Eyes and Vision
Authors: Flaherty, Alice W.; Rost, Natalia S.
Title: Massachusetts General Hospital Handbook of Neurology, The, 2nd Edition
Copyright 2007 Lippincott Williams & Wilkins
> Table of Contents > Adult Neurology > Eyes and Vision
Eyes and Vision
A. Vision
Sudden visual loss is an emergency.
1. H&P: Time course of visual loss, eye pain, headache, fevers, joint pain, DM, check BP, ocular and carotid bruits, fundi (disc pallor, papilledema, retinopathy, arterial occlusion or cholesterol plaque, cherry red spot), red desaturation, pinhole correction, Amsler grid for metamorphopsia, size of blind spot.
a. Whenever you use dilating drops to examine the fundi, note it clearly in the chart so the next examiner will not think the pt is herniating.
2. Poor acuity: See eye chart, back endpapers. Suggests eye or optic nerve problem. If acuity corrects to normal with pinhole, the problem is in the media of the eye, not nerve.
3. Binocular blindness: Usually from a lesion at the optic chiasm (e.g., pituitary mass) or in both occipital lobes (e.g., bilateral PCA infarcts), or toxic/metabolic/nutritional unless both eyes have been exposed to the same insult (e.g., shower of emboli).
4. Monocular blindness: Transient (TMB) or permanent loss, sudden and nontraumatic.
a. Causes:
1) TMB: Embolus or thrombus, often from carotid lesion. 11% of TMB pts later have stroke, 41% of them within 1 wk. Temporal arteritis or other vasculitis .
2) Sudden permanent monocular blindness: All causes of TMB, plus optic neuritis, intraocular bleed, retinal detachment, acute angle closure glaucoma, infection .
b. Types of retinal infarct:
1) Central retinal artery: Cherry red spot seen in fundus after 6 h.
2) Branch retinal artery: Fundus pallor along that branch.
3) Anterior ischemic optic neuropathy: Often idiopathic; sometimes arteritis.
c. Tests: ESR, CRP, fibrinogen, TEE, temporal artery biopsy (within days of starting steroids). See also Stroke workup, p. 20.
d. Rx of TMB:
1) Prednisone: 60 mg qd until artery biopsy results are back. Vessel inflammation can be patchy, so if clinical suspicion is high, continue prednisone and rebiopsy.
2) IV heparin: See Anticoagulants, p. 160.
3) Decrease intraocular pressure to help move a possible embolus through the eye. Hypercarbia probably does not help.
a) Massage eye: Have pt. press hard 4 sec; off 4 sec.
b) IV mannitol 50 g, or IV acetazolamide 400 mg. Watch BP.
c) Anterior paracentesis by ophthalmologist.
e. Rx of optic neuritis: See Demyelinating Disease, p. 33.
5. Visual field defects:
a. Monocular scotoma: Prechiasmal lesion, e.g., glaucoma, retinal hemorrhage, optic neuritis, retinal detachment.
b. Noncongruent bilateral scotomata: Chiasm + nerve lesion.
c. Bitemporal defect: Chiasmal lesion, e.g., aneurysm or pituitary mass. Consider glaucoma.
d. Homonymous defect (same side in both eyes): Postchiasmal.
1) Sparing macula: Visual cortex.
2) Including macula: Optic radiations.
3) Superior quadrant defect: Optic radiations in inferior temporal lobe that can be affected by mastoid infection causing cerebritis.
4) Inferior quadrant defect: Optic radiations in parietal lobe.
6. Higher visual system abnormalities:
a. Anton's syndrome: Bilateral occipital lesions cause blindness, but pt denies he is blind.
b. Bonnet's syndrome: Visual deprivation hallucinations (formed, stereotyped, no other signs of delirium).
c. Motion and visuospatial processing: Dorsal, occipitoparietal where pathway.
P.46
1) Balint's syndrome: Visual disorientation (simultanagnosia), optic ataxia (deficit of visual reaching), ocular apraxia (deficit of visual scanning). From bilateral occipitoparietal lesion.
d. Object recognition: Ventral, occipitotemporal what pathway lesions cause visual agnosia.
1) Prosopagnosia: Inability to recognize faces; from bilateral inferior visual association cortex lesions.
2) Word blindness: Alexia without agraphia. Seen in left hemisphere lesion near splenium of callosum. Usually with R homonymous hemianopsia and color anomia or achromatopsia.
3) Achromatopsia vs. color anomia: In former, pt. cannot perceive colors; in latter, pt. can perceive them but not name them.
P.45
B. Pupils
1. Causes of anisocoria: (unequal pupils)
a. Horner's syndrome: see p. 12.
b. Third nerve lesion:
1) H&P: Unilateral large pupil; also ophthalmoplegia and ptosis. Anisocoria is worse in light (vs. Horner's). Ask about time course, comorbid conditions (e.g., DM).
2) DDx: Aneurysm (especially P-comm) > ischemia (e.g., DM or HTN) > trauma, uncal herniation, tumor, etc. In an alert pt., a fixed dilated pupil is almost never herniation.
a) Pupil involvement: Suggests compression because pupillary parasympathetic fibers are the most superficial.
b) Pupil sparing: Suggests ischemic third nerve. But only consider a lesion pupil sparing if it is otherwise a complete third nerve palsy (ophthalmoplegia and ptosis). Otherwise you may be fooled by an early compressive third.
c) R/O P-comm aneurysm: Immediate CT and LP to r/o bleed, consider angiogram. May not need this if deficit is clearly pupil sparing.
c. Drug effects:
1) Dilators (mydriatics): From sympathetic agonists, e.g., atropine, scopolamine, phenylephrine, tropicamide, albuterol. Test with 1% pilocarpine (a parasympathetic agonist); it will not constrict pupil if the pupil was previously drug dilated, but will in third nerve compression or Adie's syndrome.
2) Constrictors: From parasympathetic agonists, e.g., pilocarpine.
d. Acute glaucoma: Fixed pupil, about 6 mm. Also decreased acuity; red, painful eye; hazy cornea; blurred vision; shallow ant. chamber if side-illuminate with penlight.
1) Rx: Emergent IV acetazolamide or mannitol; topical pilocarpine.
e. Adie's (tonic) pupil: One large pupil, reacts poorly to light, with better constriction to near; then redilates sluggishly. Often sudden, in young woman, with decreased DTRs.
1) Test: Dilute pilocarpine (0.1%) will constrict Adie's pupil but not normal pupil.
f. Argyll-Robertson: Small, irregular, unequal (sometimes equal) pupils, constrict to near better than light.
1) DDx: Syphilis, diabetic pseudotabes .
g. Old ocular surgery or trauma.
h. Physiologic anisocoria: Should be less than 1 mm difference in both light and dark, briskly reactive.
P.47
2. Causes of bilateral fixed or poorly reactive pupils:
a. Bilateral large pupils:
1) Fixed: Death, subtotal medullary lesion, immediately post anoxia or hypothermia, severe hypoglycemia, bilateral or nuclear third palsy, botulism.
2) Reactive (usually): Anxiety, opiate withdrawal, aerosolized albuterol, overdose of IV dopamine, atropine, aminoglycosides, tetracycline, Mg, amyl nitrite.
b. Midsized pupils: Dorsal midbrain lesion, e.g., from hydrocephalus. May see sluggish reaction to near, as in Argyll-Robertson pupil.
c. Pinpoint pupils: Opiates, pontine lesion (usually with skew deviation or ophthalmoplegia), metabolic encephalopathy.
3. Afferent pupillary defect (APD, Marcus-Gunn pupil): Transient dilation as flashlight moves from good to bad eye. From optic neuritis or retinal lesion.
C. Fundi
1. Disk edema: Ask about pulsatile tinnitus, gray/blackouts of vision lasting a few seconds, headache, N/V, and diplopia, which are all other signs of increased ICP. Look for venous pulsations, acuity, fields.
a. Papilledema: Term reserved for disk edema due to high ICP.
b. Bilateral disk edema: Usually painless. High ICP from intracranial tumors, pseudotumor cerebri, metabolic problems .
c. Unilateral edema:
1) Visual loss and pain: Optic neuritis, infection/inflammation, temporal arteritis.
2) Visual loss, no pain: Ant. ischemic optic neuropathy from temporal arteritis or vascular risk factors.
2. Optic atrophy: Glaucoma, past neuritis, toxic/metabolic optic neuropathies, chronic papilledema.
D. Eye Movement Abnormalities
1. See also: Cranial Nerves, p. 32.
2. Acute extraocular paralysis is an emergency: Consider botulism, myasthenic crisis, P-comm aneurysm, cavernous sinus thrombosis, infection, fistula, variant Guillain-Barr syndrome.
3. H&P: Direction of greatest deficit, h/o lazy eye, drugs, thyroid dz, pain, alteration with fatigue. Note head tilt (compare with old photo), check Bell's reflex, stereopsis, ocular bruit.
a. Eye muscles:
b. Figure shows the main field of action of individual eye muscles. Have pt. track your finger in these directions; also test saccades laterally and vertically.
P.48
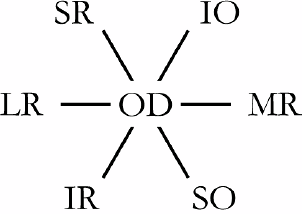
Figure 7. Direction of ocular muscle action, right eye.
c. Diplopia without visibly disconjugate gaze:
1) Red glass test: Convention is to hold it over R eye. Have pt. report relative positions of red and normal images in all directions of gaze. Diplopia is maximal in the field of gaze of the paretic muscle, and the image belonging to the paretic muscle projects peripherally.
2) Alternating cover test: For phoria (latent): shift cover to other eye while fixating. If covered eye moves in, it is exophoria; if out, it is esophoria; if down, it is hyperphoria; if up, it is hypophoria. If eyes are never conjugate (but not paralyzed), it is a tropia, not a phoria.
4. Causes of eye movement abnormalities: Nerve palsy, brainstem lesion, raised ICP with herniation, strabismus, myasthenia gravis, drugs (especially DPH), multiple sclerosis, Graves' dz, orbital entrapment, trauma, meningitis or other infection, migraine, Wernicke's syndrome, Fisher variant of GBS, mitochondrial dz.
a. Causes of painful ophthalmoplegias: Cavernous sinus tumor, thrombosis, fistula, or dissection; zoster, DM, migraine, infection, Tolosa-Hunt syndrome.
5. Bilateral conjugate gaze palsies:
a. Bilateral fixed eyes:
1) Caloric test: see p. 222.
2) Oculocephalic reflex: (Doll's eye test is a confusing term.) Do only if C-spine is stable.
b. Bilateral upgaze palsy: The main vertical gaze center is the rostral interstitial nucleus of MLF in dorsal midbrain; there may be another at the cervicomedullary junction.
1) Causes: Can tell supranuclear lesions (e.g., PSP, dorsal midbrain syndrome) from age-related eye muscle weakness by the presence of other deficits and by the following tests:
a) Bell's reflex: Eyes normally roll up when pt tries to close lids against your resistance. This reflex is intact in supranuclear lesions.
b) Vertical doll's eyes: Have pt fix on a target while you move pt.'s head. Intact in supranuclear lesions.
c) Light-near dissociation: Present in pretectal lesions. The pupil constricts better when accommodating near targets than it does to light.
2) Dorsal midbrain lesion (Parinaud's syndrome): Often from basilar stroke or pineal tumor. Upgaze worse than downgaze.
P.49
See convergence paresis, retraction nystagmus, and lid retraction ( setting sun eyes ) on attempted upgaze. May see skew deviation, light-near dissociation.
c. Bilateral downgaze palsy: Early PSP, bilateral ventral midbrain lesions, anoxic coma.
d. Bilateral lateral deviation: Contralateral cerebral hemisphere or midbrain lesion; ipsilateral pons lesion.
1) Causes: Lesion of 6th nucleus, pedunculopontine reticular formation (PPRF), parietal neglect, L frontal (in latter two, oculocephalic reflex can overcome gaze paresis).
2) vs. PPRF lesion: Although the rostral PPRF is usually affected with the 6th nerve given their close proximity, lesion of the 6th nerve nucleus involves 7th nerve as well (genu of 7th wraps around 6th nucleus), giving an ipsilateral lower motor neuron 7th palsy (forehead spared). A pure PPRF lesion spares 6th nerve function.
e. Internuclear ophthalmoplegia (INO):
1) H&P:
a) Ipsilateral eye: Poor adduction to nose.
b) Contralateral eye: Abduction nystagmus (on lateral gaze).
c) Convergence paresis: Except in very caudal lesions.
2) Location: Lesion is on side of the eye with poor adduction, in the MLF, rostral to 6th nerve nucleus (blocks path from 6th to contralateral 3rd), anywhere from pons to midbrain.
3) DDx: The elderly usually have vascular causes; young adults usually MS; children usually pontine glioma. Myasthenia can cause a pseudo-INO.
f. One-and-a-half syndrome: An INO plus horizontal gaze palsy. The ipsilateral eye cannot adduct or abduct. The contralateral eye cannot adduct and has abduction nystagmus. The lesion is lower in the pons than that causing an INO; it is at the level of the 6th nerve nucleus and involves the MLF and PPRF.
g. Congenital progressive external ophthalmoplegia (CPEO): See Mitochondrial Disorders, p. 72.
6. Skew deviation: A vertical misalignment, seen in posterior fossa and brainstem lesions.
7. Unilateral ophthalmoparesis:
a. Individual muscle palsy: See Figure 7, p. 48
b. CN III (oculomotor): See also Anisocoria (unequal pupils), p. 46.
1) H&P: Fixed and dilated pupil, ptosis, partial ophthalmoparesis. Only lateral gaze is intact, so eye is deviated down and out. Superior trunk controls upgaze and lid; inferior trunk controls downgaze and pupil.
2) Causes: Important to rule out P-comm aneurysm immediately (see p. 47). Midbrain lesion usually has contralateral hemiparesis too. Pupil-sparing palsy (ptosis plus ophthalmoparesis must be present) suggests nerve ischemia usually in setting of diabetes; also temporal arteritis or myasthenia. Often idiopathic.
c. CN IV (trochlear):
1) H&P: Diplopia on looking down and in.
2) Compensatory head tilt: Away from side of lesion. GOTS Worse Gaze Opposite, Tilt Same makes a 4th palsy Worse.
a) Chronic? Look at driver's license to see if head tilt is old.
3) Bielshowsky test: Look for hypertropia and diplopia on straight gaze, R gaze vs. L, and R head tilt vs. L tilt.
4) Causes: Closed head trauma > vascular > tumor. Often idiopathic.
P.50
d. CN VI (abducens):
1) H&P: In a nerve lesion, only the ipsilateral eye cannot look laterally. A nuclear lesion also impairs contralateral eye's ability to look towards the lesioned side.
2) Causes: Tumor (30%) > trauma, ischemic, high ICP, Graves' dz, idiopathic, Wernicke's syndrome .
3) Cavernous sinus syndromes:
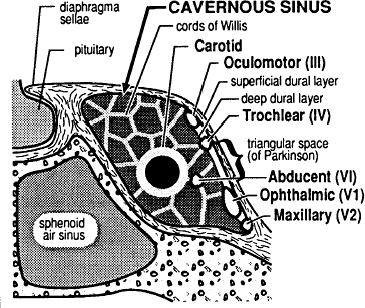
Figure 8. The cavernous sinus. (From Greenberg MS. Handbook of Neurosurgery. 3rd ed. Lakeland, FL: Greenberg Graphics; 1994: 103, with permission.)
a) H&P: Variable involvement of CN III, IV, V1-2, VI. An isolated VI palsy with a Horner's syndrome is a giveaway. Often with pain and proptosis.
b) DDx: Carotid artery aneurysm, dissection; venous thrombosis, infection, tumor, Tolosa-Hunt, Wernicke's .
c) Tolosa-Hunt syndrome: Idiopathic granuloma near the superior orbital fissure, causing pain and III, IV, or VI palsies. Responds to steroids but r/o tumors and infection first. Do not confuse Tolosa-Hunt with Ramsay-Hunt syndrome (see p. 93).
8. Nystagmus: Although jerk nystagmus is described by the direction of the fast phase, it is always a disorder of slow eye movements.
a. H&P: Note whether nystagmus is present in primary gaze; direction of fast component, whether it extinguishes with fixation. Look for accompanying palatal or facial myoclonus, which suggests denervation of the inf. olive, by damage to the central tegmental tract.
b. Causes of nystagmus: See also Vertigo, p. 127.
P.51
1) Horizontal:
a) Jerk nystagmus: Saccadic movement in one direction; slow corrective movement in the other. Causes include drugs, cerebellar or brainstem lesion, vestibular dz, congenital syndromes. A few beats of end-gaze nystagmus may be normal.
b) Pendular nystagmus: Slow movements in both directions. Drugs and vestibular causes are uncommon (unlike jerk nystagmus). Seen in congenital blindness.
2) Downbeat: Often craniocervical junction problem causing ant. cerebellar vermis lesion, e.g., with Chiari malformation. Also MS, drugs, Wernicke's syndrome .
3) Upbeat: Often medullary lesion; also MS, drugs, Wernicke's .
4) Rotatory: If in combination with horizontal nystagmus and vertigo, usually a peripheral, vestibular lesion. If pure rotatory, usually medullary or diencephalic.
9. Other ocular oscillations:
a. Square wave jerks: Small-amplitude macrosaccades on attempted fixation. Causes: Often cerebellar or demyelinating dz.
b. Ocular bobbing: Constant, conjugate down and up oscillations fast down, then slow drift back to midposition 2-12 /min, with horizontal gaze paralysis. Should distinguish it from vertical nystagmus. Causes: Often pontine lesion; sometimes metabolic or from hydrocephalus. Consider also vertical nystagmus.
c. Ocular dysmetria: Eye over- or undershoots target, then makes refixation saccades. Causes: Often cerebellar dz. Distinguish from hypometric saccades, in which eye always undershoots; a sign of extrapyramidal bradykinesia.
d. Ocular flutter: Rapid bursts of horizontal oscillations in primary gaze. Similar causes to opsoclonus.
e. Opsoclonus: Continuous, conjugate, multidirectional saccades. Often from paraneoplastic syndrome; MS, postviral opsoclonus-myoclonus; encephalitis, drugs, tumors.
E. Lids
1. Ptosis: (lid droop)
a. Unilateral ptosis: Horner's, third nerve palsy, myasthenia (varies with fatigue), trauma. Sag from 7th nerve palsy can mask ptosis. 7th nerve palsy can imitate a contralateral ptosis because it widens the ipsilateral palpebral fissure.
b. Bilateral ptosis: Nuclear third lesion, myasthenia, progressive external ophthalmoplegia, age-related periorbital atrophy, redundant lid tissue, oculopharyngeal dystrophy, bilateral third palsy.
2. Blink rate: Decreased in extrapyramidal bradykinetic syndromes. These pts often cannot suppress blinks to repeated forehead tap (Myerson's sign) and may have blepharoclonus (lid fluttering) with eyes closed.
3. Lid retraction: Consider dorsal midbrain syndrome; hyperthyroidism (often with lid lag as pt looks down), chronic steroids.
F. Exophthalmos
(AKA proptosis)
1. DDx: Carotid cavernous fistula (usually pulsatile), tumor, hyperthyroidism, infection, inflammation, hemorrhage, 3rd nerve palsy (via rectus relaxation), carotid sinus occlusion.
P.52
G. Horner's syndrome
1. H&P:
a. Ptosis: An ID photo can show if it is old.
b. Miosis (small pupil): Worse in dark because the abnormal pupil fails to dilate (vs. 3rd nerve lesion, which is worse in light). There should be a dilation lag when lights are turned off.
c. Anhidrosis: Seen if lesion is in nerve before the sweat afferents leave with ext. carotid artery. Wipe on iodine bilaterally and let it dry; then put starch from a glove on top. Sweat will turn it purple.
2. Tests for localization:
a. Cocaine test confirms Horner's: dilates normal pupil only. Blocks reuptake, so no effect unless norepinephrine being released at pupil.
b. Apraclonidine is a readily available alternative to cocaine. It dilates Horner's pupil only. It is a weak 1-agonist.
c. Hydroxyamphetamine test dilates Horner's pupils only if 3rd-order neurons are intact because it is an indirect agonist that releases norepinephrine from the intact terminal.
3. Causes of isolated Horner's syndrome:
a. 3rd-order lesion: Usually idiopathic (if congenital, iris is often heterochromic) but r/o carotid dissection (no anhidrosis if internal carotid).
b. 1st- and 2nd-order: Tumor (including Pancoast) > cluster HA > vascular (dissection, cavernous thrombosis, ischemia) > cervical disk > trauma (including thoracic surgery) > meningitis > PTX > intrinsic brainstem lesion (usually with other findings).
EAN: 2147483647
Pages: 109