105 - Diagnosis and Staging of Lung Cancer
Editors: Shields, Thomas W.; LoCicero, Joseph; Ponn, Ronald B.; Rusch, Valerie W.
Title: General Thoracic Surgery, 6th Edition
Copyright 2005 Lippincott Williams & Wilkins
> Table of Contents > Volume II > The Esophagus > Section XVIII - Anatomy > Chapter 122 - Embryology of the Esophagus
Chapter 122
Embryology of the Esophagus
Charles E. Blevins
DEVELOPMENT OF THE ESOPHAGUS
As early as the fourth week in development, the esophagus of the human embryo is merely a sphincter or constricted part of the primitive foregut, between the pharynx and stomach, as observed by Keith (1948) (Fig. 122-1). During the sixth and seventh weeks of gestation, the esophagus undergoes rapid elongation as cephalic development separates the head and neck from the thorax. The elongation is facilitated by development of the lungs and pleural cavities, which push the stomach dorsally and inferiorly (Fig. 122-2). Keith suggested that the esophagus is of dual origin, with an upper retrotracheal part originating from the pharyngeal portion and an infratracheal part originating from the pregastric segment of the foregut. During the sixth week of development, the esophagus is only 2 mm long, but at birth it extends to 100 mm. Its superior limit is marked by the inferior cricopharyngeal portion of the inferior pharyngeal constrictor. Fyke and Code (1955) recorded that the cricopharyngeal part of the inferior pharyngeal constrictor relaxes suddenly during swallowing and simultaneously lengthens the vocal folds of the larynx. The lower limit of the esophagus is marked by its entrance to the stomach, in a region that constitutes a barrier to reflux of gastric contents, but it is not marked by an anatomically recognizable sphincter. Basmajian (1980) indicated that at lower thoracic levels, the esophagus is supported away from the aorta, azygos vein, and body of the vertebra, which permits advancement of the esophagus away from the vertebral column. As the lungs approach each other in inspiration of an erect subject, a retroesophageal window is presented in radiographs.
Keibel and Mall (1912) reported that between 8.4 and 16 mm (fifth to seventh weeks), the esophagus is crescentic, with the concavity of the crescent directed toward the trachea (Fig. 122-2). Its upper part is round, but as it descends, it appears transversely elliptic. Near the level of tracheal bifurcation, it becomes round again, and finally it assumes an elliptic shape in the dorsoventral direction. The esophagus remains patent during this early period, save for a nonspecific reticular coagulum.
TISSUE DIFFERENTIATION
Endoderm
The early work of Johnson (1910) and of Keibel and Mall (1912) was reviewed and supplemented by Johns (1952). He reported that the esophagus of 3 to 6 mm embryos is lined by stratified columnar epithelium that is about three cells deep. Between 23 and 24 mm, the endoderm is two cells deep, followed by proliferation into many layers, which never occlude the esophagus but may narrow it at the level of tracheal bifurcation. Ciliated epithelium appears in the 40 mm embryo when ciliated cells form superficial layers of stratified columnar epithelium that lines the esophagus. This condition is characteristic of almost the entire esophageal lining, up to the 130-mm stage. At this time, the stratified columnar condition is replaced by stratified squamous epithelium. Patches of ciliated epithelium may still be present in the upper part of the esophagus at birth. In the 62 mm embryo, patches of simple columnar epithelium appear in the upper and lower ends of the esophagus. Some columnar cells increase in height. Later, columnar cells are replaced by stratified ciliated columnar epithelium.
Superficial glands of the esophageal epithelium develop from tall columnar cells (Fig. 122-3). They first appear at 130 mm and later undergo further development with boundaries of original areas of simple columnar epithelium. Deep glands are late in appearance (Fig. 122-4). They are scanty at first, with little differentiation. Most of their development is postnatal.
Embryos of about 20 mm (6 7 weeks) exhibit numerous large vacuoles in the esophageal epithelium. The vacuoles appear to be caused by active separation of the cells rather than an accumulation of fluids or cellular degeneration followed by resorption. A center of mitosis in the outer layer
P.1882
of cells may account for the bulging visible in the surface epithelium (Fig. 122-5).
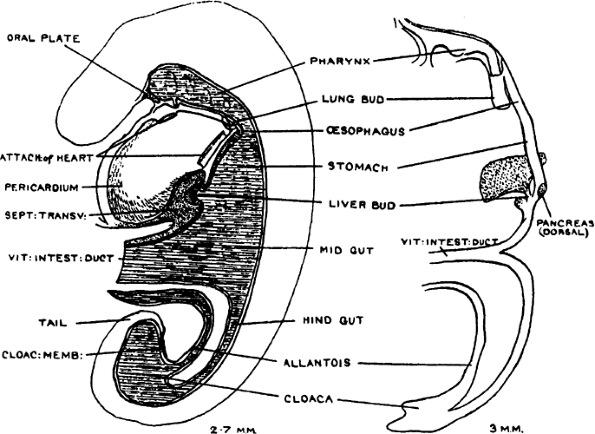 |
Fig. 122-1. Human digestive system in a 2.5-mm embryo (left) near the end of the fourth week of development and in a 3-mm embryo (right) at the end of the fifth week of development. Note the position of the future esophagus. Reproduced from Keith A: Human Embryology and Morphology. Baltimore: Williams&Wilkins, 1948, p. 381. With permission. |
Mesoderm
In similar fashion to the lung, the developing endodermal precursor of esophageal epithelium is surrounded by undifferentiated mesenchyme. As early as 10 mm (6 weeks), mesenchyme is recognizable. Keibel and Mall (1912) confirmed that by 12.5 mm, the esophagus shows a circular muscle layer but no longitudinal muscle layer. Longitudinal muscle is evident at 30 mm and is presented as a definitive layer by 55 mm. At 91 mm, a layer of longitudinal muscle fibers is well developed, and its width matches that of the tunica propria.
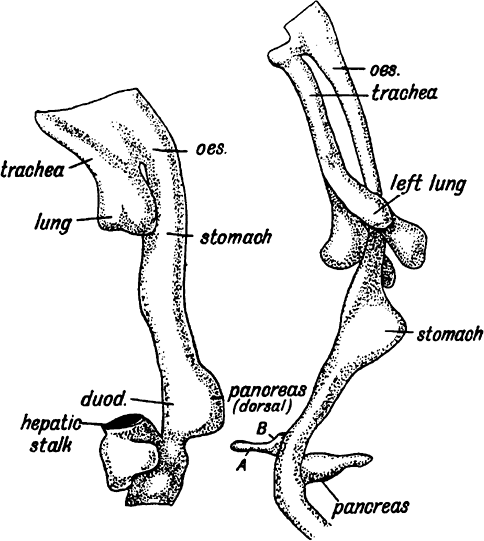 |
Fig. 122-2. Foregut of a human embryo in the fourth week (left) and end of the fifth week (right). Note the progressive elongation of the esophagus (oes.) and relative posteroinferior position of the stomach. From Keith A: Human Embryology and Morphology. Baltimore: Williams&Wilkins, 1948, p. 383. With permission. |
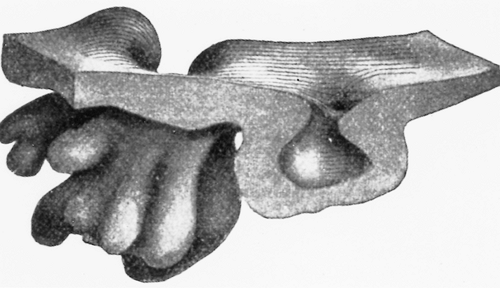 |
Fig. 122-3. Model of a superficial gland from the cardiac end of the esophagus of the human embryo at 240 mm ( 120). The squamous epithelium of the slightly indented surface characterizes the morphology of this type of gland. From Keibel F, Mall F: Manual of Human Embryology. Philadelphia: JB Lippincott, 1912, p. 364. With permission. |
ANOMALIES
The stages of development involving the separation of the trachea and esophagus in the upper portion were described well by Smith (1957). The cephalic portion of the tubular foregut, which becomes the pharynx, appears compressed dorsoventrally, and has a wide lateral extent. A series of pouchlike diverticula appear on either side (the developing pharyngeal pouches). Caudal to the level of the pouches, the foregut narrows abruptly in its lateral extent. Just cephalic to this point, at the level of the fourth pouches, the foregut gives rise to the lung bud. From this point to the dilatation that marks the beginning of the stomach, the foregut remains of relatively small and uniform diameter and becomes the esophagus. In the 21 to 23 day embryo, the first primordium of the respiratory system is seen in the midline of the ventral wall of the foregut between the thyroid primordium
P.1883
cranially and the anterior intestinal portal caudally. With further cellular proliferation, a ridge develops on the external surface of the foregut and a corresponding groove, the laryngotracheal sulcus, develops on the internal surface. The ridge widens as it extends caudally. During the next 12 days, the foregut and the laryngotracheal groove lengthen. A definite thickening of the ventral wall of the foregut occurs cephalad to the liver primordium. Near the end of this period (25 27 days), a knoblike lung bud appears adjacent to the sinus venosus. Ridges of entodermal cells develop from the lateral walls at the caudal end of the lung bud region of the foregut. The union of these proliferating ridges within the lumen of the foregut divides it into a ventral respiratory and dorsal digestive portion. Next is the development of lateral esophageal grooves. These run caudally from just dorsal to the tracheoesophageal ridges to the dorsal wall of the esophagus. In the 27 to 29 day old embryo, the diameter of the esophagus just caudal to the tracheoesophageal separation diminishes. The elongation of the esophagus apparently causes this reduction in the lumen. Independent development of the trachea and esophagus continues, and in the 34 to 36 day old embryo, separation of the respiratory tree from the esophagus is essentially complete.
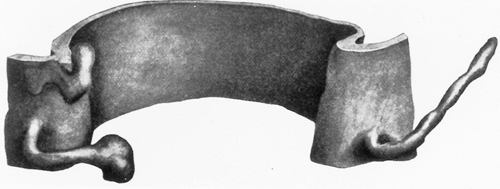 |
Fig. 122-4. Model of three deep esophageal glands at birth ( 90). Note the extensive elongated ducts compared with Fig. 122-3. From Keibel F, Mall F: Manual of Human Embryology. Philadelphia: JB Lippincott, 1912, p. 365. With permission. |
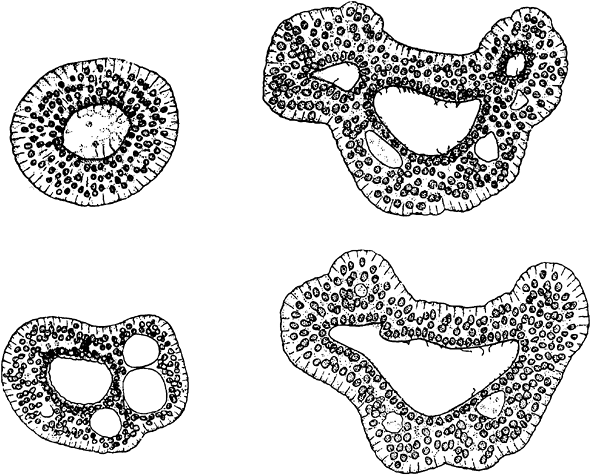 |
Fig. 122-5. Transverse sections of epithelium of the human esophagus. Note the gradual enlargement of the lumen. Active separation of the cells and a shift of mitotic activity to the outer layer of cells are believed to account for the disappearance of the peripheral outpouchings and resolution of the larger central lumen. From Keibel F, Mall F: Manual of Human Embryology. Philadelphia: JB Lippincott, 1912, p. 358. With permission. |
P.1884
Among the congenital abnormalities are atresia of the esophagus at various levels, which can occur with or without tracheoesophageal fistula. The most common forms, as classified by Vogt (1929), involve atresia of the entire esophagus, atresia of a segment of the esophagus with well formed upper and lower esophageal pouches, and various forms of atresia of the esophagus with tracheoesophageal fistula (Fig. 122-6). This anomaly seems to be a result of incomplete separation of the laryngotracheal groove from the foregut. Although many causes for tracheoesophageal fistula have been proposed, the early material of Keibel and Mall (1912) forms a basis for solid thought. Using the model illustrated by Keibel and Mall, Smith (1957) proposed that overdevelopment of the internal ridges of epithelium of the tracheoesophageal septum could occlude the esophagus along the line of the lateral esophageal groove (Fig. 122-7).
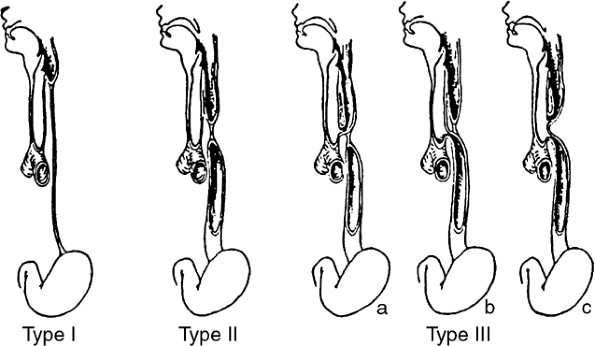 |
Fig. 122-6. Vogt's classification of atresia of the esophagus. Type I: atresia of the entire esophagus. Type II: atresia of a segment of the esophagus with defined upper and lower esophageal pouches. Type III: atresia of the esophagus with tracheoesophageal fistula: a, fistula between the upper esophageal segment and the trachea; b, fistula between the lower esophageal segment and the trachea (the most common, i.e., >90%); c, fistula between both esophageal segments and the trachea. From Smith EI: Contributions to Embryology. Publication 611, No. 245, Vol. 32:43, Carnegie Institute of Washington, 1957. With permission. |
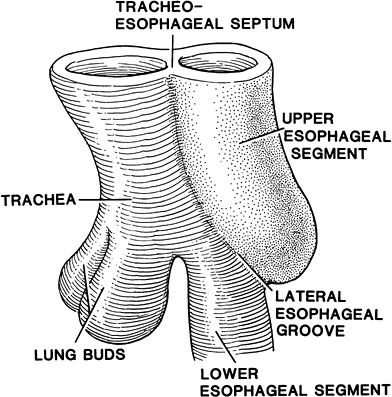 |
Fig. 122-7. Foregut of a 4-mm human embryo in the region of the developing lung bud, showing the location of the lateral esophageal groove in relation to the tracheoesophageal septum and the lumen of the esophagus. Overdevelopment of the internal ridges of this groove occludes the esophagus along the line of the groove. Maintenance of a communication between trachea and esophagus, as indicated in the drawing, would result in an anomaly similar to type IIIb (shown in Fig. 122-6). From Smith EI: Contributions to Embryology. Publication 611, No. 245, Vol. 32:43, Carnegie Institute of Washington, 1957. With permission. |
According to Warkeny (1971), esophageal stenosis may occur, but it is rarer than esophageal atresia with tracheoesophageal fistula. Although the etiology and morphogenesis of this abnormality are unknown, it is known to be associated with other anomalies of the gastrointestinal tract, such as imperforate anus and duodenal atresia. Although stenosis may be treated by dilation, inability to establish nutrition may require a gastrostomy.
Duplication of the mucous membrane may give rise to esophageal webs, which represent incomplete diaphragms within the esophagus. Such webs in the cervical esophagus may go unrecognized despite congenital dysphagia. Congenital esophageal ulcers and esophagitis have been reported, which may or may not be accompanied by hemorrhage.
REFERENCES
Basmajian JV: Grant's Method of Anatomy. 10th Ed. Baltimore: Williams&Wilkins, 1980, p. 84.
Fyke FE, Code CF: Resting and deglutition pressures in the pharyngeoesophageal region. Gastroenterology 29:24, 1955.
Johns BAE: Developmental changes in the esophageal epithelium in man. J Anat 86:431, 1952.
Johnson FP: Development of mucous membrane of esophagus, stomach, and small intestine. Am J Anat 10:521, 1910.
Keibel F, Mall FP: Human Embryology. Philadelphia: JB Lippincott, 1912.
Keith A: Human Embryology and Morphology. Baltimore: Williams&Wilkins, 1948, p. 382.
Smith EI: The early development of the trachea and esophagus in relation to atresia of the esophagus and tracheoesophageal fistula. Contributions to Embryology. Publication 611, No. 245, Vol. 32:43, Carnegie Institute of Washington, 1957.
Vogt EC: Congenital esophageal atresia. AJR 22:463, 1929.
Warkeny J: Congenital Malformations. Chicago: Yearbook, 1971, pp. 678 686.
EAN: 2147483647
Pages: 203
- MPLS Overview
- Implementing Route-Reflectors in MPLS VPN Networks
- Virtual Private LAN Service (VPLS)
- Configuration and Implementation of MPLS QoS in Uniform Mode and Short Pipe Mode Operation
- Case Study 2: Implementing Multi-VRF CE, VRF Selection Using Source IP Address, VRF Selection Using Policy-Based Routing, NAT and HSRP Support in MPLS VPN, and Multicast VPN Support over Multi-VRF CE