34 - Median Sternotomy and Parasternal Approaches to the Lower Trachea and Main-Stem Bronchi
Editors: Shields, Thomas W.; LoCicero, Joseph; Ponn, Ronald B.; Rusch, Valerie W.
Title: General Thoracic Surgery, 6th Edition
Copyright 2005 Lippincott Williams & Wilkins
> Table of Contents > Volume I - The Lung, Pleura, Diaphragm, and Chest Wall > Section IX - The Chest Wall > Chapter 42 - Infections of the Chest Wall
Chapter 42
Infections of the Chest Wall
Joseph LoCicero III
Chest wall infections can be categorized either as primary problems arising spontaneously or as secondary infections caused by previous procedures or preexisting disease states. The result is the same, with equally devastating potential complications. Management of such infections may be as simple as administering routine antibiotic therapy or may require multiple and prolonged drainage procedures and complex reconstructive operations. Prompt intervention is essential to minimize serious morbidity.
SKIN AND SOFT TISSUE INFECTIONS
The thorax accounts for one fifth of the total body surface area and thus can be afflicted with many common, nonspecific soft tissue infections. Furuncles and boils common to any hair-bearing surface frequently occur. Superficial infections often develop in minor injuries and burns of the chest, as they do elsewhere in the body.
Abscesses
Soft tissue abscesses may occur anywhere on the chest wall. They are characterized by the usual signs and symptoms of an abscess anywhere on the body and are rarely associated with an abnormal chest radiograph. Two potentially serious infections specific to the chest wall and involving large potential spaces are subpectoral and subscapular abscesses. These occasionally present as primary infections but more often are secondary to a chronically infected thoracotomy incision. They are characterized by local pain, with or without swelling, combined with fever and leukocytosis. Computed tomography (CT) easily identifies and localizes the problem. Prompt drainage and appropriate antibiotic therapy usually lead to successful resolution. Suction catheters are rarely required because these spaces are obliterated once drained. Occasionally when the abscess is large, several counterincisions are made to d bride and pack the space more completely.
With the worldwide increase in tuberculosis and immigration of people from the Third World to North America, pulmonary tuberculosis may be seen in any thoracic surgical practice. Like scrofula, mycobacteria can cause a soft tissue infection of the chest wall. Hsu and colleagues reviewed its management in 1995. Patients present with a slowly enlarging painless mass on the chest wall. A CT scan is helpful to rule out the possibility of pulmonary involvement. Diagnosis can be made with a diagnostic aspiration of the abscess. Treatment should be combination antituberculous therapy for 6 to 9 months. Surgical d bridement is reserved for failures. If the diagnosis is not made before d bridement, a broad-spectrum antibiotic should be added. Fungal infections of the chest wall should also receive long-term antibiotic therapy, but radical d bridement is a mandatory part of the therapy.
Gangrene
Necrotizing soft tissue infections may occur as a complication of empyema or trauma. These infections frequently begin when the pleural material is drained through the soft tissues either by chest tube or thoracotomy. Pingleton and Jeter (1983) reported extensive synergistic gangrene of the chest wall with Bacteroides melaninogenicus and Streptococcus viridans after tube thoracostomy for empyema. Delay in recognition led to the patient's demise. This author and Vanecko (1985) reported destruction of the pectoralis major and serratus muscles that was caused by clostridial myonecrosis at the site of a tube thoracostomy in a patient with Boerhaave's syndrome. Radical d bridement and daily dressing changes under general anesthesia eventually led to a successful outcome. Viste and colleagues (1997) reported a case of necrotizing infection caused by gastric herniation after laparoscopic fundoplication. Urschel and associates (1997) reviewed the world literature and found a 90% mortality rate for this devastating problem. A more recent review by Losanoff and colleagues (2002) found that the mortality rate had decreased to 60%.
P.683
Infections of the head and neck as well as dental manipulation have been identified as sources of necrotizing fasciitis of the chest. Steel (1987) described a case of necrotizing ulceration of the chest wall after dental manipulation; it was successfully treated by surgical d bridement and chemotherapy. He noted that the primary suspect organisms were Streptococcus milleri and Bacteroides species. Nallathambi and colleagues (1987) reviewed the current literature and discovered 28 chest wall and mediastinal infections related to dental manipulation or pharyngeal abscesses. These rapidly progressive, mixed aerobic and anaerobic infections have been associated with a 32% mortality rate. Antibiotic prophylaxis for deep dental manipulations and careful follow-up for any early signs of sepsis are essential.
Early recognition, radical d bridement of all involved necrotic tissue, high-dose antibiotic therapy, prolonged ventilatory support, and delayed closure with biologic tissue represent the only salvation for these patients. The antibiotic of choice used to be single-drug treatment with high-dose penicillin, but many organisms of the normal flora above the diaphragm have become resistant to penicillin. Therapy should begin presumptively with a combination that includes penicillin or ampicillin, an aminoglycoside, and clindamycin or metronidazole. Once cultures and susceptibilities are available, the antibiotic regimen should be tailored accordingly.
INFECTIOUS CHEST WALL INVASION
With drug resistance and superinfection during antibiotic therapy, virulent organisms occasionally cause pneumonia that has the capability of direct chest wall invasion. Suchyta and associates (1987) reported a community-acquired chronic Acinetobacter calcoaceticus pneumonia with direct chest wall involvement discovered only at autopsy. Yuan and associates (1992) successfully treated a patient with pneumonia and extensive chest wall involvement attributed to Actinobacillus actinomycetemcomitans. This patient required high-dose penicillin therapy for 3 months. However, as Hseih and colleagues (1993) point out, Actinomyces species (i.e., israelii, naeslundii, and odontolyticus) infections usually respond to antibiotic (penicillin) therapy, and surgical intervention may not be necessary if pretherapeutic diagnosis can be made.
EMPYEMA NECESSITATIS
Infrequently seen today, the soft tissue infection called empyema necessitatis is caused by an undrained underlying pleural infection. An untreated empyema may eventually burrow through the chest wall and into the subcutaneous tissue of the chest. Suspicion of this entity should be raised by the patient's history and confirmed by physical and radiographic examination of the chest. The soft tissue component may require separate drainage but often resolves with appropriate drainage of the empyema.
MONDOR'S DISEASE
Mondor's disease is a benign condition consisting of localized thrombophlebitis occurring in the superficial veins of the breast and anterior chest wall. The true incidence of this entity is unknown. Reports have been infrequent. Because the condition produces few symptoms and signs, most examples are probably not referred to informed examiners for study.
The earliest description was by Fagge (1869). Williams (1931) attributed the disease to thrombophlebitis, as did Mondor (1939), for whom the condition is named. Most cases occur in women, and frequently no antecedent cause can be found. Radical mastectomy may predispose to the development of this disease, as Herrman (1966) proposed, whereas benign conditions, such as fibrocystic disease, have no association with this entity. In a few instances in which a biopsy was performed, Farrow (1955) described a sclerosing endophlebitis with complete or partial obliteration of the lumen.
Clinically, the disease presents as a cordlike structure in the subcutaneous tissue of the axilla, chest, or abdomen. Its greatest significance may be the possible confusion with inflammatory carcinoma of the breast. It does not tend to recur or lead to thromboembolism. In most subjects, no specific therapy is indicated because it regresses spontaneously.
MISCELLANEOUS INFECTIONS
Several other conditions may manifest as infections of the chest wall. Golladay and associates (1985) noted three benign conditions in 24 children who presented with chest wall masses. These included trichinosis, nodular fasciitis, and myositis ossificans, all confirmed by excisional biopsy. The latter two were almost certainly secondary to localized trauma.
Cartilage and Bony Structures
Tietze's Syndrome
Painful, nonsuppurative swelling of the costal cartilages without abnormal histologic change is referred to as Tietze's syndrome. This condition, which is not a disease, was described in two patients by Tietze (1921), who attributed the changes to tuberculosis. This has never been confirmed. Since Tietze's publication, case reports have been sporadic. Kayser (1956), who reviewed the world literature, could find only 156 cases.
The true frequency of this condition is not known, but the symptom complex appears to be common. Peyton (1983)
P.684
described 76 women in his office practice and 156 men and women visiting an emergency room who complained of this syndrome. Symptoms include chest pain and swelling of the costochondral junction. The junction, usually the second, is usually prominent and is tender to deep palpation. He noted that emotional tension is frequently associated with this symptom complex. In a study by Disla and colleagues (1994), of 122 consecutive patients with chest wall complaints presenting to the emergency room, 30% met criteria for diagnosis of costochondritis and 8% met the American College of Rheumatology criteria for fibromyalgia. After 1 year, 55% of the patients with costochondritis still had symptoms.
Rarely are further tests necessary to confirm this diagnosis, but Edelstein and colleagues (1985) pointed out that CT scan of the chest is helpful to exclude chest wall masses in these patients.
As might be expected for a condition as vague as this, several invasive treatments have been advocated, from hydrocortisone infiltration to surgical removal of the involved area. The latter hardly seems justified. In most patients, reassurance and symptomatic treatment with compounds containing ibuprofen are sufficient.
Costochondritis
Infections of the costal cartilage cause great debility. They are chronic beyond all expectation and thus demoralizing to the patient and the surgeon alike. When recognized and treated properly, response is rapid, but the required treatment is exceedingly radical for what appears to be such a minor problem. This often leads to delay in appropriate management. Recognizing the basic problem, Moschowitz (1918) pointed out that chronicity resulted less from the type of infecting organism than from the avascular nature of the cartilage. He correctly urged removal of the cartilage for cure.
Before 1940, most chondritis was spontaneous, usually caused by tuberculosis. Some cases were caused by typhoid or paratyphoid fever. Today most infections are surgical complications. Most follow median sternotomy performed for cardiac procedures; some follow thoracotomy, tube thoracostomy, or chest wall trauma. Occasionally, fungal infections may burrow through the chest wall to cause chondritis.
Because the fifth to ninth costal cartilages are contiguous or fused, infections involving any one of these segments dictate a major resection for cure. The xiphoid is partially a cartilaginous structure and thus may promote bilateral spread of the infection. This avascular hyaline cartilage behaves like a foreign body, once infected. When free of perichondrium, it begins to take on a moth-eaten appearance in the depths of a draining wound. The disintegration of the cartilage occurs slowly, but the cartilage is never completely reabsorbed. Sequestra that are characteristic of chronic osteomyelitis do not classically form in chondritis. The cartilage remains exposed and unmoved in the depths of the narrow, granulating wound.
Many organisms have been cultured from costochondritis. The primary infecting organisms include Escherichia coli, Streptococcus pneumoniae, Pseudomonas aeruginosa, Mycobacterium tuberculosis, staphylococci, streptococci, and Nocardia. Once the wound is opened and drained, subsequent cultures may grow a variety of organisms, depending on the environment and the antibiotic regimen the patient is receiving.
Usually, the disease manifests as a draining sinus in the region of the cartilages. Local pain and tenderness are present. As with any other chronic infection, general debility and, perhaps, low-grade fever accompany an elevated white cell count. In most patients, the diagnosis is confirmed by tenderness over the cartilages and infection in the vicinity.
The preferred therapy is radical excision, as Murphy (1916) and Moschowitz (1918) advocated. Any involved cartilage should be removed completely (Fig. 42-1). If the lower ribs are involved, all fused segments must be excised. No bare cartilage should remain in the infected wound. The more conservative approach is to pack the wound and reconstruct it later, as Lewis (1967) and Talucci and Webb (1983) advocated. Others, such as Hines and Lee (1983) and Arnold and Pairolero (1984), have shown that the defect may be closed in one stage with minimal morbidity. Techniques of reconstruction are discussed later in the chapter.
Osteomyelitis
Sternal Osteomyelitis
Although spontaneously appearing osteomyelitis of the sternum or ribs did occur when tuberculosis was prevalent, it is rare today. Even when tuberculosis was more common, osteomyelitis of the sternum was uncommon. In a series of more than 1,000 patients with bone and joint tuberculosis reported by Wassersug (1941), the sternum was involved in only 1.1%. Today, primary sternal osteomyelitis occurs in heroin addicts.
P.685
More often, secondary infections, usually after cardiac surgical procedures, are the etiologic factors. Ochsner and associates (1972) noted a 1.5% infection rate with an overall 10% mortality rate. Rates today are similar.
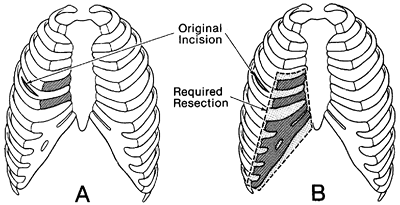 |
Fig. 42-1. Cartilage resection necessary for proper treatment of costochondritis. A. Initial incision and costal involvement. B. Delay may lead to secondary costal arch involvement, necessitating arch removal. |
The factors implicated in the development of postoperative sternal infections, enumerated by Talamonti and associates (1987), include diabetes, low cardiac output, use of bilateral internal thoracic artery grafts, and, most significantly, reoperation for excessive postoperative bleeding.
Manifestations of this condition are similar to those of chondritis. When osteomyelitis involves the sternum, an associated chondritis may occur, which can be mistaken for the principal cause of chronicity. The first sign of postoperative sternal osteomyelitis may be an unstable sternum or serosanguineous discharge. Novick and Fishman (2003) pointed out several findings on spiral CT that can be beneficial in determining if a patient has associated mediastinitis with a sternal infection. The most common findings were fat hyperdensity and stranding, fluid collections and mass effect at the level of the great vessel origin from the aortic arch.
In chronic sternal osteomyelitis, the most successful results have been achieved by extensive sternal and chondral removal followed by myocutaneous reconstruction. The most commonly used reconstruction is bilateral pectoralis major flap advancement, as described by Johnson and associates (1985). A modified H incision is used to mobilize the pectoralis major muscles, with the blood supply based on the thoracoacromial artery (Fig. 42-2A). This also allows adequate exposure of the sternum, which is then excised (Fig. 42-2B). If possible, the upper manubrium with the clavicular attachments is left intact. This prevents skeletal problems as the shoulders rotate anteriorly and inferiorly. Next, the humeral heads of the pectoralis major muscles are transected, and the flaps are advanced over drains to close the defect (Fig. 42-2C). This gives a good cosmetic result with preservation of pulmonary function.
Rib Osteomyelitis
Diagnosis of osteomyelitis of the ribs is usually made because of local inflammatory signs and symptoms or because of a persistently draining sinus. When the infection is secondary to open drainage of an empyema, it can be one cause of a slowly healing wound. Sequestration from ribs affected by osteomyelitis has been reported. The sequestrum may even pass into the lungs, as Roe and Benioff (1955) noted. Recently, Chang and colleagues (1999) reported on a series of 12 patients with tuberculous rib osteomyelitis.
Confirmation is usually made by chest radiography. Although CT scanning of the chest is usually not necessary for confirmation of the diagnosis, it may help in evaluating possible underlying associated intrathoracic pathology, as suggested by Wechsler and Steiner (1989).
Excision of all diseased bone usually provides adequate treatment for osteomyelitis of the ribs. To prevent the problem after empyema drainage, Churchill (1929) recommended a
P.686
clean division of the ribs, leaving no rib exposed or unprotected by periosteum. Occasionally, extensive excision may be required. In patients in whom the infection is overwhelming and an extensive excision is required, mechanical ventilation may be necessary until the infection is obliterated and reconstruction can be safely attempted.
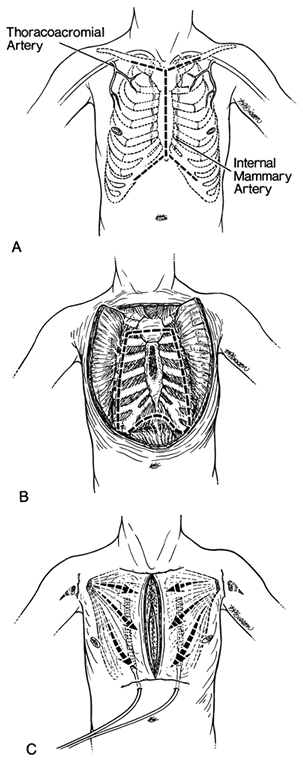 |
Fig. 42-2. Depiction of one-stage operation for chronic sternal osteomyelitis. A. The H-shaped incision used to expose the sternum and costal cartilages. B. Bilateral pectoralis major myocutaneous flaps have been raised. The extent of the planned resection is shown. C. Humeral detachment of the pectoralis muscles with advancement and closure over suction drains. From Johnson P, et al: Management of chronic sternal osteomyelitis. Ann Thorac Surg 40:69, 1985. With permission. |
Sternoclavicular Osteomyelitis
Sternoclavicular osteomyelitis is a relatively new problem that occurs not only in addicts but also in individuals who have had subclavian catheters, as well as in patients with no known antecedent interventions. However, as Haddad and colleagues (2002) report, the latter group is usually ill, either with a chronic debilitating illness such as diabetes mellitus or liver failure or an overwhelming acute illness such as sepsis from a remote site.
The inciting organisms vary widely, depending on the etiology. In my experience, both gram-positive organisms, such as Staphylococcus and group B Streptococcus, and gram-negative organisms cause these infections. Buescher and colleagues (1994) recorded a case of Aspergillus infection in a patient undergoing chemotherapy for acute myelogenous leukemia. An interesting report by Berrocal and associates (1993) from Peru found 7 cases of brucellar sternoclavicular arthritis among 1,729 cases of primary brucellosis.
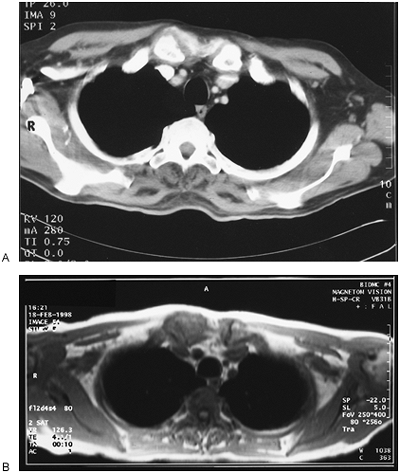 |
Fig. 42-3. Computed tomographic (CT) and magnetic resonance (MR) imaging scans of a patient with sternoclavicular osteomyelitis. The changes on CT scan are subtler than the changes seen on MR imaging. A. The CT scan shows the right sternoclavicular joint with some minimal swelling around it and bony erosion that looks nearly the same as the opposite side. B. The MR imaging is more striking, with obliteration of the cartilage of the clavicular head with striking soft tissue involvement. |
These patients present with fever and severe unremitting pain in the joint. Some patients even demonstrate instability of the joint and have difficulty lifting objects and even writing in severe cases. Routine radiographs are not helpful. Even CT scans may be of little help. These scans may not show much bony destruction because the damage begins in the joint (Fig. 42-3A). The condition must be inferred from the surrounding soft tissue involvement. Magnetic resonance (MR) imaging is a much more sensitive tool than CT for detecting joint disease and therefore presents a more dramatic image (Fig. 42-3B). The joint as well as the soft tissue swelling is more clearly defined.
Treatment requires the same radical d bridement as other cases reported here. To remove the joint completely and any possibility of recurrence, one must bear in mind that the sternoclavicular joint is contiguous with the clavicle, sternum, and first rib. This area should be removed en bloc. To create the best closure, removal of a portion of the second rib is helpful, whether it is involved or not. A trapdoor incision is made beginning above the clavicle, extending to the midline, down the midline, and across the anterior chest below the disease, usually the third rib. A flap is made, including the pectoralis muscle. Sometimes, it is involved in the infection and a portion must be sacrificed, but every effort should be made to salvage as much of it as possible. The internal thoracic artery and vein are ligated above the third rib. The platysma and scalene muscles are divided above and the sternum is bisected to the third rib. The second and third ribs are divided beyond the infection, and the clavicle is cut in half or more. The first rib is cleared at this point and divided. The specimen is removed and cultures taken before sending the specimen to the pathology laboratory. Closed suction drains are placed, and the flap is advanced into place with interrupted sutures. Foreign material or mesh should be avoided. The long-term result is excellent for both infection control and chest wall function (Fig. 42-4). Burkhart and associates (2003) reported on 26 patients with a complication rate of 7.7% and a mortality rate of 3.8%.
Osteoradionecrosis
One of the most difficult problems encountered by the thoracic surgeon is a large necrotic ulcer of the chest wall after radiation therapy for carcinoma of the breast or other condition. Often, more infection and necrosis exist than are visible externally. Prosthetic materials usually cannot be used in the infected field. With radiation becoming a standard in the minimal surgical techniques of breast cancer, and despite all the precautions taken by radiation therapists, these problems are on the rise. Treatment requires close cooperation between the thoracic surgeon and the plastic and reconstructive surgeon.
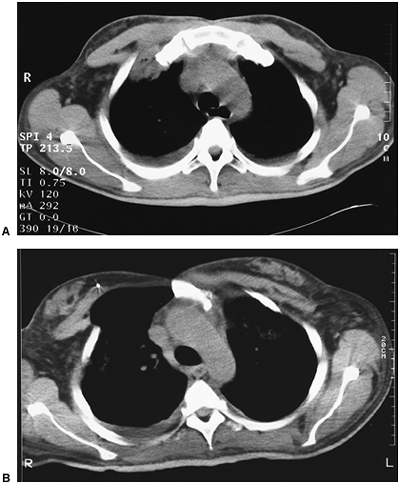 |
Fig. 42-4. Before and after computed tomographic scans of a patient with sternoclavicular osteomyelitis. A. Subtle bony changes are associated with soft tissue fluid collection. B. Two years after resection and primary closure, the hemisternum is healed, and the pectoralis muscle covers the defect to the midline. |
P.687
The foremost principle in the treatment of a radionecrotic ulcer is wide surgical excision and primary coverage of the defect, as Arnold and Pairolero (1984, 1989) described. Tissue of the affected area should be sent for pathologic analysis when radiation was performed for a local malignancy to ensure that no residual tumor is present.
Provisions for covering the expected defect with viable tissue must be carefully considered before the surgical procedure. Understanding and use of myocutaneous flaps have advanced. Jurkiewicz and colleagues (1980) described a variety of flaps, including pectoralis major, rectus abdominis, and latissimus dorsi flaps (Fig. 42-5). Other innovative flaps include segmentally split pectoral girdle flaps [proposed by Tobin (1990)] and free extended forearm flaps [suggested by Schmidt and colleagues (1987)].
The latissimus flap was first described by Tansini (1906) but was rediscovered by McCraw and colleagues (1978). Hines and Lee (1983) used this flap in five patients and noted that even if the primary blood supply the thoracodorsal artery was cut at the time of initial mastectomy, collateral blood supply appeared adequate. They also pointed out that the muscle, albeit smaller and thinner when the thoracodorsal nerve has been resected, remains usable. Within the past few years, plastic and reconstructive surgeons have applied microvascular techniques to this flap. Free flaps have been used with great success, with and without the associated skin as well as inside the chest, as reported by Hammond and associates (1993) and outside the chest as described by Hidalgo and colleagues (1993).
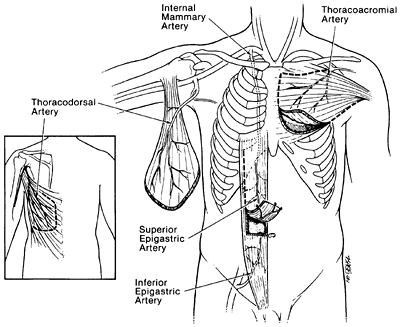 |
Fig. 42-5. Representation of the most common myocutaneous muscle flaps with their individual blood supply used for chest wall reconstruction. |
In most instances, foreign material should be avoided when infection is present. Usually, the resulting paradoxic movement of the chest wall in these patients is minimally debilitating and not worth the risk for secondary infection. Myocutaneous flaps have been beneficial when a large portion of the chest wall or sternum must be removed (see Chapter 47).
IMMUNOCOMPROMISED PATIENTS
Patients who are immunocompromised because of malignancy, malnutrition, or human immunodeficiency virus infection present special problems. In granulocytopenic patients, findings of severe chest wall infections may be subtle. Aranha and co-workers (1988) recommend antibiotic therapy and surgical d bridement with the early findings of erythema, localized tenderness, and temperature elevation. Golladay and Baker (1987) note that in immunocompromised children, invasive aspergillosis is the offending infection one third of the time, with high mortality rates even with early aggressive intervention.
In patients infected with human immunodeficiency virus, common organisms often cause serious chest wall infection. Martos and colleagues (1989) reported two cases of tuberculosis of the chest wall. Rodriguez-Barradas and associates (1992) found chest wall infections related to pneumococcal pneumonia. Asai and colleagues (2003) reported on a patient with mucormycosis during antileukemia therapy.
P.688
Despite the uniformly fatal nature of the underlying disease, standard surgical principles of aggressive d bridement and antibiotic therapy result in gratifyingly good long-term results.
REFERENCES
Arnold PG, Pairolero PC: Chest wall reconstruction. Experience with 100 consecutive patients. Ann Surg 199:725, 1984.
Arnold PG, Pairolero PC: Intrathoracic muscle flaps: a 10-year experience in the management of life threatening infections. Plast Reconstruct Surg 84:92, 1989.
Aranha GV, et al: Soft tissue infections in the compromised host. Am Surg 54:463, 1988.
Asai K, et al: Pulmonary resection with chest wall removal and reconstruction for invasive pulmonary mucormycosis during antileukemia chemotherapy. Jpn J Thorac Cardiovasc Surg 51:163, 2003.
Berrocal A, et al: Sternoclavicular brucellar arthritis: a report of 7 cases and a review of the literature. J Rheumatol 20:1184, 1993.
Buescher TM, Moritz DM, Killyon GW: Resection of the chest wall and central veins for invasive cutaneous aspergillus infection in an immunocompromised patient. Chest 105:1283, 1994.
Burkhart HM, et al: Surgical management of sternoclavicular joint infections. J Thorac Cardiovasc Surg 125:945, 2003
Chang JH, Kim SK, Lee WY: Diagnostic issues in tuberculosis of the ribs with a review of 12 surgically proven cases. Respirology 4:249, 1999.
Churchill E: The technic of rib resection and osteomyelitis of the rib ends. JAMA 92:644, 1929.
Disla E, et al: Costochondritis. A prospective analysis in an emergency department setting. Arch Intern Med 154:2466, 1994.
Edelstein G, et al: CT observation of rib abnormalities: spectrum of findings. J Comput Assist Tomogr 9:65, 1985.
Fagge CH: Remarks on certain cutaneous affections: with cases. Guy Hosp Rep 15:259, 1869.
Farrow JH: Thrombophlebitis of the superficial veins of the breast and anterior chest wall (Mondor's disease). Surg Gynecol Obstet 101:63, 1955.
Golladay ES, Baker SB: Invasive aspergillosis in children. J Pediatr Surg 22:504, 1987.
Golladay ES, et al: Chest wall masses in children. South Med J 78:292, 1985.
Haddad M, Maziak DE, Shamji FM: Spontaneous sternoclavicular joint infections. Ann Thorac Surg 74:1225, 2002.
Hammond DC, Fisher J, Meland NB: Intrathoracic free flaps. Plast Reconstr Surg 91:1259, 1993.
Herrman JB: Thrombophlebitis of breast and contiguous thoracoabdominal wall (Mondor's disease). NY State J Med 66:3146, 1966.
Hidalgo DA, Saldana EF, Rusch VW: Free flap chest wall reconstruction for recurrent breast cancer and radiation ulcers. Ann Plast Surg 30:375, 1993.
Hines GL, Lee G: Osteoradionecrosis of the chest wall: management of post resection defects using Marlex mesh and a rotated latissimus dorsi: myocutaneous flap. Am Surg 49:608, 1983.
Hseih MJ, et al: Thoracic actinomycosis. Chest 104:366, 1993.
Hsu HS, et al: Management of primary chest wall tuberculosis. Scand J Thorac Cardiovasc Surg 29:119, 1995.
Johnson P, et al: Management of chronic sternal osteomyelitis. Ann Thorac Surg 40:69, 1985.
Jurkiewicz MJ, et al: Infected median sternotomy wound: successful treatment by muscle flaps. Ann Surg 191:738, 1980.
Kayser HL: Tietze's syndrome: a review of the literature. Am J Med 21:982, 1956.
Lewis FJ: Chondritis as a postoperative complication. Lancet 87:247, 1967.
LoCicero J III, Vanecko RM: Clostridial myonecrosis of the chest wall complicating spontaneous esophageal rupture. Ann Thorac Surg 40:396, 1985.
Losanoff JE, Richman BW, Jones JW: Necrotizing soft tissue infection of the chest wall. J Cardiovasc Surg (Torino) 43:549, 2002
Martos JA, et al: Chondrocostal and chondrosternal tuberculosis in two heroin addicts infected with human immunodeficiency virus. Med Clin (Barc) 93:467, 1989.
McCraw JB, Penix JO, Baker JW: Repair of major defects of chest wall and spine with a latissimus dorsi myocutaneous flap. Plast Reconstr Surg 62:197, 1978.
Mondor MH: Tronculite soucutane subaigue de la paroi thoracique anteo-laterale. Mem Acad Chir 65:1271, 1939.
Moschowitz A: The treatment of diseases of the costal cartilages. Ann Surg 68:168, 1918.
Murphy JB: Bone and joint diseases in relation to typhoid fever. Surg Gynecol Obstet 23:119, 1916.
Nallathambi MN, et al: Craniocervical necrotizing fasciitis: critical factors in management. Can J Surg 30:61, 1987.
Novick SL, Fishman EK: Anterior mediastinal extension of primary chest wall infections: role of spiral CT in detection and management. Crit Rev Comput Tomogr 44:79, 2003.
Ochsner JL, Mills NL, Woolverton WC: Disruption and infection of the median sternotomy incision. J Cardiovasc Surg 13:394, 1972.
Peyton FW: Unexpected frequency of idiopathic costochondral pain. Obstet Gynecol 62:605, 1983.
Pingleton SK, Jeter J: Necrotizing fasciitis as a complication of tube thoracostomy. Chest 83:925, 1983.
Rodriguez-Barradas MC, et al: Unusual manifestations of pneumococcal infection in human immunodeficiency virus-infected individuals: the past revisited. Clin Infect Dis 14:192, 1992.
Roe BB, Benioff MA: Late hemoptysis from rib sequestrum thirty-four years following empyema drainage. Surgery 38:764, 1955.
Schmidt RG, Springfield DS, Dell PC: Chest wall reconstruction with a free extended forearm flap: a case report. J Reconstr Microsurg 3:189, 1987.
Steel A: An unusual case of necrotizing fasciitis. Br J Oral Maxillofac Surg 25:328, 1987.
Suchyta MR, Peters JI, Black RD: Chronic Acinetobacter calcoaceticus var anitratus pneumonia. Am J Med Sci 294:117, 1987.
Talamonti MS, et al: Early reexploration for excessive postoperative bleeding lowers wound complication rates in open heart surgery. Am J Surg 53:102, 1987.
Talucci RC, Webb WR: Costal chondritis of the costal arch. Ann Thorac Surg 35:318, 1983.
Tansini I: Sopra il mio nuovo processo di amputazione dell mammella. Riforma Medica (Palermo) 12:757, 1906.
Tietze A: Ueber eine eigenartige Haufung von Fallen mit Dystrophie der Rippenknorpel. Berl Klin Wochenschr 58:829, 1921.
Tobin GR: Segmentally split pectoral girdle muscle flaps for chest wall and intrathoracic reconstruction. Clin Plast Surg 17:683, 1990.
Urschel JD, et al: Necrotizing soft tissue infections of the chest wall. Ann Thorac Surg 64:276, 1997.
Viste A, Vidnenes H, Gjerde S: Herniation of the stomach and necrotizing chest wall infection following laparoscopic Nissen fundoplication. Surg Endosc 11:1029, 1997.
Wassersug JD: Tuberculosis of the sternum. N Engl J Med 225:445, 1941.
Wechsler RJ, Steiner RM: Cross sectional imaging of the chest wall. J Thorac Imaging 4:29, 1989.
Williams GA: Thoraco-epigastric phlebitis producing dyspnea. JAMA 96: 2196, 1931.
Yuan A, et al: Actinobacillus actinomycetemcomitans pneumonia with chest wall involvement and rib destruction. Chest 101:1450, 1992.
Reading References
Arnold PG, Pairolero PC: Chest wall reconstruction: experience with 100 consecutive patients. Ann Surg 199:725, 1984.
Culliford AT, et al: Sternal and costochondral infections following open heart surgery. J Thorac Cardiovasc Surg 72:714, 1976.
EAN: 2147483647
Pages: 203