| Note: Large images and tables on this page may necessitate printing in landscape mode.
Copyright 2007 The McGraw-Hill Companies. All rights reserved.
Current Otolaryngology > V. Salivary Glands > Chapter 17. Benign Diseases of the Salivary Glands >
| Benign Diseases of the Salivary Glands: Introduction General Considerations The salivary glands consist of two parotid glands, two submandibular glands, two principal sublingual glands, and a large number of minor salivary glands. Combined, the salivary glands produce serous secretions, mucous secretions, or both. The serous saliva of the parotid gland and the predominantly mucous secretions of the submandibular, sublingual, and minor salivary glands provide digestive enzymes, bacteriostatic functions, lubrication, and hygienic activities. The secretions of the parotid and submandibular glands are primarily stimulated by the autonomic nervous system. Classification Benign diseases of the major and minor salivary glands can often be classified as nonneoplastic and neoplastic. Most clinically significant benign diseases involve primarily the parotid and submandibular glands and less frequently the paired principal sublingual and widely distributed minor salivary glands. Parotid Gland The parotid gland is the largest of the paired major salivary glands, with an average weight of 25 grams. Each gland is located lateral to the masseter muscle anteriorly and extends posteriorly over the sternocleidomastoid muscle behind the angle of the mandible. The dermis lies laterally to the gland, and the lateral parapharyngeal space lies medially. Each encapsulated gland is artificially divided into a superficial lobe and a deep lobe by the branches of the seventh cranial nerve . The parotid duct, or Stensen duct, courses anteriorly from the parotid gland over the masseter muscle and pierces the buccinator muscle to enter through the buccal mucosa, usually opposite the second maxillary molar. The Stensen duct can be found approximately 1.5 cm below the zygoma. The parotid gland has two layers of draining lymph nodes. The superficial layer lies beneath the capsule , and the deeper layer lies within the parotid parenchyma. Submandibular Gland The paired submandibular glands are the second largest salivary glands in the body, each weighing approximately 1015 grams. Each submandibular gland is divided into superficial and deep lobes by the posterior edge of the mylohyoid muscle and occupies the submandibular triangle. The submandibular duct, also known as the Wharton duct, courses anteriorly above the mylohyoid muscle and ends in the anterior floor of the mouth. The submandibular duct is inelastic and therefore, when obstructed, causes pain. Sublingual Glands The principal sublingual glands are paired and located in the submucosa, superficial to the mylohyoid muscle. Each gland is bounded laterally by the inner cortex of the mandible and medially by the styloglossus muscle; the paired glands meet in the midline. The sublingual glands have multiple small or "minor" sublingual ducts, referred to as the ducts of Rivinus, which open directly into the oral cavity . Some of these ducts unite to form the major ducts of Bartholin. These major ducts can also join the submandibular ducts. The lingual nerve descends laterally to the anterior end of the sublingual gland and runs along its inferior border. Anteriorly, the lingual nerve and submandibular duct run parallel until the lingual nerve ascends into the tongue. Minor Salivary Glands The hard and soft palates contain the greatest concentration of minor salivary glands; however, these glands are also located in the oral cavity, lips, tongue, and oropharynx. Minor salivary glands may be identified in groups, such as the anterior lingual glands of Blandin-Nuhn. The salivary glands consist of multiple secretory units that include an acinus at the proximal end and a distal ductal unit. The ductal unit combines a sequential array of ductal elements extending away from the acinus: the intercalated duct, the striated duct, and the excretory duct. Myoepithelial cells surround the acinus and extend to the intercalated duct. These myoepithelial cells contract, enabling the glandular cells to expel their secretions. Benign disorders of the salivary glands involve abnormalities of saliva production and secretion. Saliva is produced by the clustered acinar cells and contains electrolytes, enzymes (eg, ptyalin and maltase), carbohydrates, proteins , inorganic salts , and even some antimicrobial factors. Approximately 5001500 mL of saliva is produced by the acinar cells daily and transported through the ductal elements at an average rate of 1 mL per minute. Human saliva is generally alkaline. | | Nonneoplastic Diseases: Introduction A list of nonneoplastic diseases can be found in Table 171. | Table 171. Nonneoplastic Benign Diseases of the Salivary Glands.
| | | Noninfectious, Inflammatory Disease | | Sialolithiasis | | Chronic sialadenitis | | Sjgren syndrome | | Benign lymphoepithelial lesion | | Kimura disease | | Necrotizing sialometaplasia | | Adenomatoid hyperplasia | | Sarcoidosis | | Infectious Disease | | Mumps virus | | Coxsackie virus | | Influenza virus | | Echovirus | | Human immunodeficiency virus | | Bacteria | | Granulomatous infections | | Noninflammatory Disease | | Sialadenosis | | Branchial cleft cysts | | Dermoid cysts | | Congenital cysts | | Mucoceles | |
| | | Infectious Inflammatory Diseases Infections can occur in an otherwise normal salivary gland or result from prolonged abnormalities of salivary function. Infections can be acute, subacute, or chronic. The primary etiologic agents include viruses and bacteria. However, infections may result secondarily from trauma, radiation, or duct obstruction, as is the case with acute sialadenitis. | | Acute Viral Inflammatory Disease Essentials of Diagnosis - Acute, bilateral swelling of the parotid glands accompanied by pain, erythema, tenderness, malaise, fever , and occasionally trismus.
- Peak incidence in young children aged 46 years .
- Incubation period is 1421 days.
- Disease is contagious.
- Diagnosis can be confirmed with serologic testing.
General Considerations Mumps (paramyxovirus) is the most common viral disorder causing parotitis (ie, inflammation of the parotid gland). The peak incidence occurs in children aged 46 years. The incubation period is 1421 days, and the disease is contagious during this time. Clinical Findings In an acute viral inflammation of the parotid gland, bilateral swelling may be accompanied by pain, erythema, tenderness, malaise, fever, and occasionally trismus if an extensive inflammation of the adjacent pterygoid musculature exists. After a thorough history and physical exam, checking the antibodies for the mumps S, mumps V, and hemagglutination antigens can confirm the diagnosis. Differential Diagnosis The differential diagnoses of viral parotitis include the coxsackie A virus, cytomegalovirus, influenza A virus, and echoviruses. A serologic screen to test for these viruses may verify the diagnosis. Complications Complications of acute viral parotitis may involve other organs. Rare sequelae include meningitis, encephalitis, hearing loss, orchitis, pancreatitis , and nephritis. Treatment & Prognosis The disease course of viral parotitis is self-limiting and treatment is primarily symptomatic. The administration of the mumps vaccine has likely decreased the incidence of mumps. Viral infections in immunocompetent individuals often resolve with excellent prognosis. | | Acute Suppurative Sialadenitis Essentials of Diagnosis - Acute painful swelling of the salivary glands with fever.
- Can occur in postoperative patients and in elderly patients with chronic medical conditions.
- Risk factors include dehydration, trauma, immunosuppression , and debilitation.
- Skin overlying the parotid may be warm, tender, and edematous.
- Untreated acute suppurative sialadenitis may lead to an abscess.
- Saliva from the affected gland should be cultured.
General Considerations In addition to viruses, bacteria can cause symptoms of acute painful swelling of the salivary glands, especially the parotid gland. Acute suppurative sialadenitis accounts for 0.03% of hospital admissions and can occur in up to 3040% of postoperative patients. Pathogenesis An underlying pathogenesis begins with the stasis of salivary flow in patients; stricture or obstruction of the ducts then follows . The stasis decreases the ability of saliva to contribute to oral hygiene and promote antimicrobial activity. Prevention Predisposing factors for acute suppurative sialadenitis include dehydration, immunosuppression, trauma, and debilitation. Therefore, a higher incidence of this infection is found in postoperative and elderly patients, as well as in patients who have undergone chemotherapy or radiation. Clinical Findings In addition to acute parotid swelling in parotitis, there may be overlying skin erythema, pain, tenderness, trismus, purulent ductal discharge , induration, accompanying fevers, or any combination of these symptoms and signs. The common bacteria cultured from purulent saliva include Staphylococcus aureus, Streptococcus pneumoniae, Escherichia coli, and Haemophilus influenzae. Other organisms obtained from chronically ill, hospitalized patients are Klebsiella, Enterobacter, Pseudomonas, and Candida. Complications If left untreated, acute suppurative sialadenitis can progress to an abscess, a potentially fatal complication in severely debilitated patients. Clinical palpation of the parotid gland may reveal significant induration and a doughlike consistency of the gland. An ultrasound or a computed tomography (CT) scan of the parotid gland may aid in locating an area of loculation. Treatment The principal treatment of acute suppurative sialadenitis includes rehydration, intravenous antibiotics with penicillinase-resistant gram-positive coverage, warm compresses, massage, sialogogues, improved oral hygiene, or a combination of these therapies. If there is no clinical improvement within 48 hours of nonsurgical therapy , then an abscess may be presumed . Incision and drainage using a parotidectomy incision may be performed. Care must always be used to avoid injury to the facial nerve. An alternative method may use CT- or ultrasound-guided imaging to perform a fine-needle aspiration of an abscess. Prognosis Most patients with acute suppurative sialadenitis respond to medical therapy. However, mortality rates may be higher in patients with severely debilitating or complicated medical conditions. In the case of submandibular sialadenitis, failure of improvement warrants consideration of other pathology: duct obstruction, abscess, salivary stones, or tumors . Submandibular abscesses can mimic Ludwig angina, a severe infection involving the floor of mouth and the submental and submandibular spaces. If not treated, Ludwig angina can lead to airway obstruction. Fattahi TT, Lyu PE, Van Sickels JE. Management of acute suppurative parotitis. J Oral Maxillofac Surg. 2002;60(4):446. (A review of the medical and surgical management of acute suppurative parotitis.) [PMID: 111928106]
| Honrado CP, Lam SM. Bilateral submandibular gland infection presenting as Ludwig angina: first report of a case. Ear Nose Throat J. 2001;80(4):217. (One potential complication of untreated acute submandibular sialadenitis and its management is discussed.) [PMID: 11338645]
| | | Chronic Granulomatous Sialadenitis Essentials of Diagnosis - Chronic unilateral or bilateral salivary gland swelling.
- Minimal pain.
- Fine-needle aspiration biopsy of the gland can aid in diagnosis.
- Risk factors such as exposure to tuberculosis, animal exposure, trauma, and multiorgan system involvement should be considered .
- Uveitis, facial palsy, and parotid enlargement are suggestive of sarcoidosis.
Clinical Findings Granulomatous disorders may present with acute salivary gland swelling or chronic unilateral glandular swelling. The glandular mass is not usually accompanied by significant pain. Primary tuberculosis should be considered if there are risk factors for exposure. Differential Diagnosis The diagnosis of tuberculous sialadenitis may be made with acid-fast staining for organisms, a culture of the saliva, and placement of a purified protein derivative skin test. A fine-needle aspirate of the gland helps to obtain material for diagnosis. Treatment of primary tuberculous sialadenitis includes multidrug antituberculous medications. The differential diagnoses of granulomatous sialadenitis include animal cat-scratch disease, sarcoidosis, actinomycosis, Wegener granulomatosis, and syphilis. Cat-Scratch Disease Cat-scratch disease does not directly involve the parotid gland; instead, it affects the periparotid and intraparotid lymph nodes. In the submandibular gland, it can present as an acute submandibular mass without causing ductal obstruction, which suggests the involvement of the adjacent lymph nodes. The offending organism is a gram-negative rod, Bartonella henselae, and diagnosis may be made with the Warthin-Starry silver stain . Cat-scratch disease is usually self-limiting and treatment is supportive while the mass lesions slowly resolve. Sarcoidosis Sarcoidosis is noninfectious and involves the parotid gland in less than 10% of cases. It is a diagnosis of exclusion and is confirmed by histologic findings of noncaseating granulomas. Sarcoidosis may occur as part of a syndrome known as uveoparotid fever or Heerfordt syndrome. This syndrome is characterized by parotid enlargement, facial palsy, and uveitis. The involvement of the parotid and lacrimal glands leads to xerostomia and xerophthalmia. The disease often affects adults in their twenties and thirties with spontaneous resolution occurring in the ensuing months to years. Actinomycosis Actinomycosis is easily diagnosed with special histologic stains that demonstrate sulfur granules. Actinomycosis should be suspected if a patient has painless parotid swelling with a history of recent dental infection or trauma. Trismus may develop with progression of the infection. Penicillin is the drug of choice for treatment of actinomycosis. Wegener Granulomatosis Wegener granulomatosis can present as an acute unilateral mass in the gland, often with pain. This diagnosis, characterized histologically by necrotizing inflammation and vasculitis, is confirmed with serologic testing for the cytoplasmic antineutrophil cytoplasmic antibody (C-ANCA) and histopathologic examination. The treatment of Wegener disease depends on the involvement of other organs; Wegener granulomatosis can be a rapidly fatal disease if it is untreated and involves other major organs. The initial treatment consists of several weeks of steroids with the addition of cyclophosphamide or other immunosuppressive agents. A more indolent subtype of Wegener, as often seen in the head and neck region, can be controlled with immunosuppressive therapy. The prognosis is excellent for many of the granulomatous diseases. Crean SJ, Adams R, Bennett J. Sublingual gland involvement in systemic Wegener granulomatosis: a case report. Int J Oral Maxillofac Surg. 2002;51(1):104. (A case report of sublingual gland involvement in systemic Wegener granulomatosis is discussed.) [PMID: 11936391]
| Garcia-Porrua C, Amor-Dorado JC, Gonzalez-Gay MA. Unilateral submandibular swelling as unique presentation of Wegener granulomatosis. Rheumatology. 2001;40:953. (A case report and description of the evaluation, diagnosis, and treatment of Wegener granulomatosis presenting in the salivary gland is presented.) [PMID: 11511775]
| Mandel L, Surattanont F, Miremadi R. Cat-scratch disease: considerations for dentistry. J Am Dent Assoc. 2001;132(7): 911. (Cat-scratch disease can mimic a salivary gland mass and should be considered in the differential diagnosis of salivary gland masses. A case report is also presented.) [PMID: 11480644]
| Surattanont F, Mandel L, Wolinsky B. Bilateral parotid swelling caused by sarcoidosis. J Am Dent Assoc. 2002;133(6):738. (A case report and discussion of sarcoidosis involving the salivary glands are presented.) [PMID: 12083650]
| | | HIV Infection Essentials of Diagnosis - Painless, bilateral enlarged parotid glands.
- Xerostomia.
- Known risk factors for HIV.
- Associated cervical lymphadenopathy may be associated.
- Presence of amylase in the cyst fluid helps confirm the diagnosis.
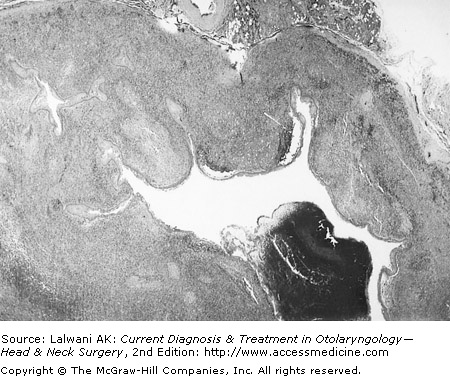
General Considerations Lymphoepithelial cysts associated with human immunodeficiency virus (HIV) occur almost exclusively in the parotid gland; however, anecdotal reports cite some occurrences of these cysts in the submandibular glands as an unusual finding. One possible explanation for the predominant presence of these cysts within the parotid gland is that this gland, unlike the submandibular gland, has intraglandular lymph nodes. Clinical Findings Symptoms and Signs HIV infection should be considered in a young individual with bilateral symmetric parotid swelling, especially if the parotid swelling appears multicystic; this finding may be the initial presenting symptom of HIV infection for some patients. Diagnostic Evaluation A CT scan or ultrasound may reveal bilateral multiple cystic masses in the parotid gland. Serologic testing for HIV antibodies confirms the diagnosis. Fine-needle aspiration of these cysts can reveal amylase in the fluid, which also leads to the diagnosis (see Figure 171). Treatment Observation or serial drainage of symptomatic cysts is the recommended treatment. A recent treatment modality includes sclerotherapy of the cysts. Rarely is parotidectomy indicated; however, when it is performed, the histopathology often shows multiple lymphoepithelial lesions and florid follicular hyperplasia with follicle lysis. Similarly, cysts involving the submandibular gland may require gland excision . Prognosis The parotid cysts found in HIV-infected patients are often associated with the histologic finding of benign lymphoepithelial lesions. There is little malignant transformation. Langford RJ, Whear NM. Serology should be a routine investigation when presented with a major salivary gland lump. Br J Oral Maxillofac Surg (Scotland). 2000;38(2):158. (Two cases where a serologic diagnosis may have precluded the need for the surgical biopsy of a salivary gland are discussed.) [PMID: 10864714]
| Marcus A, Moore CE. Sodium morrhuate sclerotherapy for the treatment of benign lymphoepithelial cysts of the parotid gland in the HIV patient. Laryngoscope. 2005;115(4):746. (A case report.) [PMID: 15805892]
| Uccini S, D'Offizi G. Cystic lymphoepithelial lesions of the parotid gland in HIV-1 infection. AIDS Patient Care STDS. 2000;14(3):143. (A review of rare benign cystic lymphoepithelial lesions of the parotid gland in HIV-infected patients is presented.) [PMID: 10763543]
| | | Sialolithiasis Essentials of Diagnosis - Acute, painful swelling of the major salivary gland, especially the submandibular gland, which may be recurrent.
- Aggravation of symptoms with eating ; swelling may subside after approximately 1 hour .
- History of gout or xerostomia.
- A stone in the floor of the mouth may be palpated; treatment depends on the location of the calculus.
- Calculus may be extracted intraorally, or if distal, then the submandibular gland may be indicated.
- Complications include acute suppurative sialadenitis, ductal ectasia, and stricture.
General Considerations Approximately 8090% of salivary calculi occur in the submandibular gland, whereas only 1020% are reported in the parotid gland; a very small percentage of salivary calculi are found in the sublingual and minor salivary glands. Sialolithiasis is a common cause of salivary gland disease and can occur at any age with a predilection in men. Risk factors for salivary stone obstruction include long illnesses with dehydration. There are also associations with gout, diabetes, and hypertension. Pathogenesis Normal saliva contains abundant hydroxyapatite, the primary compound in salivary stones. Aggregates of mineralized debris in the duct can form a nidus, promoting calculi formation, salivary stasis, and eventually obstruction. The submandibular gland is more susceptible to calculi formation than the parotid gland because of the longer course of its duct, higher salivary mucin and alkaline content, and higher concentrations of calcium and phosphate. Submandibular calculi consist primarily of calcium phosphate and hydroxyapatite; because of the high calcium content of these calculi, the majority are radiopaque and visualized on x-rays. Parotid calculi are less likely to be radiopaque. Approximately 75% of the time, a single stone is found in the gland. If the obstruction is not relieved, local inflammation, fibrosis, and acinar atrophy ensue. Clinical Findings Symptoms and Signs Recurrent swelling and pain in the submandibular gland exacerbated with eating is the common presentation of salivary calculi. Prolonged obstruction can lead to acute infection with increasing pain and erythema of the gland. Patients may also report a history of xerostomia and occasionally gritty, sandlike foreign bodies in their oral cavity. A physical exam is essential as stones often are palpated in the anterior two thirds of the submandibular duct. In addition, an induration of the mouth floor is sometimes observed . Stones located within the body of the gland are not easily palpated. Imaging X-rays with lateral and occlusal views can reveal a radiopaque stone, but these views are not always reliable. Intraoral views may be more helpful. Sialography is the most accurate imaging method to detect calculi. Sialography can be combined with CT scanning or magnetic resonance imaging (MRI), especially as CT scans are sensitive to calcium salts. Ultrasound has not proven to be useful. Endoscopy Recent advances in endoscopy have allowed endoscopic examination of the submandibular duct to detect calculi. Complications Persistent obstruction from sialolithiasis leads to salivary stasis. It also predisposes the gland to recurrent acute infections and even abscess formation. Treatment Intraoral Extraction Treatment is based on the location of the salivary stone. If the stone is palpated or visualized in the anterior portion of the submandibular duct and does not pass spontaneously, it can be extracted intraorally. The ductal papilla can be dilated serially with ease using graded lacrimal probes; the stone is then expressed . If the stone is too large, a more extensive intraoral procedure under local or general anesthesia may be attempted. The duct is cannulated, and an incision over the stone is created to allow extraction. No closure of the incision is made and careful attention must be paid to the adjacent lingual nerve. Surgical Excision Larger stones embedded in the hilum or the body of the submandibular gland causing symptoms may require surgical excision of the gland. Similarly, a symptomatic stone embedded in the body of the parotid gland will necessitate a parotidectomy. Endoscopic Techniques Recent endoscopic techniques allow an intraoral endoscopic extraction of salivary calculi and excision of the submandibular gland. The procedure has been performed with minimal morbidity and carries the advantage of avoiding a transverse cervical incision. Other Measures Other methods for calculi removal include wire basket extraction under radiologic guidance, pulsed dye laser lithotripsy, and extracorporeal shock wave lithotripsy. Prognosis The recurrence of stones is approximately 18%. If the risk factors are corrected, this may decrease the rate of recurrence . Guerrissi JO, Taborda G. Endoscopic excision of the submandibular gland by an intraoral approach. J Craniofac Surg. 2001;39(3):299. (A new, safe technique allowing intraoral excision of the submandibular gland in the treatment of sialadenitis is discussed.) [PMID: 11358106]
| Marchal F, Kurt AM. Histopathology of submandibular glands removed for sialolithiasis. Ann Otol Rhinol Laryngol. 2001;110:464. (A review of the pathophysiology of sialolithiasis is discussed.) [PMID: 11372932]
| | | Chronic Sialadenitis General Considerations Chronic sialadenitis results from either a decreased production of saliva or alterations in the salivary flow leading to salivary stasis. There may or may not be associated obstruction. This slow, progressive inflammatory process is usually found in adults, but it can affect children as well. Pathogenesis A decreased flow or stasis compromises the salivary functions, creating an environment at risk for infection. Chronic sialadenitis may be caused by retrograde infection from normal oral flora and chronic inflammation from repeated acute infections. In the latter, chronic inflammation causes changes in the ductal epithelium, which commonly leads to increased mucin in secretions, decreased flow, and mucous plugs. Histologically, the ductal epithelium in chronic sialadenitis may demonstrate mucous cell , squamous, or oncocytic metaplasia. There may be ductal dilatation and atrophy of the acinar cells. Prolonged inflammation can lead to fibrosis and infiltration with lymphocytes. If a stone obstruction is the cause, calculi may be seen within the ducts. Prevention A variety of conditions can cause chronic nonobstructive sialadenitis; these include repeated acute infections, trauma, radiation, and immunocompromised conditions. Histologic changes from radiation are likely permanent. Some patients may develop salivary gland swelling, xerostomia, and taste alterations after receiving intravenous iodine contrast. Smoking has also been found to predispose an individual to chronic sialadenitis because it reduces the antimicrobial activity of salivary secretions. Another condition known descriptively as chronic sclerosing sialadenitis or Kuttner tumor may be indistinguishable from neoplasia until a pathologic examination is done. Clinical Findings Presenting symptoms consist of chronic, intermittent painful swelling of the salivary gland, especially with eating. Swelling is often bilateral and may or may not be associated with an acute infection. A thorough history and physical examination can elicit risk factors and direct the search for treatable causes, such as a salivary stone. A CT scan or MRI may help to exclude a malignant tumor, especially if there is an associated fibrous mass in the parotid gland. Sialography and fine-needle aspiration have not been consistently diagnostic; however, sialographs can be helpful in finding obstructions, acinar atrophy, and irregular dilatations of the ducts. Differential Diagnosis The differential diagnoses include granulomatous diseases, sialolithiasis, sarcoidosis, benign lymphoepithelial lesion, inflammatory pseudotumors, Sjgren syndrome, and Mikulicz syndrome. Complications As a reactive process to trauma or disease, chronic nonobstructive sialadenitis may progress to a fibrous mass formation or an inflammatory pseudotumor. Other complications of the disease include pain and permanent damage to the acinar unit and ductal epithelium. Progressive changes further compromise the function of the acinar units, which clinically manifest as bulging, irregular, nodular glands. Treatment Conservative therapy and surgical gland excision are the most successful treatment methods of chronic nonobstructive sialadenitis. If no treatable cause is identified, patients are encouraged to improve oral hygiene with increased hydration, massage of the affected gland, adequate nutrition, and use of sialagogues. Antibiotics are administered with acute exacerbations. Superficial parotidectomy is the common surgical treatment of persistent symptoms in the parotid gland. Alternative treatments include iatrogenic fibrosis of the gland with 1% methyl violet and low-dose radiation therapy. Procedures such as parotid duct ligation and tympanic neurectomy, used to cease secretion, also may prove therapeutic. Prognosis The prognosis depends on treating an identifiable underlying cause; few recurrences have been reported following these treatments. Huang C, Damrose E, Bhuta S, Abemayor E. Kuttner tumor (chronic sclerosing sialadenitis. Am J Otolaryngol. 2003;24(4): 278. (A case report and discussion.) [PMID: 12430136]
| Mandel SJ, Mandel L. Radioactive iodine and the salivary glands. Thyroid . 2003;13(3):265.. (Description of a side effect to the salivary glands from radioactive iodine therapy.) [PMID: 12729475]
| Qi S, Liu X, Wang S. Sialoendoscopic and irrigation findings in chronic obstructive parotitis. Laryngoscope. 2005;115(3):541. (Sialoendoscopy can provide more detailed observation of the salivary ductal system.) [PMID: 15744174]
| | | Sjgren Syndrome Essentials of Diagnosis - Salivary gland swelling with dryness of the mouth and eyes leading to oral and ocular pain and sensitivity.
- Often associated with another connective tissue disease.
- More commonly seen in postmenopausal women.
- Detection of autoantibodies SS-A and SS-B and others, along with minor salivary gland biopsy, may confirm the diagnosis.
- Slowly progressive disease.
- High risk for development of malignant lymphoma in primary Sjgren syndrome.
General Considerations Sjgren syndrome is an autoimmune disorder classically characterized by parotid enlargement, xerostomia, and keratoconjunctivitis sicca. It also may be associated with a connective tissue disease such as rheumatoid arthritis or systemic lupus erythematosus. Sjgren syndrome occurs 90% of the time in females, usually in their sixth decade . It is the second most common connective tissue disorder; only rheumatoid arthritis occurs more frequently. Clinical Findings Symptoms and Signs Patients often present with bilateral, nontender salivary gland enlargement. The parotid swelling may occur intermittently or stay constant. Other symptoms include dry eye, dry mouth, altered taste, dry skin, myalgia, vaginal dryness, vasculitis, and arthritis. Laboratory Findings Useful laboratory tests showing the presence of SS-A or SS-B autoantibodies, rheumatoid factor, or antinuclear antibodies can aid the diagnosis. The microscopic examination of a minor salivary gland biopsy such as from the lip, can confirm Sjgren disease. According to histologic criteria, a focus score of greater than 1 focus/4 mm 2 is diagnostic. Characteristic histopathologic findings include a lymphocytic infiltrate in acinar units and epimyoepithelial islands surrounded by lymphoid stroma. Differential Diagnosis The differential diagnoses include benign lymphoepithelial lesion, also known as Mikulicz syndrome, and chronic nonobstructive sialadenitis. Complications Complications of primary Sjgren syndrome result from chronic progression of the disease. The deterioration of salivary function can cause patients to have difficulties with speaking, swallowing, and masticating; in addition, increased dental decay with loss of teeth and oral mucosal discomfort can result. More importantly, there is an approximate 10% incidence of lymphoma in patients with primary Sjgren syndrome. Treatment Treatment is symptomatic and supportive. Steroids and topical steroid eyedrops may be indicated for severe symptoms. Superficial parotidectomy may be required for severe recurrent parotid infections. Prognosis The prognosis for those affected with Sjgren syndrome is generally favorable. However, there is an increased incidence in malignant lymphoma or lymphoepithelial carcinoma in patients with this syndrome. Therefore, careful observation with appropriate diagnostic studies is recommended. Gannot G, Lancaster HE. Clinical course of primary Sjgren syndrome: salivary, oral, and serologic aspects. J Rheumatol. 2000;27(8):1905. (Primary Sjgren syndrome is a slow, progressive disease that affects salivary gland function. There is a high incidence of lymphoma in these patients.) [PMID: 10955331]
| | | Benign Lymphoepithelial Lesions Essentials of Diagnosis - Unilateral firm or cystic swelling of the parotid gland, with bilateral involvement in approximately 20% of cases.
- Parotid gland most often involved, but the submandibular gland may also be involved.
- Most often seen in HIV-infected populations.
- Fine-needle aspiration aids in diagnosis, showing acinar atrophy with diffuse lymphocytic infiltration, and foci of epimyoepithelial islands.
- Disease may progress to near total or total replacement of acinar tissue in the gland.
- Higher probability of progression to low-grade B-cell lymphoma of mucosa-associated lymphoid tissue (MALT).
General Considerations Benign lymphoepithelial lesions are also known as Godwin tumor, Mikulicz syndrome, or punctate parotitis. Benign lymphoepithelial lesion has a predilection for females, especially in the fifth and sixth decades of life. It is also associated with multicystic disease in HIV-infected patients. Pathogenesis A benign lymphoepithelial lesion is an inflammatory process characterized by lymphocytic infiltration around salivary gland ducts and parenchyma (Figure 171). With increasing lymphocytic infiltration, progressive acinar atrophy and even replacement of the acini result. Upon further progression, the ductal epithelia proliferate and eventually cause ductal obstruction. Clinical Findings Patients often present with recurrent unilateral firm or cystic swelling of the parotid gland with or without pain. Bilateral involvement occurs in 20% of cases. Fine-needle aspiration of the parotid mass is helpful. Sialography is rarely indicated unless a stone is suspected. This condition often affects the parotid gland and rarely affects the submandibular gland; when it does affect the submandibular gland, it presents as a painless mass. There may be an associated reactive lymphadenopathy. The diagnosis is best made on histopathologic findings of acinar atrophy with diffuse lymphocytic infiltration, with or without the presence of epimyoepithelial islands. There is an association with Sjgren syndrome. Complications Cases of progression to neoplastic disease can result, including lymphoepithelial carcinoma, low-grade B-cell lymphoma of MALT pseudolymphoma, and non-Hodgkin lymphoma. There is also an association with Kaposi sarcoma in HIV-infected patients. Treatment & Prognosis The treatment of benign lymphoepithelial lesion is symptomatic unless the parotid enlargement is severe enough to warrant a superficial parotidectomy. Complete submandibular excision is an adequate treatment of the rare benign lymphoepithelial cyst. Infrequently, there is malignant transformation; however, careful observation is warranted even after complete excision of the gland. Carbone A. Pathologic features of lymphoid proliferations of the salivary glands: lymphoepithelial sialadenitis versus low-grade B-cell lymphoma of the malt type. Ann Otol Rhinol Laryngol. 2000;109:1170. (A histopathologic study concluding that the distinction between benign lymphoepithelial lesions of the salivary glands and low-grade B-cell lymphoma of mucosa-associated lymphoid tissues relies on evaluation of morphologic features of the gland.) [PMID: 11130833]
| Ussmuller J, Reinecke T, Donath K, Jaehne M. Chronic myoepithelial sialadenitis: symptomatology, clinical signs, differential diagnostics. Laryngorhinootologie. 2002;81(2):111. (A retrospective chart review of patients with myoepithelial sialadenitisie, benign lymphoepithelial lesionshowing that the clinical relevance of this diagnosis lies in the higher risk of developing malignant lymphoma.) [PMID: 11914948]
| | | Kimura Disease Essentials of Diagnosis - Slowly growing, painless mass in the major salivary gland, primarily in Asians.
- Commonly seen in the second and third decades; 80% of patients are male.
- Enlargement of gland accompanied by regional lymphadenopathy.
- Serologic tests often demonstrate peripheral eosinophilia and elevated IgE levels.
- Recurrence may occur after surgical excision of the gland.
General Considerations Kimura disease is a rare, benign chronic inflammatory disease mimicking a tumor in regions of the head and neck. It occurs predominantly in young Asian males in their twenties and thirties. Clinical Findings When Kimura disease occurs in the head and neck regions, the major salivary glands are usually involved. In the parotid and submandibular glands, this disease presents as painless superficial swellings often accompanied by regional lymphadenopathy. The formation of lymphoid follicles and the aggregation of eosinophils in the affected tissues are found on histologic examination. Differential Diagnosis The differential diagnoses of Kimura disease include the following: (1) angiolymphoid hyperplasia with eosinophilia, (2) reactive lymphadenopathy, (3) parotid tumor, (4) extranodal manifestations of Rosai-Dorfman disease, and (5) benign lymphoepithelial lesion. Angiolymphoid hyperplasia with eosinophilia differs from Kimura disease in the lack of lymphadenopathy and decreased eosinophilia. Rosai-Dorfman disease is an idiopathic benign condition characterized by histiocytic proliferation and massive lymphadenopathy, including involvement of the intraparotid lymph nodes. Treatment The treatment of choice when Kimura disease is found in the parotid gland is parotidectomy with continued observation for potential recurrence. Kimura disease of the submandibular gland is usually treated with excision of the gland and the adjacent lymph nodes. Because Kimura disease often affects other sites, systemic therapy with steroids and radiation also may prove beneficial. | | Necrotizing Sialometaplasia Necrotizing sialometaplasia is a benign, self-healing inflammatory process mainly involving the minor salivary glands. It has a predilection in males and occurs over a wide age range. It presents as a spontaneously appearing, painless ulceration or swelling usually over the hard palate, but can occur wherever there are salivary gland tissues. The lesions are usually unilateral and can present with burning sensations and numbness. The cause is unknown, but there are associations with trauma and radiation therapy. The pathogenesis is thought to be ischemic. The diagnosis of necrotizing sialometaplasia is confirmed on biopsy. Histology shows the characteristic pseudoepitheliomatous hyperplasia and squamous metaplasia. Care must be taken to avoid confusing the diagnosis with squamous cell carcinoma or mucoepidermoid carcinoma; the main complication is misdiagnosis. Lesions in necrotizing sialometaplasia are self-healing, usually by secondary intention , and recurrences are rare. | | Adenomatoid Hyperplasia Adenomatoid hyperplasia is a rare swelling of the minor salivary glands that occurs most commonly in the palate. Local trauma, environmental irritation, and chronic inflammation are the proposed causes of this condition. Patients present with painless swellings that have been present for an indeterminate length of time. The overlying mucosa usually appears normal. Adenomatoid hyperplasia must be distinguished from minor salivary gland tumors. The differential diagnoses include benign and malignant tumors. Histologic examination reveals glandular hypertrophy and inflammatory infiltrates, but no change in the general architecture of the gland and no evidence of neoplasia or atypia. Complete excision is the treatment of choice. Because of the higher incidence of malignant tumors within the hard palate, the key is to distinguish malignant tumors from benign adenomatoid hyperplasia. Shimoyama T, Wakabayashi M. Adenomatoid hyperplasia of the palate mimicking clinically as a salivary gland tumor. J Oral Sci. 2001;43(2):135. (A case report distinguishing adenomatoid hyperplasia from salivary gland tumors based on immunohistologic findings is presented.) [PMID: 11515598]
| | | Sialadenosis Essentials of Diagnosis - Bilateral, occasionally unilateral, diffuse enlargement of the salivary glands, particularly the parotid glands.
- Pain may or may not be associated.
- The condition usually begins between the ages of 20 and 60 years and may persist for more than 20 years.
- In half of the cases, there are associated underlying systemic factors, including endocrine disorders, malnutrition, and drugs.
- Biopsy of the affected gland shows acinar enlargement.
- The cause is peripheral autonomic neuropathy of the salivary glands; present treatments are not entirely satisfactory as they do not address this underlying cause.
- Surgery should be reserved if cosmetic deformity of the gland is unacceptable.
General Considerations Sialadenosis, or sialosis, is a rare, noninflammatory condition that causes bilateral, diffuse, and painless enlargement of the salivary glands. This condition may also cause degenerative changes to the autonomic innervation of the glands. The parotid gland is the most affected, followed by the submandibular gland. Prevention Although the etiology is not clear, several metabolic and medical conditions are associated with sialadenosis. These include obesity, alcoholic cirrhosis, diabetes, hyperlipidemia, hypothyroidism , anemia, pregnancy , malnutrition, menopause, and even certain medications (eg, clozapine). Clinical Findings A thorough physical exam and screening are necessary. Fine-needle aspiration complemented with CT scanning can establish the diagnosis. Histopathologic findings show acinar enlargement. Treatment & Prognosis The treatment of sialadenosis is directed at the underlying conditions. Parotidectomy is considered if the parotid enlargement is cosmetically unacceptable. Surgical resection of the affected submandibular gland is the treatment of choice; but unless correction of the underlying disorder is addressed, there may be persistent enlargement of any residual glands. The prognosis is therefore dependent on treatment of the underlying conditions. Kastin B, Mandel L. Alcoholic sialosis. NY State Dent J. 2000;66(6):22. (Sialosis or sialadenosis is a benign salivary disorder often associated with alcoholism, endocrine disorders, and malnutrition. The presence of sialosis warrants further investigation into these unsuspected systemic disorders.) [PMID: 11132299]
| | | Parotid Cysts Essentials of Diagnosis - Fluctuant swellings of the salivary glands.
- Cysts of the parotid gland may be acquired or congenital.
- Congenital cysts may be either Type I or Type II branchial arch cysts.
- Acquired cysts may occur secondary to trauma, sialolithiasis, ductal stricture, or benign lymphoepithelial lesions.
- HIV should be considered in the differential diagnosis.
True cysts of the parotid gland account for 25% of parotid lesions. Classification Congenital Parotid Cysts Branchial Cleft Anomalies Congenital cysts may result from branchial cleft anomalies; these anomalies are subdivided into Type I and Type II cysts. Type I Cysts Type I cysts are a duplication anomaly of the ectodermal external auditory canal. The cyst may be located anteroinferior to the ear lobule. Type II Cysts Type II cysts consist of ectodermal and mesodermal elements and may open anteriorly to either the sternocleidomastoid muscle or the external auditory canal. Both Type I and Type II branchial cleft anomalies may have sinus tracts, which are intimately related to the facial nerve. Therefore, excision of these congenital parotid cysts requires a parotidectomy approach and preservation of the facial nerve. Dermoid Cysts A second type of congenital cyst occurring in the parotid gland is a dermoid cyst. This cyst results from trapped embryonic epidermis and presents as a rounded mass. It contains keratinizing squamous epithelium, sweat glands, and other associated skin appendages. Excision to prevent recurrent infections, with attention to the facial nerve, is the most successful treatment. Acquired Parotid Cysts Acquired cysts of the parotid gland may result from other parotid disorders such as tumors, trauma, chronic sialadenitis, sialolithiasis, and radiation injury. Cysts related to HIV infection have been discussed earlier in this chapter. Nasuti JF, Yu GH, Gupta PK. Fine-needle aspiration of cystic parotid gland lesions: an institutional review of 46 cases with histologic correlation. Cancer. 2000;90(2):111. (A retrospective study of 46 cases of patients with cystic parotid lesions was performed to determine the diagnostic accuracy of fine-needle cytology.) [PMID: 10794160]
| Orvidas LJ, Kasperbauer JL, Lewis JE, Olsen KD, Lesnick TG. Pediatric parotid masses. Arch Otolaryngol Head Neck Surg. 2000;126(2):177. (A retrospective review of pediatric parotid masses demonstrates a variety of pathologic diagnoses, including benign tumors, branchial cleft cysts, vascular malformations, and malignant entities.) [PMID: 10680869]
| | | Congenital Salivary Fistulas of the Submandibular Gland Congenital salivary fistulas and sinus tracts are exceedingly rare. They are thought to arise from aberrant salivary gland tissue or aberrant gland formation during the end of the sixth week of gestation. These fistula and sinus tracts may form cutaneous openings in the submandibular skin with discharge. A fistulogram or MRI may help with the diagnosis. Complete surgical excision is the recommended treatment. Kapadia LA, McClay JE. Congenital midline submandibular sinus tract . Int J Pediatr Otorhinolaryngol. 2000;53(3):221. (A case report and discussion of a rare case of a salivary gland sinus tract.) [PMID: 10930638]
| | | Mucoceles Essentials of Diagnosis - Painless, cystic lesions commonly seen on the lip, oral cavity, and often with mucous extravasation.
- Cystic lesion in the floor of mouth may be localized or extend into the neck, presenting as a neck mass.
- Presentation may be preceded by minor trauma to soft tissue or oral mucosa.
General Considerations Mucoceles represent dilatations of the minor salivary gland ducts due to both accumulated mucous secretions and, often, mucous extravasations into the connective tissue. Mucoceles are fairly common and are seen frequently in the lip (6070%), buccal mucosa, floor of the mouth, and palate. When a mucocele appears in the mouth floor, it is defined as a ranula (related to the Latin term for frog). It is also known as a mucous retention cyst. Pathogenesis Mucoceles are thought to arise from either a trauma to or a rupture of the minor salivary gland ducts with extravasation of mucus into the surrounding tissue. Sublingual glands and minor salivary glands are more susceptible to developing mucoceles owing to continuous mucous secretions in these glands, whereas the parotid and submandibular glands secrete on stimulation. The cause of ranulas is not as clear. Clinical Findings Mucous retention cysts generally present as pale, smooth, bluish-hued submucosal cysts. They are painless and may slowly enlarge. Ranulas, involving the sublingual or submandibular ducts, present as round, fluctuant masses in the mouth floor. They are usually unilateral and may affect any age group with no gender preference. A simple ranula is a true cyst with an epithelial lining that occurs intraorally with elevation of the mouth floor. A plunging ranula extends below the mylohyoid muscle, beyond the sublingual space, and involves the submandibular space. It may extend further inferiorly to present as a painless submandibular or cervical neck mass. Unlike a simple ranula, a plunging ranula does not have an epithelial lining and therefore is classified as a pseudocyst. A physical exam is usually adequate for the diagnosis, but a CT scan can provide excellent views of the extent of the cyst. Complications Mucoceles and ranulas cause few complications. However, infections can occur. Differential Diagnosis The differential diagnoses include cystic hygroma, lymphangioma, thyroglossal duct cyst, and dermoid cyst. An important differential diagnosis for a mucous retention cyst is malignant mucoepidermoid carcinoma. Treatment & Prognosis A complete surgical intraoral excision of a mucous retention cyst is curative with few recurrences at the site. The treatment of a simple ranula consists of either simple excision of the cyst and possible removal of the associated gland, or marsupialization of the cyst wall. Recurrences are possible with the latter procedure. In the case of plunging ranulas, treatment requires excision either intraorally or combined with a cervical incision and extirpation of the associated gland. Recurrence can occur with inadequate excision. Anastassov GE, Haiavy J. Submandibular gland mucocele: diagnosis and management. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89(2):159. (A review of the pathophysiology of mucoceles and rare occurrences in the submandibular gland is presented.) [PMID: 10673650]
| Kapadia LA, McClay JE. Congenital midline submandibular sinus tract. Int J Pediatr Otorhinolarygol. 2000;53(3):221. (A case report and discussion of rare congenital fistula, cysts, and sinus tracts of the salivary glands that present as head and neck masses is presented.) [PMID: 10930638]
|
| | | Xerostomia Xerostomia is defined as dry mouth. In addition to the discomfort from dry mouth, patients with xerostomia may also experience an altered sense of taste, dysphagia, and complications related to dental decay. Disorders of salivary flow in the parotid gland can cause this condition. In addition, many systemic conditions can result in dry mouth: Sjgren syndrome, stress, diabetes, chronic infection, and irradiation. Xerostomia also results as a side effect of a variety of medications. The treatment of xerostomia is aimed at the underlying conditions; symptomatic treatment includes an increased intake of fluids, sialagogues, mouthwashes, and artificial saliva. In addition, there are currently medications prescribed to minimize xerostomia for patients undergoing radiation. Daniels T. Evaluation, differential diagnosis, and treatment of xerostomia. J Rheumatol Suppl. 2000;61:6. (A review of the clinical course of xerostomia, including its differential diagnosis and treatment, is presented. The treatment combines dental decay prevention, salivary flow stimulation, the treatment of chronic oral candidiasis, and the use of salivary substitutes. Also presented is a review of pharmacotherapeutics.) [PMID: 11128701]
| | | Ptyalism Ptyalism refers to the hyperproduction of saliva. It is associated with a number of medical conditions, including inflammation, cerebral palsy, and pregnancy. Medications may also produce ptyalism as a side effect. If medications with drying agents are not effective, surgical treatment is indicated. Other treatment options include selective neurectomy of the chorda tympani nerve, excision of the salivary gland, and either ligation or transposition of the affected duct. | | Benign Neoplastic Diseases: Introduction Essentials of Diagnosis - 6480% percent of primary salivary tumors occur in the salivary gland, 715% occur in the submandibular gland, and < 1% occur in the sublingual glands.
- 5480% of all tumors are benign.
- Peak incidence of salivary tumors occurs in the sixth to seventh decades.
- Painless, slowly enlarging solitary mass in the salivary gland.
- Deep parotid lobe tumors may present as a painless, asymmetric swelling of the soft palate.
- Fine-needle aspiration cytology and imaging aid in the diagnosis.
- Complete surgical excision is most often curative.
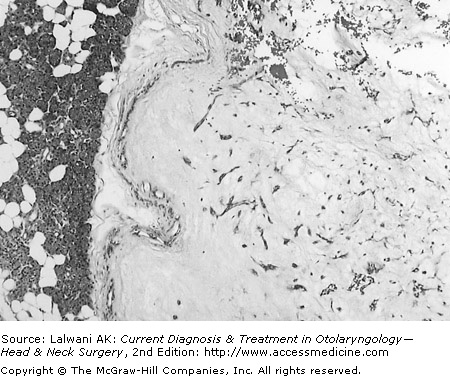
General Considerations Approximately 80% of salivary gland tumors occur in the parotid gland. Of these tumors, approximately 7580% are benign. There is no consistent correlation between the rate of tumor growth and whether a tumor is benign or malignant. Most benign tumors of the parotid gland are epithelial tumors. In general, only 15% of diseases of the submandibular gland are neoplastic. Compared with parotid tumors, approximately 5060% of submandibular tumors are benign. Minor salivary gland tumors account for approximately 15% of all salivary gland tumors. It is estimated that only 35% of minor salivary gland tumors are benign, with pleomorphic adenoma being the most common neoplasm followed by basal cell adenoma. Clinical Findings Most benign parotid tumors present as slow-growing, painless masses often in the tail of the parotid gland. Tumors of the other salivary glands similarly present as painless masses. Fine-needle aspiration of salivary tumors, although not as sensitive or specific as in other tumors (eg, the thyroid), is extremely useful in differentiating between malignant and benign processes. The accuracy rate is approximately 85% in determining if a parotid tumor is benign or malignant; this rate is higher when determining whether or not a lesion originates from parotid tissue. CT scanning and MRI may help identify deep lobe tumors if clinically warranted. Differential Diagnosis The differential diagnoses of benign salivary gland tumors not only include each other, but must also alert a clinician to their malignant counterparts. Various other benign neoplastic entities involving the salivary glands must be considered: papillary ductal adenomas, sebaceous adenomas, ancient schwannomas, congenital epithelial tumors, cavernous hemangiomas , and ectopic extraglandular tissues. Fine-needle aspiration is most useful in determining whether an asymptomatic mass in the region of the parotid gland or submandibular space is of glandular origin or not. Treatment options can be tailored based on these initial findings. Complications Complications of pleomorphic adenomas are rare and include malignant transformation into a carcinoma ex-pleomorphic adenoma. There is rare malignant transformation of Warthin tumor, monomorphic adenomas, and the benign salivary tumors to be described. Little is known about the incidence of the malignant transformation of tumors found in the submandibular gland. Complete excision ensures an excellent prognosis; however, recurrence occurs if there are positive margins. With the repeat excision of recurrences, the risk to the facial nerve expectedly rises. Recurrent tumors are frequently multinodular. Recurrence can be attributed to either inadequate margins, or in the case of Warthin tumor, to its multicentricity. Treatment Complete surgical excision with uninvolved margins is the recommended treatment of benign tumors of the salivary glands. Usually, a superficial parotidectomy with preservation of the facial nerve is adequate unless there is deep lobe involvement. Parapharyngeal space tumors require resection through a form of transcervical approach. Enucleation alone is inadequate for tumors of the parotid gland; a complete submandibular excision, with preservation of the marginal mandibular, lingual, and hypoglossal nerves, is the treatment of choice. Radiation is not indicated in the treatment of benign salivary tumors. Prognosis With the complete removal of the tumor and excision of the affected gland, the prognosis is excellent. Malignant transformation and recurrences are rare. | | Pleomorphic Adenomas Pleomorphic adenomas, or benign mixed tumors, are the most common neoplasms of the salivary glands (Figure 172). They represent approximately 6070% of all parotid tumors and 90% of submandibular benign tumors. These neoplasms affect females more than males and are commonly seen in the third to sixth decades of life. When the deep parotid lobe is involved, a pleomorphic adenoma can present as a parapharyngeal space tumor with soft palate swelling. It presents as an isolated swelling or mass in the submandibular gland with little associated pain. There are no known etiologic factors. Histologically, pleomorphic adenomas arise from the distal portions of the salivary ducts, including the intercalated ducts and acini. The mixture of epithelial, myoepithelial, and stromal elements is represented by the name , benign mixed tumor. Any of these individual components may predominate in the histology, but all three must be present to confirm the diagnosis. Both immunohistochemical stains specific for myoepithelial cells and epithelial cells can help to distinguish pleomorphic adenoma. The differential diagnoses for pleomorphic adenomas should include malignant neoplasms: adenoid cystic carcinoma, polymorphous low-grade adenocarcinoma, deep-seated adnexal neoplasms, and mesenchymal neoplasms. Rare complications of pleomorphic adenoma include malignant transformation into a tumor known as carcinoma ex-pleomorphic adenoma, or alternately, "benign" metastasizing mixed tumors. The word "benign" describes solely the histology, but not the pathologic behavior of this rare entity. Although radiation is not indicated in the treatment of benign salivary tumors, it has been used occasionally to control recurrent pleomorphic adenomas. Complete surgical excision of the tumor with uninvolved margins is the recommended treatment. For example, a superficial parotidectomy with clear margins is the treatment for a pleomorphic adenoma located in the superficial lobe of the parotid gland. The prognosis for pleomorphic adenomas is excellent, with a 96% rate of nonrecurrence. Webb AJ, Eveson JW. Pleomorphic adenomas of the major salivary glands: a study of the capsular form in relation to surgical management. Clin Otolaryngol. 2001;26(2):134. (This article provides a retrospective study that correlates capsular characteristics to histopathology. It also confirms that a parotidectomy is the treatment of choice over enucleation.) [PMID: 11309055]
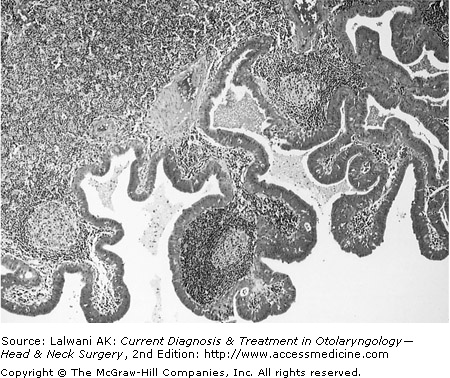
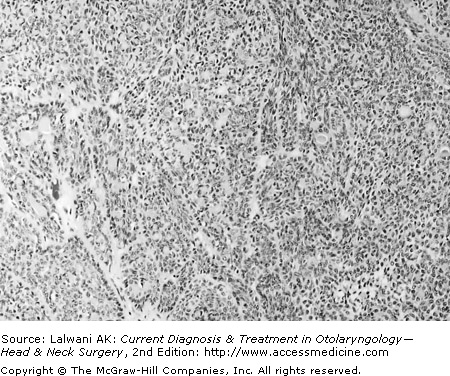
| | | Warthin Tumor Warthin tumor is also known as papillary cystadenoma lymphomatosum and is found almost exclusively in the parotid gland (Figure 173). It is characterized histologically by papillary structures composed of double layers of granular eosinophilic cells or oncocytes, cystic changes, and mature lymphocytic infiltration. It arises from the ectopic ductal epithelium. It represents approximately 5% of all salivary gland tumors and approximately 12% of benign tumors of the parotid gland. This tumor is more commonly seen in males in the fifth to seventh decades of life and there is an associated risk with smokers. There is approximately 5.07.5% bilaterality and 14% multicentricity in Warthin tumor. CT scanning may demonstrate a well-defined mass in the posteroinferior segment of the superficial lobe of the parotid. If radiosialography is performed, increased activity is seen related to the presence of oncocytes and their increased mitochondrial content. The diagnosis of Warthin tumor is easily arrived at based on histologic findings, with rare confusion with other tumors. The treatment requires complete excision of the affected portion of the gland with uninvolved margins. | | Monomorphic Adenomas These slow-growing tumors represent less than 5% of all salivary gland tumors (Figure 174). Monomorphic adenomas differ from pleomorphic adenomas, in that they consist of only one morphologic cell type. Monomorphic adenomas are subclassified into a group of mostly epithelial and myoepithelial neoplasms that include basal cell adenomas, canalicular adenomas, oncocytomas or oxyphilic adenomas, and myoepitheliomas. Basal Cell Adenomas Basal cell adenomas account for 2% of all epithelial salivary gland neoplasms. Histologic types include tubular, trabecular, cylindroma, and solid; the latter is the most common variant. Basal cell adenomas occur equally between males and females and usually between the fourth and ninth decades of life. The parotid gland is the most common site involved. A basal cell adenoma must be differentiated from adenoid cystic carcinoma, basal cell adenocarcinoma, and ameloblastoma. Canalicular Adenomas The canalicular adenoma is a benign neoplasm that affects the minor salivary glands. This tumor used to be a subtype of the basal cell adenoma; however, it is now recognized as a separate entity based on histologic features. It must also be differentiated from adenocarcinoma. The canalicular adenoma tends to be multifocal and often occurs in the upper lip mucosa, especially in the elderly. Complete intraoral excision is curative, although the multifocality of the disease can predispose to recurrence if all foci are not addressed. Oncocytomas These benign tumors are composed of large polyhedron-shaped epithelial cells, known as oncocytes, packed with granular eosinophilic cytoplasm and mitochondria. The cytoarchitecture of these tumors is best visualized with electron microscopy. Oncocytomas account for < 1% of all salivary gland neoplasms. There is no gender predilection and they occur in the sixth to eighth decades of life. There remains debate on the pathogenesis of these tumors and whether they are true neoplasms; oncocytomas may result from a hyperplastic process, a metaplastic process, or both. The parotid gland is the most common site of an oncocytoma, followed by the submandibular gland. In these sites, this tumor presents as a painless, slow-growing mass that is often solid and occasionally cystic. The swelling of the parotid gland may be diffuse with approximately 7% bilaterality. Multiple tumors have also been reported. Owing to the high mitochondrial content of the cells, radiosialography can demonstrate high uptake of technetium-99m. The oncocytoma is easily distinguished from Warthin tumor and pleomorphic adenoma. However, it must also be considered separately from the mucoepidermoid carcinoma, acinic cell adenocarcinoma, adenoid cystic carcinoma, clear cell carcinoma, and metastatic renal cell or thyroid carcinoma. Surgical excision with uninvolved margins is the recommended treatment; oncocytomas are radioresistant. Myoepitheliomas This subtype of monomorphic adenomas accounts for less than 1% of all salivary gland neoplasms. It consists almost exclusively of myoepithelial cells. There is no gender predilection and myoepitheliomas are commonly seen in the third to sixth decades of life. The tumor occurs in the parotid gland 40% of the time. Histologically, myoepitheliomas are well encapsulated. There are spindle cell and plasmacytoid cell types. The differential diagnoses include mixed tumor, schwannoma, leiomyoma, plasmacytoma, spindle cell carcinoma, and fibrous histiocytoma. Mirza S, Dutt SN, Irving RM, Jones EL. Intraductal papilloma of the submandibular gland. J Laryngol Otol. 2000:114(6):481. (Case report of intraductal papillomas in the submandibular gland; this entity is more commonly seen in the minor salivary glands.) [PMID: 0010962690]
| Toida M et al. Intraoral minor salivary gland tumors: a clinicopathological study of 82 cases. Int J Oral Maxillofac Surg. 2005;34(5):528.. (Retrospective study of 82 patients with intraoral minor salivary gland tumors at a university hospital.) [PMID: 16053873]
| | | Granular Cell Tumors The granular cell tumor is benign with malignant potential and is most commonly associated with the minor salivary glands. This tumor tends to occur in the oral cavity and is well circumscribed, mobile, and painless. Fine-needle aspiration can demonstrate a neoplastic process. A histopathologic examination shows polygonal cells with abundant eosinophilic granular cytoplasm and mildly pleomorphic nuclei that are round to oval-shaped. Because of its malignant potential, a combination of wide local excision and close observation is the most effective treatment. Hughes JH, Volk EE, Seethala RR, LiVolsi VA, Baloch ZW. Relative accuracy of fine-needle aspiration and frozen section in the diagnosis of lesions of the parotid gland. Head Neck. 2005;27(3):217. (Clinical review of 220 cases of parotid gland fine-needle aspiration with histologic follow-up.) [PMID: 15672359]
| Wilbur DC. Pitfalls in salivary gland fine-needle aspiration cytology. Arch Pathol Lab Med. 2005;129(1):26. (Data confirming the difficulty in interpreting cytology from salivary gland specimens to minimize diagnostic errors.) [PMID: 15628905]
| | | Hemangiomas General Considerations Although not of glandular origin, hemangiomas are significant in the differential diagnosis of a parotid mass, especially in children. These benign tumors are of endothelial cell origin and represent less than 5% of all salivary gland tumors. In children, the capillary hemangioma is the most common salivary gland tumor, accounting for more than 90% of parotid gland tumors in children less than 1 year of age. It affects females more than males and almost exclusively occurs in the parotid gland. Clinical Findings A hemangioma usually presents at birth as a unilateral, painless mass. It has a rapid, proliferative growth that often causes cosmetic deformity. Fine-needle aspiration is usually not necessary. CT scanning, MRI, or both may demonstrate the vascularity of the lesion. The differential diagnosis includes other vascular proliferative disorders such as lymphangioma and cavernous hemangioma. Treatment The possibility of spontaneous regression exists and therefore surgical excision may be delayed. However, if there is significant cosmetic or functional compromise, complete excision via parotidectomy with facial nerve preservation may be indicated. A caveat in children is the more superficial location of the facial nerve than that seen in adults, which is important to consider during intraoperative identification of the nerve. Malignant transformation has not been described. Bentz BG, Hughes CA, Ludemman JP, Maddolozzo J. Masses of the salivary gland region in children. Arch Otolaryngol Head Neck Surg. 2000;126(12):1435. (A retrospective review of salivary masses in children demonstrating predominance of vascular lesion over solid tumors is presented.) [PMID: 11115277]
| Zbaren P, Schar C, Hotz MA, Loosli H. Value of fine-needle aspiration cytology of parotid gland masses. Laryngoscope. 2001;111:1989. (Fine-needle aspiration cytology is a valuable adjunct to preoperative assessment of parotid masses; it provides an 86% accuracy rate, a 64% sensitivity rate, and a specificity rate of 95%.) [PMID: 0011801984]
| | | | |
 Print Close Window
Print Close Window