8 - Smoking and Cognitive Function: Issues in Cognitive Rehabilitation
Editors: Backman, Lars; Hill, Robert D.; Neely, Anna Stigsdotter
Title: Cognitive Rehabilitation in Old Age, 1st Edition
Copyright 2000 Oxford University Press
> Table of Contents > Part IV - Rehabilitation Strategies for Cognitive Loss in Age-Related Disease > 12 - Retrieval Strategies as a Rehabilitation Aid for Cognitive Loss in Pathological Aging
function show_scrollbar() {}
12
Retrieval Strategies as a Rehabilitation Aid for Cognitive Loss in Pathological Aging
Cameron J. Camp
Michael J. Bird
Katie E. Cherry
Research on memory interventions for persons with dementia and other cognitive impairments is rapidly expanding, as the existence of this volume testifies. In this chapter, we will describe the use of active retrieval strategies as an aid in cognitive rehabilitation for pathological aging. More than 20 years have passed since the original research on which this chapter is based was published. In the late 1970s, Landauer and Bjork (1978) described a technique designed to allow new information, such as the name of a person in a photograph, to be learned efficiently. They called this phenomenon spaced retrieval (SR). Their study was published as a book chapter part of the proceedings of the first Practical Aspects of Memory conference held in the United Kingdom. Today, SR is being implemented as a rehabilitation aid for cognitive loss associated with an increasingly diverse set of pathologies found in older adults. The SR technique described by Landauer and Bjork has been shown to allow persons with profound memory deficits characteristic of dementia to be able to learn new information and successfully recall it across clinically meaningful periods of time (days, weeks, months). Interventions using this approach, in combination with other techniques, can alleviate behavioral problems associated with dementia in real-world settings. Use of SR by therapists in different disciplines has recently been noted.
We will attempt to provide a historical background for the development of SR, including a brief review of early research utilizing SR as a memory intervention for persons with memory deficits. We focus primarily on research involving persons with dementia. We describe how the methods of applying SR as an intervention have evolved and are evolving. We then focus on two major topics: recent clinical applications of SR and recent efforts to determine the theoretical basis for effects produced by SR. We conclude the chapter with a case study and summary comments.
P.225
Historical Background
Landauer and Bjork's findings concerning SR were reported within the context of a movement within cognitive psychology: a drive to conduct research that would be more ecologically valid, addressing issues of everyday memory rather than lab-based phenomena. This movement has generated controversy regarding the efficacy of everyday memory research (see Baddeley, 1989; Banaji & Crowder, 1989, 1991; Landauer, 1989; Mook, 1989; Petrinovich, 1989; Tulving, 1991). Their study, in a sense, represented a bridging action. Their data were collected from a group of undergraduates in a university setting, but their findings had potential for application across a number of areas that could be explored by future investigators.
The Original Study
Landauer and Bjork's study (1978) was based on a line of research begun in the 1960s concerning the spacing effect. In essence, the spacing effect is the phenomenon in which spaced practice for learning and recalling new information results in better long-term retention than massed practice (see Landauer, 1989, for a description of the origins of spacing-effect research). Landauer and Bjork were interested in determining if one type of spacing schedule might be optimal for learning new information. Their results suggested that recall of information at successively longer intervals produced better long-term retention of new information than other schedules of recall practice. Though other schedules also produced good recall performance, such as multiple recall trials at fixed intervals, their data indicated that the expanding schedule worked best as a potential mnemonic intervention. They called their optimal technique spaced retrieval.
It is informative to note the aspects of SR as originally implemented. Information about a person in a photograph, such as his or her name, was presented along with the photo. Then, a number of other photos were interspersed between this original presentation and later presentations of the target photo. For example, the initial photo might be shown, followed by a second photo and then another presentation of the original photograph. At this latter presentation of the target photo, recall of the name or other information presented at initial presentation of the photo was attempted. The number of photos interspersed between the original presentation of the target and latter presentations kept expanding in the SR condition. For example, Figure 12.1 shows a representation of a 1:5:10 expanding recall, or SR, schedule.
At the next Practical Aspects of Memory conference held about a decade later, Bjork (1988) described SR as a shaping technique applied to memory. Successful recall trials in this context represented closer and closer approximations to a desired goal, that is, retention and recallability of new information over time periods such as days or months or years. This reference to behavioral technology within the context of cognitive research is important, for it represents the acknowledgment that an eclectic approach to understanding cognitive phenomena and implementing potential interventions is both desirable and necessary. This approach to cognitive rehabilitation, which developed in the UK, has been clearly and forcefully described and contrasted with alternative approaches to cognitive rehabilitation, by Wilson (1997).
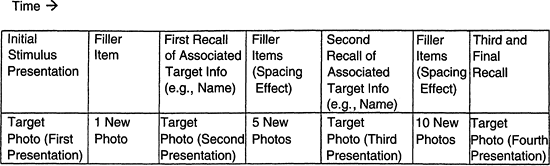 |
Figure 12.1. Example of an expanded recall schedule. |
P.226
First Uses of SR as a Rehabilitative Technique
Several years after the initial SR study, Dan Schacter and his colleagues (Schacter, Rich, & Stampp, 1985) described the use of SR as a cognitive intervention using a small sample of adults with a variety of etiologies and cognitive deficits. They used a procedure similar to that employed by Landauer and Bjork to create SR schedules (i.e., interspersing varying numbers of filler items between an initial target presentation and latter presentations of the target). Schacter's group found that persons with memory impairment could learn new information using SR, though attempts to train participants to spontaneously use a form of SR themselves when confronted with new information were not successful. They also reported that learning via SR appeared to be accomplished with relatively little expenditure of cognitive effort.
Several important points are exemplified in Schacter's use of SR as an aid to cognitive rehabilitation. First, this study was conducted within the context of a series of studies by Glisky and Schacter and their colleagues on cognitive remediation techniques designed to access implicit memory, which was assumed to be relatively spared in amnestic patients (see Glisky & Schacter, 1986, 1987; Glisky, Schacter, & Tulving, 1986; Schacter, 1992, 1994; Schacter & Tulving, 1994). Thus, the reference to cognitive effort is important. Since implicit memory is assumed to utilize relatively unconscious and automatic processes (i.e., those that should require little cognitive effort), a case was being made that SR might be accessing some aspect of implicit memory. Though the argument was based on rather anecdotal accounts of how effortful the SR procedure was to research participants, these accounts were seen as indirect evidence linking SR and implicit memory. In addition, Schacter's work had extended to the use of behavioral technologies such as fading cues as interventions for cognitive deficits (Glisky et al., 1986). These studies emphasized the need for eclectic approaches to designing cognitive rehabilitation aids, and they introduced the concepts of (low) cognitive effort and implicit memory in relation to the SR technique. Glisky and Schacter also emphasized the need to focus on training for retention of specific information rather than attempting to improve memory per se (see also Glisky & Schacter, 1986, 1987).
Moffat (1989) described the use of SR, which he referred to as expanding rehearsal, to rehabilitate a man in his late 60s who had suffered cerebral anoxia as a result of a myocardial infarction. The targeted problem was his severe dysgraphia for
P.227
letters and numbers. Moffat's study marked several important new features made available for the clinical use of SR as a rehabilitative technique. The target behavior was determined by the client, who was highly motivated to use the intervention. This intervention was implemented in a home setting, primarily by the client and the client's wife. Expanding intervals were determined by time periods rather than through interposing additional experimental stimuli. The retrieval schedule extended across hours and a large number of target stimuli. Learning acquired through SR was maintained through routinized practice schedules, and SR was implemented with a motor behavior rather than a verbal behavior.
Use of SR as an Intervention for Persons with Dementia
Moffat (1989) also described a case in which a woman diagnosed with Alzheimer's disease (AD) was trained using SR to relearn the names of objects. Impairment in naming ability is a common feature of dementia associated with AD and related disorders and is a source of frustration for those with this condition. Moffat set up a training regimen in the client's home, conducted by a nurse's aide. Names of 20 items displayed as pictures were targeted for training. At baseline, the client could not retain the name of any targeted item for any substantial length of time. Training for remembering the names of 20 common items involved giving her the name of a target item, checking its retention after a 2-minute interval, and then doubling the next recall interval after successful recall attempts and halving recall intervals after unsuccessful recall attempts. Again, here we see a shaping technology being applied to a cognitive ability. After an item was trained to a criterion level of recall, another item was initiated in an SR training sequence. Probed recall of all items was used every 2 weeks.
Several features of this case study add important information about SR. Moffat noted that the numbers of errors made for trained items and their latencies of response grew smaller across training sessions. The first few words, once learned to criterion, were always recalled immediately. These findings indicate that SR appears to be enabling learning to take place for trained stimuli, and that improvement in recall ability with practice is available for persons with AD via SR training.
Also, by the third session, only three words had been taught, but the majority of the 20 pictures were named accurately on the probe test. This finding poses some interesting questions. Does this finding mean that SR training produces a generalization of training effects (i.e., does the general ability to name objects improve after exposure to SR training for specific stimuli)? Alternatively, does the sheer act of giving practice at attempting recall as was done in the probe tests (especially if feedback is provided for failed attempts, but perhaps even if not) constitute an alternative SR schedule and result in enhanced recallability of probed items?
Landauer and Bjork (1978) tested several alternative recall intervals, of which expanding rehearsal was only one (but the most successful). Alternative spacing schedules can also be effective at enhancing recall (e.g., Foss, 1994; Landauer & Bjork, 1978). What if probes to determine whether nontrained items can be recalled constitute an alternative form of SR training or, at the very least, increase likelihood of recall over multiple probe sessions? If such is the case, this result creates challenges
P.228
to researchers seeking to create control conditions for determining the efficacy of the SR intervention as a rehabilitation technique.
Further Use of SR for Persons with Dementia: Camp's Research
Camp and his colleagues (Abrahams & Camp, 1993; Brush & Camp, 1998, in press; Camp, 1989, 1996; Camp & Foss, 1997; Camp & Schaller, 1989; Camp & Stevens, 1990; Camp et al., 1993, 1996a, 1996b; Hayden & Camp, 1995; McKitrick, 1993; McKitrick & Camp, 1993; McKitrick, Camp, & Black, 1992; Stevens, O'Hanlon, & Camp, 1993) also began using SR as an intervention for persons with dementia, using a free recall format. In initial pilot studies, he found that the expanding interval schedule used by Moffat (i.e., doubling the previous recall interval) was producing high error rates. Instead, he switched to the use of a more gradual recall interval expansion rate: 5 sec, 10 sec, 20 sec, 40 sec, 60 sec, 90 sec, 120 sec, and so on, in which intervals were increased by 30 sec once a 60-sec successful recall interval had been attained. A participant who failed in an attempt at recall was provided the answer and immediately asked to recall it. The next recall interval was shortened to that of the last successful recall interval.
This schedule was used in a number of studies in which persons with dementia were trained to remember names of persons or objects, locations of objects, motor activities, and even a strategy (remembering to look at a calendar to learn about daily appointments and other personally relevant information). A portable computer, in most instances, was used to record recall successes and failures and controlled the timing of recall intervals. A musical cue informed researchers when to institute the next recall trial. Use of this schedule was somewhat serendipitous, since Camp's initial pilot participants were more advanced in their dementia than the person trained by Moffat. Still, this approach proved successful across a variety of both levels of dementia, as assessed by measures such as the Mini-Mental State Exam (MMSE), and types of dementia.
One important finding in this research was that if participants with dementia were able to successfully recall information over a critical recall interval, perhaps 6 8 min, they could retain information across training sessions (Camp et al., 1996b). In other words, if persons with dementia could be trained by SR to retain new information across a critical interval within a training session, that information seemed to be consolidated into long-term memory and could be recalled across days. Though other researchers have reported that a longer retention interval (15 minutes or 1 hour) is required to predict long-term retention (see Bird's research, described later in this chapter), the finding that such a critical recall interval may exist has several important implications. First, training effects of SR can extend beyond the training session and thus can be brought to bear on clinically meaningful targets. Second, if the critical interval needed to place information in long-term memory can be determined for a particular individual (and the interval may vary across individuals, levels of dementia, etc.), this information will be helpful in predicting when to expect long-term retention of information outside training sessions. Third, this knowledge can be used to determine when SR training sessions are ready to be terminated and long-term maintenance of trained information can be instituted.
P.229
Extending the Use of SR: Implementation by Caregivers and Therapists
Most of this research involved persons living at home, the intervention being implemented by researchers. Some of the studies were conducted in home settings. Some were conducted in adult day care centers attended by persons with dementia. McKitrick (1993; McKitrick & Camp, 1993) extended this line of research by having family caregivers implement the training, similar to the approach taken by Moffat (1989). Other researchers likewise trained caregivers to implement SR as an intervention for persons with dementia, (Arkin, 1991; Riley, 1992). Riley (1992) also reported a case study in which a man in the initial stages of dementia was able to train himself to remember new information by utilizing SR. Brush and Camp (1998, in press) reported the use of SR by speech-language pathologists to reach clinical goals in persons with dementia, most of whom were living in a long-term care facility. Carruth (1997) reported the use of SR within the context of a music therapy session as a means of training nursing-home residents to remember names of staff members.
In these contexts, timing of recall intervals was not controlled by computer. For example, caregivers in McKitrick's studies used a hand-held digital timer and a nonelectrical tracking device to track and determine recall intervals (see McKitrick, 1993, for a detailed description of apparatus and procedures). In the case of speech-language pathologists, recall trials occurred during breaks between therapeutic activities conducted during speech therapy sessions (Brush & Camp, 1998, in press). Though this approach creates less precision than would be the case using more lab-based experimental procedures, SR appears to produce robust effects when applied in these real-world contexts. Furthermore, SR can be implemented by therapists while conducting billable procedures. Thus, it is more likely to be implemented on a large scale than if training effects were attainable only under more tightly controlled conditions, and/or only when applied by researchers.
Further Clinical Applications: Bird's Research
SR also has been implemented as a clinical intervention by Bird and his associates. His research using SR evolved from a more lab-based research paradigm, though it has taken a relatively direct route to using SR in clinical applications. As already noted, the work of Camp and associates has clear clinical implications, for example, in training dementia sufferers in daily calendar use (Camp et al., 1996b). Bird and Kinsella (1996) expanded the field in a more overtly clinical direction, attempting to add to the repertoire of well-researched psychosocial techniques that can be used to lessen behavior problems in dementia. The predominant experimental memory paradigm in dementia has been traditional verbal learning using word lists that are arguably low in ecological validity. But the major problem for many dementia sufferers and their caregivers is behavior that is far from trivial, such as violence, continuous screaming, repetitive questions, and incontinence (Patterson & Whitehouse, 1994; Teri et al., 1992). The basic research question, therefore, was whether it was possible to use SR to train persons with dementia to associate more adaptive behavior with a cue or cues so that on encountering the cue in common problem situations, they might respond differently.
P.230
The basic model is presented in Figure 12.2. The theoretical and experimental rationale that suggested such an operation might be possible drew mainly from the dementia list-learning literature, which has used a three-stage model of learning and memory: initial learning of new information (acquisition), storage of information in accessible form (retention), and accessing stored material when required (retrieval).
There were three findings of particular relevance in the literature. First, there is evidence that there are severe deficits at both acquisition and retrieval, at least in AD and vascular dementia. The provision of structured support at both these points on the processing continuum is essential to maximize learning, though performance still remains well below that of matched controls (Bird & Luszcz, 1991, 1993; Cherry & Plauche, 1996; Diesfeldt, 1984; Tuokko & Crockett, 1989). Second, a few studies that have provided extensive acquisition assistance and then strong support at retrieval in the form of forced choice recognition have shown that there can be substantial savings over clinically significant intervals (Hart, Kwentus, Taylor, & Harkin, 1987; Kopelman, 1985).
P.231
Third, the frequently found learning advantage for behavioral tasks also seems to apply in dementia (e.g., Herlitz, Adolfsson, Backman, & Nilsson, 1991).
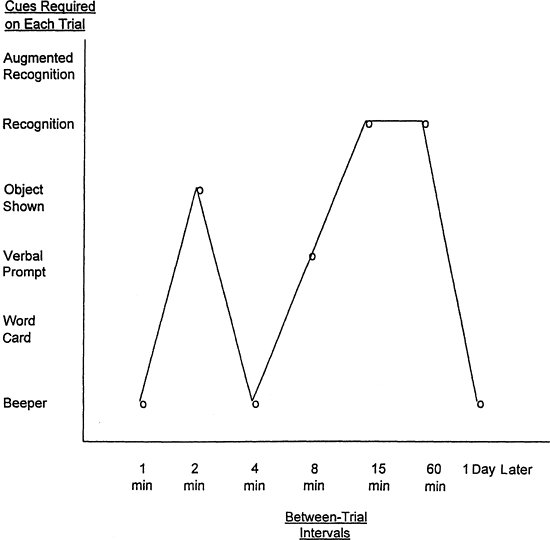 |
Figure 12.2. Example from one experiment of the sequence of supplementary cues provided at each trial where failure occurred. Sequence worked through until the participant was successful. |
From these findings, it was assumed that behavioral responses would be easier to learn than verbal material for older adults with dementia. In addition, so long as sufficient assistance was provided at acquisition and retrieval, these persons might be able to retain the information over periods long enough for such retention to be clinically relevant. However, the key to this type of intervention would be the cue, as a retrieval aid in itself, and also to ensure that retrieval occurred at the required time and/or place.
University students (Intons-Peterson & Fourner, 1986) as well as cognitively intact elderly persons (Dobbs & Rule, 1987; Einstein & McDaniel, 1990) use external cues extensively to prompt retrievals in ecologically relevant situations such as prospective memory operations; they are absolutely critical for persons with dementia. The cue thus has two roles at retrieval: determining whether the behavior is recalled at all and determining when it is recalled.
Acquisition Assistance and Use of Cues
The use of environmental cues has long been advocated in care for persons with dementia (e.g., painting toilet doors a different color), but there is little evidence other than the anecdotal of their efficacy in dementia. Unfortunately, texts advocating use of environmental cues in dementia seldom address the problem of acquisition. Yet, if the patient cannot spontaneously work out the association between the cue and the to-be-remembered information and is not assisted to acquire the association, the cue is of little value. Classic ward orientation studies (Gilleard, Mitchell, & Riordan, 1981; Hanley, 1981) showed that even signposts for example, Toilet were ineffective for persons with dementia in the absence of systematic assistance in learning what they related to.
A number of methods are known to assist acquisition of material in dementia, most commonly by inducing active processing. Two examples are requiring participants to decide about the taxonomic category of the item (e.g., Bird & Luszcz, 1991; Tuokko & Crockett, 1989) and about where it might be found (Martin, Brouwers, Cox, & Fedio, 1985). For the work under discussion, SR effect was used as the primary acquisition aid, for four reasons.
First, a preliminary study (Bird, 1995) showed that a single retrieval trial was as effective as presenting the material in a way that guaranteed active processing. That is, this study confirmed experimentally that the act of retrieval has a mnemonic effect in dementia; a successful recall increases the chance of subsequent recall. Second, Camp and his associates had already shown that learning and retention of nontrivial material over clinically significant intervals was possible by the use of SR. Third, the advantage of a series of retrieval trials over all other methods is that each presentation, as well as being a fresh learning trial, is also by definition a memory probe, enabling the experimenter or clinician to monitor progress and adjust the procedure to the patient's learning rate. Finally, Hanley (1981, 1984) used something analogous to retrieval trials in successful ward orientation studies. Rather than being repeatedly told the information (the method used by most caregivers and health professionals), persons with dementia had to provide the answer themselves in response to cues such
P.232
as Mrs. Smith, show me the dining room please ; Show me where you have your meals ; and Look, the tables are set for tea. What room is this, Mrs. Smith? (Hanley, 1984).
Two main experiments reported in Bird and Kinsella (1996) were part of a series where retrieval was used to teach cue/task associations to samples with either probable AD and/or vascular dementia. Trivial experimental tasks were used, for example, putting a card in an envelope or opening a box and reading a message. As shown in Figure 12.3, cues were primarily auditory alarms or words presented visually.
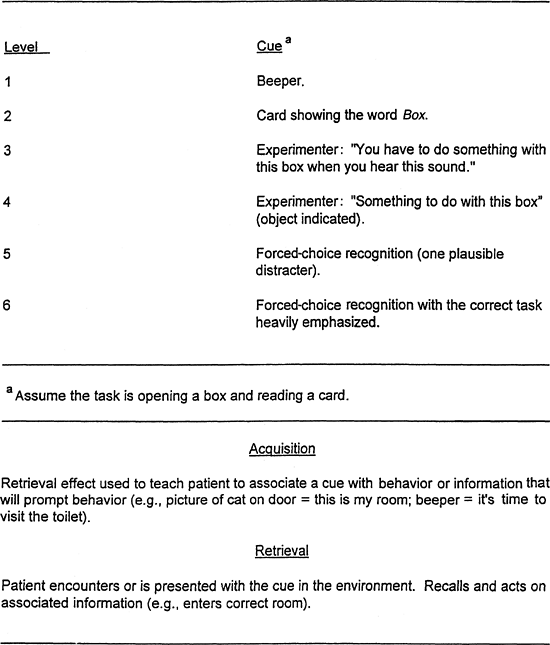 |
Figure 12.3. Number of cues required by a female subject (MMSE = 18) to retrieve a task (opening a box and reading a card) on each trial, and at a final recall trial 1 day later. |
P.233
The acquisition technique was an adaptation of SR; it was combined with the method of fading cues. Initial presentations were quite similar to the process described earlier in this chapter, with the first trial occurring immediately after first presentation of the material, for example:
This beeper (alarm sounds) is to remind you to put the card in the envelope.
(Short pause). So what will this beeper remind you to do?
Participants had their first delaeyed trial after 30 seconds. If failure occurred, they were given a series of extra cues, each successievely providing more information, until they successfully retrieved the task. The provision of supplementary cues where required also applied at all subsequent trials.
In the SR procedure described earlier in the chapter, the intertrial intervals are tailored to the subject's individual learning rate to ensure that successful retrieval will take place on most trials. If failure occurs, the intervals are reduced. For the experiments currently under discussion, it was the level of cued support that was tailored to individual needs. This method permitted standardization of intervals, which were roughly doubled for each successive trial (see Figure 12.3).
It also provided the outcome measure, tested 1 day after learning. That is, the dependent variable was not the number of items recalled from a list (the predominant experimental learning paradigm for more than a century), but the number of cues required to retrieve a single item. Single-task learning merits much more attention with this severely impaired population; it is more relevant to the clinical situation, where highly specific problems have to be addressed one at a time. Combining SR with fading cues also has the potential to significantly reduce the number of learning trials required for effective learning, because it increases the chances of successful retrieval occurring on any one trial.
At this stage, however, it is not known whether SR alone or the combined method has any other advantage, for example, in consolidation of the memory trace. In the clinical situation, there is the flexibility to use both, though the number of learning trials illustrated in Figure 12.3 is not recommended except with very mildly impaired persons with dementia. Nevertheless, despite the very limited number of trials used in the experimental work, two thirds of two separate samples, each of 24 participants (MMSE range 7 24) had retrievable memory for a task a day after learning it. Like the participant in Figure 12.3, a substantial proportion required only the primary cue and no subsidiary cues at final recall. Primary findings of this research can be summarized as follows:
A substantial proportion of participants with mild to moderate dementia could be trained, by SR, to associate a cue with a behavioral task so that the cue had specific recallable meaning after a delay of 1 day a retention interval that indicates these findings can have clinical utility.
Participants who could recall the task after a delay of 1 hour were usually able to recall it 1 day later. Capacity to remember after a 15-minute delay was a less reliable marker.
Confirming anecdotal clinical accounts (e.g., McEvoy & Patterson, 1986) and experimental work in dementia by B ckman and associates (for review, see B ckman, 1992), there was a mnemonic effect of actually performing a task on each trial, as opposed to observing it. It was equivalent to SR effects. That is, motor performance alone, in
P.234
the absence of retrieval on each trial, and retrieval alone on each trial, in the absence of motor performance, were equally effective.Motor performance combined with retrieval on each trial added nothing to the ability to verbally recall the task when tested after 1 day. However, actually performing a task made it much more likely that participants, having verbally recalled the task, would then spontaneously perform the task again a minimum requirement for clinical utility.
Research on the Basis of the SR Effect
One issue that has received scant attention in prior research concerns the potential mechanisms underlying the memorial benefit of SR. While most researchers emphasize the pragmatic implications (or clinical utility) of SR as a memory intervention technique, turning attention toward theoretical mechanisms of SR effects is an important challenge for at least two reasons. First, conceptual frameworks for research with special populations, such as persons with neurological impairment, are often borrowed from mainstream cognitive psychology. This is an advantageous practice in that findings from studies with special populations may yield important evidence regarding the theoretical constructs under investigation (Butters, 1984). For example, evidence showing that certain aspects of memory are affected in AD, while others seem unaffected, at least initially, provides convergent validity for several conceptual distinctions, including episodic/semantic memory and implicit/explicit memory (see Heindel, Salmon, Shults, Walicke, & Butters, 1989, for discussion). In principle, research on SR effects in cognitively impaired older adults may contribute to the evolution of theoretical constructs in cognitive psychology. As a second point, knowledge derived from basic research on the component processes that underlie SR effects may aid in the design of broad-based applications of the SR technique for improving retention in the daily lives of older persons with probable AD.
Accounts of Factors Underlying Spacing Effects in Normal Populations
Greene (1992) gave two accounts of the general spacing effect based on research primarily conducted with normal young adults. The first he called deficient-processing theories. By this account, information is not processed as fully when it is encountered in a massed versus a spaced presentation. One variation of this account states that persons engaged in spaced practice of items engage in more rehearsal for such items than for similar items presented in a massed-practice situation. Another variation is that more attention or cognitive effort, in general, is paid to items presented in a spaced presentation compared to a massed presentation, resulting in better recall of spaced items.
The second general account Greene (1992) gave for the spacing effect he called encoding-variability theories:
Multiple traces formed by spaced repetitions are likely to differ from each other more in some way than are the multiple traces formed by massed repetitions. This can then be used to explain the spacing effect if one goes on to assume that the probability of retrieving
P.235
at least one of two traces increases as a function of the differences between the traces, (p. 150)
Greene noted that encoding variability would best account for spacing effects found in free recall tasks, since factors facilitating retrieval such as encoding variability should have large effects in free recall. He also speculated, however, that spacing effects found in recognition tasks might best be accounted for by processing-deficit hypotheses, where access to memory traces is facilitated more than recall, and thus, the informativeness of traces is a critical component for successful recognition. Greene concluded that a dual-processing approach best explains the spacing effect, and that the underlying cause of the spacing effect seems to be task-specific.
Attempts to Determine the Locus of SR Effects in Persons with Dementia
Repetition alone does not seem to satisfactorily account for the success of SR in inducing new learning. In a study with patients diagnosed with AD, alcholomastic disorder, major depression, and normal elderly volunteers, Weingartner et al. (1993) found that persons with AD were the only group that was insensitive to repetition effects. Their AD subjects were unable to make use of multiple presentations to encode to-be-remembered words in either recognition or recall testing conditions. These researchers concluded that persons with Alzheimer's disease are unable to generate an explicit semantically appropriate context that can be used to rehearse and encode stimuli (p. 393). The effects of repetition alone, therefore, cannot explain the success of the SR technique in facilitating the learning of new information in AD and related disorders.
Bird (1995), working with a sample of persons with AD, compared effects of a form of SR with a condition he labeled baseline recall. This baseline recall condition was used to control for repetition effects and was similar to SR procedures (in this case, asking participants to name an object in a picture) except that participants were not required to retrieve information from memory, since the required information was kept visible at all times. Bird's results indicated that it is neither repetition alone nor the use of intervals alone that causes improved memory; the combination of recall practice across intervals is necessary for SR to function successfully. The problem of determining why SR should be effective for persons with dementia still remains.
Accessing an Implicit Memory System as an Explanation for SR Effects
The efficacy of SR for cognitively impaired older adults has been attributed to implicit memory processes that are thought to be spared until the later stages of AD (see Camp et al., 1993; Camp & McKitrick, 1992; Camp et al., 1996a, 1996b). Implicit memory is inferred when task performance is facilitated by previous exposure to test materials, without awareness of prior learning episodes at test (Lewandowsky, Dunn, & Kirsner, 1989). Backman (1992), among others, noted that under some testing conditions, implicit memory may be relatively spared in older adults with cognitive impairment associated with early stages of dementia (see Cherry & Plauche, 1996, for a review),
P.236
and there is evidence that for some abilities, this sparing may be seen in late stages of dementia as well (Bologna & Camp, 1995, 1997).
Much of the evidence behind the assumption that SR accesses implicit memory is either indirect or anecdotal. For example, levels of recall performance in persons with dementia trained with SR are generally not correlated with performance on standard (i.e., explicit) memory measures (Camp et al., 1996b; Foley, 1996; McKitrick et al., 1992; but also see Bird & Kinsella, 1996). Therefore, it is assumed that some mechanism other than explicit memory (such as implicit memory) must be involved in SR effects.
It was also reasoned that SR could be a form of errorless learning, in which persons with memory impairment acquire new information if they are not allowed to make errors at initial presentation and on subsequent training trials (Baddeley, 1992; Wilson, Baddeley, Evans, & Shiel, 1994). Errorless learning is assumed to access implicit memory and is effective for rehabilitation because external controls prevent errors and thus allow error-free learning to take place (Baddeley, 1992; Wilson et al., 1994). Without such controls, persons with explicit memory disorders cannot generally self-correct (i.e., they do not have conscious access to previous learning episodes) and thus may experience drift and inclusion of faulty information in learning trials over time. Since SR provides high rates of successful recall and any errors made are corrected and followed by an immediate (and therefore successful) recall trial, it would appear that SR is a type of errorless learning procedure.
Camp et al. (1996b) report anecdotal evidence of source amnesia in persons with dementia regarding use of an external memory aid (an appointment calendar). Participants would forget who had trained them or where the calendars had come from but could still remember and use the strategy of looking at the calendar to remember important information. Source amnesia is an indication of impaired explicit memory function. When seen in combination with successful SR training, an implication is that SR is utilizing an alternative memory system, implicit memory being the likely candidate.
Foss (1994) conducted an initial attempt to gather more direct evidence on the underlying basis for the effects produced by SR in persons with dementia. In her study, older adults with probable AD were trained to learn new face-name associations. The interval between retrieval trials was filled with a second activity that varied in the amount of cognitive effort required to do that activity (the Trail Making Task, Forms A and B). In Foss's study, recall intervals were fixed at 60 seconds, and eight trials were given to each participant for each face-name pair, to ensure that all participants would be expending comparable amounts of effort over comparable time periods between recall trials. Foss found that all older adults in her study were able to demonstrate near-perfect levels of learning and retention of face-name associations independent of the level of cognitive effort required to complete the Trail Making Task between recall trials.
Foss assumed that if efforts to manipulate cognitive effort on a task completed between recall trials had no effect on recall performance, then face-name learning could be taking place effortlessly and unconsciously between recall trials. Her findings were interpreted as evidence that implicit memory might be accessed via SR to enable new learning to take place in persons with dementia. This conclusion was reached based on the assumption made by Camp and his colleagues, among others (e.g., Schacter, Rich, & Stampp, 1985)
P.237
that recall attempts in SR training do not require great expenditure of cognitive effort on the part of persons with dementia (see also the description by Moffat, 1989).
Foley (1996) noted that other studies using normal participants found that long-term retention is actually improved when a difficulty task is placed between repetitions of information to be remembered (Bjork & Allen, 1970; Tzeng, 1973). This finding suggests that, at least in normal adults, recall can be influenced during SR training by manipulation of cognitive effort. There was a similar trend is Foss's data regarding better recall performance when the interpolated task required the highest cognitive effort, though small sample size and near ceiling effects for recall precluded a conclusive test to see if a similar pattern is found in persons with dementia. Clinically, we have found that when intervals between recall trials are filled with meaningful, attention-focusing activity in order to prevent rehearsal, the effectiveness of SR training seems to be enhanced. Foley (1996) concluded that this finding is evidence that learning, at least in the sense of effortful processing, cannot be occurring between trials during SR training. This was the conclusion reached by Foss and by Camp et al. (1996a), which led them to assume that the locus of the SR effect could be automatic consolidation between recall trials stimulated by the pattern of recall attempts used inSR.
It is interesting to note that Cermak, Verfaellie, Lanzon, Mather, and Chase (1996) found that amnesties could benefit from spaced repetition in a recall task, and that spacing effects found in amnesties were similar in magnitude to those found in normal controls. They speculated that in recall tasks, spacing effects found in amnesties are the result of automatic activation of associates of studied words.
While the work of Cermak et al. (1996) and Foss (1994) might militate against an explanation of SR being based on active rehearsal of items, at least in persons with dementia, other variations of Greene's deficient-processing account might still apply. For example, Magliero (1983) found that pupil dilation in persons studying word lists found greater dilation for items presented in a spaced-practice than in a massed-practice format, indicating greater processing of information in the spaced-practice format.
Cherry, Simmons, and Camp (in press) reported preliminary evidence consistent with the notion that implicit memory contributes to SR effects in cognitively impaired older adults. In the study by Cherry et al., the SR method was used to improve recall of everyday objects in four older persons with probable AD (ages 73, 86, 83, and 88). Three training sessions were administered at a local adult day care center on alternate days over 1 week. On each training trial, participants selected a designated item from an array of nine common household objects that were positioned on a flat 3 3 matrix. The items were exemplars of different taxonomic categories (e.g., carrot a vegetable; see Cherry & Park, 1993, for a description). A different object served as the target item in each training session.
To demonstrate implicit retention of the target items trained via SR, Cherry et al. (in press) used an adapted category exemplar generation task modeled after Light and Albertson (1989). They assumed that a category exemplar generation task would provide a sensitive measure of implicit memory because there is some evidence to indicate that category structures remain largely intact in AD (see Nebes, 1993, for discussion). Prior to SR training, a category exemplar generation pretest was given where participants were asked to name items that belonged to the same taxonomic category
P.238
as the to-be-trained target item. The purpose of the pretest was to obtain baseline information to aid in the interpretation of the category exemplar generation posttest data. The SR training trials followed. After the last trial, array items were removed from sight, and participants named items that belonged to the same taxonomic category as the target item. On the assumption that implicit memory contributes to SR effects, Cherry et al. expected to observe repetition-priming effects for the target items trained via SR. That is, a repetition-priming effect is observed when a target item is named in the category exemplar generation posttest, but not in the pretest.
As expected, SR training enhanced retention of the target items for all participants both within and across sessions. These findings provide further evidence of the mnemonic benefit of SR and the maintenance of SR effects over time. Importantly, each participant showed a repetition priming effect for the target item in at least one of the three training sessions, an outcome providing modest evidence of the contribution of implicit memory to SR. A limitation of this study was that one target item was never named in the posttest, while another item was named in the pretest by two of the four participants, so that repetition-priming effects for that item could not be interpreted unequivocally for those participants. Consequently, the two problematic target items were replaced with two new objects selected for training in the follow-up study described next.
Cherry and her associates have since conducted a second study to examine the reliability and generality of their earlier findings. They tested four persons with probable AD (ages 96, 84, 82, and 83 years) who were enrolled in the local adult day care program. The materials and general procedures were the same as those used in Cherry et al. (in press), except that two target items were replaced with new objects to increase the sensitivity of the category exemplar generation task as a measure of implicit retention. They also added a two-letter word-stem completion task as a second measure of implicit retention of the trained objects. The word-stem completion task was administered immediately after the category exemplar generation posttest in each training session.
Table 12.1 presents the longest retention interval achieved by each participant in each of the three training sessions. As can be seen in Table 12.1, all participants were able to continue the training for a longer period of time and showed larger performance gains in the second session than in the first. Moreover, three of the four participants reached a substantially longer retention interval in the third session than in the first. For example, on the last day of training, S2 had successfully reached a retention
P.239
interval that represented over a threefold increase in duration, relative to the first training session. Whether further gains in performance would occur if more than three training sessions are included is a potentially important direction for future research. Camp's research would indicate that further gains with increased training would be likely.
Table 12.1 Longest Retention Interval Achieved, in Minutes, by Participants Across Training Sessions | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
One participant named the target item jacket, two participants named the item bracelet, and one participant named the item carrot after SR training in Sessions 1 3, respectively. These repetition-priming effects can be interpreted unequivocally as evidence of implicit retention, insofar as none of these items were named as exemplars of their respective taxonomic categories in the pretest. Interestingly, repetition-priming effects were not found in the word-stem completion task. In addition, these same participants showed extreme deficits in external memory functioning, as expected. Future research could be directed toward developing other methods of assessing implicit retention in persons with probable AD.
Accessing the Explicit Memory System as an Explanation for SR Effects
Bird and Kinsella (1996) directly addressed the issue of effortful versus automatic processing underlying SR for persons with dementia. They concluded that while some SR trials seemed to elicit automatic processing, their participants also seemed to consciously attempt retrieval with SR tasks on other occasions. In addition, they noted that memory for the target information could at least fleetingly be made consciously available at recall. As a result, they speculated that expenditure of conscious effort may take place in SR, and that repeated practice in recalling stimuli could make retrieval eventually automatic. The implication of this line of argument is that SR is engaging an explicit memory system and requires expenditure of cognitive effort in order to succeed.
Foley (1996) further investigated the possible locus of the SR effect. She conducted a study comparing effects of SR and three other conditions (spaced reminding, massed retrieval, and massed reminding) on face-name recall in older adults with dementia. In her study, SR produced superior performance compared to all other conditions. In fact, training in the other conditions did not appear to assist memory performance in these participants. Thus, there was strong evidence that SR effects in persons with dementia require both active recall attempts and the spacing of such attempts.
In addition, Foley wished to determine whether the locus of SR effects might be due to the amount of effort expended when persons with dementia attempt recall. She used an SR training task involving cued recall, rather than free recall. In addition, she looked at the number of cues necessary to correctly recall target information, at the time taken between cue presentation and subsequent recall, and at the amount of time necessary to retrieve target information after a cue was given. She hypothesized that at least in a cued-recall paradigm, SR effects are due to effortful processing, and that the provision of cues enables an impaired explicit memory system to utilize experimentally provided compensations and operate more effectively. She further hypothesized that greater amounts of time are needed to successfully recall information after long recall intervals (i.e., 4 min) than after short recall intervals. Such an outcome
P.240
would indicate that recall in a SR paradigm is actually an effortful process, and that the amount of effort expended is a function of recall intervals.
Replicating the results of Camp et al. (1996b), Foley found that SR performance is not related to other measures of explicit memory. While the number of retrieval cues needed to elicit correct recall was smaller for persons in the SR condition than in the other conditions, as described earlier, an average of at least three cues was needed to elicit correct recall. In addition, as in the findings of Bird and Kinsella (1996), some individuals in the SR condition needed substantial amounts of time to correctly recall information at the longest time interval, but others required little time. Foley, like Greene, concluded that it seems unlikely that any single factor or process is adequate to explain SR effects.
The Problem of Defining Implicit and Explicit Memory: Task Versus Memory System
A problematic feature in discussing the nature of SR effects is that the terms implicit memory and explicit memory are sometimes used to describe both experimental tasks (e.g., defining recognition memory as an implicit memory task and recall as an explicit memory task, as was done by Cermak et al., 1996) as well as memory systems and processes (e.g., an implicit memory system or an explicit memory system, as was done by Schacter, 1994, and Squire, 1994). If a recall task such as successful recall of newly learned information is accomplished by an individual with dementia, researchers are faced with a dilemma. To claim that recall is an explicit memory task, one is faced with the need to describe a form of explicit memory that is not devastated by dementia. Since conscious/effortful process is damaged in dementia, one must decide that there are automatic/effortless/unconscious aspects of explicit memory tasks. Thus, one is faced with using the classification system shown in Figure 12.4 to describe memory research outcomes.
For example, Ostergaard, Heindel, and Paulsen (1995) found that they could induce biasing effects in a recognition task for ambiguous figures in persons with AD by labeling figures at encoding. (In contrast to Cermak et al., 1996, these researchers categorized their recognition task as an explicit memory task, exemplifying further complexities of the classification problem in this type of research.) This biasing was
P.241
shown after a 30-minute delay, even though conscious recognition of these stimulus items was at chance levels in persons with AD. Yet researchers often feel that if recall or recognition tasks are employed in a study in which priming takes place, explicit memory is critically involved. As a result, Ostergaard et al. concluded that seemingly unconscious cognitive processes can bias the explicit [italics theirs] memory performance of AD patients, whose explicit memory is otherwise severely compromised (p. 279).
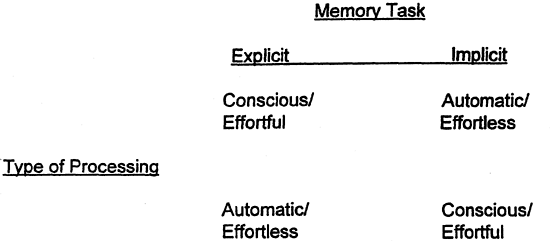 |
Figure 12.4. Classification system to describe memory research outcomes. |
In this model, recall training using SR might be classified as an explicit memory task in which persons with dementia and other memory disorders utilize automatic/ unconscious processing to successfully learn and retain new information. Alternatively, as Foley (1996) suggested, SR might be classified as an explicit memory task that requires effortful/conscious processing at initial encoding to be successful. It remains to be seen whether a model that focuses on tasks or a model that focuses on hypothesized underlying memory systems is most fruitful in generating research that will help discover the underlying locus of SR effects. We will discuss this issue further in our final summary. The following case study also illustrates a number of points germane to the discussion of the complexities involved in ascertaining the locus of SR effects.
A Case Study
Mrs. D was an 83-year-old woman with vascular dementia. Her MMSE score was 19. She had been admitted a few weeks previously to a hostel following failure to self-care at home and was referred for paranoid delusions and violence. In practice, this meant accusing staff of stealing her personal possessions and outbursts of temper, including physical aggression to caregivers and property. Detailed assessment demonstrated that the most parsimonious and clinically useful explanation was not the language of psychiatric illness, but that Mrs. D was simply making a mistake. Prior to admission to the hostel, she had given most of her property away, but the dementing process meant that she had no easily retrievable memory for this action. Early in her stay, nursing staff could successfully remind her of what had happened when she asked about her possessions, but as the memory of her property distribution became more remote, she ceased to believe them. This made some staff irritable, and heated discussions ensued. The situation escalated from there.
Hypotheses about how Mrs. D saw the world are an essential requirement of assessment with problems of this sort. Our hypotheses suggested that she was living in a place she didn't know; furthermore, she was being told, with increasing acerbity, by people she didn't know, that she had given all her possessions away. Accordingly, she arrived at what was, to her, the most parsimonious explanation: They had stolen her things, and she had a right to be furious.
The intervention involved, first, a session with Mrs. D and the family member who had assisted in disposal of her personal effects, using multiple situational cues to assist her to recall these events. A list was produced in large print, with a prominent, colored Smiley face in the corner, and posted in her wardrobe (she refused to have it on public display in her room). Over a 2-hour period, she was trained, by use of the retrieval effect and motor performance, to associate anxiety about her things with going to the wardrobe and looking at the list.
Thus, after the notice was posted with some ceremony (to make the posting more memorable), learning was initiated with questions such as What will help you remember what happened to your things? How do you find out who you gave your sewing machine
P.242
to? and Tell me what happened to your things before you came here. Intertrial intervals increased as the memory consolidated.
If failure occurred on any trial, Mrs. D was given graded cues as required, for example, Isn't there a notice somewhere that will tell you? Isn't there a notice somewhere with a smiley face? Isn't there a notice somewhere that looks like this? (blank notice with smiley face presented). On each trial after the first closely spaced few, she was encouraged to actually go and look at the notice.
Staff were subsequently trained to use graded cues to help Mrs. D remember to use the notice. Demands had dropped from a mean of 35 40 demands daily to 5 after I week, and they soon ceased entirely. Mrs. Ds' mistake had been corrected by her being given access to information she could not retrieve for herself. At 5-month follow-up, there were still no problems. Though there were other factors in this case, the memory intervention played a critical role. The behavior dropped off immediately after training, and on testing 2 weeks postintervention, Mrs. D still knew all about the smiley-face notice in her wardrobe and what it was there for.
Comments and Caveats
First, a particular feature of this and many similar cases is that the change in behavior was maintained. This is consistent with the mnemonic effects of SR. Each naturalistic encounter with the cue in which its meaning is retrieved becomes a fresh spaced-learning trial, which may maintain the association.
Second, it should be noted that the cue was an anxious thought, not a tangible auditory or visual prompt. The notice was simply the means by which anxiety was allayed. A similar case can be found in Bird, Alexopoulos, and Adamowicz (1995) with a patient who asked obsessively for her bowel medication. This type of clinical application of SR clearly extends the experimental findings significantly, as well as further challenging myths held by many health professionals and researchers about the learning capacities of people with dementia. In other cases, participants have managed to internalize cue/behavior associations (Camp & Foss, 1997; Camp et al., 1996a, 1996b; Woods & Bird, in press), with no need for external prompting. Such findings generate an argument for more memory research addressing real-life problems and capacities of people with dementia.
Third, this intervention was multifaceted, both clinically and theoretically. Equally important clinical facets of this case were building up rapport and trust with a very suspicious and angry patient and working sensitively with the exasperated caregivers, not only to ensure that they would continue to cue Mrs. D, but to change their responses from confrontation to empathy.
Theoretically, the active ingredients of the intervention are multiple and difficult to disentangle. The initial training was critical to induce use of the notice, but apart from the maintenance of memory by repeated naturalistic retrievals, operant conditioning probably helped equally in maintaining use of the notice because of its role as an anxiety reducer. Further, as staff responses changed, trust and rapport built up between them and Mrs. D, so that it was less likely that staff would be perceived as thieves. Staff change was easier to accomplish because they now had a concrete memory-prompting procedure to follow instead of acrimonious and futile argument with Mrs. D. That is, it is futile to regard cued recall of adaptive behavior or any other psychosocial
P.243
technique in isolation; it is not equivalent to a pill, which, if taken will fix the situation by itself.
Finally and more generally, SR is not a panacea for behavior problems in dementia. In many cases, as here, it will form only part of the intervention, which may require many therapeutic modalities. In yet other cases, it will be inappropriate or ineffective, or the patient will not cooperate. As discussed elsewhere in this volume, the idiosyncratic and multifaceted nature of each case profile requires detailed assessment and careful selection of the most appropriate techniques. Training in cued recall of adaptive behavior as described here is simply something that, like all other techniques (including sensitive use of medication), will assist some persons with dementia in some situations some of the time.
Summary
The use of SR as an intervention for dementia is still relatively new, though it is hoped that readers of this chapter will see that there is considerable cause for optimism about its utility as a clinical/rehabilitative intervention. Large-scale studies of the effects of SR, and the parameters that influence its effectiveness and clinical utility are yet to be performed. Within the two areas of clinical application and theoretical explanations of the locus of SR effects, a number of areas suggest themselves for future research.
Clinical Application Issues in SR
Camp (1989) listed a number of clinical application issues in SR that needed (and still need) to be addressed. One issue is the amount of information that can be trained and retained by use of SR. To date, most research has focused on a single target or, at most, up to three targets (Brush & Camp, 1998, in press; McKitrick et al., 1992). SR has the potential to train a large number of items of information, but we simply don't know the limits (such as potential interference effects) that dementia will place on this potential. For example, though McKitrick et al. (1992) reported little problem with interference effects in their study, this topic has yet to be adequately explored.
In related areas, we don't understand the forgetting functions of information learned by means of SR, nor do we know about how to best maintain information once it has been learned. We also do not know how to create individualized optimal expansion schedules. Similarly, given that in many instances standard measures of memory performance do not predict how well individuals with dementia will succeed during SR training, it would be extremely useful to develop predictors of which persons will learn most readily in an SR training paradigm.
Theoretical Explanations of the Locus of SR Effects
The attempt to determine the theoretical locus of SR effects has been hampered by a variety of problems. Is it best to assume that SR accesses one and only one type of memory in free recall and/or cued recall and/or recognition tests? Is it possible for a
P.244
single memory system to be involved across multiple tasks? That is, is it best to conceptualize any memory success seen in persons with dementia as being supported by a single memory system, such as implicit memory, and to ascribe any memory failures to a declining explicit memory system? Is it best to view each system as capable of generating memory failures and successes, though at generally different rates, depending on the specific training context?
An ultimate resolution to this discussion may await the use of on-line measures of brain functioning such as PET used in conjunction with SR training to determine which areas of the brain are being activated in SR. If memory systems' functions show anatomical correlates with areas of brain activation, the basis for SR's success across a variety of experimental contexts (e.g., recall, cued recall, recognition) may be addressed more directly through brain imaging.
Of course, much of the research in this area has taken the approach that an implicit-explicit memory dichotomy is the appropriate perspective from which to view SR training in particular and memory functioning in general. The utility of such a dichotomy in studying memory functioning is not universally shared. Rovee-Collier (1997), in reviewing research on the development of implicit and explicit memory during infancy, made the following comments:
Evidence amassed from a large number of studies that were conducted over the past 25 years disputes claims that implicit and explicit memory follow different developmental lines and challenges the utility of conscious recollection as the defining characteristic of explicit memory. It seems unlikely that any simple dichotomy could adequately characterize a process as complex as memory, even during the infancy period, (pp. 467 468)
Adults with dementia usually learn new associations when trained with SR. Some learn associations quickly, with few errors, while others learn more slowly, and it appears possible that some individuals may not learn at all. Some individuals with dementia seem to expend cognitive effort when attempting to recall information trained with SR, and others don't, and the amount of cognitive effort expended by an individual may change over time. Some retain new information learned via SR over long periods, and in others, the memory seems to fade more quickly. Why such diversity of SR effects occurs has both clinical and theoretical significance. Current theoretical formulations have proven unsatisfactory in providing a general explanation for the locus of SR effects, much less in addressing the issues of variability in SR training outcomes just described. Perhaps the studies conducted thus far have not been adequate in their efforts to design critical tests of theory. More likely, in our opinion, current theory is inadequate to deal with outcomes generated by SR training paradigms for persons with dementia. It is our hope that attempts to explain such outcomes will spur further theoretical development, which is always an important contribution of applied research to a developing science.
References
Abrahams, J. P., & Camp, C. J. (1993). Maintenance and generalization of object naming training in anomia associated with degenerative dementia. Clinical Gerontologist, 12, 57 72.
P.245
Alexopoulos, P. (1994). Management of sexually disinhibited behaviour by a demented patient. Australian Journal on Ageing, 13, 119.
Arkin, S. M. (1991). Memory training in early Alzheimer's disease: An optimistic look at the field. American Journal of Alzheimer's Care and Related Disorders and Research, 6, 17 25.
Backman, L. (1992). Memory training and memory improvement in Alzheimer's disease: Rules and exceptions. Acta Neurologica Scandinavica, 84, 84 89.
Baddeley, A. D. (1989). Finding the bloody horse. In L. W. Poon, D. C. Rubin, & B. A. Wilson (Eds)., Everyday cognition in adulthood and late life (pp. 104 115). New York: Cambridge University Press.
Baddeley, A. D. (1992). Implicit memory and errorless learning: A link between cognitive theory and neuropsychological rehabilitation? In L. R. Squire & N. Butters (Eds.), Neuropsychology of memory (2nd ed., pp. 309 314). New York: Guilford Press.
Banaji, M. R., & Crowder, R. G. (1989). The bankruptcy of everyday memory. American Psychologist, 44, 1185 1193.
Banaji, M. R., & Crowder, R. G. (1991). Some everyday thoughts on ecologically valid methods. American Psychologist, 46, 78 79.
Bird, M. (1995). Aids to acquisition in senile dementia: Retrieval and effortful processing. Unpublished manuscript.
Bird, M., Alexopoulos, P., & Adamowicz, J. (1995). Success and failure in five case studies: Use of cued recall to ameliorate behaviour problems in senile dementia. International Journal of Geriatric Psychiatry, 10, 5 11.
Bird, M., & Kinsella, G. (1996). Long-term cued recall of tasks in senile dementia. Psychology and Aging, 11, 45 56.
Bird, M. J., & Luszcz, M. A. (1991). Encoding specificity, depth of processing, and cued recall in Alzheimer's disease. Journal of Clinical and Experimental Neuropsychology, 13, 508 520.
Bird, M. J., & Luszcz, M. A. (1993). Enhancing memory performance in Alzheimer's disease: Acquisition assistance and cue effectiveness. Journal of Clinical and Experimental Neuropsychology, 15, 921 932.
Bjork, R. A. (1988). Retrieval practice and the maintenance of knowledge. In M. M. Gruneberg, P. Morris, & R. Sykes (Eds.), Practical aspects of memory (Vol. 2, pp. 396 401). London: Academic Press.
Bjork, R. A., & Allen, T. W. (1970). The spacing effect: Consolidation or differential encoding? Journal of Verbal Learning and Behavior, 9, 567 572.
Bologna, S. M., & Camp, C. J. (1995). Self-recognition in Alzheimer's disease: Evidence of an implicit/explicit dissociation. Clinical Gerontologist, 15, 51 54.
Bologna, S. M., & Camp, C. J. (1997). Covert versus overt self-recognition in late stage Alzheimer's disease. Journal of the International Neuropsychological Society, 3, 195 198.
Brush, J. A., & Camp, C. J. (1998). Using spaced retrieval as an intervention during speech-language therapy. Clinical Gerontologist, 19, 51 64.
Brush, J. A., & Camp, C. J. (in press). Using spaced retrieval to treat dysphagia in a long-term care resident with dementia. Clinical Gerontologist.
Butters, N. (1984). The clinical aspects of memory disorders: Contributions from experimental studies of amnesia and dementia. Journal of Clinical Neuropsychology, 6, 17 36.
Camp, C. J. (1989). Facilitation of new learning in Alzheimer's disease. In G. C. Gilmore, P. J. Whitehouse, & M. L. Wykle (Eds.), Memory, aging, and dementia (pp. 212 225). New York: Springer.
Camp, C. J. (1996). The return of Sherlock Holmes: A pilgrim's progress in memory and aging research. In M. R. Merrens & G. G. Brannigan (Eds.), The developmental psychologists (pp. 217 232). New York: McGraw-Hill.
P.246
Camp, C. J., & Foss, J. W. (1997). Designing ecologically valid memory interventions for persons with dementia. In D. G. Payne & F. G. Conrad (Eds.), Intersections in basic and applied memory research (pp. 311 325). Mahwah, NJ: Erlbaum.
Camp, C. J., Foss, J. W., O'Hanlon, A. M., & Stevens, A. B. (1996a). Memory interventions for persons with dementia. Applied Cognitive Psychology, 10, 193 210.
Camp, C. J., Foss, J. W., Stevens, A. B., & O'Hanlon, A. M. (1996b). Improving prospective memory task performance in Alzheimer's disease. In M. A. Brandimonte, G. O. Einstein, & M. A. McDaniel (Eds.), Prospective memory: Theory and applications (pp. 351 367). Mahwah, NJ: Erlbaum.
Camp, C. J., Foss, J. W., Stevens, A. B., Reichard, C. C, McKitrick, L. A., & O'Hanlon, A. M. (1993). Memory training in normal and demented elderly populations: The E-I-E-I-O model. Experimental Aging Research, 19, 277 290.
Camp, C. J., & McKitrick, L. A. (1992). Memory interventions in Alzheimer's-type dementia populations: Methodological and theoretical issues. In R. L. West & J. D. Sinnott (Eds.), Everyday memory and aging: Current research and methodology (pp. 155 172). New York: Springer-Verlag.
Camp, C. J., & Schaller, J. R. (1989). Epilogue: Spaced-retrieval memory training in an adult day care center. Educational Gerontology, 15, 81 88.
Camp, C. J., & Stevens, A. B. (1990). Spaced retrieval: A memory intervention for Dementia of the Alzheimer's Type (DAT). Clinical Gerontologist, 10, 58 61.
Carruth, E. K. (1997). The effects of singing and the spaced retrieval technique on improving face-name recognition in nursing home residents with memory loss. Journal of Music Therapy, 34, 165 186.
Cermak, L. S., Verfaellie, M., Lanzoni, S., Mather, M., & Chase, K. A. (1996). Effect of spaced repetitions on amnesia patients' recall and recognition performance. Neuropsychology, 2, 219 227.
Cherry, K. E., & Park, D. C. (1993). Individual difference and contextual variables influence spatial memory in younger and older adults. Psychology and Aging, 8, 517 526.
Cherry, K. E., & Plauche, M. F. (1996). Memory impairment in Alzheimer's disease: Findings, interventions, and implications. Journal of Clinical Geropsychology, 2, 263 296.
Cherry, K. E., Simmons, S. S., & Camp, C. J. (in press). Spaced-retrieval enhances memory in older adults with probable Alzheimer's disease. Journal of Clinical Geropsychology.
Diesfeldt, H. F. A. (1984). The importance of encoding instructions and retrieval cues in the assessment of memory in senile dementia. Archives of Gerontology and Geriatrics, 3, 51 57.
Dobbs, A. R., & Rule, B. G. (1987). Prospective memory and self-reports of memory abilities in older adults. Canadian Journal of Psychology, 41, 209 222.
Einstein, G. O., & McDaniel, M. A. (1990). Normal aging and prospective memory. Journal of Experimental Psychology, Learning Memory and Cognition, 16, 717 726.
Foley, L. C. (1996). Spaced retrieval as a mnemonic in dementia: Its efficacy and the role of cognitive effort. Unpublished master's theses, Australian National University, Department of Psychology, Canberra.
Foss, J. W. (1994). Cognitive effort: Effects of spaced-retrieval on learning in AD. Unpublished master's thesis, University of New Orleans, Department of Psychology.
Gilleard, C, Mitchell, R. G., & Riordan, J. (1981). Ward orientation training with psychogeriatric patients. Journal of Advanced Nursing, 6, 95 98.
Glisky, E. L., & Schacter, D. L. (1986). Remediation of organic memory disorder: Current status and future prospects. Journal of Head Trauma Rehabilitation, 1, 54 63.
Glisky, E. L., & Schacter, D. L. (1987). Aquisition of domain-specific knowledge in organic amnesia: Training for computer-related work. Neuropsychologia, 25, 893 906.
Glisky, E. L., Schacter, D. L., & Tulving, E. (1986). Learning and retention of computer-related vocabulary in amnestic patients: Method of vanishing cues. Journal of Clinical and Experimental Neuropsychology, 8, 292 312.
P.247
Greene, R. L. (1992). Repetition paradigms. In R. L. Greene (Ed.), Human memory: Paradigms and paradoxes (pp. 132 152). Hillsdale, NJ: Erlbaum.
Hanley, I. G. (1981). The use of signposts and active training to modify ward disorientation in elderly patients. Journal of Behavioural Therapy and Experimental Psychology, 12, 241 247.
Hanley, I. (1984). Theoretical and practical considerations in reality orientation therapy with the elderly. In I. Hanley & J. Hodge (Eds.), Psychological approaches to the care of the elderly (pp. 164 191). London: Croom Helm.
Hart, R. P., Kwentus, J. A., Taylor, J. R., & Harkin, S. W. (1987). Rate of forgetting in dementia and depression. Journal of Consulting and Clinical Psychology, 55, 101 105.
Hayden, C. M., & Camp, C. J. (1995). Spaced-retrieval: A memory intervention for dementia in Parkinson's disease. Clinical Gerontologist, 16(3), 80 82.
Heindel, W. C, Salmon, D. P., Shults, C. W., Walicke, P. A., & Butters, N. (1989). Neuropsychological evidence for multiple memory systems: A comparison of Alzheimer's, Huntington's, and Parkinson's disease patients. Journal of Neuroscience, 9, 582 587.
Herlitz, A., Adolfsson, R., Backman, L., & Nilsson, L.-G. (1991). Cue utilization following different forms of encoding in mildly, moderately, and severely demented patients with Alzheimer's disease. Brain and Cognition, 15, 119 130.
Intons-Peterson, M. J., & Fourner, J. (1986). External and internal memory aids: How often do we use them? Journal of Experimental Psychology, 115, 267 280.
Kopelman, M. D. (1985). Rates of forgetting in Alzheimer-type dementia and Korsakoff's syndrome. Neuropsychologia, 23(5), 623 638.
Landauer, T. K. (1989). Some bad and good reasons for studying memory and cognition in the wild. In L. W. Poon, D. C. Rubin, & B. A. Wilson (Eds.), Everyday cognition in adulthood and late life (pp. 116 125). New York: Cambridge University Press.
Landauer, T. K., & Bjork, R. A. (1978). Optimal rehearsal patterns and name learning. In M. M. Gruneberg, P. E. Harris, & R. N. Sykes (Eds.), Practical aspects of memory (pp. 625 632). New York: Academic Press.
Lewandowsky, S., Dunn, J. C, & Kirsner K. (1989). Implicit memory: Theoretical issues. Hillsdale, NJ: Erlbaum.
Light, L. L., & Albertson, S. A. (1989). Direct and indirect tests of memory for category exemplars in young and older adults. Psychology and Aging, 4, 487 492.
Magliero, A. (1983). Pupil dilations following pairs of identical and related to-be-remembered words. Memory and Cognition, 11, 609 615.
Martin, A., Brouwers, P., Cox, C, & Fedio, P. (1985). On the nature of the verbal memory deficit in Alzheimer's Disease. Brain and Language, 25, 323 341.
McEvoy, C, & Patterson, R. (1986). Behavioral treatment of deficit skills in dementia patients. Gerontologist, 26, 475 478.
McKitrick, L. A. (1993). Caregiver participation in word-retrieval training with anomic Alzheimer's disease patients. Unpublished doctoral dissertation, University of New Orleans, Department of Psychology.
McKitrick, L. A., & Camp, C. J. (1993). Relearning the names of things: The spaced-retrieval intervention implemented by a caregiver. Clinical Gerontologist, 14, 60 62.
McKitrick, L. A., Camp, C. J., & Black, F. W. (1992). Prospective memory intervention in Alzheimer's Disease. Journal of Gerontology: Psychological Sciences, 47, 337 343.
Moffat, N. J. (1989). Home-based cognitive rehabilitation with the elderly. In L. W. Poon, D. C. Rubin, & B. A. Wilson (Eds)., Everyday cognition in adulthood and late life (pp. 659 680). New York: Cambridge University Press.
Mook, D. G. (1989). The myth of external validity. In L. W. Poon, D. C. Rubin, & B. A. Wilson (Eds.), Everyday cognition in adulthood and late life (pp. 25 43). New York: Cambridge University Press.
P.248
Nebes, R. D. (1993). Cognitive dysfunction in Alzheimer's Disease. In F. I. M Craik & T. A. Salthouse (Eds.), The handbook of aging and cognition (pp. 373 446). Hillsdale, NJ: Erlbaum.
Ostergaard, A. L., Heindel, W. C, & Paulsen, J. S. (1995). The biasing effect of verbal labels on memory for ambiguous figures in patients with progressive dementia. Journal of the International Neuropsychological Society, 1, 271 280.
Patterson, M. B., & Whitehouse, P. J. (1994). Behavioral symptoms in dementia. Alzheimer Disease and Associated Disorders, 8(Suppl. 3), 1 3.
Petrinovich, L. (1989). Representative design and the quality of generalization. In L. W. Poon, D. C. Rubin, & B. A. Wilson (Eds.), Everyday cognition in adulthood and late life (pp. 11 24). New York: Cambridge University Press.
Riley, K. P. (1992). Bridging the gap between researchers and clinicians: Methodological perspectives and choices. In R. L. West & J. D. Sinnott (Eds.), Everyday memory and aging: Current research and methodology (pp. 182 189). New York: Springer-Verlag.
Rovee-Collier, C. (1997). Dissociations in infant memory: Rethinking the development of implicit and explicit memory. Psychological Review, 104, 467 498.
Schacter, D. L. (1992). Understanding implicit memory. American Psychologist, 47, 559 569.
Schacter, D. L. (1994). Priming and multiple memory systems: Perceptual mechanisms in implicit memory. In D. L. Schacter & E. Tulving (Eds.), Memory systems 1994 (pp. 233 268). Cambridge, MA: MIT Press.
Schacter, D. L., Rich, S. A., & Stampp, M. S. (1985). Remediation of memory disorders: Experimental evaluation of the spaced-retrieval technique. Journal of Clinical and Experimental Neuropsychology, 7, 70 96.
Schacter, D. L., & Tulving, E. (1994). What are the memory systems of 1994? In D. L. Schacter & E. Tulving (Eds.), Memory systems 1994 (pp. 1 38). Cambridge, MA: MIT Press.
Squire, L. R. (1994). Declarative and nondeclarative memory: Multiple brain system supporting learning and memory. In D. L. Schacter & E. Tulving (Eds.), Memory systems 1994 (pp. 203 232). Cambridge, MA: MIT Press.
Stevens, A. B., O'Hanlon, A. M., & Camp, C. J. (1993). Strategy training in Alzheimer's Disease: A case study. Clinical Gerontologist, 13, 106 109.
Teri, L., Truax, P., Logsdon, R., Uomoto, J., Zarit, S., & Vitaliano, P. P. (1992). Assessment of behavioral problems in dementia: The revised memory and behavior problems checklist. Psychology and Aging, 7, 622 631.
Tulving, E. (1991). Memory research is not a zero-sum game. American Psychologist, 46, 41 42.
Tuokko, H., & Crockett, D. (1989). Cued recall and dementia. Journal of Clinical and Experimental Neuropsychology, 11, 278 294.
Tzeng, O. J. L. (1973). Stimulus meaningfulness, encoding variability, and the spacing effect. Journal of Experimental Psychology: General, 99, 162 166.
Weingartner, H., Eckhardt, M., Grafman, J., Molchan, S., Putnam, K., Rawlings, R., & Sunderland, T. (1993). The effects of repetition on memory performance in cognitively impaired patients. Neuropsychology, 7, 385 395.
Wilson, B. A. (1997). Cognitive rehabilitation: How it is and how it might be. Journal of the International Neuropsychological Society, 5, 487 496.
Wilson, B. A., Baddeley, A., Evans, J., & Shiel, A. (1994). Errorless learning in the rehabilitation of memory impaired people. Neuropsychological Rehabilitation, 4, 307 326.
Woods, B., & Bird, M. (in press). Non-pharmacological approaches to treatment. In G. Wilcock, R. Bucks, & K. Rockwood (Eds.), Diagnosis and management of dementia: A manual for memory disorders teams. Oxford: Oxford University Press.
EAN: 2147483647
Pages: 18