6 - Carcinomas of the Head and Neck
Editors: Skeel, Roland T.
Title: Handbook of Cancer Chemotherapy, 7th Edition
Copyright 2007 Lippincott Williams & Wilkins
> Table of Contents > Section III - Chemotherapy of Human Cancer > Chapter 6 - Carcinomas of the Head and Neck
Chapter 6
Carcinomas of the Head and Neck
Harlan A. Pinto
The management of patients with advanced head and neck cancer is challenging because optimal outcome requires intensive and specialized evaluation, coupled with coordinated multimodality treatment, supportive care, and rehabilitation. The use of chemotherapy to treat head and neck cancer is especially challenging because there is a narrow therapeutic index, high rates of moderate to severe side effects, and only modest benefits for most patients. Nevertheless, successful management plans can be particularly rewarding, because great suffering can be ameliorated and combined modality treatment plans may allow for less disfigurement while maintaining cure as a goal for many patients.
This chapter focuses on the squamous cell carcinomas that arise from the mucosa that lines the aerodigestive tract from the lip to the esophagus and trachea. Squamous cell carcinomas that arise in this upper aerodigestive region account for approximately 5% of the new cancers seen in the United States annually. This chapter will not discuss the chemotherapy for the melanomas, lymphomas, sarcomas, major or minor salivary gland cancers, and thyroid or esophagus cancers that arise in this region.
Improvements in radiotherapy, surgery, and medical therapy often occur in isolation as we use the scientific method to isolate and test one factor at a time. In this setting the treatment options and variations in combined modality therapy have proliferated. This has underscored the need for careful patient selection, because the supportive care needs and interventions have expanded as the complexity of treatments have increased. Adverse effects in one aspect sometimes compromises improvement in another aspect of outcome. Balancing these outcomes that conflict is a major challenge to progress. In this context, quality of life has become an important focus of study but may be difficult to apply to an individual patient. This complexity means that selection of an optimal treatment plan to arrive at the best possible outcome
P.214
for a specific patient should be individualized and be based on the expertise of the entire treatment team.
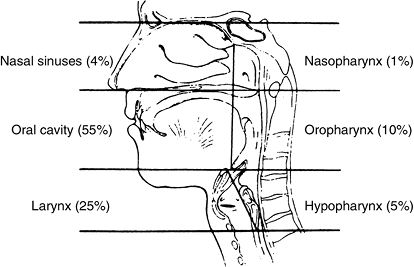 |
Figure 6.1. Anatomic divisions of the head and neck. Percentages indicate the relative frequencies of carcinoma in these regions. |
Table 6.1. Upper aerodigestive tract sites | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Understanding head and neck cancer begins with understanding the aerodigestive anatomy. A cross-sectional view of the anatomic regions and the relative frequency of cancer occurring in each area are shown in Fig. 6.1. The relationship of the anatomic structures to normal functions such as breathing, chewing, swallowing, speaking, and physical interactions related to intimacy is reflected in the anatomic recognition of site and subsite within each region. Table 6.1 lists the major sites within each of the anatomic subdivisions. Many cancers involve more than one subsite and some overlap adjacent sites. This fact has led to the use of regional terms, which can obscure factors about specific cancers that make them unsuitable for optimal outcome in regard to a specific treatment plan for surgery or radiotherapy.
I. Common and divergent characteristics
Despite this complexity of the anatomy, squamous carcinomas of the head and neck are often considered together because they share cell type, epidemiology and risk factors, natural history, and the need for head and neck surgeons to participate in optimal evaluation and management. Male predominance (3:1), heavy tobacco and alcohol use, and onset in late middle age describe a typical patient. The median age at diagnosis ranges from 55 to 67 years, depending on the site, with nasopharynx and tonsil cancer diagnosed at a younger age and oral cavity and larynx cancer diagnosed at an older age. A relatively new phenomenon of younger patients without the characteristic history of alcohol and tobacco use has been associated with infection with human papillomavirus (HPV). Identification of this population has prognostic implications in that their risk of death from the cancer is 60% to 80% less than that of those who are HPV negative.
Patterns of spread are also similar for head and neck cancers, with detectable local extension to adjacent structures and
P.215
P.216
lymphatic spread to regional lymph nodes occurring in many cases. For carcinomas of the oral cavity, oropharynx, and larynx, spread below the clavicle is unusual; however, pulmonary metastases are more frequent than bone or hepatic metastases. Direct extension to the mandible or the skull base may occur at diagnosis or recurrence. Most recurrences occur within 18 months of primary treatment, 90% within 2 years. Patients who are not cured usually die from the cancer within 3 to 4 years of diagnosis. The 5-year relative survival rate currently for all cases is approximately 58%, and those who succumb to the cancer generally suffer local, regional, and distant failure in equal proportions. The manifestations of end-stage disease are typified by inanition, cachexia, aspiration, respiratory difficulty due to trouble with secretions or obstruction, fistulas, oral or neck ulceration, edema of the mucosal structures or face, and pain. Among survivors, the risk of second primary head and neck, lung, and esophagus tumors is a perplexing problem.
The differences among carcinomas of the head and neck relate mostly to site, with nasopharynx cancer representing a distinct clinicopathologic entity with unique demographics, etiologic associations, and high susceptibility to radiotherapy and chemotherapy. Cancers that develop at particular sites manifest different presenting symptoms, such as hoarseness with early vocal cord cancer, pain with anterior tongue cancer, and sore throat or dysphagia with pharynx or supraglottic larynx cancer. Cancers at different sites also show clinically important differences in the development of bilateral lymph node or hematogenous metastasis, and comprehensive treatment plans take those differences into account.
II. Primary treatment
A detailed discussion of the specific treatment options for each site and stage, and how one selects a specific treatment for a particular patient is beyond the scope of this chapter. However, a process that identifies and clarifies the goal(s) of treatment and reflects input from the patient and the treatment team members head and neck surgeon, radiation oncologist, and medical oncologist can yield a consensus assessment. In most cases, such a consensus can be reached and the role of chemotherapy will be clearly defined.
A.
Small lesions without regional extension are generally treated with surgery or radiation The choice is usually related to the anticipated functional impact of the surgical deformity in relation to the expected complications of radiation. Secondary considerations of surgical risk for patients with significant comorbidities and compliance with daily radiotherapy treatments for patients with suboptimal social supports may be determinative.
B.
Larger primary cancers and those with clinically detectable spread to lymph nodes at diagnosis are usually treated with a combination of surgery and radiation, chemotherapy and radiation, or surgery, radiation, and chemotherapy. Disease that is unresectable at the outset rarely becomes resectable and most often will benefit from a combination of chemotherapy and radiation.
C.
Combined modality treatment plans have as their goal improved outcome (decreased local, regional, or distant failure
P.217
rates, improved survival) or decreased morbidity. How best to combine chemotherapy, radiation and surgery, and the optimal regimen for generalized use has been the focus of clinical research for the past three decades. Only recently have the benefits of combined modality treatment from these multidisciplinary efforts been realized. The addition of chemotherapy concurrently to radiation therapy results in up to a 4% to 8% absolute improvement in survival a 12% to 19% reduction in the risk of death, whether in definitive or postoperative settings. It has been more difficult to reproducibly demonstrate a survival benefit for induction chemotherapy. Although substantial progress has been made in improving end results for early stage lesions at many sites and in decreasing the morbidity and deformity from treatment, the outcome for tumors in advanced stages remains poor. For Stage III disease, the 3- to 5-year survival rate is 25% to 60%. For Stage IV disease, long-term survival ranges of 10% to 30% have been reported.
The good news is that many regimens and approaches yield similar results, which enables individualized patient care. This ability to individualize patient care, however, adds complexity and may lead to differences of opinion because the initial treatment is dependant on individual patient factors integrating site, stage, general health status, comorbidity, and goals of care.
III. Staging
Pretreatment determination of disease extent is the starting point for the care of patients with head and neck cancers.
A. TNM (Tumor, node, and metastases) classification
The American Joint Committee on Cancer (AJCC) TNM staging system integrates clinical and pathologic information on site, size, and functional consequences of the primary tumor (T), the size, number, and location of regional lymph nodes (N), and the presence of detectable distant metastases (M). The stage groupings identify patients with similar prognosis despite differences in disease extent represented by combinations of the TNM components. Table 6.2 shows the AJCC sixth edition TNM criteria and stage grouping for oral cavity cancers. Each disease site within the head and neck region has its own criteria and so reference to these prognostic groups is an essential part of the staging process. The TNM criteria for head and neck cancer recognize the adverse prognosis conferred by initial extent of disease that precludes complete surgical resection.
B. Stage grouping
The stage grouping for head and neck cancers is shown in Table 6.3. Stages I and II are determined by the size of the tumor in the absence of nodal involvement or distant metastases. Stage III includes both large tumors and tumors of any size with early regional node involvement. Stage IV lesions may be huge with local extension or may be of any size with distant metastatic disease. This stage grouping has been applied to each tumor site to demonstrate gradations in prognosis.
IV. Chemotherapy
Chemotherapy has many roles in the treatment of head and neck cancer, and the selection of agents and regimens are tailored to the specific role. Chemotherapy is often used to palliate patients with locally recurrent or metastatic
P.218
disease, and it is frequently used as a radiation sensitizer in simultaneous chemoradiation programs, either as initial treatment or following surgery. Less frequently, chemotherapy is used before radiation or surgery as initial treatment in a neoadjuvant or induction role or as a single adjuvant modality after surgery or radiation.
Table 6.2. TNM Staging System for Carcinomas of the Oral Cavity | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||
The benefits of chemotherapy are always considered in relation to the expected chemotherapy-related adverse effects. Chemotherapy added to radiotherapy clearly improves outcome in patients with nasopharynx cancer, unresectable disease, and in patients with resected tumors and adverse pathologic findings. Recently, improvements in supportive care have allowed for the development of more intensive and complex chemotherapeutic regimens. Although antitumor responses have improved, other measures of benefit are more difficult to demonstrate consistently. The routine use of more intensive and complex regimens necessitates careful patient selection and aggressive supportive care interventions. A commitment to aggressively
P.219
manage toxicity goes hand in hand with the use of regimens that have substantial rates of severe or life-threatening side effects.
Table 6.3. Stage Grouping for Carcinomas of the Oral Cavity, Pharynx, Hypopharynx, Larynx, and Paranasal Sinuses | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
A. Predictive factors
The top three predictive factors for antitumor response include stage group, performance status, and prior treatment. Table 6.4 lists factors identified as having a positive or negative influence on the response to chemotherapy.
Stage group. Small tumors with minimal regional node involvement respond more reliably (completely) to chemotherapy compared with larger tumors with extensive large regional nodes. Response rates are lowest for pulmonary or visceral metastases.
Performance status. Poor performance status shifts the balance toward increased toxicity, and the ability to deliver treatment is often compromised. Excellent performance status facilitates treatment and is correlated positively with response and survival. Because intensive and complex regimens select patients with excellent performance status, they may appear to represent an improvement.
Prior treatment. Head and neck cancers previously treated with surgery or radiation or both respond less frequently than patients treated initially with chemotherapy. This marked difference has fueled enthusiasm for neoadjuvant treatment programs. The failure to respond to radiation and a rapid recurrence after radiation have also been shown to affect response rates adversely.
Human papillomavirus associated cancers. These squamous cell cancers have a better outcome.
B. Patient assessment
The initial assessment focuses on disease extent and treatment goals; that process will determine the role of chemotherapy and thereby the suitable regimens and chemotherapeutic agents. Chemotherapeutic drugs used
P.220
in head and neck cancer affect the bone marrow, kidneys, peripheral nerves, mucosal integrity, and fertility. A careful medical history, systems review, physical examination, and complete laboratory evaluation are the next steps, and will help define areas of special concern for particular patients. Evaluation of the patient's (1) ability to perform self-care functions related to hydration and nutrition, (2) pain management, and (3) type and extent of social support is also essential. Attention to nutritional support is required from the outset as many patients have undergone a period of impaired nutrition during the diagnostic and staging process. Education on self-care as well as caregiver education is especially important if toxicity is to be minimized and successfully managed. The oncologist must evaluate and monitor several specific systems initially and during treatment:
Table 6.4. Factors Prognostic for Response to Chemotherapy | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||
Bone marrow function. Chronic alcoholism, malnutrition, and tumor-related weight loss contribute to a significant incidence of folate deficiency and decreased bone marrow reserve in many patients. Careful evaluation of baseline anemia or thrombocytopenia calls for proactive plans to carefully monitor and support granulocytes, red cell mass, and platelets.
Pulmonary function. Current or distant heavy smoking increases the likelihood of chronic obstructive pulmonary disease (COPD) and chronic bronchitis, leading to an increased risk of pulmonary infection during treatment. Impaired pulmonary reserve coupled with a propensity for aspiration related to tumor effects on swallowing or the clearing of secretions make it important to assess, monitor, and assist with airway issues and respiratory complaints.
P.221
Smoking cessation, mucolytics, home suction, nasogastric or gastrostomy tube feedings, and tracheostomy and tracheostomy care are all important adjuncts. Taxanes, cetuximab, tyrosine kinase inhibitors, and bleomycin may lead to acute or chronic pulmonary toxicity; therefore careful baseline assessment and monitoring is indicated.Renal function. Platinum compounds are first-line agents for most patients with head and neck cancer. Adequate baseline renal function, hydration and continued monitoring of renal function is needed to administer these agents safely and prevent renal failure. Methotrexate is also a useful agent, and renal impairment causes decreased excretion and prolonged exposure of normal tissues, resulting in increased Toxicity.
Hepatic function. The presence of cirrhosis, whether related to alcoholism or viral hepatitis, can complicate management, as it can impair the ability to accomplish forced hydration by leading to third-space accumulations of ascites or edema. Cytopenias may accompany congestive splenomegaly, and baseline diuretic use may exacerbate treatment-related electrolyte abnormalities.
Neuropathy. Significant peripheral or autonomic neuropathy may complicate alcoholism or diabetes, and may need careful assessment and monitoring related to the use of platinum compounds and taxanes, especially in combination. Occupational, recreational, and age-related hearing loss occur commonly, and a baseline hearing test is often indicated if cisplatin is to be included in the treatment plan.
Fertility. All chemotherapeutic agents may impair fertility either temporarily or permanently. For men who wish to ensure their reproductive capacity, sperm donation should be accomplished promptly. For women, induced ovulation and harvest and preservation of ova may delay chemotherapy and radiation, and for such patients it may be preferable to favor a treatment plan that begins with surgery.
Concomitant drugs. Antihypertensives, diuretics, and drugs used for glycemic control all need careful assessment, monitoring, and adjustment during therapy as patients undergo chemotherapy for head and neck cancer. Nausea, vomiting, anorexia, and limited oral intake often lead to substantial dehydration and weight loss, making hypotension a common occurrence during therapy. The use of glucocorticoids as an adjunct to antiemetics and to prevent anaphylactic reactions, coupled with irregular feeding patterns make glycemic control elusive. It is best to emphasize careful monitoring to avoid hypoglycemia, rather than focus on hyperglycemia that is not metabolically (homeostatically) significant.
C. Chemotherapeutic agents
Table 6.5 lists the response rates for chemotherapeutic agents primarily derived from studies palliating recurrent head and neck cancer. Treatment of recurrent or metastatic head and neck cancer with chemotherapy has been shown to improve survival compared with best supportive care, and single agents or combinations can lead to antitumor responses in 20% to 50% of patients. Median
P.222
survival is 6 to 9 months and seems most related to performance status, disease extent, and prior therapy rather than the regimen selected.
Table 6.5. Response Rate for Single Chemotherapy Agents in Recurrent Head and Neck Cancer | ||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Cisplatin. Cisplatin is the backbone of many head and neck cancer regimens. There is little enthusiasm for its use as a single agent to treat recurrent disease, because the single-agent response rate is comparable to other drugs in this clinical setting, and the supportive care needs and toxicity may be higher than with other single agents. Significant acute and delayed nausea and vomiting require aggressive antiemetics including serotonin subtype 3 (5-hydroxytryptamine-3 [5-HT3]) receptor antagonists (ondansetron, granisetron, dolasetron, palonosetron), glucocorticoids (dexamethasone or methlyprednisolone), and neurokinin 1 (NK-1) receptor antagonists (aprepitant) for optimum control. These antiemetics have made outpatient high-dose cisplatin feasible for most patients. Cisplatin 60 to 100 mg/m2 IV given once every 3 weeks preceded by 1 to 2 L of hydration, mannitol 12.5 to 25 g, and 1 to 2 L of postcisplatin hydration with mannitol and/or furosemide 10 to 20 mg to maintain urine output is a standard regimen. Adequate replacement of potassium, magnesium, and sodium losses is needed, and monitoring with hydration as needed for 1 or 2 days after outpatient administration can avoid the serious cycle of nausea and vomiting leading to dehydration, electrolyte abnormalities, and renal failure. The total dose can be divided over 3 to 5 days and is better tolerated by some patients, but it does not alter the need for aggressive antiemetics and hydration.
Carboplatin. Carboplatin is easier to administer than cisplatin because there is no requirement for forced hydration, and less nausea and vomiting, less renal toxicity, ototoxicity, and neuropathy. Dosing incorporates renal function by use of the Calvert formula where the calculated dose in milligrams equals the (creatinine clearance +25) multiplied by an area under the curve (AUC) factor of 5 or 6. Response rates comparable to single-agent cisplatin are reported but myelosuppression, in particular thrombocytopenia, can be dose limiting. This is less suitable for ulcerated mucosa or neck lesions where bleeding may already be a management issue.
Paclitaxel. Paclitaxel 175 to 250 mg/m2 over 3 hours every 3 weeks with filgrastim(G-CSF) support is an aggressive standard single-agent dose. A response rate of 15% to 40% has been reported but enthusiasm is limited because of the risk of neutropenia and neuropathy. Premedication with glucorticoids (dexamethasone 10 20 mg) 12 hours, 6 hours, and immediately before paclitaxel administration, together with histamine H1- and H2 -receptor antagonists (diphenhydramine 50 mg and cimetidine 300 mg or famotidine 20 mg) are used to minimize anaphylactic reactions.
Docetaxel. Docetaxel 75 to 100 mg/m2 IV over 1 hour every 3 weeks or docetaxel 30 to 40 mg/m2 IV over 1 hour weekly for 4 of 5 weeks or 3 of 4 weeks may be used. Dexamethasone 8 mg twice a day for 3 days 1 day before, on the treatment day, and on the day following docetaxel infusion generally controls allergic reactions and fluid accumulations. Marrow suppression may require filgrastim support with the higher doses. Caution must be exercised when administering to patients with fluid accumulation or any hepatic dysfunction. Neuropathy may be lower than with paclitaxel but asthenia may be greater with the highdose regimen.
Methotrexate. Methotrexate doses of 40 to 60 mg/m2 IV weekly given over 15 minutes is a convenient standard single-agent treatment. Response rates and survival are comparable to combination therapy. Dose escalation can increase response rates but is accompanied by increased toxicity and does not improve survival. Minimal to moderate nausea and few significant acute side effects make this a well-tolerated and easily monitored treatment. Careful assessment of renal function, nutritional status, and volume status, are important however, because renal impairment, folate deficiency, and third-space fluid collections (pleural effusions, ascites, edema) can lead to severe Toxicity. Responses may occur after 1 or 2 weeks of treatment but usually require 4 to 8 weeks of treatment so patience is needed before abandoning this regimen. Mucositis and bone marrow suppression are the most common side effects encountered. Leucovorin 10 mg PO q6 hours x 6 or more doses starting 24 hours after methotrexate can help ameliorate these problems when they develop in responding patients who continue treatment.
Fluorouracil. Fluorouracil is well tolerated and has comparable activity to cisplatin and other single agents.
P.224
It is most often given as a 4- or 5-day continuous infusion. Common side effects include mucositis, diarrhea, and bone marrow suppression. The drug is a vascular irritant at high concentrations and therefore, for prolonged infusions, a central venous catheter or access device is customary. Although suitable for use as a single agent, it is most often used in combination with other drugs.Ifosfamide. Ifosfamide 1,000 mg/m2/day IV over 2 hours x 4 days every 3 to 4 weeks yields response rates of 20% to 40%. The need for uroprotection with mesna 200 mg/m2 before and 400 mg/m2 after ifosfamide makes this a cumbersome single-agent regimen to administer. Bone marrow toxicity can be significant and often requires filgrastim support.
Bleomycin. Bleomycin is useful in head and neck cancer because of antitumor activity comparable to other agents without associated myelosuppression or nausea. Bleomycin 10 to 30 units/m2 IM or IV can be given weekly, every 2 weeks, or 5 days a month. Mucositis is commonly seen and responses are often very brief. Pulmonary toxicity is a significant problem when cumulative doses reach the range (400 units) in which responses typically occur.
Gemcitabine. Gemcitabine 1,000 mg/m2 weekly has activity in nasopharynx cancer and is well tolerated. Bone marrow toxicity is the major adverse effect.
Cetuximab. Cetuximab is a monoclonal antibody that binds to epidermal growth factor receptors, which are overexpressed in more than 90% of head and neck squamous cell carcinomas. The standard regimen begins with a loading dose of Cetuximab 400 mg/m2 IV given over 2 hours followed by weekly doses of 250 mg/m2 IV over 1 hour. Responses of up to 10% have been observed among cisplatin-resistant patients. Skin rash and diarrhea are the common side effects. Allergic reactions are preventable in most cases with diphenhydramine 50 mg premedication. Interstitial pneumonitis is rare but can be life threatening or fatal. Cisplatin-based combinations with cetuximab have reported a higher response rate compared with single-agent cisplatin.
Tyrosine kinase inhibitors. Erlotinib 150 mg orally once a day and gefitinib 250 to 500 mg orally once a day have been shown to result in a response rate of 10% among patients who have failed prior cisplatin chemotherapy. The high dose of gefitinib appears to be more active than the lower dose in head and neck cancer, and although no longer commercially available, gefitinib remains under active investigation in combination with other agents and radiation therapy. Other tyrosine kinase inhibitors are also under investigation.
Anthracyclines. Doxorubicin and mitoxantrone are useful in nasopharynx cancer, which is very responsive to multiple agents; many patients are younger with good performance status so that they often tolerate and respond to multiple sequential treatment regimens. These agents have utility in that setting.
Vinca alkaloids. Vincristine and vinblastine have low single-agent response rates and are generally not used. Vinorelbine 30 mg/m2 weekly is reported to produce 8 to 16% response rate.
P.223
P.225
D. Combination chemotherapy
The basic principle of combination chemotherapy is to combine agents with complementary or synergistic mechanisms of action and non-overlapping toxicity for improved antitumor response and outcome. Many chemotherapy combinations have been tested in head and neck cancer and have come to be utilized for the palliation of recurrent and metastatic disease, in simultaneous chemoradiation treatment programs, and in neoadjuvant treatment regimens. In general, response rates are improved with combinations but survival has not been shown to be better than that obtained with several single agents. Toxicity is usually greater, and therefore combination therapy is most appropriate for patients with an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. The goal of treatment and the clinical setting help select the most appropriate regimen for the particular patient. Simpler regimens are often favored; however, patient factors frequently make the most effective of the simpler drug regimens problematic. The most commonly used combinations used are listed in Table 6.6. Selected regimens for palliation, neoadjuvant therapy, or concurrent chemoradiotherapy are shown in Table 6.7.
Cisplatin and fluorouracil. Cisplatin 75 to 100 mg/m2 is given intravenously over 1 to 4 hours on day 1 and fluorouracil 600 to 1,000mg/m2/ day is given as a 96-to 120-hour continuous infusion for 4 or 5 days. Forced hydration, aggressive antiemetics, and close monitoring for electrolyte abnormalities, mucositis, dehydration, and cytopenias are needed. Recently, it had been appreciated that significant rates of neutropenia accompany this regimen and that these patients may benefit from filgrastim and prophylactic antibiotics. When this regimen is used during or after prior radiotherapy, only 4 days (96 hours of continuous infusion) of fluorouracil are used because of enhanced mucosal and skin toxicity in that setting.
Table 6.6. Response Rate for Combination Chemotherapy Agents in Recurrent Head and Neck Cancer
Agents Approximate Response Rate Cisplatin/fluorouracil 25% 40% Carboplatin/fluorouracil 26% Cisplatin/paclitaxel 28% 35% Cisplatin/docetaxel 42% Cisplatin/cetuximab 26% Methotrexate/bleomycin/cisplatin 48% Paclitaxel/ifosfamide/carboplatin 55% In nasopharynx cancer Gemcitabine/paclitaxel 41% P.226
Table 6.7. Selected Drug Treatment Programs in Head and Neck Cancer
Intent Suitability Scheme Palliation Any prior treatment Either Cisplatin 20 mg/m2 IV on days 1 5 or cisplatin 100 mg/m2 day 1 and fluorouracil 800 1000 mg/m2/day as 24-h infusion on days 1 4 by ambulatory infusion pump or carboplatin AUC 5 6 on day 1 and fluorouracil 800 1000 mg/m2/day as 24-h infusion on days 1 4 by ambulatory infusion pump or paclitaxel 135 mg/m2 IV day 1 and cisplatin 75 mg m2 or docetaxel 75 mg/m2 day 1 and cisplatin 75 mg/m2 day 1 Cycle repeats in 3 4 weeks Paclitaxel 175 mg/m2 as 3-h infusion on day 1 with steroid premedication and carboplatin AUC 6 on day 1 Cycle repeats in 4 weeks Methotrexate 40 60 mg/m2 IV weekly or Prior treatment and contraindications to combination drugs paclitaxel 175 200 mg/m2 IV every 3 weeks with steroid premedication, or
docetaxel 75 100 mg/m2 over 1 h with steroid premedication every 3 weeks or
docetaxel weekly 35 mg/m2 day 1 on 3 of 4 weeks.
Cycles repeat every 28 daysRefractory to cisplatin Cetuximab 400 mg/m2 IV day 1 then 250 mg/m2//week Concurrent radiotherapy Advanced stage, no prior treatment Daily radiation therapy together with either:
cisplatin 100 mg/m2 IV on day 1 with induced diuresis, repeat day 22, 43, or
carboplatin 70 mg/m2 on day 1 4 and
fluorouracil 600 mg/m2/day as 24-h infusion on day 1 4 by ambulatory infusion pump;
repeat days 23, 43
or
hydroxyurea 1,000 mg PO Q 12 h for 11 doses and
fluorouracil 1,000 mg/m2/day as 24-h infusion on days 1 4 by ambulatory infusion pump
or
twice a day radiotherapy with either
cetuximab 400 mg/m2 day 1 then 250 mg/m2 weekly
or
cisplatin 12 mg/m2 IV on days 1 5 with induced diuresis, repeat days 35 40 and
fluorouracil 600 mg/m2/day as 24-h infusion on days 1 5 by ambulatory infusion pump; repeat days 35 40Neoadjuvant (Induction) chemotherapy Advanced stage, no prior treatment, concomitant chemoradiation contraindicated CF
Cisplatin 100 mg/m2 IV on day 1 with induced diuresis and
fluorouracil 1,000 mg/m2/day as 24-h infusion on days 1 5
Cycle repeats in 3 4 weeks or
TPF
Docetaxel 75 mg/m2 day 1
cisplatin 100 mg/m2 day 1,
fluorouracil 1000 mg/m2/day as 24-h infusion days 1 4 (96 h)Carboplatin and fluorouracil. Carboplatin 300 mg/m2 IV on day 1 and fluorouracil 1,000 mg/m2/day by continuous infusion for 4 days are used for recurrent disease with responses and survival comparable to cisplatin and fluorouracil. For simultaneous chemoradiation in oropharynx cancer, carboplatin 70 mg/m2 IV daily for 4 days and fluorouracil 600 mg/m2 daily by continuous infusion (96 hours) for 4 days is a standard regimen. These regimens predate the use of the Calvert formula but roughly correspond to an AUC of 5 and AUC of 1.25 respectively.
Cisplatin and paclitaxel. Cisplatin 60 mg/m2 IV and paclitaxel 135 to 175 mg/m2 IV every 3 weeks were found
P.228
to be equivalent to fluorouracil regimens in patients with recurrent disease. The lower dose of paclitaxel was better tolerated. Careful monitoring for neuropathy is needed.Carboplatin and paclitaxel. Carboplatin AUC 6 and paclitaxel upto 175 mg/m2 given every 3 weeks is a widely utilized combination regimen with similar results.
Cisplatin and docetaxel. Cisplatin 75 mg/m2 IV and docetaxel 75 mg/m2 IV each on day 1 every 3 weeks. Frequent neutropenia is seen in this regimen.
Cisplatin, methotrexate, and bleomycin is an older combination regimen found to have superior response compared with methotrexate. Cisplatin-induced renal impairment can lead to profound toxicity if methotrexate excretion is prolonged.
Paclitaxel and gemcitabine. This non-cisplatin combination is useful in patients with recurrent nasopharynx cancer, most of whom are heavily pretreated with cisplatin.
Paclitaxel, ifosfamide, and carboplatin is a threedrug regimen with high activity and is well tolerated but requires good performance status of patients and filgrastim support.
P.227
E. Chemotherapy as a radiation sensitizer
Simultaneous chemoradiation was first demonstrated to be beneficial in nasopharynx cancer. It has subsequently been shown to improve survival among other patients with unresectable disease, to positively contribute to organ preservation in advanced larynx cancer, and to improve outcome following surgery where a positive margin, spread through the lymph node capsule, and multiple positive nodes are found. As indicated in the preceding text in Section II, the addition of chemotherapy concurrently to radiation therapy results in up to a 4% to 8% absolute improvement in survival a 12% to 19% reduction in the risk of death, whether in definitive or postoperative adjuvant settings. Simultaneous chemoradiation is also effective in treating paranasal sinus cancer (by either intra-arterial or intravenous route) where surgery is not recommended. Although many regimens have been tested in these various settings, the high-dose cisplatin regimen has been most consistently effective. A variety of radiotherapy treatment programs have been tested with chemotherapy, therefore it is also important to clarify what radiotherapy regimen will be utilized when selecting chemotherapy for concomitant treatment.
Cisplatin 100 mg/m2 IV over 1 to 4 hours every 21 days during radiation. This regimen has been shown to be effective in improving survival compared with radiotherapy alone in nasopharynx cancer, for organ preservation in larynx cancer, and as adjuvant chemoradiation for patients with adverse prognostic factors after surgery. The Radiation Therapy Oncology Group (RTOG) demonstrated 83% organ preservation rate in larynx cancer, and the European Organization for Research and Treatment of Cancer (EORTC) and RTOG demonstrated a benefit when cisplatin was given with postoperative radiation for patients with positive margins, extracapsular lymph node extension or multiple involved nodes. Weekly regimens using lower-dose cisplatin have yielded conflicting results.
Carboplatin and fluorouracil. For simultaneous chemoradiation in oropharynx cancer, carboplatin 70mg/m2 IV daily for 4 days and fluorouracil 600 mg/m2 daily for 4 days by continuous infusion (96 hours) is a standard regimen.
Cetuximab 400 mg/m2 IV day 1 as a loading dose followed by 250 mg/m2 IV weekly during radiation is an effective radiosensitizer. Most patients are treated with twice-a-day radiation or a concomitant boost radiation schedule. There is improved survival as compared with radiation alone. This regimen has a very good toxicity profile.
Cisplatin and fluorouracil. Cisplatin 60 to 75 mg/m2 IV day 1 and fluorouracil 600 to 1,000 mg/m2 daily for 4 days by continuous 96-hour infusion is a standard regimen with single fraction or hyperfractionated radiation. Mucosal toxicity is significant.
Hydroxyurea and fluorouracil (HFX). The combination of hydroxyurea 1,000 mg orally every 12 hours for 11 doses and fluorouracil 800 mg/m2 daily for 5 days given as a 120-hour intravenous infusion repeated every 14 days for 5 cycles concomitantly with radiotherapy for 5 days every 14 days is an effective non-cisplatin regimen. This regimen significantly prolongs treatment time as treatment including radiotherapy is administered every other week. It may be feasible for selected patients.
Cisplatin and paclitaxel. Cisplatin 20 mg/m2 weekly and paclitaxel 30 mg/m2 weekly during standard fractionated radiation.
Paclitaxel. Paclitaxel 20 to 40 mg/m2 given over 1 hour weekly during radiotherapy has been tested. Mucosal toxicity, which may be delayed, is dose limiting.
Paclitaxel, hydroxyurea, and fluorouracil (THFX) may be given on alternating weeks during simultaneous chemoradiation. This is an active non-platinum regimen found to be effective but requiring breaks in radiotherapy and aggressive supportive care. It is feasible but complex.
P.229
F. Neoadjuvant chemotherapy
Response rates are much higher for patients who have had no prior treatment than for those who have been treated with prior surgery, radiation, or both. Therefore the development of combination regimens for use in induction or neoadjuvant treatment programs continues to attract interest.
The initial demonstration that organ preservation could be accomplished by substituting chemotherapy for surgery led to widespread adoption of neoadjuvant approaches. In particular, this approach was demonstrated to be comparable to surgery in patients who would require total laryngectomy for larynx cancer, hypopharynx cancer, or functionally morbid oropharynx cancer. Treatment for 6 to 9 weeks (two to three cycles) is usually given to induce an antitumor response. Partial and complete responders can be treated with radiotherapy or chemoradiotherapy. Surgery can be integrated for nonresponders and those with persistent or recurrent disease. Only regimens containing cisplatin and fluorouracil have been found to improve survival. This strategy is equivalent to surgery and radiation in resectable larynx and hypopharynx
P.230
cancer where total laryngectomy is the recommended surgical option. Simultaneous cisplatin and radiotherapy is superior for organ preservation but not for survival in larynx cancer. Simultaneous chemoradiotherapy also appears to be superior for unresectable disease. Separating chemotherapy and radiation may be appropriate for selected patients who may not tolerate the simultaneous regimens well, but simultaneous regimens are currently preferred when feasible. Taxanes added to cisplatin and fluorouracil appear to be more active. Current investigational approaches are exploring neoadjuvant chemotherapy followed by chemoradiation in an attempt to improve survival outcome by maximizing chemotherapy to reduce distant metastases.
Cisplatin and fluorouracil. Cisplatin 100 mg/m2 IV on day 1 and fluorouracil 1,000 mg/m2 as a 24-hour continuous IV infusion on days 1 to 5 every 21 days for three cycles. This is the standard regimen for neoadjuvant chemotherapy.
Docetaxel, cisplatin, and fluorouracil. Docetaxel 75 mg/m2 IV on day 1, cisplatin 100 mg/m2 IV on day 1, and fluorouracil 1,000 mg/m2 IV daily on days 1 to 4 (96 hour continuous infusion) every 3 weeks for 3 cycles. This regimen requires prophylactic fluoroquinolone antibiotics.
Paclitaxel, cisplatin, and fluorouracil. Paclitaxel 175 mg/m2 IV on day 1, cisplatin 100 mg/m2 IV on day 2, and fluorouracil 500 mg/m2 daily for 5 days by continuous infusion (120 hours) every 3 weeks for 3 cycles.
Paclitaxel, ifosfamide, and carboplatin. Paclitaxel 175 mg/m2 IV on day 1, ifosfamide 1,000 mg/m2 IV on days 1 to 3 (with intravenous mesna 200 mg/m2 IV before and 400 mg/m2 IV after ifosfamide), and carboplatin IV at AUC 6 This is repeated every 3 to 4 weeks for two to four cycles. Filgrastim is recommended, given the 9% risk of febrile neutropenia.
Carboplatin and paclitaxel. Carboplatin IV at AUC 2 on day 1 and paclitaxel 135 mg/m2 IV on day 1 weekly for 6 weeks is a simple outpatient regimen with acceptable response rate. Neutropenia is seen in 18% of patients, but febrile neutropenia is uncommon.
G. Adjuvant chemotherapy
Adjuvant chemotherapy is part of the standard regimen for nasopharynx cancer. Patients are given two or three cycles of cisplatin 80 mg/m2 IV and fluorouracil 1,000 mg/m2 daily for 4 days by continuous infusion following initial chemoradiation using cisplatin as a single agent. It is poorly tolerated and has not been isolated by testing apart from the initial simultaneous chemoradiation. Several older phase III studies of adjuvant chemotherapy showed no benefit, although these studies were limited by small sample size, as well as by poor tolerance and compliance with therapy.
Adjuvant chemoradiation is indicated for high-risk patients after surgery as previously discussed.
V. Supportive care
A. Support systems
The head and neck cancer patient population includes many older people who are often socially isolated because of the behavioral effects of chronic alcohol abuse;
P.231
many live alone, are separated from family, and have few social or monetary resources. These patients need a primary caregiver to be in the house or nearby. Even among patients with extensive social supports and resources, it is difficult to comply with the prescribed multimodality treatment and self-care regimens for nutrition, mouth or wound care, pain control, and antiemetics. Depression and hopelessness, coupled with moderate to severe treatment-related symptoms often test the patient's commitment to the initial treatment goals, and inadequate social supports tend to exacerbate this problem. Early evaluation by a trained social worker, who can assist with counseling and problem solving, and facilitate hospital and community-based support services is essential. The American Cancer Society's support groups and patient assistance programs, Alcoholics Anonymous, and other social care organizations should be enlisted as part of the treatment team.
B. Nutrition
Adequate nutrition is an essential component of any medical management plan. A poor nutritional state is associated with impaired healing, increased toxicity of treatment, an impaired sense of well-being, and fatigue. Tumor location, surgical or radiation-related treatment effects, chemotherapy, and progressive cancer all lead to symptoms that can cause impaired nutrition. Patients with head and neck cancer often experience dysphagia, odynophagia, dysguesia, xerostomia, poor dentition, mucositis, nausea, vomiting, and anorexia at some point during the illness. These symptoms may be persistent and compromise nutrition by preventing adequate oral feeding. Early consultation with a clinical nutritionist is usually helpful, coupled with the setting of clear calorie goals and strategies for reaching those goals. For most patients, a goal of 2,000 to 2,500 kcal/day or more is needed to maintain weight and re-establish nutritional homeostasis. Reinforcing the nutrition plan with the patient and caregiver is essential. Many patients prefer to blend home foods into a form they can manage, whereas others prefer the prepared liquid nutritional supplements, which are a convenient alternative that greatly facilitates reaching the recommended calorie goals by providing a balanced source of calories in a relatively small volume. Endoscopically or percutaneously placed gastrostomy tubes greatly facilitate enteral feeding when patients are unable to take adequate calories or hydration by mouth. Several of the intensive chemoradiation programs rely on gastrostomy tube feeding and hydration and the long-term impact on swallowing function may be substantial and requires further study. Among patients who are cured, frequently the time and effort needed to eat limit adequate caloric intake. For patients undergoing palliative chemotherapy or supportive care only, adequate nutrition enhances well-being.
C. Mouth care
Mouth care is an important part of the support for patients undergoing treatment for head and neck cancer. Tumor involvement and the effects of surgery, radiation, or chemotherapy can all cause problems that can be helped by mouth care intervention.
Initial dental evaluation is important if prosthetics will be required after surgery, and dental procedures should be performed before radiotherapy in patients who will receive
P.232
radiation. Mucositis due to chemotherapy and radiation is a major problem and requires frequent monitoring and recognition of treatable problems that may develop such as herpes virus reactivation and superinfection with candida or pathogenic bacteria. Salt and soda mouthwashes, sucralfate mouthwashes, and a variety of mouthwash mixtures, some that contain topical anesthetics, (but not chlorhexidine) may be used to promote optimum oropharyngeal hygiene, decrease inflammation, and treat pain (see Chapter 27-III). Clinical trials of palifermin a keratinocyte growth factor effective in preventing oral mucositis in patients receiving high dose chemotherapy and total-body radiotherapy for hematologic malignancies are under way and show promise in ameliorating mucositis in patients with head and neck cancer undergoing chemoradiation. Radiation-induced bone necrosis or tumor-related fistulas need to be cleaned or debrided and occasionally packed with toothpaste or other material to promote comfort. Metronidazole 500 mg three times a day can improve tumor odor that is distressing to both the patient and caregivers.
A common problem during and after radiotherapy is dry mouth xerostomia. Sugarless gum or lozenges, artificial saliva, and pilocarpine 5 to 10 mg orally t.i.d. or cevimiline 30 mg orally t.i.d. are remedies acceptable to many patients. Amifostine, a thiophosphate compound that can protect normal tissues against chemotherapy and radiation side effects, has been shown to decrease radiation-related acute and chronic xerostomia in patients with head and neck cancer. It is given intravenously at a dose of 200 mg/m2/day as a slow IV push 15 to 30minutes before each fraction of radiotherapy. Side effects include nausea requiring 5HT-3 serotonin receptor antagonists, hypotension, and allergic reactions. These factors and the demonstration of only modest long-term benefits have limited its routine use. Subcutaneous dosing has been investigated.
D. Aspiration pneumonia
Many patients suffer from dry mouth, whereas others have copious or thick mucoid secretions and suffer from an inability to clear them because of anatomic factors. Such patients benefit from mucolytics, such as guanifensin, and portable suction machines.
These patients frequently suffer episodes of aspiration pneumonia. Fever, tachycardia, tachypnea, rales, and infiltrates in the lung are usual findings but sometimes microaspiration can simulate pulmonary metastasis. Awareness of this propensity, focusing on a careful history, and comprehensive evaluation followed by treatment with steroids, antibiotics, or both will usually manage the acute problem. A swallowing evaluation may lead to speech and swallowing therapy. Nevertheless, feeding by gastrostomy tube or laryngectomy may be the only solution if the aspiration episodes are frequent or life threatening.
E. Granulocytopenia and infection
Combination chemotherapeutic regimens have an increased risk of granulocytopenia, and patients with head and neck cancer often have multiple risk factors for developing febrile neutropenia. Pulmonary, oropharyngeal, and IV access line infections are common in this patient population and mortality is high
P.233
when granulocytopenia is present. Prophylactic filgrastim or pegfilgrastim should be administered to those with intermediate or high-risk patient factors such as age above 65, poor nutritional status, extensive prior chemotherapy, open wounds, COPD, and low baseline hemoglobin. If fever develops, evaluation with appropriate cultures and treatment with broad-spectrum antibiotics should be instituted promptly (see Chapter 28).
F. Anemia
Anemia is uncommon during chemoradiation for head and neck cancer but is more frequent during treatment for recurrent disease and in neoadjuvant regimens. One clinical trial found decreased survival when erythropoietin was used to achieve a target hemoglobin of 15 g/dL. Transfusion and erythropoietin can ameliorate fatigue and other symptoms related to anemia associated with hemoglobin levels below 12 g/dL.
G. Hypothyroidism
Weakness, apathy, listlessness, and weight loss may develop insidiously in patients subjected to thyroid irradiation or resection. Estimates are as high as 25% to 50% for radiation doses above 6,000 cGy. Such symptoms may mistakenly be construed as suggesting disease relapse. Monitoring for this phenomenon should continue indefinitely.
H. Hypercalcemia
Hypercalcemia is a common manifestation of late-stage recurrent tumor and is usually caused by parathyroid hormone related protein (PTHrp). It may be precipitated by dehydration but up to 23% of patients with advanced recurrent head and neck cancers will manifest hypercalcemia before death. In most such patients, it is mild and easily controlled with hydration, saline diuresis, or bisphosphonate therapy (see Chapter 30). If patients have advanced disease without the hope of substantial palliation, comfort care is a reasonable choice.
VI. Cancer prevention
Many patients who are cured of head and neck cancer survive to develop second primary cancers of the head and neck or lung, related in part to a field cancerization effect of tobacco and alcohol exposure. Smoking cessation and abstinence from alcohol are important adjuncts to the care of these patients.
Isotretinoin (13-cis-retinoic acid) can reverse oral premalignancy; a high dose of 1 to 2 mg/kg was shown to prevent second primary cancers in patients with head and neck cancer but lower, more tolerable doses were ineffective. Tobacco control is the single most important preventive effort under way. The control of HPV infections may lead to decreases in tumors associated with this virus.
Suggested Readings
Adelstein DJ, Li Y, Adams GL, et al. An intergroup phase III comparison of standard radiation therapy and two schedules of concurrent chemoradiotherapy in patients with unresectable squamous cell head and neck cancer. J Clin Oncol 2003;21:92 98.
Al-Sarraf M, LeBlanc M, Giri PG, et al. Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal cancer: phase III randomized Intergroup study 0099. J Clin Oncol 1998;16:1310 1317.
P.234
Bernier J, Cooper JS, Pajak TF, et al. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck 2005;27:843 850.
Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med 2006;354(6):567 578.
Brizel DM, Albers ME, Fisher SR, et al. Hyperfractionated irradiation with or without concurrent chemotherapy for locally advanced head and neck cancer. N Engl J Med 1998;338:1798 1804.
Cohen EE. Role of epidermal growth factor receptor pathway targeted therapy in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck. J Clin Oncol 2006;24:2659 2665.
Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 2004;350:1937 1944.
Denis F, Garaud P, Bardet E, et al. Final results of the 94-01 French Head and Neck Oncology and Radiotherapy Group randomized trial comparing radiotherapy alone with concomitant radiochemotherapy in advanced-stage oropharynx carcinoma. J Clin Oncol 2004;22:69 76.
Department of Veterans Affairs Laryngeal Cancer Study Group. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. N Engl J Med 1991;324:1685 1690.
Fakhry C, Gillison ML. Clinical implications of human papillomavirus in head and neck cancers. J Clin Oncol 2006;24:2606 2611.
Forastiere AA, Ang K, Brizel D, et al. Head and neck cancers. J Natl Compr Canc Netw 2005;3(3):316 391.
Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med 2003;349:2091 2098.
Forastiere AA, Metch B, Schuller DE, et al. Randomized comparison of cisplatin plus fluorouracil and carboplatin plus fluorouracil vs. methotrexate in advanced squamous-cell carcinoma of the head and neck: A Southwest Oncology Group study. J Clin Oncol 1992;10:1245 1251.
Forastiere AA, Trotti A, Pfister DG, et al. Head and neck cancer: recent advances and new standards of care. J Clin Oncol 2006;24:2603 2605.
Garden AS, Harris J, Vokes EE, et al. Preliminary results of Radiation Therapy Oncology Group 97-03: a randomized phase II trial of concurrent radiation and chemotherapy for advanced squamous cell carcinomas of the head and neck. J Clin Oncol 2004;22:2856 2864.
Gibson MK, Li Y, Murphy B, et al. Randomized phase III evaluation of cisplatin plus fluorouracil versus cisplatin plus paclitaxel in advanced head and neck cancer (E1395): an intergroup trial of the Eastern Cooperative Oncology Group. J Clin Oncol 2005;23:3562 3567.
P.235
Greene FL, Page DL, Fleming ID, et al. eds. AJCC cancer staging manual, 6th ed. New York: Springer-Verlag, 2002. Hitt R, Lopez-Pousa A, Martinez-Trufero, et al. Phase III study comparing cisplatin plus fluorouracil to paclitaxel, cisplatin, and fluorouracil induction chemotherapy followed by chemoradiotherapy in locally advanced head and neck cancer. J Clin Oncol 2005;23:8636 8645.
Kim JG, Sohn SK, Kim DH, et al. Phase II study of concurrent chemoradiotherapy with capecitabine and cisplatin in patients with locally advanced squamous cell carcinoma of the head and neck. Br J Cancer 2005;93:1117 1121.
Lefebvre J-L, Chevalier D, Luboinski B, et al. Larynx preservation in pyriform sinus cancer: preliminary results of a European Organization for Research and Treatment of Cancer phase III trial. J Natl Cancer Inst 1996;88:890 899.
Piccirillo JF, Lacy PD, Basu A, et al. Development of a new head and neck cancer-specific comorbidity index. Arch Otolaryngol Head Neck Surg 2002;128:1172 1179.
Pignon JP, Bourhis J, Domenge C, et al. on behalf of the MACHNC Collaborative Group. Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: three metaanalyses of updated individual data. Lancet 2000;355:949 955.
Pfister DG, Laurie SA, Weinstein GS, et al. American Society of Clinical Oncology clinical practice guideline for the use of larynxpreservation strategies in the treatment of laryngeal cancer. J Clin Oncol 2006;24:3693 3704.