21 - Voiding Disorders
Authors: Macfarlane, Michael T.
Title: Urology, 4th Edition
Copyright 2006 Lippincott Williams & Wilkins
> Table of Contents > Part Two - Selected Topics > Chapter 21 - Voiding Disorders
Chapter 21
Voiding Disorders
Neurophysiology of Voiding
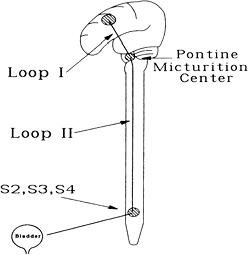
The act of micturition is a complex reflex function under voluntary control. The following diagram gives a simplified way of understanding the general neurologic innervation of the bladder and sphincter mechanisms. The coordination of the micturition reflex (i.e., detrusor contraction with sphincter relaxation) is controlled by the brainstem (pontine) micturition center via the long spinal (loop II) pathways to the sacral cord (S2, S3, S4). This in turn is under voluntary control by suprapontine higher functions via loop I.
 |
No Caption Available |
Detrusor hyperreflexia with a coordinated external sphincter is caused by suprapontine lesions involving loop I (e.g., stroke, Parkinson's disease, and tumors) as well as nonneurologic local causes (e.g., infection, outlet obstruction, tumor, stone, foreign body).
Detrusor hyperreflexia with external sphincter dyssynergia is generally caused by suprasacral spinal lesions involving loop II (e.g., tumor, multiple sclerosis, myelodysplasia, and spinal arteriovenous malformations).
P.135
Detrusor areflexia can result from interruption of sacral reflex arcs (e.g., diabetic neuropathy, multiple sclerosis, herniated disks, and spinal cord tumors), as well as direct myogenic causes (e.g., prolonged urinary retention). Areflexia also occurs during the period of spinal shock after suprasacral spinal cord injury.
Classifications of Dysfunctional Voiding
Many classification systems have been promoted for categorizing voiding disorders based on neuroanatomic, urodynamic, or functional criteria. The Wein classification system is a beautifully simplistic functional categorization based on the failure of the bladder to store or empty. It serves most clinical voiding disorders well, whether of neurogenic or nonneurogenic origin, and helps guide one toward the correct treatment options.
Functional Classification of Voiding Disorders
![]() Failure to Store
Failure to Store
Because of the bladder
Because of the outlet
![]() Failure to Empty
Failure to Empty
Because of the bladder
Because of the outlet
Failures to store because of the bladder simply include involuntary bladder contractions, low compliance, and hypersensitivity, whereas outlet problems are simply due to inadequate outlet resistance. Failures to empty because of the bladder are a result of poor or no bladder contractility, whereas outlet problems are from mechanical [e.g., benign prostatic hyperplasia (BPH), stricture] or functional (dyssynergia) obstruction. Combination deficits can also occur as in spinal cord injury (detrusor hyperreflexia and sphincter dyssynergia).
Detrusor hyperreflexia refers to involuntary bladder contractions on urodynamic studies caused by a neurologic disorder, whereas involuntary contractions without a neurologic cause are termed detrusor instability. More popular today is the general term overactive bladder, which refers to the symptoms of frequency and urgency without urodynamic confirmation of detrusor hyperreflexia or instability.
Urodynamics
Urodynamics is the study of lower urinary tract physiology. It is a complex field that includes uroflowmetry, cystometry, urethral pressure profilometry, and electromyography. Even a brief overview of all these areas is beyond the scope of this manual.
P.136
Only basic uroflowmetry and cystometry are covered because they are generally all that are required for most clinical urodynamic workups. Remember that a detailed history is the foundation of any evaluation of a voiding disorder.
Urinary Flow Rate/Residual Urine
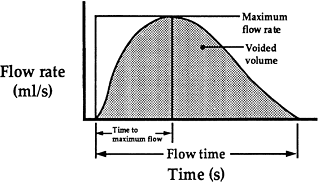
The combination of a uroflow followed by determination of the residual urine is the most useful test in the study of any voiding disorder. Urinary flow rate is best recorded on an electronic flowmeter, which plots the flow pattern in a graphic representation of instantaneous flow rate versus voiding time.
Peak uroflow rate is the only objective measure of functional bladder outlet obstruction, and it is directly dependent on the volume voided. Peak flows measured when the voided volume was less than 150 mL should be disregarded.
 |
No Caption Available |
Use of this flow nomogram allows a more accurate determination of outflow resistance by removing the effect of intravesical volume on flow rate. Peak flow rates more than two standard deviations below the mean are highly suggestive of outflow obstruction.
 |
No Caption Available |
P.137
Cystometry
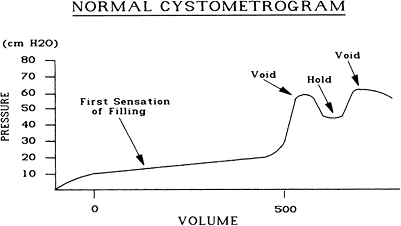
Cystometry is generally used to evaluate bladder filling and storage. A cystometrogram is a pressure/volume curve obtained by filling the bladder with a fluid (either water or carbon dioxide) at a constant infusion rate while monitoring changes in intravesical pressure. The patient is asked to inhibit any urge to void during the study. Any detrusor contractions greater than 15 cmH2O are considered abnormal or uninhibited contractions. A voiding phase cystometrogram may be obtained at the end of the study when the patient has a strong urge to void by asking him or her to voluntarily urinate around the catheter.
Data to be noted during the cystometrogram include the following:
Volume at first sensation of filling (proprioception)
Volume at sensation of fullness
Volume at desire to void
Occurrence of a voluntary detrusor contraction when asked to void
Ability to inhibit a voluntary detrusor contraction
 |
No Caption Available |
![]() Normal Cystometrogram
Normal Cystometrogram
A normal cystometrogram should demonstrate a first sensation of filling at 100 to 200 mL, normal accommodation with continued filling and good compliance (i.e., <10 cmH2O change in intravesical pressure), and a sensation of fullness and desire to urinate at 350 to 450 mL. Asking the patient to produce a voluntary detrusor contraction at the end of the study is often unsuccessful because of the patient's inability to properly relax in the test setting. Normal sensation and compliance with an absence of uninhibited contractions are all that are needed to consider the study normal.
P.138
Uropharmacology
Overview
Bladder contraction is mediated by stimulation of the parasympathetic nervous system and release of acetylcholine. Cholinergic muscarinic receptors are located in the dome of the bladder. Five muscarinic receptor subtypes (M1 M5) have been identified. M3 receptors appear to be primary in detrusor contraction, perhaps with assistance for M2 receptors.
-Adrenergic receptors in the bladder neck and urethra moderate smooth muscle contraction and increase outlet resistance on stimulation by the sympathetic nervous system. -Adrenergic receptors in the dome of the bladder facilitate accommodation during filling by causing smooth muscle relaxation in the bladder.
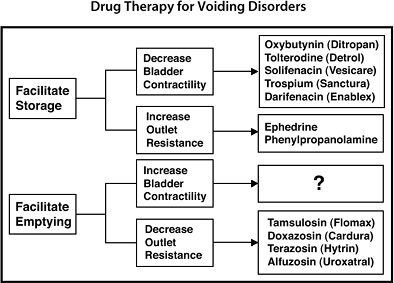
Pharmacotherapy for voiding disorders has been disappointingly ineffective on the whole. Despite the pharmacologic effectiveness of certain drugs, clinical improvement is impeded by a lack of specificity of the agent and untoward side effects on other organ systems with similar receptors at pharmacologic doses.
Drugs to Facilitate Storage
![]() Decrease Bladder Contractility
Decrease Bladder Contractility
Propantheline (Pro-Banthine) is an anticholinergic that blocks bladder contraction by competitive blockade at receptors of parasympathetic postganglionic nerve endings. It is variably effective in patients with uninhibited hyperreflexic neurogenic bladders. Side effects include dry mouth, visual disturbances, and constipation [dosage: 15 mg orally (PO) three times a day (tid)/four times a day (qid)].
Oxybutynin (Ditropan) has a direct antispasmodic effect on smooth muscle and blocks cholinergic receptors. It has variable clinical effectiveness in patients with uninhibited bladder contractions (dosage: 5 mg PO tid/qid). Oxybutynin extended release (Ditropan XL) is dosed once a day and has fewer side effects [dosage: 5 10 mg PO daily (qd)]. Oxybutynin transdermal patch (Oxytrol) is a form of immediate release oxybutynin (dosage: 3.9 mg patch twice per week).
Tolterodine tartrate (Detrol) is a competitive muscarinic receptor antagonist indicated for treatment of bladder overactivity [dosage: 2 mg PO twice a day (bid)]. An extended release
P.139
formulation of tolterodine (Detrol LA) is a once-daily formulation (dosage: 4 mg PO qd).Flavoxate (Urispas) has anticholinergic, local, anesthetic, and analgesic properties and may also have a direct relaxant effect on smooth muscle. Flavoxate has been used to reduce irritative voiding symptoms and suprapubic pain (dosage: 100 200 mg PO tid/qid).
Trospium (Sanctura) is a balanced M3/M2 selective anticholinergic (dosage: 20 mg PO bid).
Darifenacin (Enablex) is an M3 selective anticholinergic (dosage: 7.5 15 mg PO qd).
Solifenacin (VESIcare) is an antimuscarinic with smooth muscle relaxing properties (dosage: 5 10 mg PO qd).
Imipramine (Tofranil) has been shown to be clinically effective in facilitating urine storage; however, its mechanism of action is unclear. Peripheral anticholinergic and sympathomimetic actions have been noted in addition to a direct smooth muscle relaxation. Thus, it decreases bladder contractility and increases outlet resistance. It is effective for controlling bedwetting in children (dosage: 25 mg PO tid/qid).
Hyoscyamine sulfate (Levsin) is one of the principal anticholinergic/antispasmodic components of belladonna alkaloids. Hyoscyamine has been effective in the treatment of spastic neurogenic bladders [dosage: 1 2 tablets (0.125 mg) PO/sublingual (SL) q4h]. Extended release hyoscyamine (Levbid) affords better dosing (dosage: 1 tablet PO bid).
Dicyclomine (Bentyl) has direct smooth muscle relaxant and anticholinergic effects primarily indicated for irritable bowel syndrome (dosage: 20 mg PO tid).
![]() Increase Outlet Resistance
Increase Outlet Resistance
Ephedrine is an -adrenergic agonist that causes contraction of smooth muscle of the bladder outlet and urethral sphincter. Dosage is 25 to 50 mg PO qid.
Phenylpropanolamine (Ornade) is also an -adrenergic agonist and thus causes increased bladder outlet resistance secondary to smooth muscle contraction (dosage: 50 mg PO bid).
Estrogens are believed to increase outlet resistance in females with stress incontinence by increasing -adrenergic receptor sensitivity and improving the mucosal seal of the urethral wall (dosage: Estrace vaginal cream 1/2 g Monday, Wednesday, Friday).
P.140
Drugs to Facilitate Emptying
![]() Increase Bladder Contractility
Increase Bladder Contractility
Bethanechol chloride (Urecholine) is a cholinergic agonist that acts at the postganglionic parasympathetic effector cells to enhance contraction of smooth muscle. Oral Urecholine is largely ineffective clinically.
![]() Decrease Outlet Resistance
Decrease Outlet Resistance
Phenoxybenzamine (Dibenzyline) is an -adrenergic blocking agent that has been shown to be effective in blocking hyperactivity of the bladder outlet smooth muscle sphincter. However, it has negative systemic effects (orthostatic hypotension), and it has been shown to have in vitro mutagenic activity. These factors have significantly curtailed its use.
Prazosin (Minipress) is also an -adrenergic blocking agent that has been used to inhibit bladder neck contractility. Its negative effects include postural hypotension, reflex tachycardia, nasal congestion, inhibition of seminal emission, and retrograde ejaculation. Initial dosage is 1 mg bid or tid.
Terazosin (Hytrin) is a selective 1-blocking agent that has been used to relax smooth muscle fibers of the prostate and bladder neck. It requires only once a day dosing starting at 1 mg/day initially. Dosages of 2 to 10 mg/day may be necessary. Dose must be titrated.
Doxazosin (Cardura) is another selective 1-blocking agent with activity and side effects similar to those of terazosin (dosage: 2 8 mg PO qd). Dose must be titrated.
Tamsulosin (Flomax) is a highly selective antagonist of the 1a-subtype adrenoceptors. It promotes smooth muscle relaxation in the bladder neck and prostatic urethra. Dose titration is unnecessary (dosage: 0.4 mg PO qd).
Alfuzosin (Uroxatral) is an extended release selective antagonist of 1-adrenoceptors (dosage: 10 mg PO qd).
Diazepam (Valium) has striated muscle relaxant ability but has had only limited success in treating external sphincter dyssynergia at tolerable dosages.
Dantrolene (Dantrium) also has striated muscle relaxant effects but limited success in treating external sphincter dyssynergia at tolerable dosages. It has a significant risk of producing fatal hepatotoxicity and should, therefore, be avoided.
Baclofen (Lioresal) is a polysynaptic inhibitor of both the bladder and outlet with muscle relaxant and antispasmodic activity. It has some limited usefulness in treating external sphincter dyssynergia.
P.141
Management
Therapy for voiding disorders consists of surgical, pharmacologic, or mechanical interventions. After determining whether the patient has primarily a storage or an emptying disorder, the following brief lists can help guide therapy.
To Promote Storage
![]() Decrease Bladder Contractility
Decrease Bladder Contractility
Removal of local irritative factors (treat infection or tumors and remove stones or foreign bodies)
Pharmacotherapy (oxybutynin, tolterodine, solifenacin, trospium, darifenacin)
Surgery: bladder denervation (cystolysis) and augmentation cystoplasty
![]() Increase Outlet Resistance
Increase Outlet Resistance
Pharmacotherapy (ephedrine, imipramine, phenylpropanolamine)
Biofeedback or electrical stimulation
Surgery (bladder neck sling, collagen injection, artificial sphincters)
![]() Bypass Problem
Bypass Problem
Condom catheter, Foley catheter, or urinary diversion
 |
Drug Therapy for Voiding Disorders |
P.142
To Promote Emptying
![]() Increase Bladder Contractility
Increase Bladder Contractility
No clinically effective therapy
![]() Decrease Outlet Resistance
Decrease Outlet Resistance
Pharmacotherapy (terazosin, doxazosin, tamsulosin, alfuzosin, diazepam, baclofen)
Surgery: transurethral resection of the prostate, incision of strictures, urethral dilatation, urethroplasty, Y-V plasty of bladder neck, external sphincterotomy
![]() Bypass Problem
Bypass Problem
External bladder compression (Crede's method)
Catheterization: intermittent or continuous
Surgery: urinary diversion
Specific Guidelines
Failure to Store
![]() Because of the Bladder
Because of the Bladder
Infection. The local irritative effects of cystitis or prostatitis can produce significant frequency and urgency. Treat with appropriate antibiotic therapy.
Outlet obstruction. Bladder outlet obstruction from BPH or strictures produces a primary disorder of failure to empty with a secondary disorder of failure to store (i.e., frequency, urgency, and nocturia) because of bladder instability. Correction of the primary disorder will usually result in resolution of the secondary bladder instability.
Tumor. A bladder tumor can cause significant local irritability manifested by frequency and urgency. Treat the tumor.
Bladder stone. A stone can cause a primary local irritative focus in the bladder that is often compounded by a secondary infection. Removal of the stone and eradication of infection should be effective.
Poor compliance. Decreased bladder compliance is usually secondary to inflammation, obstruction, or neurogenic causes. Elimination of the primary disorder is the goal. The small fibrotic contracted bladder may require augmentation cystoplasty or urinary diversion.
Neurogenic hyperreflexia. A hyperreflexic neurogenic bladder can be managed by pharmacotherapy (oxybutynin, tolterodine, solifenacin, darifenacin) or can be converted to a failure
P.143
to empty by augmentation cystoplasty and placed on clean intermittent catheterization (CIC).
![]() Because of the Outlet
Because of the Outlet
Sphincter incompetence. Incompetent internal or external sphincter mechanisms can be managed with pharmacotherapy (ephedrine, imipramine, phenylpropanolamine) and surgical procedures (bladder neck sling, artificial sphincters). Failures must be consigned to condom catheters, Foley catheters, or urinary diversion.
Failure to Empty
![]() Because of the Bladder
Because of the Bladder
Areflexia. There is no effective means of increasing detrusor contractility. Patients are best managed with CIC, indwelling Foley catheter, or urinary diversion.
![]() Because of the Outlet
Because of the Outlet
Outlet obstruction. Mechanical outlet obstruction from BPH or strictures requires relief of the primary disorder (e.g., transurethral resection of the prostate, pharmacotherapy, or urethrotomy).
Sphincter dyssynergia. Detrusor hyperreflexia with sphincter dyssynergia is a combined disorder of a failure to store and a failure to empty. The hyperactive uncoordinated external sphincter produces a functional outlet obstruction while the detrusor hyperreflexia results in small functional bladder capacities. These patients are best managed by first converting them to a primary disorder of emptying by pharmacotherapy, cystolysis, or bladder augmentation and then using CIC to empty the bladder.
Spinal Cord Injury
Injury to the spinal cord can result in various patterns of function based on the degree and level of the injury. Initial evaluation, including urodynamic testing and intravenous urography, should be conducted approximately 8 weeks after the injury. A period of spinal shock, usually lasting several days to weeks after the injury, can be expected. During this time, cord segments below the level of the injury will demonstrate decreased excitability. Detrusor areflexia with a continent internal urethral sphincter is the rule. Intermittent or chronic catheterization will be necessary. Recovery of
P.144
reflex vesical activity with sphincter dyssynergia is the most common outcome in patients with suprasacral lesions. If intravesical pressures are elevated (>40 cm H2O), upper tract damage can be expected if treatment is not undertaken. Lesions of the sacral cord or cauda equina usually result in detrusor areflexia with low bladder pressures and can be safely managed with intermittent catheterization.
![]() Autonomic Dysreflexia
Autonomic Dysreflexia
Autonomic dysreflexia is a syndrome characterized by a major sympathetic nervous response to afferent visceral stimulation in the spinal cord injury patient. Clinical manifestations include sweating, piloerection, a pounding headache, bradycardia, a widened pulse pressure, and a subjective sense of impending doom on the part of the patient. This can occur in response to stimulation of the bladder, urethra, or rectum in patients with cord lesions above T5, usually in the cervical region, and most frequently during the period from 3 to 8 months after injury. Acute bladder filling as occurs during cystoscopy or urodynamic testing can trigger an episode. Catheter drainage of the bladder can be used to minimize chronic autonomic dysreflexia.
Treatment
Treatment of an acute episode is with nifedipine (sublingual), hydralazine, or phentolamine and removal of the afferent stimulus (i.e., drain the bladder). Chlorpromazine (Thorazine), 25 mg IM q6h, can be used prophylactically in patients with potential for such a response during cystoscopy.
EAN: 2147483647
Pages: 44