Notice
Editors: McPhee, Stephen J.; Papadakis, Maxine A.; Tierney, Lawrence M.
Title: Current Medical Diagnosis & Treatment, 46th Edition
Copyright 2007 McGraw-Hill
> Table of Contents > 2 - Common Symptoms
function show_scrollbar() {}
2
Common Symptoms
Ralph Gonzales MD, MSPH
New or unexplained symptoms account for about half of all office visits; the remainder of visits are for ongoing care of established medical conditions. Evidence-based symptom evaluation combines knowledge of a symptom's clinical epidemiology with disease candidates according to Bayesian principles (see Chapter 42), such that the likelihood of a specific disease is a function of patient demographics, comorbidities, and clinical features. This knowledge can help support decisions about further testing or treatment or whether to perform additional testing before treatment, or to treat without further testing.
In addition to epidemiologic factors, biological, psychological, social, and cultural factors affect how patients process, filter, and interpret symptoms. Patients vary in deciding when symptoms are sufficiently bothersome or worrisome to cause them to seek medical attention, and in what they expect from the office visit.
Many symptoms defy diagnosis. If symptom relief is not easily achieved, treatment of these patients becomes challenging. The shift toward evidence-based principles of medicine, which encourage narrow study questions in homogeneous study populations, inadvertently ignores syndromes that are not readily explained by current biomedical models of disease. Conversely, even when the cause of a disease is known, host and environmental factors can influence the symptoms that are manifested. For example, in 1967, Evans proposed five realities that reflect the conundrum clinicians face when associating an acute respiratory syndrome with an etiologic pathogen: (1) The same clinical syndrome may be produced by a variety of infectious pathogens; (2) the same pathogen may produce a variety of syndromes; (3) the most likely cause of a syndrome may vary by patient age, year, geography, and setting; (4) diagnosis of the pathogen is frequently impossible on the basis of clinical findings alone; and (5) the causes of a large proportion of infectious disease syndromes are still unknown.
Cough
![]() Essential Inquiries
Essential Inquiries
Duration of cough.
Dyspnea (at rest or with exertion).
Constitutional symptoms.
Tobacco use history.
Vital signs (heart rate, respiratory rate, body temperature).
Chest examination.
Chest radiography when unexplained cough lasts more than 3 6 weeks.
General Considerations
Cough adversely affects personal and work-related interactions, disrupts sleep, and often causes discomfort of the throat and chest wall. Most people seeking medical attention for acute cough desire symptom relief; few are worried about serious illness. Cough results from stimulation of mechanical or chemical afferent nerve receptors in the bronchial tree. Effective cough depends on an intact afferent-efferent reflex arc, adequate expiratory and chest wall muscle strength, and normal mucociliary production and clearance.
Clinical Findings
A. Symptoms
Distinguishing acute (< 3 weeks) and persistent (> 3 weeks) cough illness syndromes is a useful first step in evaluation. In healthy adults, most acute cough syndromes are due to viral respiratory tract infections. Additional features of infection such as fever, nasal congestion, and sore throat help confirm the diagnosis. Dyspnea (at rest or with exertion) may reflect a more serious condition, and further evaluation should include assessment of oxygenation (pulse oximetry or arterial blood gas measurement), airflow (peak flow or spirometry), and pulmonary parenchymal disease (chest radiography). The timing and character of the cough have not been found to be useful in establishing the cause of acute or persistent cough syndromes, although cough-variant asthma should be considered in adults with prominent nocturnal cough. Uncommon causes of acute cough illness should be suspected in those with heart disease (congestive heart failure [CHF]) or hay fever (allergic rhinitis) and those with environmental risk factors.
Cough due to acute respiratory tract infection resolves within 3 weeks in the vast majority of patients (over
P.22
90%). Pertussis infection should be considered in previously immunized adults with persistent or severe cough lasting more than 2 3 weeks and approaches a prevalence of 20% when cough has persisted beyond 3 weeks.
When angiotensin-converting enzyme (ACE) inhibitor therapy, acute respiratory tract infection, and chest radiograph abnormalities are absent, up to 90% of cases of persistent cough are due to postnasal drip, asthma, or gastroesophageal reflux disease (GERD). A history of nasal or sinus congestion, wheezing, or heartburn should direct subsequent evaluation and treatment, though these conditions frequently cause persistent cough in the absence of typical symptoms. Bronchogenic carcinoma is suspected when cough is accompanied by unexplained weight loss and fevers with night sweats, particularly in persons with significant tobacco or occupational exposures. Persistent cough accompanied by excessive mucus secretions suggests chronic bronchitis in a smoker, or bronchiectasis in a patient with a history of recurrent or complicated pneumonia; chest radiographs are helpful in diagnosis. Dyspnea at rest or with exertion is not commonly reported among patients with persistent cough. The report of dyspnea requires assessment for other evidence of chronic lung disease or CHF.
B. Physical Examination
Examination can direct subsequent diagnostic testing for acute and persistent cough. Pneumonia is suspected when acute cough is accompanied by vital sign abnormalities (tachycardia, tachypnea, fever) or findings suggestive of airspace consolidation (rales, decreased breath sounds, fremitus, egophony). Purulent sputum is a poor predictor of pneumonia in the otherwise healthy adult. In the outpatient setting, pneumonia was present in 4% of adults with purulent sputum compared with 2% of adults without purulent sputum (relative risk = 2.0). In addition, antibiotic treatment of adults with purulent sputum production shows no benefit. Wheezing and rhonchi are frequent findings in adults with acute bronchitis and do not represent adult-onset asthma in most cases.
Physical examination of adults with persistent cough may also reveal evidence of chronic sinusitis, contributing to postnasal drip syndrome or asthma. Chest and cardiac signs may distinguish chronic obstructive pulmonary disease (COPD) from CHF. In patients with cough and dyspnea, a normal match test (ability to blow out a match from 25 cm away) and maximum laryngeal height > 4 cm (measured from the sternal notch to the cricoid cartilage at end expiration) substantially decrease the likelihood of COPD. Similarly, normal jugular venous pressure and negative hepatojugular reflux decrease the likelihood of biventricular CHF.
Differential Diagnosis
A. Acute Cough
Acute cough may be a symptom of acute respiratory tract infection, asthma, allergic rhinitis, and CHF, as well as a myriad of other less common causes.
B. Persistent Cough
Causes of persistent cough include postnasal drip syndrome, asthma (including cough-variant asthma), GERD, chronic bronchitis, bronchiectasis, tuberculosis or other chronic infection, interstitial lung disease, and bronchogenic carcinoma. Persistent cough may also be psychogenic.
Diagnostic Studies
A. Acute Cough
Chest radiography should be considered for any adult with acute cough who shows abnormal vital signs or in whom the chest examination is suggestive of pneumonia. The relationship between specific clinical findings and the probability of pneumonia is shown in Figure 2-1. In patients with dyspnea, pulse oximetry and peak flow help exclude hypoxemia or obstructive airway disease. However, a normal pulse oximetry value (eg, > 93%) does not rule out a significant alveolar-arterial (A-a) gradient when patients have effective respiratory compensation.
B. Persistent Cough
Chest radiography is indicated when ACE inhibitor therapy-related and postinfectious cough are excluded by history or further diagnostic testing. Pertussis infection should be evaluated with polymerase chain reaction tests as well as culture from a nasopharyngeal swab specimen. When the chest film is normal, evaluation for postnasal drip, asthma, and GERD should be initiated. The presence of typical symptoms of these conditions directs further evaluation or empiric therapy, though typical symptoms are often absent. Definitive procedures for determining the presence of each are available (Table 2-1). However, empiric treatment with a maximum-strength regimen for postnasal drip, asthma, or GERD for 2 4 weeks is the recommended approach since documenting the presence of postnasal drip, asthma, and GERD does not mean they are the cause of the cough illness. In about 25% of cases,
P.23
persistent cough has multiple contributors. Spirometry may help identify large airway obstruction in patients who have persistent cough and wheezing and who are not responding to asthma treatment.
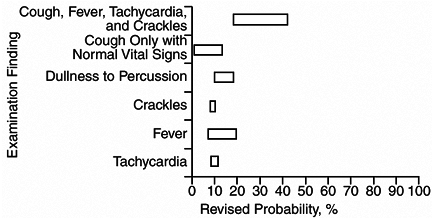 |
Figure 2-1. Revised pneumonia probabilities based on history and physical examination findings. (Reproduced, with permission, from Metlay JP et al: Testing strategies in the initial management of patients with community-acquired pneumonia. Ann Intern Med 2003;138:109. ) |
Table 2-1. Empiric treatments or tests for persistent cough. | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||
Haque RA et al: Chronic idiopathic cough: a discrete clinical entity? Chest 2005;127:1710.
Hewlett EL et al: Clinical practice. Pertussis not just for kids. N Engl J Med 2005;352:1215.
Irwin RS et al: The persistently troublesome cough. Am J Respir Crit Care Med 2002;165:1469.
Lin DA et al: Asthma or not? The value of flow volume loops in evaluating airflow obstruction. Allergy Asthma Proc 2003; 24:107.
Madison MD et al: Pharmacotherapy of chronic cough in adults. Expert Opin Pharmacother 2003;4:1039.
Metlay JP et al: Testing strategies in the initial management of patients with community-acquired pneumonia. Ann Intern Med 2003;138:109.
Schroeder K et al: Over-the-counter medications for acute cough in children and adults in ambulatory settings. Cochrane Database Syst Rev 2004;(4):CD001831.
Dyspnea
![]() Essential Inquiries
Essential Inquiries
Fever.
Cough.
Chest pain.
Vital sign measurements.
Pulse oximetry.
Chest examination.
Cardiac examination.
Chest radiography.
Arterial blood gas measurement.
General Considerations
Dyspnea is a subjective experience or perception of uncomfortable breathing. However, the relationship between level of dyspnea and the severity of underlying disease varies widely across individuals. Dyspnea can result from conditions that increase the mechanical effort of breathing (eg, COPD, restrictive lung disease, respiratory muscle weakness), from conditions that produce compensatory tachypnea (eg, hypoxemia or acidosis), or from psychogenic origins. Rate of onset, previous dyspnea, medications, comorbidities, psychological profile, and severity of underlying disorder play a role in how and when persons present with dyspnea. Nonetheless, in patients with established COPD, the severity of dyspnea is superior to forced expiratory volume in 1 second (FEV1) in predicting quality of life and 5-year mortality.
Dyspnea commonly accompanies a multitude of acute and chronic medical conditions. Acute dyspnea, particularly as the chief complaint, demands urgent evaluation. Urgent/emergent conditions causing acute dyspnea include pneumonia, COPD, asthma, pneumothorax, pulmonary embolism, cardiac disease (eg, CHF, acute myocardial infarction, valvular dysfunction, arrhythmia, cardiac shunt), metabolic acidosis, cyanide toxicity, methemoglobinemia, and carbon monoxide poisoning.
With two notable exceptions (carbon monoxide poisoning and cyanide toxicity), routine arterial blood gas measurement distinguishes increased mechanical effort causes of dyspnea (respiratory acidosis with or without hypoxemia) from compensatory tachypnea (respiratory alkalosis with or without hypoxemia or metabolic acidosis) from psychogenic dyspnea (respiratory alkalosis). Carbon monoxide and cyanide impair oxygen delivery with minimal alterations in PO2; percent carboxyhemoglobin identifies carbon monoxide toxicity. Cyanide poisoning should be considered in a patient with profound lactic acidosis following a theater fire.
Clinical Findings
A. Symptoms
The duration, severity, and periodicity of dyspnea influence the tempo of the clinical evaluation. Rapid onset, severe dyspnea in the absence of other clinical features should raise concern for pneumothorax, pulmonary embolism, or increased left ventricular end-diastolic pressure (LVEDP). Spontaneous pneumothorax is usually accompanied by chest pain and occurs most often in thin, young males, or in those with underlying lung disease. Pulmonary embolism should always be suspected when a patient reports a recent history (previous 4 weeks) of prolonged immobilization, estrogen therapy, or other risk factors for deep venous thrombosis (DVT) (eg, previous history of thromboembolism, cancer, obesity) and when the cause of dyspnea is not apparent. Silent myocardial infarction, which occurs more frequently
P.24
in diabetic persons and women, can result in acute heart failure and dyspnea.
Accompanying symptoms provide important clues to various etiologies of dyspnea. When cough and fever are present, pulmonary disease (particularly infections) is the primary concern, although myocarditis, pericarditis, and septic emboli can also present in this manner. Chest pain should be further characterized as acute or chronic, pleuritic or exertional. Although acute pleuritic chest pain is the rule in acute pericarditis and pneumothorax, most patients with pleuritic chest pain in the outpatient clinic have pleurisy due to acute viral respiratory tract infection. Periodic chest pain that precedes the onset of dyspnea is suspicious for myocardial ischemia as well as pulmonary embolism. Most cases of dyspnea associated with wheezing are due to acute bronchitis; however, when acute bronchitis seems unlikely, the clinician should also consider new-onset asthma, foreign body, and vocal cord dysfunction.
When a patient reports prominent dyspnea with mild or no accompanying features, consider noncardiopulmonary causes of impaired oxygen delivery (anemia, methemoglobinemia, cyanide ingestion, carbon monoxide), pulmonary embolism, metabolic acidosis due to a variety of conditions, and panic attacks.
B. Physical Examination
A focused physical examination should include evaluation of the head and neck, chest, heart, and lower extremities. Visual inspection of the patient's respiratory pattern can suggest obstructive airway disease (pursed-lip breathing, use of extrarespiratory muscles, barrel-shaped chest), pneumothorax (asymmetric excursion), or metabolic acidosis (Kussmaul respirations). Patients with impending upper airway obstruction (eg, epiglottitis, foreign body), or severe asthma exacerbation, sometimes assume a tripod position. Focal wheezing raises the suspicion for a foreign body or other bronchial obstruction. Maximum laryngeal height (the distance between the top of the thyroid cartilage and the suprasternal notch at end expiration) is a measure of hyperinflation. Obstructive airway disease is virtually nonexistent when a nonsmoking patient younger than 45 years has a maximum laryngeal height < 4 cm (Table 2-2).
Because arterial blood gas testing is impractical in most outpatient settings, pulse oximetry has assumed a central role in the office evaluation of dyspnea. Oxygen saturation values above 96% almost always correspond with a PO2 > 70 mm Hg, and values less than 94% almost always represent clinically significant hypoxemia. Important exceptions to this rule include carbon monoxide toxicity, which leads to a normal oxygen saturation (due to the similar wavelengths of oxyhemoglobin and carboxyhemoglobin), and methemoglobinemia, which results in an oxygen saturation of about 85%. Supplemental oxygen fails to improve desaturation due to methemoglobinemia. A normal or mildly abnormal oxygen saturation (< 90%) in a delirious or obtunded patient with obstructive lung disease warrants immediate measurement of arterial blood gases to exclude hypercapnia and the need for intubation. When pulse oximetry yields equivocal results, assessment of desaturation with ambulation (eg, a brisk walk around the clinic) can be a useful finding (eg, when Pneumocystis jiroveci [formerly P carinii] pneumonia is suspected).
Table 2-2. Clinical findings suggesting obstructive airway disease. | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
A systematic review has identified several clinical predictors of increased LVEDP useful in the evaluation of dyspneic patients with no prior history of CHF (Table 2-3). When none is present, there is a very low probability (< 10%) of increased LVEDP, and when two or more are present, there is a very high probability (> 90%) of increased LVEDP.
Table 2-3. Clinical findings suggesting increased left ventricular end-diastolic pressure. | ||
|---|---|---|
|
P.25
Diagnostic Studies
Causes of dyspnea that can be managed without chest radiography are few: ingestions causing lactic acidosis, methemoglobinemia, and carbon monoxide poisoning. The diagnosis of pneumonia should be confirmed by chest radiography in most patients. When COPD exacerbation is severe enough to require hospitalization, results of chest radiography influence management decisions in up to 20% of patients. Chest radiography (detection of redistribution of pulmonary venous circulation) is fairly sensitive and specific for new-onset CHF and can help guide treatment decisions in patients with dyspnea secondary to cardiac disease. End-expiratory chest radiography enhances detection of a small pneumothorax.
A normal chest radiograph has substantial diagnostic value. In the absence of physical examination evidence of COPD or CHF, the major remaining causes of dyspnea include pulmonary embolism, upper airway obstruction, foreign body, and metabolic acidosis. If a patient has tachycardia and hypoxemia but a normal chest radiograph and ECG, then further tests to exclude pulmonary emboli are warranted (see Chapter 9), provided blood tests exclude significant anemia or metabolic acidosis. High-resolution chest CT is particularly useful in the evaluation of pulmonary embolism and interstitial lung disease. Suspected carbon monoxide poisoning or methemoglobinemia can be confirmed with either arterial or venous carboxyhemoglobin or methemoglobin levels.
Serum or whole blood brain natriuretic peptide (BNP) testing can be useful in the evaluation of dyspnea in the emergency department, since elevated BNP levels are both sensitive and specific for increased LVEDP in symptomatic persons.
Clinical examination and routine diagnostic testing will identify the cause of dyspnea in most cases. Persistent uncertainty warrants arterial blood gas measurement. Spirometry is very helpful in further classifying patients with obstructive airway disease, but is rarely needed in the initial or emergent evaluation of patients with acute dyspnea.
Episodic dyspnea can be challenging if an evaluation cannot be performed during symptoms. Life-threatening causes include recurrent pulmonary embolism, myocardial ischemia, and reactive airway disease. When associated with audible wheezing, vocal cord dysfunction should be considered, particularly in a young woman who does not respond to asthma therapy.
Treatment
The treatment of urgent or emergent causes of dyspnea should aim to relieve the underlying cause. Pending diagnosis, patients with hypoxemia should be immediately provided supplemental oxygen unless significant hypercapnia is present. Dyspnea frequently occurs in patients nearing the end of life, and opioid and oxygen therapy can be very effective in providing relief (see Chapter 5).
Collins SP et al: Diagnostic and prognostic usefulness of natriuretic peptides in emergency department patients with dyspnea. Ann Emerg Med 2003;41:532.
Jennings AL et al: A systematic review of the use of opioids in the management of dyspnea. Thorax 2002;57:929.
Karnani NG et al: Evaluation of chronic dyspnea. Am Fam Physician 2005;71:1529.
Luce JM et al: Management of dyspnea in patients with far-advanced lung disease: once I lose it, it's kind of hard to catch it. JAMA 2001;285:1331.
Mahler DA et al: Evaluation of dyspnea in the elderly. Clin Geriatr Med 2003;19:19.
Straus SE et al: The accuracy of patient history, wheezing, and laryngeal measurements in diagnosing obstructive airway disease. JAMA 2000;283:1853.
Lower Extremity Edema
![]() Essential Inquiries
Essential Inquiries
History of venous thromboembolism.
Symmetry.
Pain.
Dependence.
General Considerations
Acute and chronic lower extremity edema present important diagnostic and treatment challenges. Lower extremities can swell in response to increased venous or lymphatic pressures, decreased intravascular oncotic pressure, increased capillary leak, and local injury or infection. Chronic venous insufficiency is by far the most common cause, affecting up to 2% of the population, and the incidence of venous insufficiency has not changed during the past 25 years. Venous insufficiency is a common complication of DVT; however, only a small number of patients with chronic venous insufficiency report a history of this disorder. Venous ulcer formation commonly affects patients with chronic venous insufficiency, and management of venous ulceration is labor intensive and expensive.
Clinical Findings
A. Symptoms and Signs
Normal lower extremity venous pressure (in the erect position: 80 mm Hg in deep veins, 20 30 mm Hg in superficial veins) and cephalad venous blood flow require competent bicuspid venous valves, effective muscle contractions, and normal respirations. When one or more of these components fail, venous hypertension may result. Chronic exposure to elevated venous pressure by the postcapillary venules in the legs leads to leakage of fibrinogen and growth factors into the interstitial space, leukocyte aggregation and activation,
P.26
and obliteration of the cutaneous lymphatic network. These changes account for the brawny, fibrotic skin changes observed in patients with chronic venous insufficiency, and the predisposition toward skin ulceration, particularly in the medial malleolar area.
Among common causes of lower extremity swelling, DVT is the most life-threatening. Clues suggesting DVT include a history of cancer, recent limb immobilization, or confinement to bed for at least 3 days following major surgery within the past month (Table 2-4). A search for alternative explanations is equally important in excluding DVT. Bilateral involvement and significant improvement upon awakening favor systemic causes (eg, venous insufficiency, CHF, and cirrhosis). Heavy legs are the most frequent symptom among patients with chronic venous insufficiency, followed by itching. Pain, particularly if severe, is uncommon in uncomplicated venous insufficiency. Lower extremity swelling and inflammation in a limb recently affected by DVT could represent anticoagulation failure and thrombus recurrence but more often are caused by postphlebitic syndrome with valvular incompetence. Other causes of a painful, swollen calf include ruptured popliteal cyst, calf strain or trauma, and cellulitis. Lower extremity swelling is a familiar complication of therapy with calcium channel blockers (particularly felodipine and amlodipine), thioglitazones, and minoxidil. Prolonged airline flights (>10 hours) are associated with increased risk of edema. In those with low to medium risk of thromboembolism (eg, women taking oral contraceptives), long flights are associated with a 2% incidence of asymptomatic popliteal DVT.
Table 2-4. Risk stratification of adults referred for ultrasound to rule out DVT. | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
B. Physical Examination
Physical examination should include assessment of the heart, lungs, and abdomen for evidence of pulmonary hypertension (primary, or secondary to chronic lung disease), CHF, or cirrhosis. Some patients with the latter have pulmonary hypertension without lung disease. There is a spectrum of skin findings related to chronic venous insufficiency that depends on the severity and chronicity of the disease, ranging from hyperpigmentation and stasis dermatitis to abnormalities highly specific for chronic venous insufficiency: lipodermatosclerosis (thick brawny skin; in advanced cases, the lower leg resembles an inverted champagne bottle) and atrophie blanche (small depigmented macules within areas of heavy pigmentation). The size of both calves should be measured 10 cm below the tibial tuberosity and elicitation of pitting and tenderness performed. Swelling of the entire leg or swelling of one leg 3 cm more than the other suggests deep venous obstruction. In normal persons, the left calf is slightly larger than the right as a result of the left common iliac vein coursing under the aorta.
An ulcer located over the medial malleolus is a hallmark of chronic venous insufficiency but can be due to other causes. Shallow, large, modestly painful ulcers are characteristic of venous insufficiency, whereas small, deep, and more painful ulcers are more apt to be due to arterial insufficiency, vasculitis, or infection (including cutaneous diphtheria). Diabetic vascular ulcers, however, may be painless. When an ulcer is on the foot or above the mid calf, causes other than venous insufficiency should be considered.
C. Diagnostic Studies
Most causes of lower extremity swelling can be demonstrated with color duplex ultrasonography. Patients without an obvious cause of acute lower extremity swelling (eg, calf strain) should have an ultrasound performed, since DVT is difficult to exclude on clinical grounds. Assessment of the ankle-brachial pressure index (ABPI) is important in the management of chronic venous insufficiency, since peripheral arterial disease may be exacerbated by compression therapy. This can be performed at the same time as ultrasound. Caution is required in interpreting the results of ABPI in older patients and diabetics due to decreased compressibility of their arteries.
Differential Diagnosis
Possible causes include chronic venous insufficiency, DVT, cellulitis, musculoskeletal disorders (Baker's
P.27
cyst rupture, gastrocnemius tear or rupture), lymphedema, CHF, cirrhosis, and nephrotic syndrome, as well as side effects from calcium channel blockers, minoxidil, or thioglitazones.
Treatment
In patients with chronic venous insufficiency without a comorbid volume overload state (eg, CHF), it is best to avoid diuretic therapy. These patients have relatively decreased intravascular volume, and administration of diuretics may result in acute renal insufficiency and oliguria. The most effective treatment involves (1) leg elevation, above the level of the heart, for 30 minutes three to four times daily, and during sleep; and (2) compression therapy. A wide variety of stockings and devices are effective in decreasing swelling and preventing ulcer formation. They should be put on with awakening, before hydration forces result in edema. Horse chestnut seed extract has been shown in several randomized trials to be equivalent to compression stockings, and can be quite useful in nonambulatory patients. Patients with decreased ABPI should be managed in concert with a vascular surgeon. Compression stockings (12 18 mm Hg at the ankle) are effective in preventing edema and asymptomatic thrombosis associated with long airline flights in low- to medium-risk persons.
Barwell JR et al: Comparison of surgery and compression with compression alone in chronic venous ulceration (ESCHAR study): randomised controlled trial. Lancet 2004;363:1854.
Belcaro G et al: Prevention of edema, flight microangiopathy and venous thrombosis in long flights with elastic stockings. A randomized trial: the LONFLIT 4 Concorde Edema-SSL Study. Angiology 2002;53:635.
Criqui MH et al: Chronic venous disease in an ethnically diverse population: the San Diego Population Study. Am J Epidemiol 2003;158:448.
Eberhardt RT et al: Chronic venous insufficiency. Circulation 2005;111:2398.
Felty CL et al: Compression therapy for chronic venous insufficiency. Semin Vasc Surg 2005;18:36.
Kahn SR et al: Relationship between deep venous thrombosis and the postthrombotic syndrome. Arch Intern Med 2004; 164:17.
Fever & Hyperthermia
![]() Essential Inquiries
Essential Inquiries
Localizing symptoms.
Weight loss.
Joint pain.
Injection substance use.
Immunosuppression or neutropenia.
History of cancer.
Medications.
Travel.
General Considerations
The average normal oral body temperature taken in mid-morning is 36.7 C (range 36 37.4 C). This spectrum includes a mean and 2 standard deviations, thus encompassing 95% of a normal population, measured in mid-morning (normal diurnal temperature variation is 0.5 1 C). The normal rectal or vaginal temperature is 0.5 C higher than the oral temperature, and the axillary temperature is correspondingly lower. Rectal temperature is more reliable than oral temperature, particularly in mouth breathers or in tachypneic states.
Fever is a regulated rise to a new set point of body temperature. When proper stimuli act on appropriate monocyte-macrophages, these cells elaborate pyrogenic cytokines, causing elevation of the set point through effects in the hypothalamus. These cytokines include interleukin-1 (IL-1), tumor necrosis factor (TNF), interferon- , and interleukin-6 (IL-6). The elevation in temperature results from either increased heat production (eg, shivering) or decreased loss (eg, peripheral vasoconstriction). Body temperature in cytokine-induced fever seldom exceeds 41.1 C unless there is structural damage to hypothalamic regulatory centers.
Hyperthermia
Hyperthermia not mediated by cytokines occurs when body metabolic heat production or environmental heat load exceeds normal heat loss capacity or when there is impaired heat loss; heat stroke is an example. Body temperature may rise to levels (> 41.1 C) capable of producing irreversible protein denaturation and resultant brain damage; no diurnal variation is observed.
Neuroleptic malignant syndrome is a rare and potentially lethal idiosyncratic reaction to major tranquilizers, particularly haloperidol and fluphenazine. It has clinical and pathophysiologic similarities to malignant hyperthermia of anesthesia (see Chapters 25 and 39).
Fever as a symptom provides important information about the presence of illness particularly infections and about changes in the clinical status of the patient. The fever pattern, however, is of marginal value for most specific diagnoses except for the relapsing fever of malaria, borreliosis, and occasional cases of lymphoma, especially Hodgkin's disease. Furthermore, the degree of temperature elevation does not necessarily correspond to the severity of the illness. In general, the febrile response tends to be greater in children than in adults. In older persons, neonates, and in persons receiving certain medications (eg, nonsteroidal anti-inflammatory drugs [NSAIDs] or corticosteroids), a normal temperature or even hypothermia may be observed.
P.28
Markedly elevated body temperature may result in profound metabolic disturbances. High temperature during the first trimester of pregnancy may cause birth defects, such as anencephaly. Fever increases insulin requirements and alters the metabolism and disposition of drugs used for the treatment of the diverse diseases associated with fever.
Prolonged Fever
Most febrile illnesses are due to common infections, are short-lived, and are relatively easy to diagnose. In certain instances, however, the origin of the fever may remain obscure ( fever of undetermined origin, FUO) even after protracted diagnostic examination. In upper respiratory tract infections, fever typically lasts no more than 3 5 days, beyond which additional evaluation is warranted. The term FUO has traditionally been reserved for unexplained cases of fever exceeding 38.3 C on several occasions for at least 3 weeks in patients without neutropenia or immunosuppression (see Chapter 30).
After extensive evaluation, 25% of these patients are judged to have chronic or indolent infection, about 25% autoimmune diseases, and about 10% a malignancy; the remainder have miscellaneous other disorders or no diagnosis is reached. With improved imaging and microbiology testing, fewer cases are being attributed to infectious disease and more are being attributed to cancer and autoimmune disease (particularly among the elderly). Long-term follow-up of patients with initially undiagnosed FUO demonstrates that 50% become symptom free during evaluation. In the remainder, a definitive diagnosis is established in 20%, usually within 2 months after investigation, and 30% have persistent or recurring fever for months or even years.
Approach to the Patient with Fever of Undetermined Origin
Standardized algorithms for FUO are difficult to extrapolate to the individual patient. Nevertheless, the results of a history, physical examination, routine laboratory tests, and blood cultures provide important diagnostic clues that lead to a definitive diagnosis in most cases. Chest radiography, abdominal ultrasound, and CT scans, often repeated after previous nondiagnostic studies, are most helpful. Radionuclide agents include labeled leukocytes, gallium-67, and radiolabeled human immunoglobulin; however, these tests appear to be most useful in patients with localizing signs of inflammation. There is little or no value to be derived from undirected immunologic, microbiologic, serologic, or endocrinologic studies. In older patients, a temporal artery biopsy is occasionally of use. Newer imaging modalities that may be useful in challenging cases include fluorodeoxyglucose-positron emission tomography imaging.
FUO is commonly associated with AIDS and HIV-related infections, though uncomplicated HIV infection is not a cause of prolonged fever. When FUO is observed in HIV-infected individuals, it usually occurs in the late stages. The most common causes are disseminated Mycobacterium avium infection, P jiroveci pneumonia, cytomegalovirus infection, disseminated histoplasmosis, and lymphoma.
The differential diagnosis of a febrile illness in the returned traveler is extensive but most commonly includes tropical infections such as malaria, dysentery, hepatitis, and dengue fever. A substantial number of febrile illnesses in travelers are never diagnosed.
Differential Diagnosis
See Table 2-5.
Treatment
Most fever is well tolerated. When the temperature is greater than 40 C, symptomatic treatment may be required. A reading over 41 C is likely to be hyperthermia and thus not cytokine mediated, and emergent management is indicated. (See Heat Stroke, Chapter 38.)
A. Measures for Removal of Heat
Alcohol sponges, cold sponges, ice bags, ice-water enemas, and ice baths will lower body temperature. They are more useful in hyperthermia, since patients with cytokine-related fever will attempt to override these therapies.
B. Antipyretic Drugs
Antipyretic therapy is not needed except for patients with marginal hemodynamic status. Aspirin or acetaminophen,
P.29
325 650 mg every 4 hours, is effective in reducing fever. These drugs are best administered continuously rather than as needed, since prn dosing results in periodic chills and sweats due to fluctuations in temperature caused by varying levels of drug.
Table 2-5. Differential diagnosis of fever and hyperthermia. | |
|---|---|
|
C. Antimicrobial Therapy
In most febrile patients, empiric antibiotic therapy should be deferred pending further evaluation. However, empiric antibiotic therapy is sometimes warranted. Prompt broad-spectrum antimicrobials are indicated for febrile patients who are clinically unstable, even before infection can be documented. These include patients with hemodynamic instability, those with neutropenia (neutrophils < 500/mcL), others who are asplenic (surgically or secondary to sickle cell disease) or immunosuppressed (including individuals taking systemic corticosteroids, azathioprine, cyclosporine, or other immunosuppressive medications), and those who are HIV infected (see Chapter 31). For treatment of fever during neutropenia following chemotherapy, outpatient parenteral antimicrobial therapy with an agent such as ceftriaxone can be provided effectively and safely. If a fungal infection is suspected in patients with prolonged fever and neutropenia, fluconazole is an equally effective but less toxic alternative to amphotericin B.
Carapetis JR et al: Acute rheumatic fever. Lancet 2005;366:155.
Marik PE: Fever in the ICU. Chest 2000;117:855.
Roth AR et al: Approach to the adult patient with fever of unknown origin. Am Fam Physician 2003;68:2223.
Rusyniak DE et al: Toxin-induced hyperthermic syndromes. Med Clin North Am 2005;89:1277.
Sipsas NV et al: Perspectives for the management of febrile neutropenic patients with cancer in the 21st century. Cancer 2005;103:1103.
Vanderschueren S et al: From prolonged febrile illness to fever of unknown origin: the challenge continues. Arch Intern Med 2003;163:1033.
Watson JT et al: Clinical characteristics and functional outcomes of West Nile Fever. Ann Intern Med 2004;141:360.
Woolery WA et al: Fever of unknown origin: keys to determining the etiology in older patients. Geriatrics 2004;59:41.
Involuntary Weight Loss
![]() Essential Inquiries
Essential Inquiries
Age.
Caloric intake.
Fever.
Change in bowel habits.
Secondary confirmation (eg, changes in clothing size).
Substance use.
Age-appropriate cancer screening history.
General Considerations
Body weight is determined by a person's caloric intake, absorptive capacity, metabolic rate, and energy losses. The metabolic rate can be affected by a multitude of medical conditions through the release of various cytokines such as cachectin and interleukins. Body weight normally peaks by the fifth or sixth decade and then gradually declines at a rate of 1-2 kg per decade. In NHANES II, a national survey of community-dwelling elders (age 50 80 years), recent involuntary weight loss (> 5% usual body weight) was reported by 7% of respondents, and this was associated with a 24% higher mortality.
Clinical Findings
Involuntary weight loss is regarded as clinically significant when it exceeds 5% or more of usual body weight over a 6- to 12-month period and often indicates serious physical or psychological illness. Physical causes are usually evident during the initial evaluation. Cancer (about 30%), gastrointestinal disorders (about 15%), and dementia or depression (about 15%) are the most common causes. When an adequately nourished-appearing patient complains of weight loss, inquiry should be made about exact weight changes (with approximate dates) and about changes in clothing size. Family members can provide confirmation of weight loss, as can old documents such as driver's licenses.
Once the weight loss is established, the history, medication profile, physical examination, and conventional laboratory and radiologic investigations such as complete blood count, serologic tests, thyroid-stimulating hormone (TSH) level, urinalysis, fecal occult blood test, chest radiography, and upper gastrointestinal series usually reveal the cause. When these tests are normal, the second phase of evaluation should focus on more definitive gastrointestinal investigation (eg, tests for malabsorption; endoscopy) and cancer screening (eg, Papanicolaou smear, mammography, prostate specific antigen [PSA]).
If the initial evaluation is unrevealing, follow-up is preferable to further diagnostic testing. Death at 2-year follow-up was not nearly as high in patients with unexplained involuntary weight loss (8%) as in those with weight loss due to malignant (79%) and established nonmalignant diseases (19%). Psychiatric consultation should be considered when there is evidence of depression, dementia, anorexia nervosa, or other emotional problems. Ultimately, in approximately 15 25% of cases, no cause for the weight loss can be found.
A mild, gradual weight loss occurs in some older individuals. It is due to changes in body composition, including loss of height and lean body mass and lower
P.30
basal metabolic rate, leading to decreased energy requirements. However, rapid unintentional weight loss is predictive of morbidity and mortality in any population. In addition to various disease states, causes in older individuals include loss of teeth and consequent difficulty with chewing, alcoholism, and social isolation.
Differential Diagnosis
Malignancy, gastrointestinal disorders (eg, malabsorption, pancreatic insufficiency), dementia, depression, anorexia nervosa, hyperthyroidism, alcoholism, and social isolation are all established causes.
Treatment
Weight stabilization occurs in most surviving patients with both established and unknown causes of weight loss through treatment of the underlying disorder and caloric supplementation. Nutrient intake goals are established in relation to the severity of weight loss, in general ranging from 30 to 40 kcal/kg/d. In order of preference, route of administration options include oral, temporary nasojejunal tube, or percutaneous gastric or jejunal tube. Parenteral nutrition is reserved for patients with serious associated problems. A variety of pharmacologic agents have been proposed for the treatment of weight loss. These can be categorized into appetite stimulants (corticosteroids, progestational agents, dronabinol, and serotonin antagonists); anabolic agents (growth hormone and testosterone derivatives); and anticatabolic agents (omega-3 fatty acids, pentoxifylline, hydrazine sulfate, and thalidomide).
Alibhai SM et al: An approach to the management of unintentional weight loss in elderly people. CMAJ 2005;172:773.
Collins N: Protein-energy malnutrition and involuntary weight loss: nutritional and pharmacological strategies to enhance wound healing. Expert Opin Pharmacother 2003;4:1121.
Hernandez JL et al: Clinical evaluation for cancer in patients with involuntary weight loss without specific symptoms. Am J Med 2003;114:631.
Lankisch P et al: Unintentional weight loss: diagnosis and prognosis. The first prospective follow-up study from a secondary referral centre. J Intern Med 2001;249:41.
Sahyoun NR et al: The epidemiology of recent involuntary weight loss in the United States population. J Nutr Health Aging 2004;8:510.
Fatigue & Chronic Fatigue Syndrome
![]() Essential Inquiries
Essential Inquiries
Weight loss.
Fever.
Sleep-disordered breathing.
Medications.
Substance use.
General Considerations
As an isolated symptom, fatigue accounts for 1 3% of visits to generalists. The symptom of fatigue may be less well defined and explained by patients than symptoms associated with specific functions. Fatigue or lassitude and the closely related complaints of weakness, tiredness, and lethargy are often attributed to overexertion, poor physical conditioning, sleep disturbance, obesity, undernutrition, and emotional problems. A history of the patient's daily living and working habits may obviate the need for extensive and unproductive diagnostic studies.
Clinical Findings
Important diseases that can cause fatigue include hyperthyroidism and hypothyroidism, CHF, infections (endocarditis, hepatitis), COPD, sleep apnea, anemia, autoimmune disorders, and cancer. Alcoholism, drug side effects such as from sedatives and -blockers, and psychological conditions (such as insomnia, depression, and somatization disorder) are other causes. The lifetime prevalence of significant fatigue (present for at least 2 weeks) is about 25%. Fatigue of unknown cause or related to psychiatric illness exceeds that due to physical illness, injury, medications, drugs, or alcohol. Psychiatric disorders associated with fatigue include depression, dysthymia, somatoform disorders, panic attack, and alcohol abuse. Prolonged fatigue is a central feature of several syndromes, such as irritable bowel syndrome and anxiety (Figure 2-2). Exercise and treatment of anemia are the two most established interventions for cancer-related fatigue. Psychostimulants appear promising based on early studies.
Chronic Fatigue Syndrome
A working case definition of chronic fatigue syndrome indicates that it is not a homogeneous abnormality, and there is no single pathogenic mechanism (Figure 2-3). No physical finding or laboratory test can be used to confirm the diagnosis of this disorder.
With regard to its pathophysiology, early theories postulated an infectious or immune dysregulation mechanism, and it appears that neurologic, affective, and cognitive symptoms also occur frequently. Neuropsychological, neuroendocrine, and brain imaging studies have confirmed the occurrence of neurobiologic abnormalities in most patients. Sleep disorders have been reported in 40 80% of patients with chronic fatigue syndrome, but their treatment has provided only modest benefit, suggesting that it is an effect rather than a cause of the fatigue. MRI scans may show brain abnormalities on T2-weighted images chiefly small, punctate, subcortical white matter hyperintensities, predominantly in the frontal lobes. Veterans of the Gulf War
P.31
show a tenfold greater incidence of chronic fatigue syndrome compared with nondeployed military personnel.
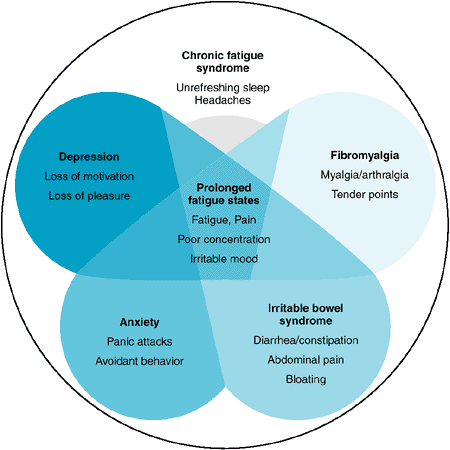 |
Figure 2-2. Overlapping diagnoses. Prolonged fatigue states are found in fibromyalgia, irritable bowel syndrome, anxiety, and depression as well as chronic fatigue syndrome. (Reproduced, with permission, from Chronic fatigue syndrome. Clinical practice guidelines-2002. Med J Aust 2002;176:S17. ) |
In evaluating chronic fatigue, after the history and physical examination process is completed, standard investigation includes complete blood count, erythrocyte sedimentation rate, serum chemistries blood urea nitrogen (BUN), electrolytes, glucose, creatinine, and calcium; liver and thyroid function tests antinuclear antibody, urinalysis, and tuberculin skin test; and screening questionnaires for psychiatric disorders. Other tests to be performed as clinically indicated are serum cortisol, rheumatoid factor, immunoglobulin levels, Lyme serology in endemic areas, and tests for HIV antibody. More extensive testing is usually unhelpful, including antibody to Epstein-Barr virus. There may be an abnormally high rate of postural hypotension; some of these patients report response to increases in dietary sodium as well as antihypotensive agents such as fludrocortisone, 0.1 mg/d.
In treatment, a variety of agents and modalities have been tried. Acyclovir, intravenous immunoglobulin, nystatin, and low-dose hydrocortisone/fludrocortisone do not improve symptoms. There is a greater prevalence of past and current psychiatric diagnoses in patients with this syndrome. Affective disorders are especially common, but fluoxetine alone, 20 mg daily, is not beneficial. Patients with chronic fatigue syndrome have benefited from a comprehensive multidisciplinary intervention, including optimal medical management, treating any ongoing affective or anxiety disorder pharmacologically, and implementing a comprehensive cognitive-behavioral treatment program. Cognitive-behavioral therapy, a form of nonpharmacologic treatment emphasizing self-help and aiming to change perceptions and behaviors that may perpetuate symptoms and disability, is helpful. Although few patients are cured, the treatment effect is substantial. Response to cognitive-behavioral therapy is not predictable on the basis of severity or duration of chronic fatigue syndrome, although patients with low interest in psychotherapy rarely benefit. Graded exercise has also been shown to improve functional work capacity and physical function. At present, intensive individual cognitive-behavioral therapy administered
P.32
by a skilled therapist and graded exercise are the treatments of choice for patients with chronic fatigue syndrome.
 |
Figure 2-3. Evaluation and classification of unexplained chronic fatigue. (CBC, complete blood count; ESR, erythrocyte sedimentation rate; ALT, alanine aminotransferase; Ca2+, calcium; PO43-, phosphate; BUN, blood urea nitrogen; TSH, thyroid-stimulating hormone; UA, urinalysis.) (Modified and reproduced, with permission, from Fukuda K et al: The chronic fatigue syndrome: a comprehensive approach to its definition and study. Ann Intern Med 1994;121:953. ) |
In addition, the clinician's sympathetic listening and explanatory responses can help overcome the patient's frustrations and debilitation by this still mysterious illness. All patients should be encouraged to engage in normal activities to the extent possible and should be reassured that full recovery is eventually possible in most cases.
Chalder T et al: Predictors of outcome in a fatigued population in primary care following a randomized controlled trial. Psychol Med 2003;33:283.
Chronic fatigue syndrome. Clinical practice guidelines 2002. Med J Aust 2002;176(Suppl):S23.
Reyes M et al: Prevalence and incidence of chronic fatigue syndrome in Wichita, Kansas. Arch Intern Med 2003;163: 1530.
Sood A et al: Cancer-related fatigue: an update. Curr Oncol Rep 2005;7:277.
Viner R et al: Fatigue and somatic symptoms. BMJ 2005;330: 1012.
Whiting P et al: Interventions for the treatment and management of chronic fatigue syndrome: a systematic review. JAMA 2001;286:1360.
Acute Headache
![]() Essential Inquiries
Essential Inquiries
Age > 50 years.
Rapid onset and severe intensity.
Fever.
Trauma.
Vision changes.
Past medical history of hypertension or HIV infection.
Hypertension.
Neurologic findings (mental status changes, motor or sensory deficits).
P.33
General Considerations
Headache is a common reason that adults seek medical care, accounting for approximately 13 million visits each year in the United States to physicians' offices, urgent care clinics, and emergency departments. A broad range of disorders can lead to headache. This chapter will deal only with the approach to a new acute headache not due to trauma in adolescents and adults. The challenge in the initial evaluation of acute headache is to identify those conditions that are life-threatening. In the emergency department setting, approximately 1% of patients seeking medical attention for acute headache will have a life-threatening condition, whereas the prevalence of life-threatening conditions in the office practice setting is considerably lower.
Regardless of the underlying cause, headache is currently believed to occur as a result of the release of neuropeptides from trigeminal nerve endings that encapsulate the blood vessels of the pia mater and dura mater, resulting in neurogenic inflammation. Because this represents a final common pathway, diminution of headache in response to typical migraine therapies (such as serotonin receptor antagonists or ketorolac tromethamine) does not rule out critical conditions such as subarachnoid hemorrhage or meningitis as the underlying cause.
Clinical Findings
A careful history and physical examination should be aimed at identifying causes of acute headache that require immediate treatment. These causes can be broadly classified as imminent or completed vascular events (intracranial hemorrhage, thrombosis, vasculitis, malignant hypertension, arterial dissection, or aneurysm), infections (abscess, encephalitis, meningitis), intracranial masses causing intracranial hypertension, preeclampsia, and carbon monoxide poisoning. The natural history of the onset of headache can be helpful. Report of a sudden-onset headache that reaches maximal and severe intensity within seconds or a few minutes is the classic description of a thunderclap headache and should precipitate workup for subarachnoid hemorrhage. A new headache in a patient of advanced age or with a history of HIV disease under most circumstances (including a normal neurologic examination) warrants neuroimaging immediately (Table 2-6). When the patient has a medical history of hypertension particularly uncontrolled hypertension a complete search for criteria satisfying a diagnosis of malignant hypertension is appropriate to determine the correct urgency level of hypertension management (see Chapter 11). Headache and hypertension associated with pregnancy may be due to preeclampsia. Episodic headache associated with the triad of hypertension, heart palpitations, and sweats should suggest the possibility of pheochromocytoma. In the absence of thunderclap headache, advanced age, and HIV disease, findings on physical examination will usually determine the time course and need for further diagnostic testing.
Table 2-6. Clinical features associated with acute headache that warrant urgent or emergent neuroimaging. | ||
|---|---|---|
|
Critical components of the physical examination of the patient with acute headache include vital sign measurements, neurologic examination, and vision testing with funduscopic examination. The finding of fever with acute headache should suggest additional maneuvers to elicit evidence of meningeal inflammation, such as Kernig and Brudzinski signs. Besides malignant hypertension, significant hypertension can also be a sign of intracranial hemorrhage, preeclampsia, and pheochromocytoma. Patients over 60 years of age should be examined for scalp or temporal artery tenderness.
Careful assessment of visual acuity, ocular gaze, visual fields, pupillary defects, the optic disk, and retinal vein pulsations is crucial. Diminished visual acuity is suggestive of glaucoma, temporal arteritis, or optic neuritis. Ophthalmoplegia or visual field defects may be signs of venous sinus thrombosis, tumor, or aneurysm. Afferent pupillary defects can be due to intracranial masses or optic neuritis. Ipsilateral ptosis and miosis suggest Horner's syndrome and in conjunction
P.34
with acute headache may signify carotid artery dissection. Finally, papilledema or absent retinal venous pulsations are signs of elevated intracranial pressure findings that should be followed by neuroimaging prior to performing lumbar puncture (Table 2-6).
Mental status and complete neurologic evaluations are also critical and should include assessment of motor and sensory systems, reflexes, gait, cerebellar function, and pronator drift. Any abnormality on mental status or neurologic evaluation warrants emergent neuroimaging (Table 2-6).
Diagnostic Studies
Under most circumstances, a noncontrast head CT is sufficient to exclude intracranial hypertension with impending herniation, intracranial hemorrhage, and many types of intracranial masses (notable exceptions include lymphoma and toxoplasmosis in HIV-positive patients, herpes simplex encephalitis, and brain abscess). When appropriate, a contrast study can often be ordered to follow a normal noncontrast study. A normal neuroimaging study does not sufficiently exclude subarachnoid hemorrhage and should be followed by lumbar puncture. In patients for whom there is a high level of suspicion for subarachnoid hemorrhage or aneurysm, a normal CT and lumbar puncture should be followed by angiography within the next few days (provided the patient is medically stable). Lumbar puncture is also indicated to exclude infectious causes of acute headache, particularly in patients with fever or meningeal signs. Cerebrospinal fluid tests should routinely include Gram stain, white blood cell count with differential, red blood cell count, glucose, total protein, and bacterial culture. In appropriate patients, also consider testing cerebrospinal fluid for VDRL (syphilis), cryptococcal antigen (HIV-positive patients), acid-fast bacillus stain and culture, and complement fixation and culture for coccidioidomycosis. Storage of an extra tube with 5 mL of cerebrospinal fluid is also prudent for conducting unanticipated tests in the immediate future. Consultation with infectious disease experts regarding local availability of newer polymerase chain reaction tests for specific infectious pathogens (eg, herpes simplex 2) should also be considered in patients with evidence of central nervous system infection but no identifiable pathogen.
In addition to neuroimaging and lumbar puncture, additional diagnostic tests for exclusion of life-threatening causes of acute headache include erythrocyte sedimentation rate (temporal arteritis; endocarditis), urinalysis (malignant hypertension; preeclampsia), and sinus CT or x-ray (bacterial sinusitis, independently or as a cause of venous sinus thrombosis).
Treatment
Treatment should be based on determination of the cause of acute headache.
Beck E et al: Management of cluster headache. Am Fam Physician 2005;71:717.
Colman I et al: Parenteral dihydroergotamine for acute migraine headache: a systematic review of the literature. Ann Emerg Med 2005;45:393.
Evans RW: New daily persistent headache. Curr Pain Headache Rep 2003;7:303.
Ryan RE: Common headache misdiagnoses. Prim Care 2004;31: 395.
Silberstein SD: Migraine. Lancet 2004;363:381.
van de Beek D et al: Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med 2004;351:1849.
Dysuria
![]() Essential Inquiries
Essential Inquiries
Fever.
Nausea/Vomiting.
New back or flank pain.
Vaginal discharge.
Pregnancy risk.
Structural abnormalities.
Instrumentation of urethra or bladder.
General Considerations
Dysuria (painful urination) is a common reason for adolescents and adults to seek urgent medical attention. An inflammatory process (eg, infection; autoimmune disorder) underlies most causes of dysuria. In women, cystitis will be diagnosed in up to 50 60% of cases and has an incidence of 0.5 0.7% per year in sexually active young women. The key objective in evaluating women with dysuria is to exclude serious upper urinary tract disease, such as acute pyelonephritis, and sexually transmitted diseases. In contrast, in men, urethritis accounts for the vast majority of cases of dysuria.
Clinical Findings
A. Symptoms
Well-designed cohort studies have shown that some women can be reliably diagnosed with uncomplicated cystitis without a physical examination or urinalysis, and randomized controlled trials show that telephone management of uncomplicated cystitis is safe and effective. An increased likelihood of cystitis is present when women report multiple irritative voiding symptoms (dysuria, urgency, frequency), fever, or back pain (likelihood ratios = 1.6 2.0). Inquiring about symptoms of vulvovaginitis is important, since the presence of vaginal discharge or itching substantially decreases the likelihood of cystitis (likelihood ratios = 0.2 0.3). When women report dysuria and urinary frequency, and deny vaginal discharge and irritation, the likelihood
P.35
ratio for culture-confirmed cystitis is 24.5. In contrast, when vaginal discharge or irritation is present, as well as dysuria or urinary frequency, the likelihood ratio is 0.7. Gross hematuria in women with voiding symptoms usually represents hemorrhagic cystitis, but can also be a sign of bladder cancer (particularly in older patients) or upper tract disease. Failure of hematuria to resolve with antibiotic treatment should prompt further evaluation of the bladder and kidneys. Finally, chlamydial infection should be strongly considered among women age 25 years or younger who are sexually active and who are seeking medical attention for a suspected urinary tract infection for the first time.
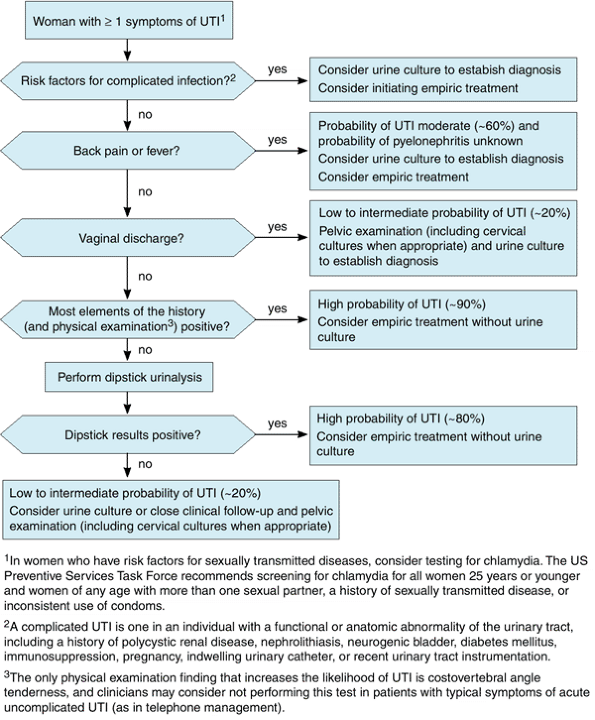 |
Figure 2-4. Proposed algorithm for evaluating women with symptoms of acute urinary tract infection (UTI). (Modified and reproduced, with permission, from Bent S et al: Does this woman have an acute uncomplicated urinary tract infection? JAMA 2002;297:2701. ) |
Because fever and back pain, as well as nausea and vomiting, are considered harbingers of (or clinical criteria for) acute pyelonephritis, women with these symptoms should usually be examined by a clinician prior to treatment in order to exclude coexistent urosepsis, hydronephrosis, or nephrolithiasis. Other major risk factors for
P.36
acute pyelonephritis (among women 18 49 years of age) relate to sexual behaviors (frequency of sexual intercourse three or more times per week, new sexual partner in previous year, recent spermicide use), as well as diabetes mellitus and recent urinary tract infection or incontinence. Finally, pregnancy risk, underlying structural factors (polycystic kidney disease, nephrolithiasis, neurogenic bladder), immunosuppression, diabetes, and a history of recent bladder or urethral instrumentation usually alter the treatment regimen (antibiotic choice or duration of treatment, or both) of uncomplicated cystitis.
B. Physical Examination
The presence of fever, tachycardia, or hypotension should alert the clinician to the possibility of urosepsis and the potential need for hospitalization. A focused examination in women, in uncomplicated circumstances, could be limited to ascertainment of costovertebral angle tenderness and to a pelvic examination, if the history suggests vulvovaginitis or cervicitis.
C. Diagnostic Studies
1. Urinalysis
Urinalysis is probably overutilized in the evaluation of dysuria. The probability of culture-confirmed urinary tract infection among women with a history and physical examination compatible with uncomplicated cystitis is about 90%. Urinalysis is most helpful when the woman with dysuria does not have other typical features of cystitis. Dipstick detection (> trace) of leukocytes, nitrites, or blood supports a diagnosis of cystitis. When both leukocyte and nitrite tests are positive, the likelihood ratio is 4.2, and when both are negative, the likelihood ratio is 0.3.
2. Urine culture
Urine culture should be considered for all women with upper tract symptoms (prior to initiating antibiotic therapy), as well as those with dysuria and a negative urine dipstick test. In symptomatic women, a clean-catch urine culture is considered positive when 102-103 colony-forming units/mL of a uropathogenic organism is detected.
3. Renal imaging
When severe flank or back pain is present, the possibility of complicated kidney infection (perinephric abscess, nephrolithiasis) or of hydronephrosis should be considered. Depending on local availability, acceptable imaging options to assess for hydronephrosis include abdominal radiographs, renal ultrasound, or CT scanning. To exclude nephrolithiasis, noncontrast helical CT scanning is more accurate than intravenous urography and is rapidly becoming the diagnostic test of choice for this purpose. In a meta-analysis, the positive and negative likelihood ratios of helical CT scanning for diagnosis of nephrolithiasis were 23.2 and 0.05, respectively.
D. Differential Diagnosis
The differential diagnosis of dysuria in women includes acute cystitis, acute pyelonephritis, vaginitis (Candida, bacterial vaginosis, Trichomonas, herpes simplex), urethritis/cervicitis (Chlamydia, gonorrhea), and interstitial cystitis. Nucleic acid amplification tests from first-void urine or vaginal swab specimens are highly sensitive for detecting chlamydial infection.
E. Treatment
Definitive treatment is directed to the underlying cause of the dysuria. An evidence-informed algorithm for managing suspected urinary tract infection in women is shown in Figure 2-4. Symptomatic relief can be provided with phenazopyridine, a urinary analgesic that is available over-the-counter; it is used in combination with antibiotic therapy (when a urinary tract infection has been confirmed) but for no more than 2 days. Patients should be informed that phenazopyridine will cause orange/red discoloration of their urine and other bodily fluids (eg, some contact lens wearers have reported discoloration of their lenses). Rare cases of methemoglobinemia and hemolytic anemia have been reported, usually with overdoses or underlying renal dysfunction. Although current convention is to consider noninfectious causes of dysuria in women with negative urine dipstick tests, a recent randomized trial showed more rapid symptom resolution associated with antibiotic therapy.
Bent S et al: Does this woman have an acute uncomplicated urinary tract infection? JAMA 2002;287:2701.
Fihn S: Acute uncomplicated urinary tract infection in women. N Engl J Med 2003;349:259.
Richards D et al: Response to antibiotics of women with symptoms of urinary tract infection but negative dipstick urine test results: double blind randomised controlled trial. BMJ 2005;331:143.
Sholes D et al: Risk factors associated with acute pyelonephritis in healthy women. Ann Intern Med 2005;142:20.
EAN: 2147483647
Pages: 49