seen readily. In the adult, paradoxic movement of the lower chest wall or abdomen is not evident.
Paralysis of the hemidiaphragm may be suggested by elevation of that leaf of the diaphragm on a standard chest radiograph, and evidence of some basilar atelectasis on the involved side may also be present. Paralysis may be positively identified by the fluoroscopic observation of paradoxic movement of the paralyzed hemidiaphragm on sudden inspiration. This is best demonstrated by the classic sniff test. The sudden inspiratory movement causes the normal hemidiaphragm to descend, whereas the paralyzed hemidiaphragm moves in the opposite direction; an excursion of 2 cm or greater is required for the diagnosis according to Miller and colleagues (2001). It has been suggested by Houston and associates (1995) that the use of ultrasound is superior to that of fluoroscopy in the evaluation of hemidiaphragmatic motion. According to the studies of Ueki and co-workers (1995), as well as those of Gottesman and McCool (1997), the thickness of the muscle of the paralyzed hemidiaphragmatic leaf was significantly less than that of the normal contralateral leaf. The change of the muscular thickness was likewise increased significantly less on inspiration on the involved side as compared with the increase on the normal side. Finally, in critically ill patients requiring mechanical ventilation, electrophysiologic evaluation of the phrenic nerves has been suggested by Moorthy and associates (1985). This appears to be a reliable and satisfactory method for determining the presence of paralysis of a diaphragmatic leaf under adverse clinical conditions.
Etiology
In infants, the most common cause of unilateral hemidiaphragmatic paralysis is injury of one of the phrenic nerves during a cardiac procedure. Stone and associates (1987) reported an incidence of only 0.3%, but Watanabe and colleagues (1987) noted an incidence of 1.6%. The incidence was slightly higher for open heart procedures and somewhat lower for closed heart operations (1.9% versus 1.3%). The Mustard procedure and the Glenn anastomosis had the highest incidences in each respective group. Procedures after previous operations had almost twice the incidence of an initial procedure. Most of the injuries were temporary (84%) but initially were associated with considerable morbidity. Before modern management, Shoemaker and colleagues (1981) recorded an overall mortality rate of 20% to 25%; the high rate was due mainly to underlying cardiac conditions. Birth trauma is also an occasional cause of phrenic nerve injury, as is the removal of a mediastinal tumor in an infant or young child. In pubescent girls, Helps and associates (1993) reported that a high incidence of right phrenic nerve injury occurred when a low submammary incision was used as the access for a right thoracotomy in the repair of secundum atrial defect, as compared with a low rate of injury with the use of a midline sternal approach. It is suggested that the former approach be abandoned in this group of patients.
In adults, posttraumatic injury after a cardiac procedure, particularly with the use of topical hypothermia with ice slush, is the most common cause. Scannell and associates (1963) initially reported two deaths in four patients with cold injury to the phrenic nerves. Subsequently, Dajee and colleagues (1983) reported an incidence of topically hypothermic-induced injury of 9.6% but with no resulting mortality. Usually, the left phrenic nerve is the involved nerve, but right or bilateral nerve injury does occur. Some degree of paresis probably occurred in even a much higher percentage in the early experience with topical hypothermia. Wheeler and associates (1985) reported the use of a cardiac insulation pad to reduce the incidence of injury. Hypothermic injury, however, is now less of a problem with the avoidance of opening of the pleural space, and if this does occur, inflation of the lung to protect the nerve from contact with the ice slush has reduced the incidence to less than 2% in most centers. When injury does occur, it is generally only temporary but can be permanent in 15% to 25% of patients.
Other traumatic causes of phrenic nerve damage are involvement by tumor (e.g., primary carcinoma of the lung, invasive thymoma, malignant germ cell tumors, and non-Hodgkin's lymphoma). Surgical injury likewise may occur and has been noted after mediastinotomy, surgical resections in the thorax and neck, and even placement of a subclavian or jugular vein catheter or electrode. High cervical spinal cord injuries may also result in diaphragmatic paralysis.
Idiopathic diaphragmatic paralysis is not uncommon in adults. It frequently is the result of a subclinical viral infection. The paralysis is most often unilateral, but patients with bilateral involvement have been reported by Spitzer (1973), Camfferman (1985), and Celli (1987) and their associates. Piehler and colleagues (1982) reviewed the records of 142 patients with unexplained diaphragmatic paralysis. Less than half were symptomatic. Subsequent improvement was better in those who had pain or cough than in those with dyspnea. The diaphragm returned to a normal position in less than 10%. Only 3.5% had an underlying malignancy, and only one patient (0.7%) had progressive atrophy. A rare cause of hemidiaphragmatic paralysis is the occurrence of paralytic brachial neuritis (neuralgic amyotrophy or brachial plexus neuropathy) that is called the Parsonage-Turner syndrome after the two neurologists who fully described this condition in 1948 and 1957, although it was first reported by Spillane in 1943. The syndrome most commonly involves the brachial plexus nerve roots, either unilaterally or bilaterally, with the sudden onset of severe pain in the distribution of the involved nerve roots, and is subsequently followed by paralysis or paresis of the associated muscle groups of the involved upper extremity or shoulder girdle. The cause is unknown, and recovery may take as long as 3 years. Infrequently, one or both of the phrenic nerves are involved, as first noted by Alajouanine and associates (1950), according to the review of Patterson and colleagues (1994). The resultant diaphragmatic
P.742
involvement is accompanied by varying degrees of dyspnea that may be quite severe with bilateral hemidiaphragmatic involvement. Diaphragmatic function is slow to recover, and more often than not, it does not occur. This is particularly true in patients with bilateral phrenic nerve involvement, and these patients have the poorer prognosis as to their recovery. The reports of Walsh (1987) and Mulvey (1993) and their associates discuss this problem in detail.
Management
In infants and young children, initial therapy is mechanical ventilation, including continuous positive airway pressure. Proper positioning with the involved side down appears helpful. If continued support is required beyond 2 weeks, Watanabe and colleagues (1987) advise operative plication of the involved diaphragmatic leaf, as suggested by Shoemaker and associates (1981), for example. The technique of plication [i.e., central pleating, as described by Schwartz and Filler (1978)], which does not require muscle resection and minimizes the possibility of injury to the phrenic nerve branches of the hemidiaphragm, is suggested as the method of choice. A different approach has been suggested by Jaklitsch and colleagues (1997). They reported the successful use of radial diaphragmatic plication in infants with moderate to severe respiratory distress. In their technique using a lateral thoracotomy, multiple sutures reinforced with Teflon pledgets are placed circumferentially in the periphery of the hemidiaphragm that avoid the central tendon. This minimizes the possibility of further injury to the phrenic nerve or injury to the blood supply of the central tendon. Moores (personal communication, 1997) suggests a somewhat similar approach to hemidiaphragmatic plication that uses only four sutures that are radially placed into the central tendon and then brought out at the peripheral margin of the hemidiaphragm and encircle the adjacent rib. This latter procedure can be accomplished readily by a video-assisted thoracic surgery (VATS) approach. The effect of plication of the paralyzed leaf of the diaphragm is the immobilization of the leaf in the flat position to reduce maximally its paradoxic movement with the associated shift of the mobile mediastinum to the contralateral side on inspiration. Ventilatory exchange becomes more efficient, and the infant may be more readily weaned from ventilatory support. The value of early plication has been supported further by the long-term study reported by Stone and colleagues (1987), who showed that plication did not prevent return of diaphragmatic function.
At times, direct repair of a severed nerve may be attempted. Brouillette and associates (1986) reported the successful repair of one transected phrenic nerve but failure of an interposed nerve graft in the other in a patient with bilateral nerve transections during the operative removal of a mediastinal lesion. Schoeller and co-workers (2001) reported a successful restoration of function of the right hemidiaphragm 9 months after insertion of a sural nerve graft at the time of excision of a segment of the right phrenic nerve during the resection of a malignant thymoma. These authors believe that the sooner the nerve is repaired, the greater is the chance of success; any repair later than 12 months after injury is doomed to fail.
In adults and children older than 2 years, conservative therapy is most often indicated. Surgical intervention and plication of the involved diaphragmatic leaf has been done with good success, however, by Wright and colleagues (1985) in patients with continuing disability. Graham and associates (1990) reported the use of plication in 17 adult patients who had persistent dyspnea and orthopnea due to paralysis of a hemidiaphragm with a reduction in the forced vital capacity and lung volume. All showed subjective and objective improvement. In a 5- to 12-year follow-up in six patients, objective improvement in the lung functions were maintained. In patients with idiopathic bilateral paralysis, Celli and associates (1987) have reported salutary results by the use of intermittent external negative-positive ventilation.
Therapeutic Use of Phrenic Nerve Paralysis
Therapeutic temporary paralysis of a phrenic nerve has been used in the past for treatment of pulmonary tuberculosis. This procedure can be used to elevate the hemidiaphragm to help obliterate the pleural space after the removal of a portion of the lung when there is insufficient residual lung tissue to fill the pleural space. Temporary paralysis can be obtained postoperatively by percutaneous infiltration around the nerve trunk in the neck with local anesthetic. At times, direct exposure of the nerve in the neck is required. Additional elevation of the paralyzed diaphragm can be obtained by the induction of a temporary pneumoperitoneum.
Temporary Induction of a Pneumoperitoneum
Handy and colleagues (1997) used a temporary pneumoperitoneum to treat air leaks and residual pleural spaces after lung volume reduction surgery. De Giacomo and associates (2001) also have used the establishment of a pneumoperitoneum to help control prolonged air leaks associated with a persistent pleural space after a lobectomy for lung cancer, and Cerfolio and co-workers (2000) used it as a prophylactic measure after a bilobectomy of the right lower and middle lobes to reduce the incidence of postoperative basilar as well as apical pleural spaces.
EVENTRATION OF THE DIAPHRAGM
Eventration of the diaphragm is a rare anomaly, the cause of which remains to be understood completely. In general, congenital eventration of the diaphragm or the eventration
P.743
occurring in newborn infants is probably a true congenital defect acquired during the fetal period. Severe cardiorespiratory symptoms in the newborn or neonate with a large unilateral eventration may be present because of secondary hypoplasia of the lung on the involved side. The appropriate resuscitative measures are required to correct acid-base balance, ventilatory insufficiency, and poor systemic perfusions, as in the neonate with a symptomatic congenital posterolateral diaphragmatic hernia (see Chapter 51). After the newborn's condition is stabilized, surgical correction of the eventration is indicated.
The repair of the defect is an emergency procedure in newborns or neonates with respiratory distress. It usually is accomplished through a thoracic approach. An incision is made in the circumference of the diaphragm, a few centimeters from the costal margin. The thinned-out diaphragm then is put on a stretch and reattached to the costal margin.
Eventration that occurs in older children and adults is thought to be caused by an acquired complete or incomplete paralysis of a diaphragmatic leaf. More often than not, localized eventration, which usually occurs on the right, with protrusion of liver through the defect, does not require surgical treatment. With a major hernia or a complete eventration, the patient may have cardiorespiratory symptoms, gastrointestinal symptoms, or both secondary to the elevation of the diaphragmatic leaf. Operative repair is indicated for older patients who have symptoms. Peters (1994) succinctly defined the value of plication of the diaphragm, but he emphasized that it only should be done when evidence exists of ventilatory compromise leading to ventilatory insufficiency because of the paradoxic movement of the involved hemidiaphragmatic leaf:
Plication of the diaphragm substitutes a fixed for a paradoxical diaphragm. The patient wastes less energy if the position of the diaphragm at end-expiration results in an adequate preload on the remaining inspiratory muscles. If the paralyzed diaphragm is made very tight to assume the position of maximum inspiration, this should decrease the ventilatory work by eliminating the paradoxical motion and at the same time result in a better preload on the inspiratory muscles by providing a more subatmospheric pleural pressure at end-expiration. Plication of the paralyzed diaphragm increases both end-expiratory and end-inspiratory lung volumes by preventing the abdominal contents from displacing the lung during both inspiration and expiration. In a patient with chronic obstructive lung disease who has poor elastic recoil of the lungs and chronic hyperexpansion of the lungs, fixing the paradoxical diaphragm in the inspiratory position provides more room for the large lungs and results in a more subatmospheric end-expiratory pressure, which exerts greater force to pull in the chest and elevate the innervated diaphragm to provide a better preload to the inspiratory muscles.
A transthoracic approach is preferred. Entry into the pleural space is made through the bed of the eighth rib or the eighth intercostal space. After any adhesions that may be present are freed, the thinned-out diaphragmatic leaf is repaired by plication (Fig. 49-1). A second method is by incision of the leaf, and the repair then is carried out by imbricating one layer over the other with interrupted sutures of No. 00 or No. 0 silk or
P.744
other nonabsorbable suture material (Fig. 49-2). Either repair is usually attended with low mortality and morbidity rates; however, plication of the diaphragmatic leaf is the preferred method in most centers. Mouroux and colleagues (1996) have suggested that the repair of an eventration be carried out by a VATS approach rather than by a standard thoracotomy. Knight and Clarke (1998) also have suggested the technique of diaphragmatic plication by a VATS approach, but only a small number of repairs have been reported using this approach. In fact, Hazelrigg (2000) cautions that the VATS approach in the surgical management of diaphragmatic eventration should not be attempted unless the individual surgeon has had considerable experience with numerous VATS procedures. The technique in the VATS approach is that the diaphragmatic leaf is invaginated and held in place by two rows of continuous sutures (Fig. 49-3).
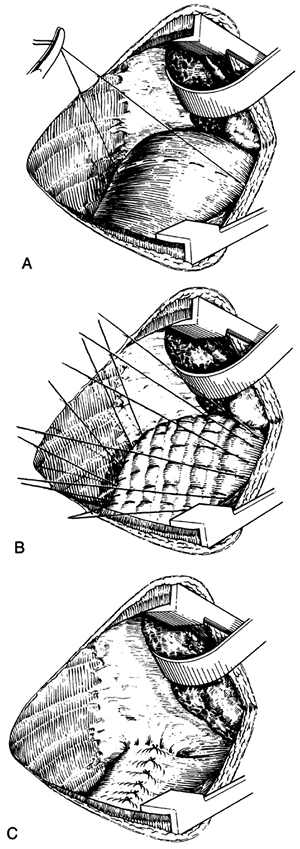 |
Fig. 49-1. Technique of plication of an eventration of the diaphragm. A. Four to six rows of No. 00 or 000 nonabsorbable sutures are inserted into the hemidiaphragm in an anterolateral to a posterolateral direction. Each row consists of five to six pleats. The branches of the phrenic nerve are avoided when the nerve is still functional. B. The sutures are left untied until all rows are in place. C. Sutures are tied to plicate and shorten the nonfunctioning leaf. From Spitz L. In: Jackson JW, Cooper DKC, eds. Rob and Smith's Operative Surgery: Thoracic Surgery. 4th Ed. London: Butterworths, 1986, p. 7. With permission. |
 |
Fig. 49-2. Technique of repair of symptomatic eventration of the diaphragm. From Shields TW. The diaphragm. In: Nora P, ed. Operative Surgery: Principles and Techniques. Philadelphia: Lea & Febiger, 1972. With permission. |
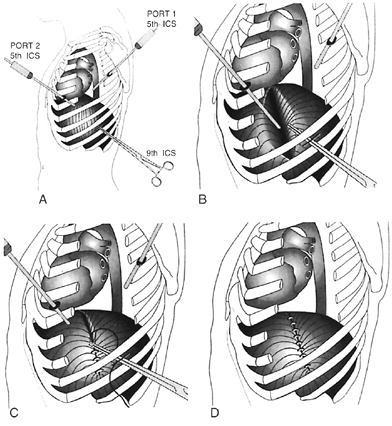 |
Fig. 49-3. A. Position of the two thoracoscopic ports: PORT 1 for the thoracoscope and PORT 2 for site of insertion of the forceps used to group the apex of the eventration. A minithoracotomy is made over the ninth intercostal space (ICS) for the suturing of the diaphragm. B. With the use of a Duval forceps, the apex of the eventration is pushed down toward the abdomen. C. The created transverse fold of the diaphragm is sutured with nonabsorbable material. D. Completed operation. From Mouroux J, et al: Technique for the repair of diaphragmatic eventration. Ann Thorac Surg 62:205, 1996. With permission. |
Results of Diaphragmatic Plication
Regardless of the individual surgical technique used, the results of diaphragmatic plication have been satisfactory. Wright (1985) and Graham (1990) and their associates achieved excellent relief of exertional dyspnea and orthopnea after transthoracic diaphragmatic plication of unilateral, nonmalignant diaphragmatic paralysis. A significant increase occurred in arterial oxygen tension and all lung volumes except residual volume in their patients. Higgs and colleagues (2002) reported the long-term follow-up of 15 patients for an average of 10 years (range, 7 to 14 years) after unilateral diaphragmatic plication. Initial postoperative functional evaluations were conducted 6 weeks postoperatively, and the late evaluations were conducted between the seventh and fourteenth years. At 6 weeks and at the late term of evaluations, there were significant improvements in all spirometric values and lung volumes in the sitting position compared with the preoperative values and in all but the forced expiratory volume in 1 second at long-term follow-up in the supine position. Dyspnea scores were improved in all but three patients (two remained unchanged, and one showed a slight decrease).
P.745
RARE DIAPHRAGMATIC DEFECTS
Agenesis of the diaphragm and the presence of an accessory diaphragm have been reported by Nazarian (1971) and Geisler (1977) and their colleagues. A syndrome described by Spitz and associates (1975) consists of multiple supraumbilical abdominal wall defects, defects of the lower sternum, deficiency of the anterior diaphragm and diaphragmatic pericardium, and congenital cardiac defects (i.e., Cantrell's pentalogy) (see Chapter 41).
REFERENCES
Agostoni E, Torri G: Diaphragm contraction as a limit to maximum expiration. J Appl Physiol 17:427, 1962.
Alajouanine T, Thurel B, Blatrix C: Paralysie amyotrophique des muscles p riscapulaires, bilat rale et asym trique, d but brusque et douloureux. Rev Neurol 82:280, 1950.
Brouillette RT, et al: Successful reinnervation of the diaphragm after phrenic nerve transection. J Pediatr Surg 21:63, 1986.
Camfferman F, et al: Idiopathic bilateral diaphragmatic paralysis. Eur J Respir Dis 66:65, 1985.
Celli BR, Rassulo J, Corral R: Ventilatory muscle dysfunction in patients with bilateral idiopathic diaphragmatic paralysis: reversal by intermittent external negative pressure ventilation. Am Rev Respir Dis 136:1276, 1987.
Cerfolio RJ, Holman WL, Katholi CR: Pneumoperitoneum after concomitant resection of the right middle and lower lobes (bilobectomy). Ann Thorac Surg 70:942, 2000.
Dajee A, et al: Phrenic nerve palsy after topical cardiac hypothermia. Int Surg 68:345, 1983.
De Giacomo T, et al: Pneumoperitoneum for the management of pleural air space problems associated with major pulmonary resections. Ann Thorac Surg 72:1716, 2001.
De Troyer A, et al: Action of costal and crural parts of the diaphragm on the rib cage in dogs. J Appl Physiol 53:30, 1982.
Fackler CD, Perret GE, Bedell GN: Effect of unilateral phrenic nerve section on lung function. J Appl Physiol 23:923, 1967.
Geisler F, Gottlieb A, Fried D: Agenesis of the right diaphragm repaired with Marlex. J Pediatr Surg 12:587, 1977.
Graham DR, et al: Diaphragmatic plication for unilateral diaphragmatic paralysis: a 10 year experience. Ann Thorac Surg 49:248, 1990.
Gottesman E, McCool FD: Ultrasound evaluation of the paralyzed diaphragm. Am J Respir Crit Care Med 155:1570, 1997.
Hagan R, et al: Neonatal chest wall afferents and regulation of respiration. J Appl Physiol 42:362, 1977.
Handy JR Jr, Judson MA, Zeller JL: Pneumoperitoneum to treat air leaks and spaces after a lung volume reduction operation. Ann Thorac Surg 64:1803, 1997.
Hazelrigg SR: Commentary: Knight SR, Clarke CP: The diaphragm. In Yim APC, et al (eds): Minimal Access Cardiothoracic Surgery. Philadelphia: WB Saunders, 2000, p. 301.
Helps BA, et al: Phrenic nerve damage via a right thoracotomy in older children with secundum ASD. Ann Thorac Surg 53:328, 1993.
Higgs SM, et al: Long-term results of diaphragmatic plication for unilateral diaphragm paralysis. Eur J Cardiothorac Surg 21:294, 2002.
Houston JG, et al: Comparison of ultrasound with fluoroscopy in the assessment of suspected hemidiaphragmatic movement abnormality. Clin Radiol 50:95, 1995.
Jaklitsch MT, et al: Twenty-year experience with peripheral radial plication of the diaphragm. Presented at the 33rd Annual Meeting of the Society of Thoracic Surgery. February 3, 1997, San Diego, CA.
Knight SR, Clarke CP: VATS plication of diaphragmatic eventration. Ann Thorac Cardiovasc Surg 4:240, 1998.
McCredie M, Lovejoy FW Jr, Kalfrieder NL: Pulmonary function in diaphragmatic paralysis. Thorax 17:213, 1962.
Miller NL, et al (eds): Radiologic Diagnostic of Diseases of the Chest. Philadelphia: WB Saunders Co, 2001, p. 751.
Moorthy SS, et al: Electrophysiologic evaluation of phrenic nerves in severe respiratory insufficiency requiring mechanical ventilation. Chest 88:211, 1985.
Mouroux J, et al: Technique for the repair of diaphragmatic eventration. Ann Thorac Surg 62:905, 1996.
Mulvey DA, et al: Diaphragmatic dysfunction in neuralgic amyotrophy: an electrophysiologic evaluation of 16 patients presenting with dyspnea. Am Rev Respir Dis 147:66, 1993.
Nazarian M, et al: Accessory diaphragm: report of a case with complete physiological evaluation and surgical correction. J Thorac Cardiovasc Surg 61:293, 1971.
Parsonage MJ, Turner JWA: Neurologic amyotrophy: the shoulder-girdle syndrome. Lancet 1:973, 1948.
Patterson DL, DeRemee RA, Hunt LW: Severe asthma complicated by bilateral disphragmatic paralysis attributed to Parsonage-Turner syndrome. Mayo Clin Proc 69:774, 1994.
Peters RM: Invited commentary of Takeda S, et al: Plication of the hemidiaphragm after sleeve pneumonectomy, p. 1755, and Glassman LR, et al: Successful plication for postoperative diaphragmatic paralysis in an adult, p. 1754. Ann Thorac Surg 58:1757, 1994.
Piehler JM, et al: Unexplained diaphragmatic paralysis: a harbinger of malignant disease? J Thorac Cardiovasc Surg 84:861, 1982.
Robotham JL: A physiological approach to hemidiaphragm paralysis. Crit Care Med 7:563, 1979.
Rochester DF: The diaphragm: contractile properties and fatigue. J Clin Invest 75:1397, 1985.
Scannell SC: Results of open heart operation for acquired aortic valve disease. J Thorac Cardiovasc Surg 45:47, 1963.
Schoeller T, et al: Successful immediate phrenic nerve reconstruction during mediastinal tumor resection. J Thorac Cardiovasc Surg 122:1235, 2001.
Schwartz MZ, Filler RM: Plication of the diaphragm for symptomatic phrenic nerve paralysis. J Pediatr Surg 13:259, 1978.
Shoemaker R, et al: Aggressive treatment of required phrenic nerve paralysis in infants and small children. Ann Thorac Surg 32:250, 1981.
Spillane JD: Localized neuritis of the shoulder girdle: a report of 46 cases in the MEF. Lancet 2:532, 1943.
Spitz L, et al: Combined anterior abdominal wall, sternal, diaphragmatic, pericardial and intracardiac defects: a report of five cases and their management. J Pediatr Surg 10:491, 1975.
Spitzer SA, Korczym AD, Kalaci J: Transient bilateral diaphragmatic paralysis. Chest 64:355, 1973.
Stone KS, et al: Long-term fate of the diaphragm surgically plicated during infancy and early childhood. Ann Thorac Surg 44:62, 1987.
Turner JWA, Parsonage MJ: Neurologic amyotrophy (paralytic brachial neuritis) with special reference to prognosis. Lancet 2:209, 1957.
Ueki J, De Bruin PF, Pride NB: In vivo assessment of diaphragm contraction by ultrasound in normal subjects. Thorax 50:1157, 1995.
Walsh NE, et al: Brachial neuritis involving the bilateral phrenic nerves. Arch Phys Med Rehabil 68:46, 1987.
Watanabe T, et al: Phrenic nerve paralysis after pediatric cardiac surgery. Retrospective study of 125 cases. J Thorac Cardiovasc Surg 94:383, 1987.
Wheeler WE, et al: Etiology and prevention of topical cardiac hypothermia-induced phrenic nerve injury and left lower lobe atelectasis during cardiac surgery. Chest 88:680, 1985.
Wright CD, et al: Results of diaphragmatic plication for unilateral diaphragmatic paralysis. J Thorac Cardiovasc Surg 90:195, 1985.
Reading References
Campbell EJM. The Respiratory Muscles and the Mechanics of Breathing. London: Lloyd-Luke, 1958.
Easton PA, et al: Respiratory function after paralysis of the right hemidiaphragm. Am Rev Respir Dis 127:125, 1983.
Haller JA Jr, et al: Management of diaphragmatic paralysis in infants with special emphasis on selection of patients for operative plication. J Pediatr Surg 14:779, 1979.
Keltz H, Kaplan S, Stone DJ: Effect of quadriplegia and hemidiaphragmatic paralysis on the thoraco-abdominal pressure during respiration. Am J Phys Med 48:109, 1969.
Koontz AR, Levin MB: Agenesis of the right half of the diaphragm. Am Surg 34:657, 1968.
McNamara JJ, et al: Eventration of the diaphragm. Surgery 64:1013, 1968.
Ribet M, Linder JL: Plication of the diaphragm for unilateral eventration or paralysis. Eur J Cardiothorac Surg 6:357, 1992.
Thomas TV: Congenital eventration of the diaphragm. Ann Thorac Surg 10:180, 1970.
EAN: 2147483647
Pages: 203