11 - Cardiovascular Disorders
Editors: Kane, Robert L.; Ouslander, Joseph G.; Abrass, Itamar B.
Title: Essentials of Clinical Geriatrics, 5th Edition
Copyright 2004 McGraw-Hill
> Table of Contents > Part II - Differential Diagnosis and Management > Chapter 10 - Immobility
function show_scrollbar() {}
Chapter 10
Immobility
Immobility is a common pathway by which a host of diseases and problems in older individuals produce further disability. Immobility often cannot be prevented, but many of its adverse effects can be. Improvements in mobility are almost always possible, even in the most immobile older patients. Relatively small improvements in mobility can decrease the incidence and severity of complications, improve the patient's well-being, and make life easier for caregivers.
This chapter outlines the common causes and complications of immobility and reviews the principles of management for some of the more common conditions associated with immobility in the older population.
CAUSES
Many physical, psychological, and environmental factors can cause immobility in older persons (Table 10-1). The most common causes are musculoskeletal, neurological, and cardiovascular disorders. Pain is a common pathway by which these disorders result in immobility, and its management is highlighted in this chapter.
TABLE 10-1 COMMON CAUSES OF IMMOBILITY IN OLDER ADULTS | |
|---|---|
|
Degenerative joint disease (especially those involving the weight-bearing joints), osteoporosis, and hip fractures are probably the most prevalent conditions that predispose to immobility among older adults. Podiatric problems such as bunions, calluses, and onychomycoses frequently cause pain and reluctance or inability to walk.
The incidence of several neurological disorders that can cause immobility increases with age. About half of the individuals who suffer a stroke have residual deficits for which they require assistance; most of these deficits involve immobility. Parkinson's disease, especially in its later stages, causes severe limitations in mobility. Early and active management of these patients can improve their mobility and help to avoid complications.
Severe congestive heart failure, coronary artery disease with frequent angina, peripheral vascular disease with frequent claudication, and severe chronic lung disease can restrict activity and mobility in many elderly patients. Peripheral vascular disease, especially in older diabetics, can cause claudication, limit ambulation, and eventually result in lower extremity amputations, which can restrict mobility further.
P.246
Psychological and environmental factors can play an important role in immobility. Decreased mobility (i.e., taking to bed) is a common manifestation of depression. Fear of falling, especially among those with a history of instability and previous falls or with impaired vision, can lead to a bed-and-chair existence. Older patients with instability, impaired vision, and acute illnesses are often inappropriately restricted to bed or chair in acute care hospitals and nursing homes. Lack of mobility aids (e.g., canes, walkers, and appropriately
P.247
placed railings) also contributes to immobility in acute care hospitals and home settings.
Drug side effects may cause immobility. Sedatives and hypnotics, by causing drowsiness and ataxia, can impair mobility. Antipsychotic drugs (especially the phenothiazine-like agents) have prominent extrapyramidal effects and can cause muscle rigidity and diminished mobility (see Chap. 14).
COMPLICATIONS
Immobility can lead to complications in almost every major organ system (Table 10-2). Prolonged inactivity or bed rest has adverse physical and psychological consequences. Metabolic effects include negative nitrogen and calcium balance and impaired glucose tolerance; diminished plasma volume and altered drug pharmacokinetics can result. Immobilized older patients often become depressed, are deprived of environmental stimulation, and, in some instances, become delirious. Deconditioning can occur rapidly, especially among older people with little physiological reserve.
TABLE 10-2 COMPLICATIONS OF IMMOBILITY | |
|---|---|
|
The skin and musculoskeletal system often bear the brunt of immobility. Pressure sores are all too common. Muscle weakness, atrophy, and contractures can lead to prolonged disability and dysfunction. Bone density decreases in immobile patients, predisposing to fractures when the patient is mobilized. Cardiopulmonary complications of immobility are probably the most serious and life-threatening. Prolonged immobility results in cardiovascular deconditioning; the combination of deconditioned cardiovascular reflexes and diminished plasma volume can lead to postural hypotension. Postural hypotension may not only impair rehabilitative efforts but also predispose to falls and serious cardiovascular events such as stroke and myocardial infarction. Deep venous thrombosis and pulmonary embolism are well-known complications. Immobility, especially bed rest, also impairs pulmonary function. Tidal volume is diminished; atelectasis may occur, and, when combined with the supine position, predisposes to the development of aspiration pneumonia.
Gastrointestinal and genitourinary problems are among the most bothersome consequences of immobility to the patient and can lead to further complications. Immobility slows down both the gastrointestinal tract and urine flow. This predisposes to constipation, fecal impaction, urinary tract stones and infection, and fecal and urinary incontinence. These conditions and their management are discussed in Chap. 8.
ASSESSING IMMOBILE PATIENTS
Several aspects of the history and physical examination are important in the assessment of immobile patients (Table 10-3). Useful historical information includes the extent and duration of disabilities causing immobility, the underlying
P.248
P.249
medical conditions that influence mobility, and a review of medications in order to eliminate iatrogenic problems contributing to immobility. Pain should be routinely assessed as it may be a major contributing factor. Standardized pain assessment tools have been recommended for this purpose (AGS Panel on Persistent Pain in Older Persons, 2002). Psychological factors, such as depression and fear, may contribute to immobility and may make recovery difficult. They should, therefore, receive special attention. An assessment of the environment is important in determining measures that may improve the patient's mobility, such as an overhead triangle, bedside commode, railing, and other environmental manipulations.
TABLE 10-3 ASSESSMENT OF IMMOBILE OLDER PATIENTS | |
|---|---|
|
When immobile patients are being examined, the skin should be inspected repeatedly to identify early pressure sores. Cardiopulmonary status, especially intravascular volume, and postural changes in blood pressure and pulse are
P.250
important to the process of treatment. A detailed musculoskeletal examination including evaluation of muscle tone and strength and testing of joint range of motion and a search for potentially remediable podiatric problems should be carried out. Standardized and repeated measures of muscle strength can be helpful in gauging a patient's progress (Table 10-4). The neurological examination should identify focal weakness, as well as sensory and perceptual problems, that can impair mobility and frustrate rehabilitative efforts. Hemianopsia, or neglect of and inattention to one side of the body (usually the left side is ignored in patients with nondominant hemisphere lesions), and various apraxias are common after strokes.
TABLE 10-4 EXAMPLE OF A GRADING SYSTEM FOR MUSCLE STRENGTH IN IMMOBILE OLDER PATIENTS | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Most importantly, the patient's mobility should be assessed and reassessed on an ongoing basis. There are several levels of mobility (see Table 10-3) as well as important distinctions within each level. For example, a patient may be bed-bound but may be able to sit up without help, or the patient may be able to transfer independently into a wheelchair, but be unable to propel the wheelchair. Pain should also be assessed during mobility because patients may deny pain at rest but experience considerable pain with movement. Rehabilitation therapists are skilled in making these detailed evaluations of mobility and should be involved in the care of immobile patients.
MANAGEMENT OF IMMOBILITY
Optimal management of immobile older patients necessitates a thorough assessment, specific diagnoses, and multimodal treatment directed at specific diseases
P.251
and disabilities. This process generally involves a team of health professionals. Physical and occupational therapists can be especially helpful in the assessment and management of immobility and associated functional disabilities, and they should be consulted as early as possible when the problem of an immobile patient presents itself. In many patients, mobility cannot be completely restored and intensive rehabilitative efforts will not be cost-effective. Specific goals must be individualized, and in some patients these goals will involve preventing complications of immobility and adapting the environment to the individual (and vice versa).
It is beyond the scope of this text to detail the management of all conditions associated with immobility in older adults; important general principles of the management of some of the most common of these conditions are reviewed. Brief sections at the end of the chapter provide an overview of key principles in the management of pain and the rehabilitation of geriatric patients.
![]() Arthritis
Arthritis
Several different rheumatological disorders occur in the older persons. They can usually be distinguished from each other by clinical features, radiographic abnormalities, synovial fluid analysis, and selected laboratory studies (Table 10-5).
TABLE 10-5 CLINICAL ASPECTS OF COMMON RHEUMATOLOGICAL DISORDERS IN OLDER PATIENTS | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Specific diagnoses for these conditions should be made whenever possible, because the most appropriate treatment(s) of the primary disorders, as well as associated abnormalities, may differ. For example, polymyalgia rheumatica is a common condition in elderly women; its clinical features are often nonspecific fatigue, malaise, muscle aches. Because this disorder necessitates treatment with systemic steroids and is highly associated with temporal arteritis (a disease that can rapidly lead to blindness if appropriate treatment is not instituted), it is essential to make this diagnosis. Older patients with fatigue and symmetrical muscle aches (especially in the shoulders) should be tested for sedimentation rate, which will generally be markedly elevated (approximately 75 percent of patients have values greater than 40 mm/h in polymyalgia rheumatica [Goodwin, 1992]). Any symptoms suggestive of involvement of the temporal artery headache, jaw claudication, recent changes in vision especially when the sedimentation rate is very high (greater than 75 mm/h) should prompt consideration of temporal artery biopsy because treatment of temporal arteritis requires higher doses of steroids than does the treatment of polymyalgia alone. Patients with polymyalgia are generally treated with 10 to 20 mg of prednisone in a single dose, whereas patients with temporal arteritis are treated with 40 to 80 mg of prednisone daily in divided doses.
Another example of the importance of making a specific diagnosis is the carpal tunnel syndrome. This disorder may be overlooked when symptoms of pain, weakness, and paresthesias in the hand are mistaken for osteoarthritis.
P.252
P.253
Objective weakness, sensory deficit, and atrophy of intrinsic musculature of the hand should prompt consideration of performing nerve conduction studies and surgical therapy to relieve symptoms and prevent progressive disability. Wrist splints, generally provided by occupational therapists, are sometimes effective in relieving the discomfort of this syndrome.
The history and physical examination can be helpful in differentiating osteoarthritis from inflammatory arthritides (Table 10-6); however, other procedures are often essential. Osteoarthritis itself may be inflammatory in some instances.
TABLE 10-6 CLINICAL FEATURES OF OSTEOARTHRITIS VERSUS INFLAMMATORY ARTHRITIDES | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Synovial fluid analysis can be especially helpful in differentiating osteoarthritis from crystal-induced arthritides such as gout and pseudogout (Table 10-5). Because clinical examination alone cannot determine whether an inflamed joint is infected and joint infections can occur in conjunction with other inflammatory joint diseases, all newly inflamed joints should be tapped, Gram stained, and cultured to rule out infection. Failure to diagnose and treat joint infections can lead to osteomyelitis, joint destruction, and permanent disability.
In addition to making specific diagnoses of rheumatological disorders whenever possible, careful physical examination can detect treatable nonarticular conditions such as tendinitis and bursitis. For example, bicipital tendinitis and trochanteric bursitis are common in geriatric patients. Dramatic relief from pain and disability from these conditions can be achieved by local treatments such as the injection of steroids.
Osteoarthritis is by far the most common rheumatological disorder afflicting older adults. A wide variety of modalities can be used to treat osteoarthritis as well as other painful musculoskeletal conditions. Optimal management often involves the use of multiple treatment modalities, and the best combination of treatments will vary from patient to patient.
P.254
In general, patients with osteoarthritis and pain from inflammatory musculoskeletal conditions should be treated with an antiinflammatory agent unless they respond to local measures alone. Some older patients with chronic pain caused by osteoarthritis will respond to acetaminophen; however, when inflammation is present, nonsteroidal antiinflammatory drugs are generally appropriate. There are many such drugs; their side effects and prices vary. Nonsteroidal antiinflammatory drugs have several potential adverse effects in geriatric patients. Although the absolute risk of a significant gastrointestinal bleed may be small, monitoring of patients on chronic nonsteroidal therapy for bleeding with periodic hemoglobin levels and/or stools for occult blood is advisable. Nonsteroidal agents can also cause sodium retention and impair renal function, especially in patients with already compromised renal function and those on loop diuretics, may interfere with the efficacy of antihypertensive therapy, and are associated with hospitalization among patients with congestive heart failure. The cyclooxygenase (COX)-2 inhibitors may have fewer adverse effects than the older agents, but definitive data in the geriatric population are lacking. Combining lower doses of these drugs with acetaminophen can sometimes improve pain relief and minimize side effects. Guidelines for the management of pain in older persons have been published (AGS Panel on Persistent Pain in Older Persons, 2002) and are discussed below.
![]() Osteoporosis
Osteoporosis
Osteoporosis is a common disorder in the elderly and frequently leads to complications that result in pain, disability, and immobility. Approximately one third of women older than age 65 have suffered either a vertebral or hip fracture related to osteoporosis; by age 80, approximately half of women have evidence of vertebral fractures, and close to 30 percent will have suffered a hip fracture. Thus, osteoporosis is a major health problem in the older adult population, resulting in substantial morbidity and cost. The US Preventive Services Task Force now recommends routine screening for osteoporosis among women age 65 and older (Nelson et al., 2002). (See Chap. 5)
Osteoporosis is a generalized bone disorder in which bone mass is diminished but the relative composition (i.e., the ratio of mineral to organic matrix content) is not changed. This is in contrast to osteomalacia, in which the ratio of mineral to matrix is diminished. Aging is associated with a decrease in bone mass. White women lose the greatest proportion of bone mass with increasing age; the bone loss accelerates after menopause, and as much as 40 percent of bone mass may be lost by age 90. A working group of the World Health Organization has defined osteoporosis as a bone mineral density that is 2.5 SD (standard deviations) below the mean peak value in young adults. Values between 1.0 and 2.5 SD below the mean are defined as osteopenia.
P.255
Two major types of age-related osteoporosis have been defined (Table 10-7). Type I (postmenopausal) osteoporosis affects mainly trabecular bone and is related to accelerated bone loss in women during the first two decades after menopause. Type II (senile) osteoporosis affects both trabecular and cortical bone and is related to impaired production of 1,25-dihydroxy vitamin D. Several factors are associated with increased risk of osteoporosis among women (Table 10-8); many of them (e.g., gastric resection, steroid or anticonvulsant use, immobility) are also risk factors among men.
TABLE 10-7 TWO BASIC TYPES OF AGE-RELATED OSTEOPOROSIS | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
TABLE 10-8 FACTORS ASSOCIATED WITH AN INCREASED RISK OF OSTEOPOROSIS AMONG WOMEN* | ||
|---|---|---|
|
The most useful technique for measuring bone density is dual-energy x-ray absorptiometry (DEXA). It is helpful in making decisions for treatment when therapy might not otherwise be started, and in monitoring therapeutic response. Bone density of the hip is most helpful in predicting hip fractures, and bone density of the spine is helpful for monitoring therapy (Eastell, 1998).
Laboratory studies in uncomplicated osteoporosis should be normal, including serum calcium, phosphorus, magnesium, alkaline phosphatase, and parathyroid and thyroid hormones. Some older patients with senile osteoporosis have elevated parathyroid hormone, presumably related to a primary decrease in 1,25-dihydroxy vitamin D levels. Vitamin D blood levels and 24-hour urinary calcium excretion (which should be greater than 100 mg/24 h) should be measured if malabsorption is suspected.
The presenting manifestations of osteoporosis most often relate to a fracture of the hip (discussed below), the wrist (Colles fracture), or the lower thoracic and
P.256
upper lumbar vertebrae. Vertebral compression fractures can be asymptomatic and cause progressive kyphosis and loss of height. They may also be excruciatingly painful and be precipitated by relatively minor stress, such as sitting down quickly. The pain is exacerbated by twisting and increases in intraabdominal pressure (e.g., from coughing or straining to have a bowel movement). The pain can radiate around the thoracic cavity and mimic cardiac pain. Diagnosing a new compression fracture can be difficult, especially when old radiographs are not available. The combination of the new onset of characteristic pain and radiographic evidence of a compression fracture in a compatible location should be treated with bed rest (for as short a period as possible), heat, and analgesics. Posterior wedging of the fracture, fractures above the midthoracic vertebrae, and irregular-appearing vertebral bodies should raise the suspicion of a metastatic malignancy or plasmacytoma.
Several treatments are available for osteoporosis, including exercise, supplemental dietary calcium, vitamin D, bisphosphonates, fluoride, calcitonin, estrogen, and selective estrogen-receptor modulators (Eastell, 1998; Nelson et al., 2002). The most effective treatment for the different types of osteoporosis
P.257
remains somewhat controversial and is influenced by a number of patient-related factors. Preventive approaches are clearly the most effective; but to be effective in preventing fractures and associated morbidity later in life, treatment should be initiated soon after the menopause and continued for 10 to 20 years. Exercise probably has modest beneficial effects on bone mass and has other potential beneficial effects on muscle strength and agility (which may help prevent falls) and cardiovascular status. Thus, prescribing an exercise program suitable to the individual's preferences is certainly reasonable. Calcium supplementation of 1000 to 1500 mg/d is recommended as a preventive measure. Routine vitamin D supplementation of 400 to 800 IU per day is also recommended because it may help reduce the incidence of vertebral and hip fractures. Sodium fluoride can increase bone mass, particularly vertebral bone mass, but data on its effectiveness in preventing vertebral and hip fractures are conflicting. There is also a high incidence of gastrointestinal toxicity from fluoride, which is reduced with lower doses and simultaneous ingestion of calcium. Calcitonin therapy results in an increase in bone mineral density and a decrease in the rate of vertebral fractures, but it is expensive and can cause nausea, diarrhea, and flushing. Nasal calcitonin has fewer side effects, but has a small effect on reducing vertebral fractures in older women. Both forms of calcitonin have analgesic effects on bone pain of new vertebral fractures.
Bisphosphonate therapy results in increased bone mineral density and a decreased fracture rate. The two drugs commonly used in the United States are alendronate and risedronate. Both drugs have been shown, largely in industry sponsored trials, to prevent vertebral and nonvertebral fractures (Nelson et al., 2002; McClung et al., 2001; Harris et al., 1999). Both are available in daily and weekly dosages, and must be taken carefully (after an overnight fast with 6 to 8 ounces of water in an upright position) in order to avoid esophageal irritation.
Estrogen is also an effective treatment for preventing postmenopausal bone loss and subsequent fractures. Despite the benefits of estrogens, side effects and risks of its use must be considered in deciding whether to choose estrogen as therapy for osteoporosis in a postmenopausal woman. In women who are at high risk for osteoporosis (see Table 10-8) and who do not have a uterus, contraindications to estrogen treatment would be a history of breast cancer or recurrent thromboembolic disease. In women who have a uterus, the risk of endometrial cancer is reduced by the addition of a progestational agent to the estrogen. Cyclical estrogen-progestogen treatment can result in withdrawal bleeding, which some postmenopausal women may find unacceptable. Recent data suggest that combined estrogen-progesterone therapy is associated with an increase risk of cardiovascular events. These data make the decision about the use of postmenopausal estrogen even more complex.
The selective estrogen-receptor modulators (SERMs) have been developed to take advantage of estrogen's benefits and to minimize the side effects and risks. Raloxifene increases bone density without stimulating the endometrium. It also
P.258
decreases total and low-density lipoprotein cholesterol, but its effect on reducing ischemic heart disease is not known. In short-term studies, it is also reported to decrease the incidence of breast cancer. Its beneficial effect on bone density is less than that of estrogen, and studies on reduction of fractures are still ongoing. New SERMs may take greater advantage of estrogen's benefits and further lower the risks.
![]() Hip Fracture
Hip Fracture
Fractures of the hip and femoral neck, especially when associated with osteoporosis, are among the major causes of immobility, disability, and health care expenditures in older adults. Fear of hip fracture because of a prior fracture or its occurrence in a friend or relative is a common concern that contributes to limitation of mobility in many elderly persons. This fear is realistic: there are more than 250,000 hip fractures in the United States every year, with the incidence increasing dramatically with advanced age. The mortality rate in the year after hip fracture can be as high as 30 percent, and as many as one-third of hip fracture patients remain in a nursing home 1 year after the fracture. There is also a high rate of decline in ability to ambulate and perform activities of daily living in the 6 to 12 months after fracture. Thus, the prevention and optimal management of hip fractures are critical to the health of our older population. The assessment and management of falls, the major cause of hip fracture, is discussed in Chap. 9.
The degree of immobility and disability caused by a hip fracture depends on several factors, including coexisting medical conditions, patient motivation, the nature of the fracture, and the techniques of management. Many older patients with hip fracture already have impaired mobility, and there is a high incidence of medical illnesses that necessitate treatment (e.g., infection, heart failure, anemia, dehydration) at the time of hip fracture. Patients with these underlying conditions and those with dementia are at especially high risk for poor functional recovery. The location of the fracture is especially important in determining the most appropriate management and the outcome of treatment (Table 10-9 and Fig. 10-1). Subcapital fractures (which are inside the joint capsule) disrupt the blood supply to the proximal femoral head, thus resulting in a higher probability of necrosis of the femoral head and nonunion of the fracture. Replacement of the femoral head is often warranted in these cases. Inter- and subtrochanteric fractures generally do not disrupt the blood supply to the femoral head; open reduction and pinning are usually successful.
TABLE 10-9 CHARACTERISTICS OF SELECTED TREATMENTS FOR HIP FRACTURE | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
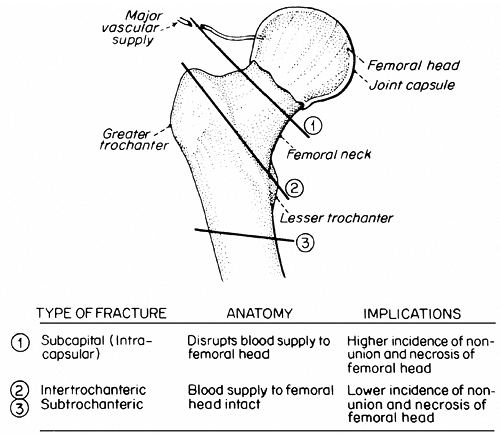 |
FIGURE 10-1 Characteristics of different types of hip fractures. |
In general, it takes 12 weeks for a hip fracture to heal. Surgical techniques such as a femoral head prosthesis and certain compression screws allow for almost immediate ambulation in many patients. Like almost all acute conditions in elderly patients, early mobilization is critical to the outcome. When combined with good rehabilitation and patient motivation, early mobilization can minimize disability and immobility from hip fracture. The current standard of care is for
P.259
patients to receive prophylactic anticoagulation to prevent thromboembolic complications. Subcutaneous injection of low-molecular-weight heparin is an effective method of prophylaxis in patients with hip fractures. Intermittent pneumatic compression is of value, but the equipment is costly and the need to apply and remove the device limits its usefulness. The long-term outcome of older patients with hip fracture depends on many factors besides the type of fracture and patient motivation. Many hip fracture patients have functional disabilities prior to the fracture, as well as active medical conditions at the time of the fracture, and they may suffer complications while in the acute care hospital. Intensive interdisciplinary rehabilitation programs may improve outcome in this patient population. Such programs should begin in the acute hospital and can be completed in subacute rehabilitation facilities, nursing homes, or at home.
![]() Parkinson's Disease
Parkinson's Disease
The first step in successful management of Parkinson's disease is to recognize its presence. Although many parkinsonian patients have the classic triad of resting tremor, rigidity, and bradykinesia, many others do not. Early in the disease, the symptoms and signs can be subtle and sometimes unilateral. Many elderly patients, especially in long-term care institutions, have undiagnosed and treatable forms of parkinsonism. Many patients have drug-induced parkinsonism resulting
P.260
from the extrapyramidal side effects of antipsychotics (see Chap. 14). Left untreated, parkinsonian patients eventually become immobile and can develop flexion contractures, pressure sores, malnutrition, and aspiration pneumonia.
Because Parkinson's disease often responds to treatment, especially early in its course, there should be a high index of suspicion for this diagnosis. Patients with more advanced Parkinson's disease frequently appear depressed or demented (sometimes both); in fact, many parkinsonian patients become depressed and develop cognitive dysfunction. Experienced neurologists or psychiatrists should be consulted when the diagnosis is in question and when the clinical picture is complicated by dementia and/or depression.
Pharmacological treatment of Parkinson's disease is based on an attempt to increase the ratio of dopamine to acetylcholine in the central nervous system, specifically the nigrostriatal system. Several drugs can be used, sometimes in combination (Table 10-10). Carbidopa/levodopa remains the mainstay of therapy. All of the antiparkinsonian drugs must be used carefully; treatment should begin with small doses that are gradually increased. Clinical response may take several weeks. Side effects are common and often limit pharmacological treatment. Wide
P.261
variations in response can also occur, including morning akinesia, peak dose dyskinesias, and freezing episodes (sometimes referred to as the on off phenomenon ). Excessive dopamine can also cause sleep disturbances, delirium, and psychosis. These patients may require hospitalization to determine the cause(s) of their symptoms and readjustment of therapy.
TABLE 10-10 DRUGS USED TO TREAT PARKINSON'S DISEASE | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Patients who are difficult to manage or who do not respond should be referred to an experienced neurologist. Some of these patients may benefit from neurosurgical procedures, such as deep brain stimulation. Parkinsonian patients with more advanced disease will also benefit from rehabilitation therapy and an ongoing program of exercise and activity in order to maintain strength and functional capabilities and to prevent complications of immobility.
![]() Stroke
Stroke
To prevent disability from immobility and its complications, patients with completed strokes should receive prompt and intensive rehabilitative therapy. In many elderly patients, coexisting medical conditions (e.g., cardiovascular disease) limit the intensity of rehabilitation treatment that can be tolerated in order to qualify for Medicare coverage in an inpatient or skilled nursing facility. However, all patients should be evaluated and managed as actively as possible during the first several weeks after a stroke. Although all stroke patients deserve an assessment and consideration for intensive rehabilitation, the cost-effectiveness of various approaches to stroke rehabilitation is controversial. Whether the rehabilitative efforts occur in the acute care hospital, special rehabilitation unit, nursing home, or at home these efforts should involve a multidisciplinary rehabilitation team, and the basic principles remain the same (see Rehabilitation below).
Despite the lack of data from controlled trials, even some of the most severely affected stroke patients can achieve meaningful improvements in functional status by early rehabilitative efforts. Although complete functional recovery occurs in less than half of stroke patients, immobility and its attendant complications can almost always be prevented or minimized. Development of realistic goals for individual patients is essential. Intensive efforts directed at functional recovery are probably not appropriate for patients with large or bilateral strokes causing flaccid paralysis or severe perceptual deficits or for patients with severe underlying medical conditions or dementia. The goals in these latter patients should be to prevent complications and adapt the environment. The management of older patients with cerebrovascular disease is discussed further in Chap. 11.
![]() Pressure Ulcers
Pressure Ulcers
Pressure ulcers are among the most preventable and treatable conditions associated with immobility in older adults. Four factors contribute to the development
P.262
P.263
P.264
of pressure sores: pressure, shearing forces, friction, and moisture. As the name implies, pressure ulcers develop because areas of the body (most often overlying bony prominences) are exposed to prolonged pressure. The amount of pressure necessary to occlude blood supply to the skin (and thus predispose to irreversible tissue damage) is small and is generated in normal sitting and supine positions. Irreversible tissue damage can occur (especially in aging skin) after only 2 hours of continuous pressure that exceeds capillary pressure.
Shearing forces (such as those created when the head of a bed is elevated and the torso slides down and transmits pressure to the sacral area) contribute to the stretching and angulation of subcutaneous tissues. Friction, caused by the repeated movement of skin across surfaces such as bed sheets or clothing, increases the shearing force. This can eventually lead to thrombosis of small blood vessels, thus undermining and then destroying skin. Shearing forces and friction are worsened by loose, folded skin, which is common in the elderly because of loss of subcutaneous tissue and/or dehydration. Moisture from bathing, sweat, urine, and feces compounds the damage. Other risk factors for pressure ulcers include those that exacerbate oxygen transport (e.g., anemia) or impede healing (e.g., malnutrition) (Bergstrom and Braden, 1992). Hospitalized patients with fractures, fecal incontinence, and hypoalbuminemia are at especially high risk (Allman et al., 1986). The Agency for Health Care Policy and Research (AHCPR, now the Agency for Healthcare Research and Quality) has published clinical practice guidelines for the prevention of pressure ulcers (AHCPR, 1992).
Pressure ulcers can be classified into four stages, depending on their clinical appearance and extent (Table 10-11). The area of damage below the pressure ulcer can be much larger than the ulcer itself. This is caused by the manner in which pressure and shearing forces are transmitted to subcutaneous tissues. More than 90 percent of pressure ulcer occur in the lower body mainly in the sacral and coccygeal areas, at the ischial tuberosities, and in the greater trochanter area.
TABLE 10-11 CLINICAL CHARACTERISTICS OF PRESSURE SORES | |
|---|---|
|
The cornerstone of management of the skin in immobile patients is prevention of pressure ulcers (Table 10-12). Once a stage I or II pressure ulcer develops, all preventive measures listed in Table 10-12 should be used to avoid progression of the ulcer, and intensive local skin care must be instituted. Many techniques have been advocated for local skin care; none is more successful than the others. The most important factor in all these techniques is the attention (and thus the relief from pressure) that the skin gets. Almost any technique that involves removing pressure from the area and regularly cleansing and drying the skin will work.
TABLE 10-12 PRINCIPLES OF SKIN CARE IN IMMOBILE OLDER PATIENTS | |||
|---|---|---|---|
|
The management of stages III and IV pressure ulcers is more complicated. D bridement of necrotic tissue and frequent irrigation (two to three times daily), cleansing (with saline or peroxide), and dressing of the wound are essential. Eschars should be undermined and removed if they are suspected of hiding large amounts of necrotic and infected tissue. Chemical d briding agents can be helpful. The role of wound cultures and antimicrobials in the management of stage III pressure ulcers is controversial. Topical antimicrobials may be useful, especially
P.265
when bacterial colony counts are high, but they are generally not recommended. Systemic antimicrobials should not be used because they do not reach sufficient concentrations in the area of the ulcer; topical therapy will be more effective unless cellulitis is present. Routine wound cultures are probably not warranted for stage III lesions because they almost always grow several different organisms and do not detect anaerobic bacteria, which are often pathogenic. Results of such cultures generally reflect colonization rather than infection. Once a lesion has progressed to stage IV, systemic antimicrobials are often necessary. Routine and anaerobic cultures of tissue or bone are most helpful in directing antimicrobial therapy. Patients with large pressure ulcers who become septic should be treated with broad-spectrum antimicrobials that will cover anaerobes, gram-negative organisms, and Staphylococcus aureus. In selected instances, consideration of plastic surgery for stage IV lesions is warranted. Air-fluidized and low-air-loss beds are being used with increasing frequency for the management of patients with stage III and IV pressure ulcers, as well as to prevent deep ulcers in high-risk patients. Although these beds are expensive, they may be helpful in accelerating the healing of pressure ulcers in selected patients in hospital and nursing home settings (Allman et al., 1987; Ferrell et al., 1992).
P.266
PAIN MANAGEMENT
Pain is a major factor in causing immobility in older adults. Immobility, in turn, can exacerbate painful conditions and create a vicious cycle of pain, decreased mobility, and worsened pain. The American Geriatrics Society has published recommendations of an expert panel for the management of persistent pain in older adults, and readers are referred to this publication for more details (AGS Panel on Persistent Pain in Older Persons, 2002). Pain is also discussed in Chap. 3 of this text.
Pain in older persons is commonly underdiagnosed and undertreated despite the availability of many effective therapeutic interventions. Pain is now viewed as a fifth vital sign, and acute hospital staff and other health professionals are increasingly routinely inquiring about pain. When pain is identified, it should be carefully characterized. In addition to the standard questions about location, timing,
P.267
aggravating factors, and the like, a simple standardized pain scale can be helpful in rating the severity of pain and following response to therapy. Several such scales are available (AGS Panel on Persistent Pain in Older Persons, 2002; see Chap. 3). The degree to which pain interferes with activities of daily living and sleep is especially important to explore. Recurrent or persistent pain can result in complications such as a predisposition to falling (as a consequence of musculoskeletal pain that occurs with specific movements), depression, and the use of expensive and unproven treatments for poorly managed pain. Pain may be difficult to assess in patients with moderate or advanced dementia. In this patient population, caregivers must be observant for more subtle clues to the presence of pain, such as facial expressions and changes in activities, behavior, or mental status.
Pain is generally best treated when a specific cause for the pain is identified. A careful physical examination can supplement the history in order to help pinpoint the source(s) of pain. In many situations, however, such as visceral pain, back pain, and referred pain, the cause may not be clear. In these situations careful consideration must be given to the use of selected diagnostic tests and imaging to make a specific diagnosis. The decision about whether to pursue expensive and potentially uncomfortable diagnostic procedures, such as magnetic resonance imaging and nerve conduction studies, must be individualized, weighing the potential risks and costs versus the importance of identifying the precise etiology of the pain.
Pain management usually includes both nonpharmacological and pharmacological approaches. The former include patient and caregiver education, a program of physical activity to help avoid disability from immobility, and a variety of therapeutic modalities including heat, ice, stretching, massage, ultrasonography, acupuncture and other techniques. A regular program of exercise is recommended for older patients with pain related to osteoarthritis (American Geriatrics Society Panel on Exercise and Osteoarthritis, 2001). Physical therapists should be involved in these nonpharmacological management techniques. Local injections to trigger points or joint space injections of steroids under fluoroscopy can provide dramatic relief from pain in some patients. Topical application of capsaicin, lidocaine, and other local analgesics is sometime helpful for brief periods.
The mainstay of pain management is drug therapy. Table 10-13 lists drugs that can be helpful in managing pain in older adults. For persistent pain, most experts recommend initiating treatment with acetaminophen. The chronic use of nonsteroidal antiinflammatory agents (NSAIDs) and COX-2 inhibitors can be very effective, but there are risks of these drugs with long-term use. The higher costs of the COX-2 inhibitors must be weighed against their benefits. Older patients with renal insufficiency and/or congestive heart failure are especially vulnerable to the effects of NSAIDs and COX-2 inhibitors on the kidney and fluid retention. Acetaminophen or an NSAID with an opioid can be helpful for episodic and breakthrough type pain. Severe persistent pain often requires opioid therapy, which can be given alone or in combination with one of a number of adjuvant drugs (see Table 10-13). There are many subtleties in
P.268
P.269
P.270
P.271
the effective drug treatment of pain and the avoidance of bothersome and potentially dangerous complications. The reader is referred to the AGS recommendations as well as other more comprehensive textbooks for more specific information on pain management.
TABLE 10-13 DRUG THERAPY FOR PAIN MANAGEMENT | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
EXERCISE
Exercise is a critical intervention for preventing immobility and its complications, and is also discussed in Chapter 5 of this text. The development of musculoskeletal disability with age frequently decreases quality of life. Musculoskeletal disability among older adults is commonly linked to osteoarthritis, deconditioning, soft-tissue changes, and other chronic diseases. Smoking, body mass index, and exercise patterns in midlife and late adulthood are predictors of subsequent disability (Vita et al., 1998). Persons with better health habits not only survive longer but their disability is postponed. In a longitudinal study, older persons who engaged in vigorous running had slower development of disability than the general population (Fries et al., 1994). Maximal cardiac output and aerobic exercise capacity decline with advancing age and physical inactivity. Endurance exercise training induces adaptations that can counteract some of the deleterious effects of aging, including an increase in maximal oxygen uptake and enhancement of cardiac function. Another potential benefit of exercise is maintenance of the bone mineral density of the lumbar spine in postmenopausal women (Kelley, 1998).
Strength training also is feasible and effective in both community-dwelling older adults and in frail nursing home residents (Ades et al., 1996; Fiatarone et al., 1994; Hunter et al., 1995). Training improves strength, walking endurance, and ability to carry out daily tasks. Many studies have demonstrated that exercise programs, both for endurance and strength, can be initiated in older adults with safety and with resultant benefit in delaying disability and improving function (American Geriatrics Society Panel on Exercise and Osteoarthritis, 2001). Walking is cheap and safe, and strength training can be done with inexpensive devices. The program should be tailored with specific goals for the exercise and outcomes.
REHABILITATION
The goal of rehabilitation is to restore function and prevent further disability. It is therefore a core element of geriatric practice, especially for immobile elderly patients, and usually necessitates a team effort. Physiatrists can be very helpful in developing appropriate and optimal rehabilitation plans for geriatric patients with complicated rehabilitation needs. It is beyond the scope of this text to provide a detailed discussion of rehabilitation in the older adult. Table 10-14
P.272
outlines some of the key principles. Careful assessment of a patient's function, the setting of realistic goals, prevention of secondary disabilities and complications of immobility, repeated measures of functional abilities that are relevant to the patient's environment, and adapting the environment to the patients' abilities (and vice versa) are all essential elements of the rehabilitation process.
TABLE 10-14 BASIC PRINCIPLES OF REHABILITATION IN OLDER PATIENTS | |
|---|---|
|
Physical and occupational therapists can be extremely valuable in assessing, treating, motivating, and monitoring patients whose mobility is impaired. Physical therapists generally attend to the relief of pain, muscle strength and endurance, joint range of motion, and gait. They use a variety of treatment modalities (Table 10-15). Occupational therapists focus on functional abilities, especially as they relate to activities of daily living. They make detailed assessments of mobility and help patients improve or adapt to their abilities to perform basic and instrumental activities of daily living. Even when mobility and function remain impaired, occupational therapists can make life easier for these patients by performing environmental assessments and recommending modifications and assistive devices that will improve the patient's ability to function independently (Table 10-16). Speech therapists are helpful in assessing and implementing rehabilitation for disorders of communication and swallowing.
TABLE 10-15 PHYSICAL THERAPY IN THE MANAGEMENT OF IMMOBILE OLDER PATIENTS | |
|---|---|
|
TABLE 10-16 OCCUPATIONAL THERAPY IN THE MANAGEMNET OF IMMORBILE OLDER PATIENTS | |
|---|---|
|
Although these basic principles of geriatric rehabilitation are essential in providing optimal care for the growing populations of geriatric patients who may need rehabilitation, the cost-effectiveness of various approaches to rehabilitation in the elderly remains controversial. Most of the data on the effectiveness of rehabilitation for older adults come from studies of geriatric assessment units, where
P.273
short-term rehabilitation is a major component of the intervention. Most geriatric assessment units described to date have been in either acute care hospitals or ambulatory settings. The effectiveness of such units was summarized in Chap. 3. It is clear that targeting rehabilitative efforts to patients who are most likely to benefit is critical to cost-effectiveness. The decision to admit an older patient to a specialized inpatient acute rehabilitation or stroke unit as opposed to a skilled nursing facility depends on many factors including the patient's potential for benefit and ability to tolerate intensive therapy, as well as the nature and extent of medical comorbidities. More data are needed to accurately predict which geriatric patients will benefit most from specific types of rehabilitative efforts. Until these data are available, geriatricians should work closely with experienced rehabilitation therapists in setting realistic and individualized goals for their patients. The goals should be compatible with the patients' preferences and socioeconomic environment, and should be directed toward the maximum functional outcome realistic for that patient. Ongoing assessment of progress and the prevention of medical and psychological complications are also fundamental to the rehabilitative process.
P.274
References
Ades PA, Ballor DL, Ashikaga T, et al: Weight training improves walking endurance in healthy elderly persons. Ann Intern Med 124:568 572, 1996.
AGS Panel on Persistent Pain in Older Persons: The management of persistent pain in older persons. J Am Geriatr Soc 50:S205 S224, 2002.
AHCPR: Pressure Ulcers in Adults: Prediction and Prevention. AHCPR Publication No. 92 0047. Rockville, MD, Agency for Health Care Policy and Research, 1992.
Allman RM, Laprade CA, Noel LB, et al: Pressure sores among hospitalized patients. Ann Intern Med 105:337 342, 1986.
Allman RM, Walker JM, Hart MK, et al: Air-fluidized beds or conventional therapy for pressure sores: a randomized trial. Ann Intern Med 107:641 648, 1987.
P.275
American Geriatrics Society Panel on Exercise and Osteoarthritis: Exercise prescription for older adults with osteoarthritis pain: consensus practice recommendations. A supplement to the AGS Clinical Practice Guidelines on the management of chronic pain in older adults. J Am Geriatr Soc 49:808 823, 2001.
Bergstrom N, Braden B: A prospective study of pressure sore risk among institutionalized elderly. J Am Geriatr Soc 40:747 758, 1992.
Eastell R: Treatment of postmenopausal osteoporosis. N Engl J Med 338:736 746, 1998.
Ferrell BA, Osterweil D, Christenson P: A randomized trial of low-air-loss beds for treatment of pressure ulcers. JAMA 269:494 497, 1992.
Fiatarone MA, O'Neill EF, Ryan ND, et al: Exercise training and nutritional supplementation for physical frailty in very elderly people. N Engl J Med 330:1769 1775, 1994.
Fries JF, Singh G, Morfeld D, et al: Running and the development of disability with age. Ann Intern Med 121:502 509, 1994.
Goodwin JS: Progress in gerontology: polymyalgia rheumatica and temporal arteritis. J Am Geriatr Soc 40:515 525, 1992.
Harris ST, Watts NB, Genant HK, et al: Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis. JAMA 282:1344 1352, 1999.
Hunter GR, Treuth MS, Weinsier RL, et al: The effects of strength conditioning on older women's ability to perform daily tasks. J Am Geriatr Soc 43:756 760, 1995.
Kelley G: Aerobic exercise and lumbar spine bone mineral density in postmenopausal women: a meta-analysis. J Am Geriatr Soc 46:143 152, 1998.
McClung MR, Geusens P, Miller PD, et al: Effect of risedronate on the risk of hip fracture in elderly women. N Engl J Med 344:333 340, 2001.
Nelson HD, Helfand M, Woolf SH, et al: Screening for postmenopausal osteoporosis: a review of the evidence for the US Preventive Services Task Force. Ann Intern Med 137:529 541, 2002.
Reich ML: Arthritis: avoiding diagnostic pitfalls. Geriatrics 37:46 54, 1982.
Riggs BL, Melton JL: Involutional osteoporosis. N Engl J Med 314:1676 1684, 1986.
Vita AJ, Terry RB, Hubert HB, Fries JF: Aging, health risks, and cumulative disability. N Engl J Med 338:1035 1041, 1998.
Suggested Readings
Immobility, General
Gill TM, Desai MM, Gahbauer EA, et al: Restricted activity among community-living older persons: incidence, precipitants, and health care utilization. Ann Intern Med 135:313 321, 2001.
Harper CM, Lyles YM: Physiology and complications of bed rest. J Am Geriatr Soc 36:1047 1054, 1988.
P.276
Musculoskeletal Disorders
Borenstein DG, Burton JR: Lumbar spine disease in the elderly. J Am Geriatr Soc 41:167 175, 1993.
Felson DT, Lawrence RC, Dieppe PA, et al: Osteoarthritis: new insights. Part I: the disease and its risk factors. Ann Intern Med 133:635 646, 2000.
Felson DT, Lawrence RC, Hochberg MC, et al: Osteoarthritis: new insights. Part II: treatment approaches. Ann Intern Med 133:726 737, 2000.
Osteoporosis and Hip Fracture
Cummings SR, Bates D, Black DM: Clinical use of bone densitometry. JAMA 288:1889 1897, 2002.
Hannan EL, Magaziner J, Wang JJ, et al: Mortality and locomotion 6 months after hospitalization for hip fracture: risk factors and risk-adjusted hospital outcomes. JAMA 285:2736 2742, 2001.
Kannus P, Parkkari J, Niemi S, et al: Prevention of hip fracture in elderly people with use of a hip protector. N Engl J Med 343:1506 1513, 2000.
Marottoli RA, Berkman LF, Leo-Summers L, Cooney LM Jr: Predictors of mortality and institutionalization after hip fracture: the New Haven EPESE cohort. Am J Public Health 84:1807 1812, 1994.
NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy: Osteoporosis prevention, diagnosis, and therapy. JAMA 285:785 795, 2001.
US Preventive Services Task Force: Screening for osteoporosis in postmenopausal women: recommendations and rationale. Ann Intern Med 137:526 528, 2002.
Zuckerman JD: Hip fracture. N Engl J Med 334:1519 1525, 1996.
Parkinson's Disease
Lang AE, Lozano AM: Parkinson's disease: first of two parts. N Engl J Med 339:1044 1053, 1998.
Lang AE, Lozano AM: Parkinson's disease: second of two parts. N Engl J Med 339:1130 1143, 1998.
Pressure Ulcers
Agency for Health Care Policy and Research, Panel for the Prediction and Prevention of Pressure Ulcers in Adults: Pressure Ulcers in Adults: Prediction and Prevention. Clinical Practice Guideline, Number 3, AHCPR Publication No. 92 0047. Rockville, MD, ACPHR, May 1992.
Ouslander JG, Osterweil D, Morley J: Medical Care in the Nursing Home. New York, McGraw-Hill, 1991, pp 147 164.
P.277
Rehabilitation
Gill TM, Baker DI, Gottschalk M, et al: A program to prevent functional decline in physically frail, elderly persons who live at home. N Engl J Med 347:1068 1074, 2002.
Hoenig H, Nusbaum N, Brummel-Smith K: Geriatric rehabilitation: state of the art. J Am Geriatr Soc 45:1371 1381, 1997.
Wasson JH, Gall V, McDonald R, Liang MH: The prescription of assistive devices for the elderly: practical considerations. J Gen Intern Med 5:46 54, 1990.
Stroke
Brott T, Bogousslavsky J: Treatment of acute ischemic stroke. N Engl J Med 343:710 722, 2000.
Straus SE, Majumdar SR, McAlister FA: New evidence for stroke prevention. JAMA 288:1388 1395, 2002.
EAN: 2147483647
Pages: 23
- Article 220 Branch-Circuit, Feeder, and Service Calculations
- Article 500 Hazardous (Classified) Locations, Classes I, II, and III, Divisions 1 and 2
- Example No. D4(b) Optional Calculation for Multifamily Dwelling
- Example No. D6 Maximum Demand for Range Loads
- Example No. D10 Feeder Ampacity Determination for Adjustable-Speed Drive Control [See 215.2, 430.24, 620.13, 620.14, 620.61, Tables 430.22(E), and 620.14]