119 - Uncommon Primary Malignant Tumors of the Lung
Editors: Shields, Thomas W.; LoCicero, Joseph; Ponn, Ronald B.; Rusch, Valerie W.
Title: General Thoracic Surgery, 6th Edition
Copyright 2005 Lippincott Williams & Wilkins
> Table of Contents > Volume II > The Esophagus > Section XXII - Trauma to the Esophagus > Chapter 137 - Foreign Bodies in the Esophagus
Chapter 137
Foreign Bodies in the Esophagus
Christian G. Stevoff
Robert M. Craig
Foreign bodies in the esophagus can be classified into four categories. The first is the purposeful ingestion of a foreign body either by a child or psychiatric patient. The second is accidental ingestion of a foreign body, usually in food. The third is the impaction of a foreign body in an obstructed element in the esophagus. And the fourth is the so-called steak house syndrome, in which a bolus, usually meat, is obstructed at the distal end of the esophagus. The diagnosis and management of each are described separately. The importance of early diagnosis and treatment of esophageal obstruction from a foreign body is attested by the high mortality that attends a perforated esophagus that may ensue if these disorders are not managed appropriately. Whereas most foreign bodies pass through the gastrointestinal tract, as many as 15% to 20% lodge in the esophagus or more distally in the gastrointestinal tract, may require surgery, and occasionally result in death. Bloom and colleagues (1986) point out that most of the foreign bodies that fail to pass through the gastrointestinal tract lodge in the esophagus.
PURPOSEFUL INGESTION OF A FOREIGN BODY
The first major cause of foreign bodies in the esophagus is the purposeful ingestion of foreign bodies. Infants or children are prone to ingest many types of foreign bodies, but the ingestion of alkaline batteries is particularly troublesome, as indicated by Temple and McNeese (1983) and by Votteler (1983) and Blatnik (1977) and their colleagues. Kost and Shapiro (1987) noted that the hazard from these batteries may result from electrolyte leakage, pressure necrosis, mercury toxicity, or the alkali within the batteries. Litovitz (1985) pointed out that hearing aid batteries are the most common battery ingestion. The alkaline batteries may have a corrosive action in the esophagus from the release of concentrated potassium hydroxide, and can produce perforation and mediastinitis. Studley and co workers (1990) noted the lack of a consensus on management among surveyed pediatricians, with half believing that the battery can be followed radiographically through the gastrointestinal tract. We believe, however, that the risks of endoscopic removal are so low and the potential hazards so high that these small alkaline batteries should be removed endoscopically from the esophagus as quickly as possible. This is supported by Webb (1995). Litovitz and Schmitz (1992) reviewed 2,382 cases of button battery ingestion from the national register and noted the benign course overall, with no deaths and only two patients having a bad outcome, each with the battery lodged in the esophagus. They cautioned against using ipecac, because the induction of forceful vomiting could be traumatic.
The series by Chaikhouni and associates (1985), Jackson (1957), and Bakara and Bikhazi (1975) stressed the high frequency of coin ingestion by children. Webb (1995) and Ginsberg (1995) stressed that most coins, especially dimes, pennies, and nickels, pass through the gastrointestinal tract if they pass into the stomach, and that they can be followed radiographically once esophageal transit has been confirmed. Esophageal coins should be removed urgently. Kelley and colleagues (1993) described a technique involving a Foley catheter for removal of proximal esophageal coins, but this seems somewhat cumbersome compared with endoscopic techniques. Adams (1986) reported an unusual patient with a foreign body entrapped in a duodenal diverticulum for 20 years, which was removed endoscopically.
Burton and Smith (1992) reported that esophageal perforation can occur, even with a blunt foreign body. Children or psychiatric patients may also swallow sharp objects, including pins, razor blades, and toothpicks, which can become some of the most difficult objects to address. Carp (1950) recorded that often these objects pass into the stomach, but Brady (1991) noted that they can lodge at the level of the thoracic arch, at the gastroesophageal junction, or in the hypopharynx. Safety pins can be removed by placing a forceps through the open ring of the safety pin and opening the forceps so that it can be pulled out with the endoscope smooth side first (Fig. 137-1). In addition, an overtube can facilitate the removal of safety pins or other sharp objects. Foreign body retrievers and baskets, especially the Roth basket, have been used successfully in the removal of coins or other objects.
P.2096
Iafrati and associates (1996) reported a novel combination of upper endoscopy in combination with laparoscopic removal of large bedsprings that were purposefully ingested and had perforated the stomach. Kamal and colleagues (1999) reported on the difficulty of vinyl glove ingestions, because they fragment upon attempted removal.
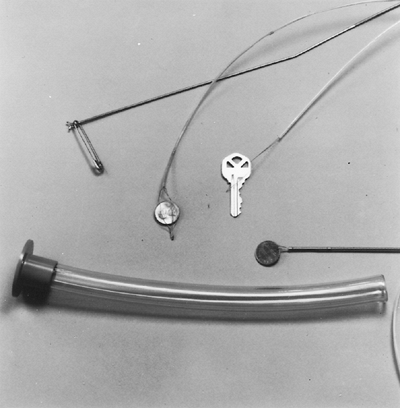 |
Fig. 137-1. Various techniques used for removing foreign bodies through the fiberendoscope. The overtube can be left in place as the endoscope is removed and reintroduced for removal of a meat bolus or as a protective mechanism for sharp objects. A forceps can be opened up after it is introduced into the eye of a safety pin. Baskets or foreign body graspers can be used for coins. A snare can be used for a key or a similar asymmetric foreign body. |
Gracia and associates (1984) and Velitchkov and colleagues (1996) stressed that most foreign bodies pass into the stomach, but 38 of Gracia's 87 patients had the foreign body lodge in the esophagus. Most series, such as those of Webb (1995), Bloom and associates (1986), and Spitz (1971), showed that the endoscopic removal of these foreign bodies is successful about 80% of the time. Bendig (1986) described 23 consecutive pediatric patients with blunt foreign bodies in whom he was able to push the foreign body into the stomach in 5 and remove the foreign body endoscopically in the other 18. Narcotics have been smuggled into the United States by body packers. Usually cocaine is swallowed in a condom bag, and retrieved later through the feces. This process is hazardous because of the high concentration of narcotic transported. Chan and co-workers (1997) described a patient who consumed a blister pack with narcotics that lodged at the ileocecal valve area and induced hemorrhage. Webb (1995) and Ginsberg (1995) assert that no endoscopic attempt at removal of the packs, either by upper endoscopy or colonoscopy, should be attempted because their rupture could prove fatal.
FOREIGN BODIES INGESTED WITH FOOD
The second category of esophageal foreign body is the inadvertent ingestion of a foreign body. Most series of esophageal perforation, such as those reported by Haglund (1978) and Chaikhouni (1985) and their associates, Jackson (1957), and Bakara and Bikhazi (1975), demonstrated that foreign bodies occur more frequently in the elderly and in children. Edentulous patients should be questioned as to how well their dentures fit, because poorly fitting dentures often are responsible for the swallowing of foreign bodies. In Nandi and Ong's (1978) review of 2,394 patients with esophageal foreign bodies, chicken and fish bones were the most common in adults; fish bones and coins were the most frequent foreign bodies in children. Newell and associates (2000) reported on the hazards of the accidental ingestion of plastic bread clips, which may lodge at the level of the ileocecal valve. The foreign body, especially a fish bone, is often lodged in the cervical esophagus, and the patient may note a feeling of being scratched in the hypopharynx. Under these circumstances, an evaluation by an otolaryngologist often reveals the source of the problem. Sometimes patients complain only of dysphagia but often odynophagia is significant if the foreign body is lodged in the esophagus. This large series included 24 perforations with three deaths attributable to mediastinal abscess or aortoenteric fistula, chicken or fish bones being the major culprits. Maglinte and co workers (1979) also stressed the danger of chicken bone foreign bodies, although their perforations occurred after passage from the esophagus into the stomach and the intestines. According to Maleki and Evans (1970), less than 1% of ingested foreign bodies results in either esophageal or intestinal perforation.
Diagnosis
A radiograph of the chest and of the neck is obtained first to locate the foreign body if indeed it is radiopaque (Figs. 137-2 and 137-3). Cheng and Tam (1999), however, stress the insensitivity of simple radiographs. Takada and co-workers (2000) emphasize that CT scanning is more useful in identifying foreign bodies, but Eng and colleagues (1999) report the insensitivity of CT scans in identifying body stuffing. A hand held metal detector has been useful in experienced hands in identifying metallic foreign bodies, as discussed by Seikel and associates (1999) and Bassett and colleagues (1999). If the patient has fever or leukocytosis, it is necessary to consider an esophageal perforation. Under these circumstances, a chest surgeon should be consulted and a CT scan of the chest should be obtained prior to attempted endoscopic removal of the foreign body. Physical examination should reveal crepitation in the neck, which
P.2097
would signal an esophageal perforation. Mediastinal air may be noted on the plain film radiograph, eliminating the need for a contrast enhanced study prior to mediastinal drainage.
 |
Fig. 137-2. A radiopaque chicken bone is evident in the cervical esophagus. |
If an obvious perforation is not apparent from the radiograph, water-soluble contrast administration followed by barium studies may be performed, as advised by Rosoff and White (1974) and Jones and Samson (1975), although the radiologist should use as little as possible to yield the diagnosis so that large quantities of contrast material do not fill the mediastinum. Haglund and co workers (1978) reported that radiologic diagnosis of the esophageal foreign body was accurate, with only one false negative evaluation and only 43 false positive examinations in their series of 264 Swedish patients.
 |
Fig. 137-3. A coin is evident in the cervical esophagus. |
Treatment
Following the initial evaluation, endoscopic removal of the foreign body from the esophagus should be attempted. As stated by Rogers and associates (1982), the availability of an overtube into which the foreign body can be introduced is also advisable, particularly for pins or coins (see Fig. 137-1). A latex protector hood may also be used, fashioned over the endoscope, as pointed out by Bertoni and co-workers (1996). It is preferable to have all of the necessary equipment lined up prior to the procedure. Toothpicks, fish bones, and chicken bones often can be removed with a snare or a basket without the use of an overtube. In the event of possible perforation of the esophagus, it is wise to notify a chest surgical consultant that the procedure is planned.
Although it is somewhat controversial whether to use a rigid esophagoscope or a flexible fiberoptic endoscope, most researchers, including Rosch and Classen (1972), Kline (1974), and DeLuca (1976) and Ricote (1985) and their associates, believe the latter is safer and should be used first. In a prospective randomized trial comparing a flexible gastroscope to a bronchoscope, Chu and colleagues (1998) found the flexible gastroscope superior. In the series by Ricote and associates (1985), 94% of patients with upper gastrointestinal foreign bodies underwent successful removal with the fiberoptic endoscope. Similarly Kim and co workers (1999) reported a 99% success rate with endoscopic therapy in children. In general, the endoscopic removal of these foreign bodies from the esophagus is relatively simple and nontraumatic. Schwarz and Polsky (1976) described the successful surgical removal of esophageal foreign bodies in seven patients, indicating that the necessity of surgical removal is unusual, generally precluded by successful endoscopic management. If significant edema in the esophagus restricts visibility, the possibility of an inflammatory process secondary to esophageal perforation should be considered. Removal of the endoscope and a reassessment of the situation, including a surgical consultation and a CT scan of the chest, is in order. Perforation of the esophagus carries a grave prognosis. If an esophagoaortic fistula ensues, the patient rarely survives. Ctercteko and Mok (1980) reported on a patient in whom an aortoesophageal fistula was treated successfully by surgery, but reviewed 86 previously reported patients, all with fatal outcome.
PRESENCE OF UNDERLYING ESOPHAGEAL DISEASE
The third situation in which foreign bodies can become impaled in the esophagus is the presence of obstructing esophageal diseases. As pointed out by Bakara and Bikhazi (1975),
P.2098
most adults have a predisposing cause for the occurrence of a foreign body lodging in the esophagus. Carcinoma of the esophagus and esophageal stricture secondary to gastroesophageal reflux present with symptoms of progressive obstructive dysphagia. Esophageal carcinoma often has associated odynophagia. Gastroesophageal reflux is suggested by a long history of heartburn followed by the progressive obstructive dysphagia. If the patient has poorly fitting dentures or eats something that is of a larger caliber than the lumen size, total obstructive dysphagia ensues. In these patients, the history often suggests some organic obstruction before the acute circumstance. If nothing suggests perforation in the patient's history or physical examination, the patient can undergo a flexible fiberoptic esophagoscopic examination. Usually, the food bolus or the foreign body can be maneuvered gently beyond the obstructing area with the endoscope. The safety of this technique has to be judged by the expertise and experience of the endoscopist. If too much pressure has to be exerted to move the bolus through the obstruction, the obstructing object has to be removed piecemeal through the endoscope. Often, the use of an overtube can facilitate this process. Pieces of an obstructing meat bolus can be removed with a biopsy forceps, a snare, or a basket. Following the removal of the foreign body, the patient should undergo gradual dilation of the esophageal stricture or of the obstructing carcinoma.
 |
Fig. 137-4. A meat bolus is seen above a lower esophageal ring. |
Esophageal rings and webs may also cause secondary obstruction by foreign bodies, mostly food, lodging in the esophagus. Figure 137-4 shows a meat bolus behind a lower esophageal ring. The lower esophageal ring seen endoscopically can be dilated with esophageal dilators (Fig. 137-5). Sometimes the indentation of the aortic knob is enough to cause some obstruction in the proximal esophagus on which food or foreign bodies can lodge. More recently, Opper and associates (1990) and Buto and colleagues (1990), respectively, reported guar gum used for obesity control and bay leaves to have caused acute esophageal obstruction.
STEAK HOUSE SYNDROME
The fourth situation in which foreign bodies can lodge in the esophagus is the so called steak house syndrome that was reported by Hargrove and Boyce (1970). The patient presents with intermittent total obstructive dysphagia. The syndrome usually occurs while the patient has been eating quickly, often swallowing incompletely chewed meat, and frequently after the consumption of alcoholic beverages. The patient notes
P.2099
that the meat becomes stuck and he or she is unable to swallow anything, including saliva. Sometimes, the meat bolus can be regurgitated or can be forced through the lower end of the esophagus with Valsalva maneuvers or by drinking large quantities of water. The patient often visits an emergency room necessitating the emergent removal of the bolus.
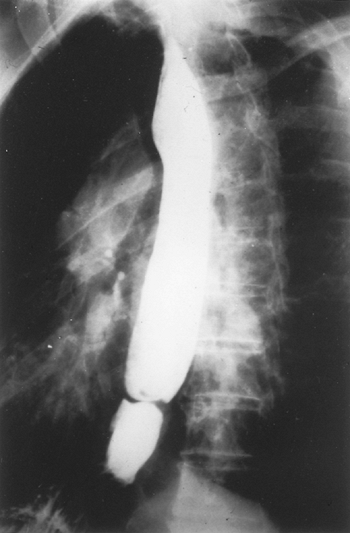 |
Fig. 137-5. A lower esophageal ring seen endoscopically following the passage of the meat bolus. |
Glucagon can be tried, and Ferrucci and Long (1977) report that this has been successful in some patients. Smith and colleagues (1986) described two patients with the successful egress of esophageal food impactions with glucagon in combination with a gas-forming agent given orally. In our experience, however, it is generally unsuccessful in relaxing the lower end of the esophagus to permit discharge into the stomach. This view is supported by Trenkner and associates (1983), who reported only 37% success with this technique.
The use of papain has been suggested by some researchers, including Richardson (1945), Jones and Samson (1975), and Hargrove and Boyce (1970), but it is inadvisable, because perforations have occurred with its use, as reported by Holsinger (1968), Cavo (1977), and Anderson (1959) and their co workers.
Sawyers (1975) and Cavo (1977) and their colleagues noted that if there are no signs or symptoms suggesting esophageal perforation, the food bolus can be removed with flexible fiberoptic esophagoscopy, which has a complication rate of less than 1%. Usually, gentle manipulation of the endoscope along the side of the food bolus permits the endoscopist gradually to push the food bolus into the stomach, as pointed out by Vicari and associates (2001) and Longstreth and colleagues (2001). Thereafter, the food bolus goes through the gastrointestinal tract without difficulty. If the food bolus cannot be pushed safely into the stomach, it must be removed piecemeal with forceps, baskets, or snares. The use of an overtube can facilitate this process, as it will preclude the necessity to reintubate the esophagus following the removal of parts of the food bolus. Neustater and Barkin (1996) recently reported the use of a Roth basket to facilitate the removal of a large esophageal food bolus.
This syndrome should be differentiated from the acute occlusion of the airway that also occurs during meals, the so-called caf coronary, which may require the immediate dislodgment of the bolus with a Heimlich maneuver, as Haugen (1963) emphasized.
CONCLUSION
Foreign bodies of the esophagus should be removed endoscopically after appropriate radiologic investigations. The possibility of an esophageal perforation secondary to the foreign body should always be entertained, particularly if the foreign body is sharp. If there is evidence of esophageal perforation, the attempted removal of the foreign body should proceed only with the advice and consent of a surgical colleague.
REFERENCES
Adams DB: Endoscopic removal of entrapped coins from an intraluminal diverticulum 20 years after ingestion. Gastrointest Endosc 32:415,1986.
Anderson HA, et al: Perforation of the esophagus after use of a digestive agent: report of a case and experimental study. Ann Otol Rhinol 68:890, 1959.
Bakara A, Bikhazi G: Oesophageal foreign bodies. BMJ 1:561, 1975.
Bassett KE, Schunk JE, Logan L: Localizing metal coins with a metal detector. Am J Emerg Med 17:338,1999.
Bendig DW: Removal of blunt esophageal foreign bodies by flexible endoscopy with general anesthesia. Am J Dis Child 140:789, 1986.
Bertoni G, et al: A simple latex protector hood for safe endoscopic removal of sharp-pointed gastrointestinal foreign bodies. Gastrointest Endosc 44:458, 1996.
Blatnik DS, Toohill RJ, Lehrman RH: Fatal complication from an alkaline battery foreign in the esophagus. Ann Otol Rhinol Laryngol 86:611, 1977.
Bloom RR, et al: Foreign bodies of the gastrointestinal tract. Am Surg 52:618, 1986.
Brady PG: Esophageal foreign bodies. Gastrointest Clin North Am 20:691, 1991.
Burton DM, Smith JA: Extraluminal esophageal coin erosion in children. Case report and review. Int J Pediatr Otorhinolaryngol 23:187, 1992.
Buto SK, et al: Bay leaf impaction in the esophagus and hypopharynx. Ann Intern Med 113:82, 1990.
Carp L: Foreign bodies in the gastrointestinal tract of psychotic patients. Arch Surg 60:1055, 1950.
Cavo JW Jr, Koops HJ, Gryboski RA: Use of enzymes for meat impaction in the esophagus. Laryngoscope 87:630, 1977.
Chaikhouni A, Kratz JM, Crawford FA: Foreign bodies of the esophagus. Am Surg 51:173, 1985.
Chan FKL, et al: Blister pack induced gastrointestinal hemorrhage. Am J Gastroenterol 92:172, 1997.
Cheng W, Tam PKH: Foreign body ingestion in children: experience with 1265 cases. J Pediatr Surg 34:1472, 1999.
Chu K-M, et al: A prospective randomized trial comparing the use of the flexible gastroscope versus the bronchoscope in the management of foreign body ingestion. Gastrointest Endosc 47:23, 1998.
Ctercteko G, Mok CK: Aorto-esophageal fistula induced by a foreign body: the first recorded survival. J Thorac Cardiovasc Surg 80:233, 1980.
DeLuca RF, Ferrer JP, Wortzel EM: Polypectomy snare extraction of foreign bodies from the esophagus: two interesting cases. Am J Gastroenterol 66:374, 1976.
Eng JGH, et al: False-negative abdominal CT scan in a cocaine body stuffer. Am J Emerg Med 17:702, 1999.
Ferrucci JT Jr, Long JA Jr: Radiologic treatment of food impaction using intravenous glucagon. Radiology 125:25, 1977.
Ginsberg GG: Management of ingested foreign objects and food bolus impactions. Gastrointest Endosc 41:33, 1995.
Gracia C, Frey CF, Bodai BI: Diagnosis and management of ingested foreign bodies: a ten year experience. Ann Emerg Med 13:55, 1984.
Haglund S, et al: Radiographic diagnosis of foreign bodies in the oesophagus. J Laryngol Otol 92:1117, 1978.
Hargrove MD Jr, Boyce HW Jr: Meat impaction of the esophagus. Arch Intern Med 125:277, 1970.
Haugen RK: The cafe coronary: sudden death in restaurants. JAMA 186:142, 1963.
Holsinger JW Jr, et al: Esophageal perforation following meat impaction and papain ingestion. JAMA 204:734, 1968.
Iafrati MD, et al: A novel approach to the removal of sharp foreign bodies from the stomach using a combined endoscopic and laparoscopic technique. Gastrointest Endosc 43:67, 1996.
Jackson C: Foreign bodies in the esophagus. Am J Surg 93:308, 1957.
Jones RJ, Samson PC: Esophageal injury. Ann Thorac Surg 19:216, 1975.
Kamal I, Thompson J, Paquette DM: The hazards of vinyl glove ingestion in the mentally retarded with pica: new implications for surgical management. Can J Surg 42:201, 1999.
Kelley JE, Leech MH, Carr MG: A safe and cost-effective protocol for the management of esophageal coins in children. J Pediatr Surg 28:898, 1993.
Kim JK, et al: Management of foreign bodies in the gastrointestinal tract: an analysis of 104 cases in children. Endoscopy 31:302, 1999.
Kline MM: Endoscopic snare in removal of an esophageal foreign body. Gastrointest Endosc 20:165, 1974.
P.2100
Kost KM, Shapiro RS: Button battery ingestion: a case report and review of the literature. J Otolaryngol 16:252, 1987.
Litovitz TL: Battery ingestions: product accessibility and clinical course. Pediatrics 75:469, 1985.
Litovitz TL, Schmitz BF: Ingestion of cylindrical and button batteries: an analysis of 2382 cases. Pediatrics 89:747, 1992.
Longstreth GF, Longstreth KJ, Yao YF: Esophageal food impaction: epidemiology and therapy. A retrospective, observational study. Gastrointest Endosc 53:193, 2001.
Maglinte DDT, Taylor SD, Ng AC: Gastrointestinal perforation by chicken bones. Radiology 130:597, 1979.
Maleki M, Evans WE: Foreign body perforation of the intestinal tract. Report of 12 cases and review of the literature. Arch Surg 101:475, 1970.
Nandi P, Ong GB: Foreign body in the oesophagus: review of 2394 cases. Br J Surg 65:5, 1978.
Neustater B, Barkin JS: Extraction of an esophageal food impaction with a Roth retrieval net. Gastrointest Endosc 43:66, 1996.
Newell KJ, et al: Plastic bread-bag clips in the gastrointestinal tract: report of 5 cases and review of the literature. CMAJ 162:527, 2000.
Opper FH, Isaacs KL, Warshauer DM: Esophageal obstruction with a dietary fiber product designed for weight reduction. J Clin Gastroenterol 12:667, 1990.
Richardson JR: New treatment for esophageal obstruction due to meat impaction. Ann Otol Rhinol Laryngol 54:328, 1945.
Ricote GC, et al: Fiberendoscopic removal of foreign bodies of the upper part of the gastrointestinal tract. Surg Gynecol Obstet 160:499, 1985.
Rogers BHG, et al: An overtube for the flexible esophagogastroduodenoscope. Gastrointest Endosc 28:256, 1982.
Rosch W, Classen M: Fiberendoscopic foreign body removal from the upper gastrointestinal tract. Endoscopy 4:193, 1972.
Rosoff L Sr, White EJ: Perforation of the esophagus. Am J Surg 128:207, 1974.
Sawyers JL, et al: Esophageal perforation: an increasing challenge. Ann Thorac Surg 19:233, 1975.
Schwarz GF, Polsky HS: Ingested foreign bodies of the gastrointestinal tract. Am Surg 42:236, 1976.
Seikel K, et al: Handheld metal detector localization of ingested metallic foreign bodies. Arch Pediatr Adolesc Med 153:853, 1999.
Smith JC, Janower ML, Geiger AH: Use of glucagon and gas-forming agents in acute esophageal food impaction. Radiology 159:567, 1986.
Spitz L: Management of ingested foreign bodies in children. BMJ 4:469, 1971.
Studley JGN, et al: Swallowed button batteries: is there a consensus on management? Gut 31:867, 1990.
Takada M, et al: 3D-CT diagnosis for ingested foreign bodies. Am J Emerg Med 18:192, 2000.
Temple DM, McNeese MC: Hazards of battery ingestion. Pediatrics 71:100, 1983.
Trenkner SW, et al: Esophageal food impaction: treatment with glucagon. Radiology 149:401, 1983.
Velitchkov NG, et al: Ingested foreign bodies of the gastrointestinal tract: retrospective analysis of 542 cases. World J Surg 20:1001, 1996.
Vicari JJ, Johanson JF, Frakes JT: Outcomes of acute esophageal impaction: success of the push technique. Gastrointest Endosc 53:178, 2001.
Votteler TP, Nash JC, Rutledge JC: The hazard of ingested alkaline disk batteries in children. JAMA 249:2504, 1983.
Webb WA: Management of foreign bodies of the upper gastrointestinal tract. Update. Gastrointest Endosc 41:39, 1995.
EAN: 2147483647
Pages: 203