8 - Management of Diabetes in Pregnancy, Childhood, and Adolescence
Authors: Unger, Jeff
Title: Diabetes Management in the Primary Care Setting, 1st Edition
Copyright 2007 Lippincott Williams & Wilkins
> Table of Contents > 8 - Management of Diabetes in Pregnancy, Childhood, and Adolescence
function show_scrollbar() {}
8
Management of Diabetes in Pregnancy, Childhood, and Adolescence
Take Home Points
Preconception planning should begin when all female patients with diabetes reach puberty.
Patients should attain and maintain an A1C of 6.5% to 7% for at least 6 months before becoming pregnant.
During pregnancy, a basal-bolus insulin regimen should be prescribed with close monitoring of 1-hour postprandial glucose levels.
Babies born to mothers with gestational diabetes mellitus (GDM) are more likely to have macrosomia. Patients (with GDM) are at high risk for developing type 2 diabetes (T2DM). Lifestyle intervention strategies during pregnancy include caloric modification and moderate exercise.
Scheduled antepartum monitoring can detect fetal anomalies in a high percentage of patients with diabetes. However, maternal hyperglycemia may limit the sensitivity of some of the third-trimester tests.
Children born to mothers with GDM are at high risk for developing T2DM as adolescents. This can result in cardiovascular disease occurring at a very young age.
The differential diagnosis between type 1 diabetes (T1DM) and T2DM in children is based on the initial clinical presentation and presence of autoantibodies.
The glycemic targets of children and adolescents vary, depending on their age group.
Eating disorders are twice as common in adolescents with diabetes as in nondiabetics. Patients with eating disorders omit insulin to control weight gain. These individuals have frequent episodes of diabetic ketoacidosis, recurrent hospitalizations, and premature microvascular complications.
Parents believe hypoglycemia is the most feared complication associated with intensive management of T1DM in children and adolescents.
P.364
Preconception Planning
Case 1
Phyllis is accompanied by her mother for her first-ever Pap smear. After Phyllis confided in her mother 2 weeks ago that she has become sexually active for the first time, Phyllis' mother is requesting that her 16-year-old daughter immediately be placed on oral contraceptives. During the past 2 years, Phyllis' control of her diabetes has been far from desirable. She has been hospitalized twice for diabetic ketoacidosis (DKA), including one stay that lasted 10 days. Her last A1C was 11.2% despite being on a basal-bolus insulin regimen. Phyllis is a cheerleader and tends to party with her friends on weekends. She admits to omitting doses of insulin on occasions because she is trying to control her weight since being forced to take insulin. Fortunately, Phyllis is not hesitant to begin an oral contraceptive and promises to begin taking a more intensive approach to her diabetes.
For this family's primary care physician (PCP), several important management issues must be addressed:
At what age and how often should preconception counseling occur?
What are the risks involved in unplanned pregnancies occurring during times of persistent hyperglycemia?
How does one evaluate and treat eating disorders that are commonly associated with adolescent T1DM?
What is the American Diabetes Association (ADA) recommended A1C treatment target in adolescence, and how can this goal be safely achieved?
Hyperglycemia during pregnancy significantly increases the risk of birth defects in babies born to mothers with diabetes.1 Prior to the discovery of insulin in 1922, diabetic maternal mortality was as high as 44%, whereas the perinatal death rate approached 60%.2 Uncontrolled diabetes at the time of conception can result in spontaneous miscarriages in 30% to 60% of all pregnancies.3 The risk of congenital anomalies in infants of diabetic mothers is 6% to 12%, which is 2 to 5 times greater than that of the normal population.3 Congenital anomalies and spontaneous abortions account for 65% of perinatal losses in diabetic gestations.4 An elevated maternal A1C level early in pregnancy, is an independent risk factor for pregnancy-induced hypertension and preeclampsia.5 The presence of diabetic nephropathy (defined as persistent proteinuria or albuminuria >300 mg per day) in the first 20 weeks of pregnancy is associated with an increased risk of intrauterine growth retardation, fetal distress, and pre-eclampsia.5
The risks of DKA during pregnancy include life-threatening metabolic derangements for the woman and intrauterine death for the fetus.6 Furthermore, the tightly controlled blood sugars recommended in pregnancy increase the risk for maternal hypoglycemia and fetal injury. A sobering fact is that
P.365
congenital anomalies in infants born to mothers with diabetes are more likely to be multiple, severe, and lethal, when compared with those in infants born to women without diabetes. Intensive management of diabetes during pregnancy coupled with aggressive fetal surveillance and perinatal care can result in outcomes that are nearly identical to those in the nondiabetic population.7
Preferably, pregnancy should be planned and managed while the maternal glycemic control is as close to normal as possible. Unfortunately, preconception planning for pregnancy is the exception rather than the rule. Between 1986 and 1988, only 7% of women in California sought preconception care, whereas 34% of eligible women in Maine sought preconception counseling from 1987 to 1990.8,9 A recent analysis demonstrated the benefits of targeting preconception care for patients with T1DM.9a Of the 288 women enrolled in the study, the 38% who elected to pursue preconception counseling had significantly fewer adverse pregnancy outcomes (malformations, stillbirths, neonatal deaths) when compared with women who declined the specialized care (2.9% vs. 10.2%). The counseled patients had fewer premature deliveries (<34 weeks' gestation) (5% vs. 14%) and better glycemic control during the initial 20 weeks of their pregnancies. In contrast, there was no significant difference in rates of delivery before 37 weeks, pre-eclampsia, macrosomia, or cesarean section between women with and without prepregnancy care.
Preconception care is critical to improving the outcomes of all pregnancies as well as the general health of the nation. The Centers for Disease Control and Prevention (CDC) has established a goal to have PCPs provide age-appropriate preconception care to all adolescent and women patients.9b However, only 25% of our nation's PCPs address preconception planning with any of their patients. Preconception planning for all patients, especially those with high-risk pregnancies, should include the following interventions:
General reproductive health education
Prevention of unwanted or mistimed pregnancies
Ways to prepare mentally, socially, and physically for a pregnancy
Prevention of sexually transmitted diseases
Promotion of healthy nutrition and physical activity beginning in adolescence and continuing throughout one's lifespan
Folic acid supplementation during reproductive years
Cessation of alcohol, nicotine, and illicit drugs
Vaccination against infectious diseases associated with poor birth outcomes and sexually transmitted diseases (e.g., rubella and cervical cancer)
Aggressive management of chronic diseases such as diabetes, hypertension, mental illness, and hypothyroidism
Cessation of any prescription or over-the-counter medications that are teratogenic
As only 41% of pregnancies in the United States are planned,10 preconception awareness counseling should begin when girls with diabetes reach
P.366
puberty. The topic of preconception care should then be revisited at regular intervals, perhaps at the time of the patient's annual physical examination or Papanicolaou (Pap) smear.11 Clinicians should inform women about the importance of achieving and maintaining targeted glycemic control before conception as well as throughout pregnancy. Patients who are considering becoming pregnant should be placed on either multiple daily injections (MDIs) using basal-bolus insulin therapy or an insulin pump. Frequent blood glucose self-monitoring, coupled with adherence to positive lifestyle choices (smoking and alcohol cessation, regularly scheduled physical activity, and selection of healthy foods), should be emphasized. A1C levels should be checked frequently to ensure compliance with the program. Changes in A1C levels can provide guidance on whether postprandial or fasting blood glucose levels should be targeted for improvement.
A1C levels at the time of fertilization and embryogenesis have been linked to a higher rate of spontaneous abortions and congenital malformations.12 Patients should be informed that long-term complications such as retinopathy, nephropathy, and neuropathy may be exacerbated during pregnancy. In general, targeted glycemic control should be obtained (A1C, 6.5% to 7%) and maintained for at least 6 months before a patient becomes pregnant.13 In any patient who has retinopathy at the onset of pregnancy, worsening of her retinopathy may develop as one attempts to normalize her blood glucose levels rapidly.14 Therefore, the clinician should consider slowly improving glycemic control in patients with retinopathy, and make certain to have all women with diabetes evaluated by an ophthalmologist as part of the initial pregnancy evaluation.
Gestational Diabetes Mellitus
Gestational diabetes mellitus (GDM), defined as the new onset or new diagnosis of glucose intolerance during pregnancy, affects 200,000 pregnancies in the United States annually.15 GDM results from peripheral insulin resistance, hepatic insulin resistance, and impaired insulin secretion, similar to the pathophysiologic process involved with T2DM (Fig. 8-1).
Although screening for GDM has not been proven to prevent adverse perinatal outcomes, risk assessment for GDM should be performed at the first prenatal visit. Women considered to be at high risk for GDM (Table 8-1) should undergo immediate diagnostic testing. If the initial test is negative, the patient should be retested at between 24 and 28 weeks of gestation. Pregnant women at low risk (younger than 25 years, normal weight, and no personal or family history of diabetes) need not be tested for GDM.16
Pregnant women with an average risk should undergo a two-step glucose testing protocol: A 50-g, 1-hour glucose challenge test; then a 100-g, oral, 3-hour glucose tolerance test if the patient exceeds the glucose threshold on the initial test of greater than 140 mg per dL. In women with multiple risk factors, a one-step 100-g, 3-hour glucose challenge test may be a more cost-effective way to diagnose GDM. Diagnostic thresholds for the 100-g test are
P.367
shown (Table 8-2). Patients who meet or exceed two or more of these venous plasma concentrations are diagnosed with GDM. The test should be performed in the morning after 8 to 14 hours of fasting and after at least 3 days of unrestricted diet (>150 g carbohydrate per day) and unlimited physical activity.
 |
Figure 8-1 Pathogenesis of Gestational Diabetes Mellitus (GDM). As normal pregnancy progresses, insulin resistance deteriorates as patients gain weight and reduce their level of physical activity. Impaired glucose tolerance develops, which can result in beta-cell cytotoxicity, reducing the ability of the beta cell to produce enough insulin for the maintenance of euglycemia. Strict dietary measures in GDM are needed to maintain normal blood glucose levels. Cytokines such as interleukin-6 and tumor necrosis factor may stimulate an acute-phase inflammatory response, as noted by an elevation in circulation concentrations of C-reactive protein (CRP). CRP levels are significantly increased in the first trimester of women in whom GDM develops.39 |
P.368
TABLE 8-1 Risk Factors for Gestational Diabetes | |
|---|---|
|
TABLE 8-2 Criteria for Abnormal Result on 100-g, 3-Hour Oral Glucose Tolerance Tests in Pregnant Women | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
GDM can result in complications for both the fetus and mother, as outlined below.
| Maternal Complications of GDM | Fetal Complications of GDM |
|---|---|
| Pre-eclampsia | Macrosomia |
| Hypertension | Intrauterine death |
| Urinary tract infections | Preterm delivery |
| Preterm labor | Postnatal hypoglycemia |
| Need for cesarean section | Hyperbilirubinemia |
| Future risk of diabetes and metabolic syndrome | Hypocalcemia Respiratory distress syndrome Polycythemia Future risk of obesity, metabolic syndrome, cardiovascular disease, and diabetes |
Approximately 50% of patients with GDM will have a recurrence of GDM during future pregnancies. Women with higher prepregnancy weight, older women (older than 35),17 and multiparous women have recurrence rates of more than 90%.18 With each episode of GDM, beta-cell dysfunction may deteriorate, increasing the risk of T2DM developing after delivery.
P.369
Often GDM is diagnosed well after embryogenesis occurs and has been associated with an increased risk of congenital anomalies. The most common fetal abnormality of GDM is macrosomia, defined as fetal weight greater than 4 to 4.5 kg.
Prevention of Gestational Diabetes Mellitus
Despite the prevalence of GDM, little research has been performed on preventing the disorder. The only modifiable risk factor of GDM is prepregnancy obesity. Recurrence of GDM appears to be greater in women who consumed more fat between subsequent pregnancies as compared with women who consumed low-fat, high-carbohydrate diets.19
Exercise may play a role in both prevention and management of GDM. The process of glucose transport into insulin-sensitive cells has not been studied in pregnancy. Because gestational diabetes is a state of altered insulin sensitivity, exercise is a logical therapeutic intervention. Experts at the Third International Workshop-Conference on Gestational Diabetes Mellitus20 suggested that active women with GDM may continue moderate exercise. Regular exercise in previously inactive women may normalize blood glucose levels. Initiating an active lifestyle program in a group of inherently inactive pregnant woman may not only improve glycemic control immediately but also may reduce the risk or delay the onset of diabetes in the future.
A clinical protocol published by Artal et al21 provides some exercise guideline protocols for pregnant women with GDM who wish to initiate a home-based program:
Patient is informed of potential complications.
Patient rests for 30 minutes before breakfast, lunch, and dinner, and monitors fetal activity.
Patient monitors fasting and 2-hour postprandial plasma glucose.
If fetal activity and glucose level are OK, she exercises for 20 to 30 minutes at 50% VO2 max (percentage exertion fairly light to somewhat hard; see Table 9-12) after each prescribed meal.
Patient rests for 30 minutes and counts fetal movements.
If uterine contractions become regular or occur 15 minutes apart or less, patient notifies obstetrician.
Patient keeps accurate records of blood glucose, food intake, physical activities, and fetal movements.
Beginning at 32 weeks' gestation, nonstress testing is done weekly; further fetal tests are conducted as indicated.
Other patients may want to begin a simple walking program, which requires little medical monitoring. Along with the exercise program, women with gestational diabetes should follow a daily balanced diet calculated for 30 kcal per kg ideal body weight (consisting of 60% carbohydrates, 20% protein, and 20% fat).22 Obese women [body mass index (BMI) >30 kg per m2]
P.370
should limit their carbohydrate intake to 35% to 40% of the total daily calories. Approximately 75% to 80% of women with GDM can achieve euglycemia on dietary restrictions alone.23
Medical Management of Gestational Diabetes Mellitus
Four times daily blood glucose self-monitoring is recommended for all women with GDM, performed fasting and 1 hour after meals. Postprandial sampling has been associated with better glycemic control, a lower incidence of large-for-gestational-age infants, and a lower rate of cesarean sections.16 Approximately 20% to 60% of pregnancies complicated by GDM require the use of insulin therapy. The ADA16 recommends initiating insulin therapy when the following glycemic targets are not achieved:
| Timing of Glucose Check | Upper Limits of Normal (mg/dL) |
|---|---|
| Fasting | >105 |
| 1 h preprandial | >155 |
| 1 h postprandial | >130 |
Insulin dosing should be based on the amount of carbohydrates consumed at each meal. Patients should be referred to a registered dietician to learn how to correlate their insulin dose with their carbohydrate intake. In general, 1.5 units of regular lispro or aspart insulin for every 10 g of carbohydrates (carbs) covers breakfast, and 1 unit of regular, lispro, or aspart insulin covers 10 g of carbs for lunch and supper. Elevated fasting blood glucose levels can be controlled with NPH by using an initial dose of 0.15 U per kg, or glargine, 0.3 U per kg per day.
Some physicians advocate the use of serial ultrasonography to measure the fetal abdominal circumference as an alternative means to determine which patients require insulin therapy.24
Use of oral hypoglycemic agents to treat gestational diabetes has not been recommended because of concerns about potential teratogenicity and transport of glucose across the placenta (causing prolonged neonatal hypoglycemia).25 Although first-generation hypoglycemic agents (chlorpropamide and tolbutamide) have been shown to cross the placenta, recent in vitro and in vivo evidence has determined that glyburide does not enter the fetal circulation.26
A recent randomized control trial (RCT)27 comparing the use of glyburide and insulin in women with gestational diabetes demonstrated that glyburide therapy resulted in comparable maternal outcomes (e.g., glycemic control, cesarean deliveries) and neonatal outcomes (e.g., macrosomia, hypoglycemia, intensive care unit admissions). Glyburide therapy was not started before 11 weeks of gestation and the drug was not detected in any of the neonatal cord blood samples. Preliminary evidence from this trial suggests that glyburide may be a safe, effective alternative to insulin in the management of GDM.
P.371
The American College of Obstetricians and Gynecologists (ACOG)28 and the ADA19 agree that glyburide should not be prescribed for the treatment of gestational diabetes until additional RCTs support its safety and effectiveness. Because of the ease of use of glyburide, many physicians prescribe glyburide to patients with GDM in spite of these expert opinions. In a recent prospective cohort study of patients with polycystic ovary syndrome,29 metformin therapy was shown to decrease the subsequent incidence of GDM, reduce first-trimester miscarriage rates, and result in no apparent increase in congenital anomalies. RCTs are needed to demonstrate the safety and effectiveness of metformin in pregnancy before use of this medication is warranted for the treatment of GDM.
After delivery, blood glucose levels should be monitored to make certain that the euglycemic state has been restored (fasting blood glucose, <100 mg per dL, and 1-hour postprandial blood glucose, <140 mg per dL). Monitoring should be continued for 6 to 8 weeks, and if the levels are consistently normal, testing may be stopped. Active lifestyle, caloric restriction, weight reduction, and healthy food choices should be encouraged at each visit. An annual 2-hour postglucose challenge should be used on all patients to screen these high-risk individuals for diabetes. Finally, PCPs should be aware that children born to mothers with GDM have a higher risk of developing T2DM as children and adolescents. Healthful lifestyle issues should be discussed with all family members at each visit so that weight can be controlled and diabetes onset may be delayed.
Management of Type 1 Diabetes during Pregnancy
Most women with diabetes who become pregnant will require the services of a perinatologist, obstetrician, registered dietician, certified diabetic educator, and an endocrinologist who specializes in pregnancies in women with diabetes.
Table 8-3 lists the pertinent historic information that should be obtained when women with diabetes are contemplating pregnancy or become pregnant.
As soon as pregnancy is confirmed, insulin dose requirements will begin to change. Total daily doses are approximately 0.6 U per kg before 6 weeks' gestation, 0.7 U per kg from 6 to 18 weeks, 0.8 U per kg from 18 to 26 weeks, 0.9 U per kg from 26 to 30 weeks, and 1.0 U per kg from 36 to 40 weeks.40 These insulin doses are designed to match a diet that is calculated at 30 kcal per kg per day for a woman who is of normal weight (80% to 120% ideal body weight) and is divided into 40% carbs, 40% fat, and 20% protein. The diet is then subdivided into three primary meals and frequent small snacks.
The questions that should be discussed with patients during pregnancy involve the (a) type of insulin that will be used during gestation; (b) frequency and timing of dosing; (c) fasting and postprandial glycemic targets; (d) frequency of meals and snacks; (e) necessity and timing of frequent blood glucose self-monitoring; (f) management of hypoglycemia; (g) appropriateness, safety, and timing of exercise; and (h) management strategies to prevent DKA.
P.372
P.373
P.374
P.375
TABLE 8-3 Prepregnancy Diabetes History | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Fetal anomalies, particularly macrosomia, may be prevented by maintaining strict glycemic control during pregnancy.8 Any blood glucose values that lie outside of the targets shown earlier are considered suboptimal. Patients should monitor before meals, 1 hour postprandially, and between 2 and 3 AM to evaluate and treat hypoglycemia. Patients are taught to recognize and respond to hypoglycemia (Fig. 8-2). Common symptoms such as perioral tingling, excessive sweating, palpitations, weakness, or confusion should prompt
P.376
a blood glucose check (Table 8-4) and correction of hypoglycemia by using glucose tablets or gels.
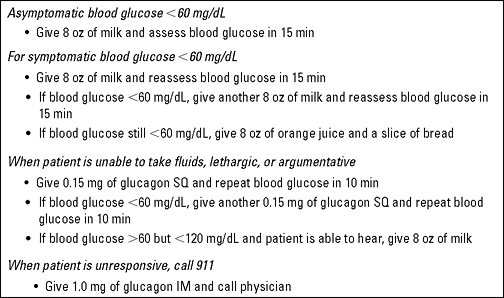 |
Figure 8-2 Home Treatment of Hypoglycemia. |
TABLE 8-4 Target Blood Glucose Levels during Pregnancya | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||
Pregnant patients with diabetes should be managed in partnership with an endocrinologist. The frequency of outpatient visits is based on the degree of patient's glycemic control. Patients with documented hyperglycemia, severe infections such as pyelonephritis, hypertension, preeclampsia, spontaneous labor, or those demonstrating poor adherence to the diabetes self-management program warrant hospitalization.
The endocrinologist should do the following:
Review patient's medical diary regarding blood glucose control and urinary acetone levels. Adjust insulin, if needed. Ensure that blood pressure remains in the normal range
Check that obstetrical antepartum testing is being performed in a timely manner, and discuss any abnormal findings with the obstetrical team (Table 8-5).
Make necessary dietary adjustments to improve glucose control. Provide dietary counseling, as needed.
Ensure that patient has all necessary materials for blood glucose self-monitoring and administration of insulin.
Schedule testing for first-, second-, and third-trimester creatinine clearance, total proteinuria, microalbuminuria, urine culture and sensitivity, thyroid function, and complete ophthalmologic consultation.
After 32 weeks, review daily fetal movement record.
Safety of Insulin Use during Pregnancy
Although no insulin has a category A pregnancy classification, regular and NPH insulin have been used extensively in pregnant women. Lispro has a
P.377
P.378
category B classification, whereas aspart, glulisine, glargine, and detemir are classified as category C. Glargine is approved for use in patients 6 years and older; no other insulins have an age restriction.
TABLE 8-5 Antepartum Fetal Surveillance in Pregnancies Complicated by Diabetes | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||
Concerns regarding the use of insulin lispro during pregnancy first surfaced in 1997.30 One patient who became pregnant while using insulin lispro had a pregnancy termination at 20 weeks' gestation. A second patient using lispro delivered a normal baby at term. However, the baby died 3 weeks later unexpectedly. Both babies were found to have congenital anomalies, although, in retrospect, insulin lispro was probably not the reason for the birth defects. A more recent multicenter, multinational study evaluating the possible effects on organogenesis in women using lispro during early pregnancy found no difference in the rate of congenital anomalies between lispro users and nondiabetic controls.31 Both lispro and aspart appear to be safe insulins to use for women with gestational diabetes as well as for those with preexisting type 1 diabetes.32 Currently no data exist on long-acting analogue safety in pregnancy.33
Experimental studies suggest an increased risk of mitogenicity on tumor cell lines exposed to high doses of glargine. However, glargine use during the first trimester has been shown to have no adverse outcomes associated with fetal development.34 This is important because so many pregnancies are unplanned, as patients continue using their basal insulin past the time of their first missed menstrual period. Only 1% to 5% of maternal endogenous insulin crosses the placental barrier and passes into the fetal circulation, as proven with both regular insulin and insulin lispro,35,36 so the effects of glargine on adverse fetal development are likely to be minimal. Randomized clinical trials using glargine in pregnancy are not likely to be performed for ethical reasons. Most experts believe that the glycemic control that patients are able to maintain in pregnancy with glargine is superior to that with NPH. Anecdotally, patients also feel better on glargine. The continuation of glargine during pregnancy should be discussed in detail with patients who are unable or unwilling to use insulin pump therapy. Most patients will choose to maintain better glycemic control throughout pregnancy with glargine and be less concerned with the high affinity that glargine has on insulin-like growth factor binding sites, based on cell-line studies. Not enough information is available to recommend the use of insulin detemir during pregnancy at this time.
Exercising during Pregnancy
During physical activity, muscles consume glucose at a rate of 2 to 3 mg per kg of body weight per minute of exercise.37 An exercise program should be initiated in an untrained individual only when glycemic levels are adequately controlled. The blood glucose target at the onset of exercise is 90 to 140 mg per dL. A meal should be consumed 1 to 3 hours before beginning an exercise session not lasting longer than 45 minutes. The prandial
P.379
bolus of insulin should be decreased by 50% if the insulin is expected to peak while exercising. Complications38 that would preclude exercise participation include
Preterm labor
Premature rupture of the membranes
Incompetent cervix
Persistent second- and third-trimester bleeding
Intrauterine growth retardation
Placenta previa beyond week 26
Pregnancy-induced hypertension
Recommended modes of exercise include walking, stationary cycling, low-impact aerobics, and swimming. Each exercise session should begin with a 5- to 10-minute warm-up period, followed by an endurance phase, during which the heart rate should not exceed 140 beats per minute (bpm) [rate of perceived exertion (RPE), 12 to 13] (see Table 9-12).
A summary of the general rules for exercising with T1DM and pregnancy is found in Tables 8-6 and 8-7.
P.380
TABLE 8-6 Hints for Safely Exercising with Type 1 Diabetes and Pregnancy | ||
|---|---|---|
|
TABLE 8-7 Rate of Perceived Exertion (RPE) Scalea | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
Delivery
The timing of the final admission for delivery is dependent on the quality of glycemic control throughout pregnancy, the accuracy of dating information gathered during the prenatal visits, and the confirmation of fetal pulmonary maturity by amniocentesis. Delivery may be prompted by fetal distress. Spontaneous labor after 36 weeks may precipitate delivery. However, if spontaneous labor does not occur, labor is induced at 40 to 42 weeks in patients with normoglycemia.
The night before labor is induced, the usual dose of basal insulin is administered. Before active labor begins (3 contractions per 10 minutes, each lasting 60 seconds), insulin requirements are high. However, when active labor begins, insulin requirements drop to zero, whereas glucose requirements increase to 2.55 mg per kg per minute. Hourly blood glucose determinations help guide the administration of dextrose and insulin during labor and delivery, as described in Table 8-8.
Induction of Labor40
The protocol for blood glucose stabilization before labor induction is as follows. Give the usual bedtime basal insulin the night before, and induce labor in the morning, if possible. Mix oxytocin in 50% isotonic saline, and do not
P.381
P.382
begin dextrose infusion until the patient is in active labor or the blood glucose value is less than 70 mg per dL. Proceed toward target glucose infusion rate as labor progresses, as in spontaneous labor. If the blood glucose is more than 120 mg per dL, an alternative protocol for reducing the glucose level is to begin a constant infusion of insulin at a rate of 0.05 U per kg per hour and increase the rate of infusion of insulin until the glucose is stabilized at a level near 10 mg per dL.
TABLE 8-8 Labor and Delivery: Insulin and Glucose Requirements | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
Elective Cesarean Section40
The protocol for blood glucose stabilization for an elective cesarean section is as follows. Give usual bedtime basal insulin the night before a planned cesarean section. Monitor fingerstick blood glucose hourly preoperatively and throughout the cesarean procedure. Maintain the blood glucose level at 80 to 100 mg per dL. Manage intravenous infusions and insulin as in spontaneous labor.
Premature Labor
Intravenous infusions and administration of insulin are managed as in spontaneous labor. Caution must be exercised when tocolytic agents are used to stop premature labor because these drugs may alter glucose homeostasis. Beta-mimetics may elevate serum glucose levels, whereas alcohol may cause hypoglycemia.
P.383
Postpartum Management
Insulin requirements may decrease precipitously in the immediate postpartum period and remain considerably depressed for 48 to 96 hours. Any suspected postpartum infections should be cultured and aggressively treated. All women should have a repeated ophthalmologic examination. Women who had evidence of retinopathy need special attention and advice about follow-up plans for optimal eye care.
After Vaginal Delivery
Postpartum care should be routine, with a calculated diet based on 25 cal per kg per day of 20% protein, 40% carbohydrate, and 40% fat if the patient is not breastfeeding. Diet should be calculated on the basis of postpartum weight and should be divided into antepartum meal and snack proportions.
Basal-bolus insulin therapy may resume based on a predicted total daily dose of 0.6 U per kg. The blood glucose level is assessed before each meal, and after 1 hour.
After Cesarean Section
After cesarean section (or during no oral intake), insulin and glucose regimens are as follows (based on postpartum body weight):
Give 1/6 total daily insulin as NPH every 8 hours while fasting or on clear- or full-liquid diet (equal to the 10:00 PM dose when eating). The glargine dose of 0.3 U per kg per day may be continued. Patients on detemir can resume at 0.3 U per kg per day, with 50% of the total dose given in the morning and 50% given 12 hours later.
When a regular diet is not being consumed, the intravenous solutions should be given on the basis of blood glucose determinations every 2 to 4 hours, as outlined for spontaneous labor.
When a regular diet is being ingested, calculate insulin based on postpartum body weight at 0.6 U per kg per day if the patient is not breastfeeding. Basal-bolus insulin therapy may be initiated with long- and short-acting insulin analogues. Increase insulin as needed to maintain normoglycemia. Half (50%) of the total daily dose is provided as basal insulin, and 50% is given as preprandial bolus insulin.
Insulin and Medical Nutrition for Nursing Mothers41
The caloric requirement for a nursing mother is approximately 27 kcal per kg per 24 hours.41 These calories should be divided as usual; however, the feeding routine of each infant will directly affect the mother's feeding schedule. Specifically, if the infant consumes a majority of calories at bedtime or in the middle of the night, the mother must also consume her calories then.
P.384
Management of Diabetes in Children and Adolescents
Type 2 Diabetes
Case 2
Marisol, age 14, is reluctantly brought to the family doctor by her concerned mother to have her vaginal discharge evaluated. Marisol denies that she is now or ever has been sexually active but does have regular periods, which began 10 months ago. Her mother has T2DM, and both parents are Hispanic. Her physical examination is remarkable primarily for her size. She is 5 feet tall and weighs 247 lb. Her blood pressure is 140 per 94, and her random blood glucose level is 294 mg per dL. Marisol has evidence of acanthosis nigricans in both axillae (see Fig. 3-9). Her point-of-service A1C test is 9.2 %. Her urinalysis is negative for ketones, and the vaginal discharge is consistent with vaginal candidiasis.
Marisol most likely has T2DM. She has no evidence of ketosis, which, if present, would suggest a state of absolute insulin deficiency. She has acanthosis nigricans (suggestive of severe insulin resistance), is obese and hypertensive, has a family history of T2DM, and is Hispanic. Although the diagnosis may be clear, the management of T2DM in children and adolescents is controversial. Treatment options for Marisol are discussed later.
No longer considered to be a condition of primarily adult onset, T2DM has become increasingly common among children aged 6 to 11 years and adolescents aged 12 to 19 years. Although no definitive large-scale reporting of incidence within these age groups has occurred, a recent epidemiologic review42 led to the suggestion that as many as 8% to 45% of new-onset pediatric diabetes cases in the United States may be type 2. The Centers for Disease Control and Prevention (CDC)43 reported 206,000 cases of diabetes among those younger than 20 years in the United States, giving an estimated prevalence of 0.25%. As in adults, many childhood cases go unrecognized, resulting in the possibility of a substantial number of children and adolescents with undiagnosed T2DM.
The increase in T2DM among children and adolescents has emerged in parallel with an alarming increase in the number of young people who have become overweight or obese. Along with family history, obesity stands out as a prominent risk factor for the development of T2DM. Over the past 20 years, the prevalence of childhood and adolescent obesity has doubled, and without increased measures for prevention, these numbers will likely continue to increase. Although children and adolescents representing all racial, ethnic, and socioeconomic groups have been affected by this trend, Native Americans, Hispanics, and African Americans have become particularly susceptible to the epidemic of obesity.44 T2DM is especially on the rise within these groups, and the prevalence
P.385
of hypertension among African-American and Hispanic children is also increasing, putting them at increased risk for cardiovascular disease developing.
A troubling concern is that in children with T2DM, microvascular and macrovascular complications similar to those in adults will develop, only at a much younger age and sooner after their initial diagnosis is made when compared with adults. This may add a tremendous burden to healthcare costs in the future. In a study from Canada, subjects in whom T2DM developed as children were resurveyed as young adults between 18 and 33 years of age. Of the 51 subjects, 9% had died, 6% were on dialysis, 1 had a toe amputation, and 1 was blind.45
The ADA criteria for diagnosis of diabetes are the same for children, adolescents, and adults. Classification of the type of diabetes is generally more difficult than establishing a diagnosis of diabetes. In many cases, classification is based on observation of clinical features and course, or it may be accomplished with the aid of data from additional testing (e.g., C-peptide test, detection of autoantibodies, and determination of fasting insulin level; see Table 8-9). These tests may not be practical or available in the primary care environment. The presence of DKA is a classic manifestation of T1DM but may also occur in patients initially with new-onset T2DM.46 Such patients may be initially seen in DKA, have elevated C-peptide levels, and an absence of islet cell antibodies (ICAs) or glutamic acid decarboxylase (anti-GAD) antibodies. After the initial metabolic disturbance is corrected, these patients do not require insulin. In an ideal setting, T1DM should be confirmed by measuring autoantibodies, whereas T2DM is diagnosed with a fasting C-peptide, which, when elevated, is suggestive of insulin resistance. However, C-peptide levels have not been standardized and often the test is not affordable.
The pathogenesis of T2DM in children and adolescents is multifactorial and includes the following:
Genetic (defects affecting multiple genes, some caused by mutations)47
Obesity48
Physical inactivity49
Insulin resistance, compensatory hyperinsulinemia, and subsequent beta-cell failure, leading to clinical expression of T2DM50
Acanthosis nigricans, as a marker of insulin resistance, occurs in 60% to 90% of children with T2DM,51 especially in African Americans, Hispanics, and some Native Americans.
Polycystic ovary syndrome is associated with insulin resistance co-expressed with hyperinsulinemia.52
Children with either low birth weight (less than 2.5 kg) or high birth weight (more than 4 kg), especially those with low birth weight who gain weight rapidly after puberty53
Mothers with GDM have an 8 times greater chance of having T2DM develop in a child between ages 10 and 16, when compared with age-matched controls whose mothers had normoglycemia during pregnancy.54
P.386
P.387
TABLE 8-9 Differentiation of Type 1 and Type 2 Diabetes in Children and Adolescents
Type 1 Diabetes (T1DM) Type 2 Diabetes (T2DM) Onset Acute, symptomatic Slow, often asymptomatic Clinical picture Weight loss
Polyuria
Polydipsia
Altered consciousness
Polyphagia
Fatigue
Visual changesObesity
Strong family history of T2DM
Family history of coronary artery disease common
High prevalence in African Americans, Native Americans, Asians, Pacific Islanders, and Alaska Natives
Acanthosis nigricans suggests insulin resistance.
Polycystic ovary syndrome
Maternal history of GDM
Personal history of low (<2 kg) or high (>4 kg) birth weight
Rapid weight gain during childhood
Inactive lifestyleKetosis Almost always present May be present C-peptide Negative Fasting C-peptide levels elevated, suggestive of insulin resistance. (However, standardization of fasting C-peptide levels in children has not been done.) Antibodies for autoimmune disease ICA+
Anti-GAD+
ICA 512+Negative antibody studies Pathophysiology Autoimmune disorder Insulin resistance, decreased insulin sensitivity similar to that in adult T2DM Treatment Insulin (basal/bolus)
Insulin-pump therapy
Screen and treat comorbiditiesInsulin if A1C >11 % (basal + orals, basal alone, mixed dose analogue, basal/bolus, inhaled insulin?)
Oral agents (metformin)
Lifestyle intervention
Monitor and treat comorbidities (hypertension, hyperlipidemia, proteinuria, coronary artery disease)ICA, islet cell antibody; GAD, glutamic acid decarboxylase; GDM, gestational diabetes mellitus; T2DM, type 2 diabetes mellitus.
Adapted with permission from Alberti G, Zimmet P, Shaw J, et al, for the Consensus Workshop Group. Type 2 diabetes in the young: the evolving epidemic: The International Diabetes Federation Consensus Workshop. Diabetes Care. 2004;27:1798 1811.Forty-five percent to 80% of children with T2DM have at least one parent with diabetes, and 74% to 100% have a first- or second-degree relative with T2DM.54 A strong correlation with a family history of coronary artery disease also is common.55
The primary goals of management for children and adolescents with T2DM include
Stabilization of any acute metabolic deficiencies while improving long-term glycemic control
Targeting and maintaining an A1C of 7% or less56
Preventing microvascular and macrovascular disease
Educating patients and family members on behavioral interventions and lifestyle changes that must be incorporated into one's daily routine
Reinforcing and stabilizing the psychological well-being of the adolescent patient
Differences of opinion exist as to how to manage children with T2DM. Pharmacotherapy must almost always be used in partnership with lifestyle and behavioral intervention to achieve the acceptable glycemic and metabolic targets. In the United States, approximately 50% of young patients with T2DM receive oral agents, primarily metformin, and 50% are placed on insulin.56 Although there is no reason to believe the oral agents will work differently in children than in adults, there is uncertainty about the long-term implications of pharmacotherapy in this age group.
A simplified approach using oral agents as monotherapy or in combination may allow patients time to adjust psychologically to their new diagnosis. However, a more rapid intensification with exogenous insulin therapy would certainly be appropriate, especially if the patient were symptomatic and had an A1C greater than 10%. Once the metabolic status is corrected by using intensive therapy, a more simplified treatment can be used for maintenance control of the hyperglycemia. A patient such as Marisol (Case 2) would most likely be unable to achieve an A1C less than 7% with oral agents alone. Therefore, one might consider using a once-daily basal insulin + metformin as her initial treatment. Using a twice-daily premixed insulin analogue in a treat-to-target protocol (see Chapter 5) might also help restore her metabolic status to target quickly. The insulin can be given before breakfast and at dinner. Aggressive initial management of T2DM might also be more readily acceptable to patients in whom bad habits and routines may develop months or years after the diagnosis is made.
Metformin has been shown to be safe and effective in pediatric use,57 although as monotherapy in children and adolescents with T2DM, combination therapy may be necessary to provide adequate glycemic control over an extended period.58
The comorbidities associated with T2DM in children and adolescents must be monitored and treated as shown in Table 8-10. One must keep in mind that lifestyle intervention is always in the forefront of diabetes management in children with T2DM.
P.388
TABLE 8-10 Pharmacotherapy for T2DM in Children and Adolescents | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||
Type 1 Diabetes
The diagnosis of T1DM in children is usually straightforward and requires little or no specialized testing (Table 8-10). Most children and adolescents with type 1 diabetes are first seen with a several-week history of polyuria, polydipsia, polyphagia, and weight loss, with hyperglycemia, glycosuria, ketonemia, and ketonuria. The criteria for diagnosing T1DM in children are similar
P.389
to those for adults. In the asymptomatic child or adolescent who is screened because of high risk for diabetes, a fasting plasma glucose (FPG) of 126 mg per dL or more or a 2-hour plasma glucose/random glucose of 200 mg per dL or more should be repeated on a second day to confirm the diagnosis. The child or adolescent with typical symptoms of diabetes and a random plasma glucose 200 mg per dL or more does not require a repeated value on another day or any further testing to diagnose diabetes. Because of the potential for rapid clinical deterioration expected in untreated children with T1DM, unnecessary delays in the diagnosis must be avoided, and a definitive diagnosis should be made promptly.
Although differentiating T1DM from T2DM at first may be difficult, any child who is initially seen with severe fasting hyperglycemia, metabolic derangements, and ketonemia will require insulin therapy to reverse the metabolic abnormalities. Approximately 30% of children with newly diagnosed T1DM are ill with DKA.40 Many require treatment in an intensive care unit. Most of the other 70% are not acutely ill and do not require hospitalization for medical management unless facilities for prolonged outpatient care and self-management education are not available. The ADA recommends that every child newly diagnosed with T1DM be evaluated by a diabetes team (consisting of a pediatric endocrinologist, a nurse educator, a dietitian, and a mental health professional) qualified to provide up-to-date pediatric-specific education and support.59
Proper diabetes education for a child and family of a child with T1DM is intensive, complex, and age specific. Educators with a set of skills including good communication, compassion, sensitivity, spontaneity, humor, and in-depth knowledge of childhood diabetes establish the foundation of the diabetes support network. The substantial educational material (necessary for basic management, often referred to as survival skills ) must be conveyed to a family of a child with T1DM immediately after the initial diagnosis. The family is likely to be adjusting to the shock and perhaps anger or grief over the diabetes diagnosis and may not be able to focus on learning new material. The PCP may assist by becoming a source of continued medical support for the patient and the family. Insist that the patient always wear a form of identification, especially when an adolescent with diabetes begins to drive. Emphasis should always be placed on having the family join the ADA and becoming active participants in their local chapter activities.
Preconception planning should begin with the PCP. Making certain that patients' routine vaccinations are up to date is also within the responsibilities of primary care. Occasionally, family physicians may need to discuss treatment plans with school nurses and even help design updated emergency protocols for entire school districts for patients with T1DM. Consider becoming an advocate for patients with diabetes who wish to participate in extracurricular activities. PCPs can also provide basic nutritional education for school-age children, encouraging them to make healthful food and drink choices while increasing their activity levels. Adolescent girls should be observed for
P.390
signs of eating disorders, especially bulimia. Become a teacher of diabetes for all patients, regardless of their ages. As PCPs become more confident in their ability to manage diabetes, they will witness a tremendous growth in their practice census. Group classes for patients with diabetes and their families can be held in the medical office setting or in a local community center, if additional space is needed.
Enthusiasm for embracing the target achieved by the intensively treated adult cohort of the Diabetes Control and Complications Trial (DCCT) is tempered by the recent results of Epidemiology of Diabetes Interventions and Complications (EDIC),60 the follow-up study of DCCT participants. Of the DCCT trial participants, 95% participated in EDIC; of the adolescent cohort, 90% participated. After the closeout of the DCCT, most EDIC participants were converted to or continued on intensified diabetes management (95% of the prior intensive cohort and 80% of the prior conventional cohort). This intensified management was provided in a nontrial setting, with visits every 3 months and contact with the diabetes care team initiated by the patient, as deemed necessary. The EDIC study showed an increase in A1C levels in those adolescents in the intensive treatment group (from 8.1% to 8.4%) and a decrease in those in the conventional group (from 9.8% to 8.5%) after the end of the study. These data suggest that although intensification of treatment outside of a clinical trial can decrease A1C significantly, achieving an A1C consistently less than 8% outside of a clinical trial may be difficult in the adolescent population.
Despite the difficulty of achieving A1C values close to 7%, results from the EDIC also suggest that intensive diabetes management has significant and long-lasting health benefits. The adolescents in the intensive-treatment cohort of the DCCT had little further progression to proliferative retinopathy 4 years after the DCCT, whereas the previously conventionally treated group (A1C 9.8% at the end of the DCCT) had progression in an additional 15% of participants 4 years after close of the DCCT, despite their more than 1% decline in A1C (from a mean of 9.8% to 8.5%). Data from the EDIC study suggest that 4 to 7 years of intensified management may have prolonged beneficial effects (Fig. 8-3). Conversely, 4 to 6 years of suboptimal diabetes control, as frequently seen during adolescence, may have lasting adverse effects on the risk of micro- and macrovascular disease. Thus, one should attempt to optimize diabetes treatment as early as possible once the diagnosis is made.
In selecting glycemic goals, the difficulty in achieving an optimal A1C must be balanced against the disadvantages of targeting a higher (although more achievable) goal that may not promote optimal long-term health outcomes. In addition, the benefits of improved glycemic control in children must be balanced with careful consideration of the child's unique vulnerability to hypoglycemia. To address these unique needs of the developing child, age-specific glycemic goals are presented for children younger than 6 years, 6 to 12 years of age (prepubertal), and 13 years of age (or pubertal) to adulthood in Table 8-11.
As adolescents approach adulthood, the glycemic standards should approach those for adults. The adult standards of glycemic control are virtually
P.391
impossible to achieve in the adolescent population, the only age group in whom substantial evidence-based data exist. Investigators in the DCCT were able to control diabetes in this age group only at a level approximately 1% higher than that achieved by adults. Hypoglycemia and the fear of inducing hypoglycemia is the rate-limiting step to achieving ideal glycemic control safely in all age groups.
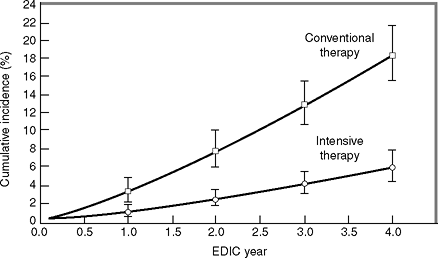 |
Figure 8-3 Results of the EDIC Trial Demonstrating the Importance of Early Intensive Intervention in the Reduction of Retinopathy. The EDIC study showed an increase in A1C levels in those adolescents in the intensivetreatment group (from 8.1% to 8.4%) and a decrease in those in the conventional group (from 9.8% to 8.5%) after study's end, despite the difficulty of achieving A1C values close to 7%. Results from the EDIC also suggest that intensive diabetes management has significant and longlasting health benefits. Note that this graph represents the cumulative data on 1,208 patients (including adults and adolescents) at the conclusion of the 4-year EDIC study. The vertical bars represent the 95% confidence intervals. (Used with permission from The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Retinopathy and nephropathy in patients with type 1 diabetes 4 years after a trial of intensive therapy. N Engl J Med. 2000;342:381 389. Erratum in N Engl J Med. 2000;342:1376.) |
TABLE 8-11 Glycemic Goals for Children and Adolescents | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
P.392
Use of Insulin in Type 1 Diabetes
Although no one established formula exists for determining a child's insulin requirement, dosing is usually based on body weight, age, and pubertal status. Children newly diagnosed with T1DM require an initial total daily dose of approximately 0.5 to 1.0 U per kg. The small insulin needs of infants and toddlers may require diluted insulin (U-40 or U-50 insulin) to allow more precise dosing and measurement of insulin in less than 1-U increments. Diluents are available for specific types of insulins from the manufacturers. Insulin can be diluted either at a pharmacy or at home once parental training has been completed. Insulin pens that deliver insulin in 0.5-U increments also are available (NovoPen Junior-Novo Nordisk: http://www.insulindevice.com/).
Newly diagnosed children with T1DM frequently enter into a honeymoon phase as their own beta-cell insulin production is restored. Data from the DCCT indicate that some subjects with T1DM continue to have residual C-peptide, even 5 years after diagnosis.61 During this phase of diabetes, insulin requirements may be well below the initial dose of 0.5 to 1.0 U per kg per day needed to maintain blood glucose targets. Minute doses of insulin should be used by patients who are honeymooning, in hope of prolonging this initial phase of new-onset type 1 diabetes. A twice-daily fixed-dose mixed-analogue insulin may also be used at this time. In general, intensive physiologic therapy in the form of a basal-bolus regimen (utilizing either MDIs or insulin pump therapy) should be prescribed to children and adolescents with T1DM. Glargine and detemir insulin are both Food and Drug Administration (FDA) approved for use in patients ages 6 and older. Regular insulin or a short-acting insulin analogue is used before meals, with the dose based on the preprandial glucose level as well as the amount of carbohydrates consumed during the meal. In small children, carbohydrate counting can be performed by the adult after the child finishes eating, after which the appropriate dose of insulin is determined and injected. Chapters 5 and 6 provide specific insulin protocols for patients who are placed on either MDIs or continuous subcutaneous insulin infusion (CSII) therapy. Table 8-12 lists age-specific diabetes self-management skills that should be emphasized for patients and families living with T1DM.
Medical Nutrition Therapy
The most difficult and most challenging aspect of diabetes management in T1DM for children involves nutritional therapy. Consultation with a registered dietician trained in pediatric nutrition and diabetes is strongly encouraged. Individualized meal plans should be designed to accommodate food preferences, cultural influences, physical activity patterns, and family meal schedules. Most important, patients and families must learn to anticipate the effect that different foods will have on glycemic excursions. For example, patients receiving insulin-pump therapy may need to use an extended-wave bolus while eating ice cream, but a dual-wave bolus for a regularly scheduled meal. Pizza, which is laden with fat and carbohydrates, will require a
P.393
P.394
dual-wave bolus, with more insulin being placed on the extended-wave portion than for the initial bolus. The patient may need to dose the insulin over a 5- to 6-hour period instead of the usual 2 to 3 hours after such a meal. Patients need to be informed that all snacks require insulin supplementation. A trip to the movie theatre where popcorn is eaten will cost 2 to 3 units of insulin. Failure to dose insulin for snacks will result in hyperglycemia, short-term insulin resistance, and worsening of the A1C levels.
TABLE 8-12 Appropriate Diabetes Self-management Skills by Age Group | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
Of critical importance is reminding adolescents that alcohol plus insulin without the use of food can result in severe hypoglycemia. Those patients who insist on drinking alcohol should always dose insulin and consume carbohydrates at the same time. Although using injections in front of peers may not be cool, point out that the patient should feel very proud of his or her efforts to manage diabetes, and do not hesitate to offer some words of encouragement.
How many of your buddies are checking their blood sugars 5 times a day and injecting insulin 4 times a day? How many of your friends can count carbs? No one. Only you. Diabetes is a bummer, but give yourself credit for what you are able to do. Your friends have a normally functioning pancreas. You don't, so you are doing everything by hand. I'm very proud of you and so are your parents. Keep up the good work, and let me know if you ever have any questions or concerns.
At the time of the initial diagnosis of T1DM, many patients appear in a malnourished and dehydrated state. Once insulin therapy is initiated, weight
P.395
gain and nutritional status improve. Patients' growth parameters should be carefully monitored. Pediatric growth charts are available at http://www.cdc.gov/growthcharts. As patients gain weight and begin puberty, their insulin requirements will also increase dramatically. Frequent changes of insulin will be needed. Monthly or even weekly dose alterations are needed when the child is growing rapidly. Insulin requirement may increase to 1.6 to 2 U per kg per day. Children and adolescents should be fed to satiety, whereas insulin doses are adjusted to meet the caloric requirements of growing children. A major effort must be made to keep up with these changing caloric and insulin needs so that appropriate growth and development are not compromised.
Once the growth spurt is over, usually around 12 to 13 years of age in girls and 15 to 18 years of age in boys, caloric needs and insulin requirement will decrease. This is particularly true in girls, because rapid growth ceases soon after the onset of menses. In boys, the growth spurt starts later than that in girls and ceases later and more slowly.
Eating Disorders in Adolescents with Type 1 Diabetes
Although the DCCT provided indisputable evidence linking intensive diabetes control to a reduced incidence of microvascular complications, metabolic control during adolescence is very difficult to achieve. The many factors responsible for deterioration of glycemic control during adolescence include increasing insulin resistance associated with onset of puberty, the psychological challenges associated with a perception of increased self-independence favoring nonadherence, and eating disorders.
The link between eating disorders, poor metabolic control, recurrent DKA, premature development of diabetes-related complications, and earlier-than-expected mortality in adolescent girls and young adult women with T1DM was initially reported in 1980.62,63 Subsequent research has provided the following evidence-based conclusions regarding eating disorders and T1DM:
All eating disorders are twice as common in adolescent girls with T1DM as in their nondiabetic peers.64
Eating disorders are associated with higher A1C levels and earlier-than-expected complications, particularly retinopathy.65
Adolescent girls with T1DM omit insulin to achieve weight control or weight loss.64,66
Treatment interventions for eating disorders in adolescents with T1DM have not been highly successful.67
On the basis of criteria from the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV), the prevalence of eating disorders is approximately 10% of all adolescent girls with T1DM64 or twice as common as in adolescent girls without diabetes. The diagnosis of T1DM during adolescence is typically associated with a period of poor metabolic control and subsequent weight loss. Although the patient may be highly symptomatic, the weight reduction, which may occur rapidly, is all too often perceived as being highly desirable.
P.396
Once insulin therapy is initiated, and metabolic control improves, the patient invariably will gain weight. Teenagers, especially girls, will view this weight gain as a negative consequence of having diabetes rather than a positive attribute associated with improved metabolic control. Adolescents are also subjected to nutritional education, which may be perceived as being rigid or too restrictive. Although carbohydrate counting allows patients to dose insulin based on the amount of carbohydrates they consume without limiting food quantity, younger patients tend to perceive carbohydrate counting as also being too restrictive. As weight increases, deliberate insulin omission or dose manipulation becomes the most common method of purging among girls with diabetes in a dangerous attempt to induce hyperglycemia and calorie-consuming glycosuria.68
Patients with poor family relationships defined by impaired communication, parental mistrust, feelings of anger or hopelessness within the home environment have an increased likelihood of developing an eating disorder and having a more treatment-resistant illness.69 In particular, a communication disconnect between the adolescent girl patient and her mother fuels the efforts of the patient to gain control of her life through weight manipulation.70
Metabolic control and A1C levels tend to deteriorate during adolescence, more so in girls than in boys, coinciding with the period of highest risk for eating disorders, from mid to older adolescence into young adulthood.70
Short-term complications related to eating disorders include recurrent episodes of DKA, hypoglycemia (due to food restriction after the administration of insulin), and frequent hospitalizations. Persistence of eating disorders can cause growth impairment, delay in pubertal development, amenorrhea, and osteoporosis.70
Managing patients with eating disorders requires specialized care. Therapists must find a balance between promoting behavioral change and accepting the adolescents' difficulties in achieving dietary self-regulation. Treatment strategies that should be considered include the following:
Maintain food diaries, blood glucose logs, insulin dosing logs, and insulin dose omission records. Although many patients object to keeping these records because they fear the connection between hyperglycemia and complications, self-monitoring does increase one's awareness of the diabetes and provides a connection between various behaviors.
Some insulin is better than none. Consider changing the patient from multiple daily injections of insulin to twice-daily mixed insulin analogues. Inhaled insulin, as a novel therapy, may also be considered for prandial administration.
Teach appropriate management of hypoglycemia. Patients may view an episode of hypoglycemia as an opportunity to binge eat. This will cause weight gain. Focus on prevention of hypoglycemia with the use of oral glucose tablets when appropriate.
Prepare patients for the possibility of weight gain with the use of insulin. Insulin is a growth hormone and will result in weight gain in most patients.
P.397
Weight can be managed successfully by learning basic dietary and behavioral principles.Address the fact that the strong emotional aspects of diabetes self-management can be managed without resorting to binge eating or purging. Patients can accept the feelings of imperfection without attempting to diminish them through weight restriction.
Family support and interpersonal relationships must be addressed. Patients must be provided with skills to manage these relationships on a long-term basis. Family-based interventions have a high rate of success.70
Sick Days
Illness can be a very stressful time for a child with diabetes and for his or her family. Illness will almost always increase the blood glucose levels, even as nutritional intake is decreased. Cases of gastroenteritis associated with minimal nutritional supplementation may result in hypoglycemia. Many parents and teens will omit insulin during illness when intake is decreased. In most instances, this is a mistake and may result in DKA.
During illness, blood glucose levels and urine ketones should be monitored frequently, often hourly, and extra insulin administered to prevent DKA. Many methods exist for supplementing insulin during illness.
Supplemental doses of rapid-acting insulin equal to 10% to 20% of the daily insulin dose may be given as an extra dose as needed to clear the ketones or control the blood glucose levels.
Whatever methods are used to calculate supplemental doses of insulin, fluid and electrolyte balance must be maintained and calories given in the form of simple sugar or glucose.
Guidelines for appropriate rehydration in the child's specific age group should be followed. If dehydration occurs, insulin is not absorbed well, and no amount of subcutaneous or even intramuscularly administered insulin may be sufficient to correct the problems.
Managing Glycemic Control in Children and Adolescents with Type 1 Diabetes during Exercise
Exercise provides many healthy benefits for children with T1DM and should be encouraged. However, up to 10% to 20% of all hypoglycemia in children and adolescents will occur in relation to a period of increased physical activity.71 Therefore, blood glucose levels should be monitored before and up to 6 hours after the completion of any exercise session until glycemic patterns can be clearly identified. Strenuous exercise with a blood glucose level less than 100 mg per dL should be preceded by a 15-g carbohydrate snack. Any exercise lasting longer than 1 hour should necessitate blood glucose testing every 30 minutes. Pre-exercise insulin-dose adjustments and carbohydrate ingestion may be necessary during the 30 to 60 minutes of daily exercise recommended by the CDC.
P.398
P.399
TABLE 8-13 Screening and Management of T1DM Comorbidities in Children and Adolescents | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
Children should be advised never to swim unsupervised and always to wear their diabetes ID bracelet during exercise. Obese children with T1DM should be encouraged to increase their level of physical activity. Exercising (riding a bike, walking to school) may be easier for many children than reducing their caloric intake.
The other comorbidities associated with T1DM in children and adolescents, including autoimmune hypothyroidism, celiac disease, microalbuminuria, hypertension, hyperlipidemia, and retinopathy, must all be screened for and managed. Table 8-13 summarizes the suggested protocols for total metabolic management of children with T1DM.
P.400
Continuous Subcutaneous Insulin Infusion (Insulin Pump) Therapy in Children and Adolescents
Insulin pump therapy is a safe and effective treatment strategy for children of all ages with T1DM.72 In an attempt to limit hypoglycemia by making insulin absorption more physiologic, 9 patients ranging from age 1.7 to 6.1 years used CSII for 1 year.73 One concern was a possible increase in occurrence of DKA should the infusion set become disconnected. When compared with 10 aged-matched controls using MDIs, their A1C values at the conclusion of the trial were identical, as were the recorded frequencies of hypoglycemia, dosages of insulin, and quality of life. No DKA occurred in the pump users, and the patients did not inappropriately disconnect their infusion sets. The authors concluded that CSII can be used safely in very young children, provided the family is given appropriate instructions and backup.
A study of 95 children and adolescents placed on insulin pump therapy, ranging in age from 4 to 18, showed improvement in A1C levels (8.1% to 7.7%) and had fewer episodes of DKA and fewer emergency department visits compared with pre-pump data. Only 2 of the 95 children discontinued their pumps, preferring to return to MDIs. Thus, insulin pump therapy is safe and advantageous in all patients with diabetes, including children, adolescents, and pregnant women.74
The use of continuous glucose sensors, alone or as a component of the sensor-augmented insulin pump, can help to improve A1C levels, minimize hypoglycemic and hyperglycemic excursions, and fine-tune one's overall glycemic control.75 A comprehensive approach to using insulin pumps in a primary care practice can be found in Chapter 6.
Summary
PCPs are likely to become directly involved with the care of many types of patients with diabetes, including children, adolescents, and women with diabetes who either plan a pregnancy or successfully become pregnant. Although specialty consultation is necessary for these patients, the PCP often provides a strong cornerstone of therapy revolving around complication surveillance, disease prevention, and counseling. A patient with a history of gestational diabetes is at high risk for diabetes developing in the future. Physicians should also ask the patient about the weight of her baby at birth at the time of her GDM pregnancy. A low birth weight (<2.5 kg) or a weight more than 4 kg places the child at high risk of metabolic syndrome developing as an adolescent. Therefore, these children should be appropriately screened for metabolic syndrome and managed with appropriate behavioral and lifestyle interventions at an early age.
One of the best ways primary care doctors can efficiently assist in the management of their diabetes patients is by promoting healthful lifestyle choices, such as exercise, to our young children who might be at risk for T2DM developing. Family physicians are in a unique position of knowing a
P.401
patient's family history, birth weight, and obstetric/gynecologic (OB/GYN) history. A patient identified as having a birth weight more than 4 kg, a father who has T2DM, a mother who has hyperlipidemia, and a history of gestational diabetes would certainly benefit from an aggressive lifestyle-intervention program. That patient will also require additional interventions for other metabolic abnormalities including hypertension, obesity, hyperlipidemia, and coronary artery disease.
One must always attempt to attain the individualized glycemic and metabolic targets established for patients with T1DM and T2DM, especially those who are planning to become pregnant or who are successful in becoming pregnant. Children with diabetes have glycemic goals that are different from those of adults. We must be vigilant in protecting them against hypoglycemia while doing our best to prescribe a regimen that offers the safest and most efficient route towards attaining the ideal A1C. Adolescent patients present unique challenges to all physicians. PCPs should be vigilant in identifying patients suspected of having eating disorders, as failure to do so could lead to frequent hospitalizations and premature retinopathy.
Managing diabetes is not easy. If hypoglycemia never occurred, patients would not need to seek our expertise on medication use, diet, exercise, pregnancy, or even home blood glucose monitoring. As professionals, we can make a difference in the lives of our patients. They are counting on us to guide them through this maze of uncertainty and fear. We must also keep a watchful eye on our young female patients with T1DM, who have a high incidence of eating disorders associated with frequent hospitalizations, DKA, and premature retinopathy. Failure to recognize this pathology may lead to devastating psychological and physiological consequences.
Around every corner of diabetes supervision and education lies another potential short- or long-term complication. PCPs have the unique ability to see around these dangerous corners and lead our patients into a safe haven of living complication-free lives.
References
1. Reece EA, Hobins JC. Diabetic embryopathy: pathogenesis, prenatal diagnosis, and prevention. Obstet Gynecol Surv. 1986;41:325 335.
2. Hare JW, White P. Pregnancy in diabetes complicated by vascular disease. Diabetes. 1977;26:953 955.
3. Miodovnik M, Lavin JP, Knowles HC, et al. Spontaneous abortions among insulin-dependent diabetic women. Am J Obstet Gynecol. 1984;150:372 375.
4. Greene MF. Prevention and diagnosis of congenital anomalies in diabetic pregnancy. Clin Perinatol. 1993;20:533 547.
5. Hanson U, Persson B. Epidemiology of pregnancy-induced hypertension and preeclampsia in type 1 (insulin-dependent) diabetic pregnancies in Sweden. Acta Obstet Gynecol Scand. 1998;77:620 624.
6. Carroll MF, Schade DS. Ten pivotal questions about diabetic ketoacidosis. Answers that clarify new concepts in treatment. Postgrad Med. 2001;110:89 93. Available online: http://www.postgradmed.com/issues/2001/11_01/carroll.htm. Accessed and verified 12/30/06.
P.402
7. Coustan DR, Berkowitz RL, Hobbins JC. Tight metabolic control of overt diabetes in pregnancy. Am J Med. 1980;68:845 852.
8. Cousins L. The California Diabetes and Pregnancy Program: a statewide collaborative program for the preconception and prenatal care of diabetic women. Clin Obstet Gynecol. 1991;6: 443 460.
9. Willhoite MG, Bennert HW, Palomaki GE, et al. The impact of preconception counseling on pregnancy outcomes: the experience of the Maine Diabetes in Pregnancy Program. Diabetes Care. 1993;16:450 455.
9a. Temple RC, Aldridge VJ, Murphy HR. Prepregnancy care and pregnancy outcomes in women with type 1 diabetes. Diabetes Care. 2006;29:1744 1749.
9b. Johnson K, Posner SF, Biermann J, et al. MMWR. Recommendations to improve preconception health and health care United States. A Report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. April 21, 2006 / 55(RR06);1 23.
10. Holing EV, Beyer CS, Brown ZA, Connell FA. Why don't women with diabetes plan their pregnancies? Diabetes Care. 1998;21:889 905.
11. Unger J. Preconception management of women with type 1 diabetes. Female Patient. 2001; 26:40 46.
12. Temple R, Aldridge V, Greenwood R, et al. Association between outcome of pregnancy and glycaemic control in early pregnancy in type 1 diabetes: population based study. Br Med J. 2002;325:1275 1276.
13. Hanson U, Persson B, Thunell S. Relationship between hemoglobin A1C in early type 1 (insulin-dependent) diabetic pregnancies and the occurrence of spontaneous abortions and fetal malformations in Sweden. Diabetologia. 1990;33:100 104.
14. Laatikainen L, Teramo K, Hieta-Heikurainen H, Koivisjov V, Pelkonen R. A controlled study of the influence of continuous subcutaneous insulin infusion on diabetic retinopathy during pregnancy. Acta Med Scand. 1987;221:367 376.
15. Jordan M, Hundal R. Gestational diabetes. Pract Diabetol. 2005;24:6 13.
16. American Diabetes Association. Gestational diabetes mellitus. Diabetes Care. 2004;27(suppl 1): S88-S90).
17. Naylor DC, Phil D, Sermer M, et al. Selective screening for gestational diabetes mellitus. N Engl J Med. 1997;337:1591 1596.
18. Casey BM, Lucas MJ, Mcintire DD, Leveno KJ. Pregnancy outcomes in women with gestational diabetes compared with the general obstetric population. Obstet Gynecol. 1997;90: 69 73.
19. Walkinshaw SA. Dietary regulation for gestational diabetes. Cochrane Database Syst Rev. 2003(2):CD000070.
20. Metzger BE. Summary and recommendations of the Third International Workshop-Conference on Gestational Diabetes Mellitus. Diabetes. 1991;40(suppl 2):197 201.
21. Artal R, Dorey FJ, Kirschbaum TA. Effect of maternal exercise on pregnancy outcome, In: Artal R, Wiswell RA, Drinkwater BL, eds. Exercise in Pregnancy. 2nd ed. Baltimore: Williams & Wilkins, 1991:225 229.
22. American Diabetes Association. Gestational Diabetes Mellitus. Position Statement. Gestational diabetes mellitus. Diabetes Care. 2003;26(suppl 1):S103-S105.
23. Langer O. When diet fails: insulin and oral hypoglycemic agents as alternatives for the management of gestational diabetes mellitus. J Matern Fetal Neonatal Med. 2002;11:218 225.
24. Kjos SL, Buchanan TA. Gestational diabetes mellitus. N Engl J Med. 1999;341:1749 1756.
25. Ziegler MH, Grafton TF, Hansen DK. The effect of tolbutamide on rat embryonic development in vitro. Teratology. 1993;48:45 51.
26. Elliott BD, Schenker S, Langer O, Johnson R, Prihoda T. Comparative placental transport of oral hypoglycemic agents in humans: a model of human placental drug transfer. Am J Obstet Gynecol. 1994;171:653 660.
27. Langer O, Conway DL, Berkus MD, Xenakis EM, Gonzales O. A comparison of glyburide and insulin in women with gestational diabetes mellitus. N Engl J Med. 2000;343:1134 1138.
P.403
28. ACOG. Practice bulletin: clinical management guidelines for obstetrician-gynecologists. Number 30, September 2001 (replaces Technical Bulletin Number 200, December 1994). gestational diabetes. Obstet Gynecol. 2001;98:525 538.
29. Glueck CJ, Wang P, Goldenberg N, Sieve-Smith L. Pregnancy outcomes among women with polycystic ovarian syndrome treated with metformin. Hum Reprod. 2002;17:2858 2864.
30. Diamond T, Kormas R. Possible adverse fetal effects of insulin lispro. N Engl J Med. 1997;337:1009.
31. Wyatt JW, Frias J, Hoyme E, et al. Congenital anomaly rate in offspring of women with diabetes treated with Humalog. Diabetologia. 2003;46(suppl 2):A259.
32. Gamson K, Chia S, Jovanovic L. The safety and efficacy of insulin analogs in pregnancy. J Matern Fetal Neonatol Med. 2004;15:26 34.
33. Ratner R, Bode B, Jovanovic L. Insulin analogs. Program of the 11th annual meeting of the AACE. May 1 5, 2002. Chicago, Illinois.
34. Di Cianni G, Volpe L, Lencioni C, et al. Use of insulin glargine during the first weeks of pregnancy in 5 type 1 diabetic women. Diabetes Care. 2005;28:982 983.
35. Challier JC, Haugel S, Desmaizieres V. Effects of insulin on glucose uptake and metabolism in the human placenta. J Clin Endocrinol Metab. 1986;62:803 807.
36. Boskovic R, Feig DS, Derewlany L, et al. Transfer of insulin lispro across the human placenta: in vitro perfusion studies. Diabetes Care. 2003;26:1390 1394.
37. Harris GD, White RD. Diabetes management and exercise in pregnant patients with diabetes. Clin Diabetes. 2005;23:165 168.
38. Harris GD. Exercise and the pregnant patient: a clinical overview. Woman Health Primary Care. 2005;8:79 86.
39. Kim C, Newton KM, Knopp RH. Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care. 2002;25:1862 1868.
40. Jovanovic-Peterson L, Peterson C. The art and science of maintenance of normoglycemia in pregnancies complicated by insulin-dependent diabetes mellitus. Endocr Pract. 1996;2:130 143.
41. Jovanovic L. Role of diet and insulin treatment of diabetes in pregnancy. Clin Obstet Gynecol. 2000;43:46 55.
42. Fagot-Campagna A, Petitt DJ, Engelgau MM, et al. Type 2 diabetes among North American children and adolescents: an epidemiologic review and a public health perspective. J Pediatr. 2000;136:664 672.
43. Centers for Disease Control and Prevention. National Diabetes Fact Sheet: general information and national estimates on diabetes in the United States. 2003. Rev. ed. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2004.
44. American Diabetes Association. Type 2 diabetes in children and adolescents. Am Diabetes Assoc Diabetes Care. 2000;23:381 389.
45. Krakoff J, Lindsay RS, Looker HC, et al. Incidence of retinopathy and nephropathy in youth-onset compared with adult-onset type 2 diabetes. Diabetes Care. 2003;26:76 81.
46. Banerji M, Chaiken R, Huey H, et al. GAD antibody negative NIDDM in adult black subjects with diabetic ketoacidosis and increased frequency of human leukocyte antigen DR3 and DR4: Flatbush diabetes. Diabetes. 1994;43:741 745.
47. Hegele RA, Zinman B, Hanley AJ, et al. Genes, environment and Oji-Cree type 2 diabetes. Clin Biochem. 2003;36:163 170.
48. Zimmet P, Alberti KG, Shaw J. Global and societal implications of the diabetes epidemic. Nature. 2001;414:782 787.
49. Kimm SY, Glynn NW, Kriska AM, et al. Longitudinal changes in physical activity in a biracial cohort during adolescence. Med Sci Sports Exerc. 2000;32:1445 1454.
50. Gungor N, Arslanian S. Pathophysiology of type 2 diabetes mellitus in children and adolescents: treatment implications. Treat Endocrinol. 2002;1:359 371.
51. Scott R, Brown L. Rates and causes of mortality in IDDM: a nine year follow-up study [abstract]. Diabetes. 1997;46(suppl 1):146A.
52. Lewy VD, Danadian K, Witchel SF, Arslanian S. Early metabolic abnormalities in adolescent girls with polycystic ovarian syndrome. J Pediatr. 2001;138:38 44.
P.404
53. Bhargava SK, Sachdev HS, Fall CH, et al. Relation of serial changes in childhood body-mass index to impaired glucose tolerance in young adulthood. N Engl J Med. 2004;350:865 875.
54. Silverman BL, Metzger BE, Cho NH, Loeb CA. Impaired glucose tolerance in adolescent offspring of diabetic mothers: relationship to fetal hyperinsulinism. Diabetes Care. 1995; 18:611 617.
55. Glowinska B, Urban M, Koput A: Cardiovascular risk factors in children with obesity, hypertension and diabetes: lipoprotein(a) levels and body mass index correlate with family history of cardiovascular disease. Eur J Pediatr. 2002;161:511 518.
56. Alberti G, Zimmet P, Shaw J, et al. Type 2 diabetes in the young: the evolving epidemic: the International Diabetes Federation Consensus Workshop. Diabetes Care. 2004;27:1798 1811.
57. Jones KL, Arslanian S, Peterokova VA, Park J-S, Tomlinson MJ. Effect of metformin in pediatric patients with type 2 diabetes. Diabetes Care. 2002;25:89 94.
58. Zuhri-Yafi MI, Brosnan PG, Hardin DS. Treatment of type 2 diabetes in children and adolescents. J Pediatr Endocrinol Metab. 2002;15(suppl 1):541 546.
59. Silverstein J, Klingensmith G, Copeland K, et al. Care of children and adolescents with type 1 diabetes: a statement of the American Diabetes Association. Diabetes Care. 2005;28:186 212.
60. Diabetes Control and Complications Trial Research Group. Effect of intensive therapy on the microvascular complications of type 1 diabetes mellitus. JAMA. 2002;287:2563 2569.
61. Diabetes Control and Complications Trial Research Group. Effect of intensive therapy on residual beta-cell function in patients with type 1 diabetes in the Diabetes Control and Complications Trial: a randomized, controlled trial. Ann Intern Med. 1998;28:517 523.
62. Gomez J, Dally P, Isaacs AJ. Anorexia nervosa in diabetes mellitus. Br Med J. 1980;281:61 62.
63. Fairburn CG, Steel JM. Anorexia nervosa in diabetes mellitus. Br Med J. 1980;280:1167 1168.
64. Jones JM, Lawson ML, Daneman D, et al. Eating disorders in adolescent females with and without type 1 diabetes: cross sectional study. Br Med J. 2000;320:1563 1566.
65. Steel JM, Young RJ, Lloyd GG, et al. Clinically apparent eating disorders in young diabetic women: associations with painful neuropathy and other complications. Br Med J. 1987;294: 859 862.
66. Rydall AC, Rodin GM, Olmsted MP, et al. Disordered eating behavior and microvascular complications in young women with insulin-dependent diabetes mellitus. N Engl J Med. 1997;336:1849 1854.
67. Peveler RC, Fairburn CG. The treatment of bulimia nervosa in patients with diabetes mellitus. Int J Eating Disord. 1992;11:45 53.
68. Fairburn CG, Peveler RC, Davies B, et al. Eating disorders in young adults with insulin dependent diabetes mellitus: a controlled study. Br Med J. 991;303:17 20.
69. Daneman D, Rodin G, Jones J, et al. Eating disorders in adolescent girls and young adult women with type 1 diabetes. Diabetes Spectrum. 2002;15:83 105.
70. Maharaj SI, Rodin GM, Olmsted MP, et al. Eating disturbances, diabetes and the family: an empirical study. J Psychosom Res. 1998;44:479 490.
71. Austin A, Warty V, Janosky J, Arslanian S. The relationship of physical fitness to lipid and lipoprotein(a) levels in adolescents with IDDM. Diabetes Care. 1993;16:421 425.
72. Maniatis AK, Klingensmith GJ, Slover RH, Mowry CJ, Chase HP. Continuous subcutaneous insulin infusion therapy for children and adolescents: an option for routine diabetes care. Pediatrics. 2001;107:351 356.
73. Wilson DM, Buckingham BA, Kunselman EL, et al. A two-center randomized controlled feasibility trial of insulin pump therapy in young children with diabetes. Diabetes Care. 2005;28:1519.
74. Plotnick LP, Clark LM, Brancati FL, Erlinger T. Safety and effectiveness of insulin pump therapy in children and adolescents with type 1 diabetes. Diabetes Care. 2003;26:1142 1146.
75. Deiss D, Bolinder J, Riveline JP, et al. Improved glycemic control in poorly controlled patients with type 1 diabetes using real-time continuous glucose monitoring. Diabetes Care. 2006;29:2730 2732.
EAN: 2147483647
Pages: 19