| Note: Large images and tables on this page may necessitate printing in landscape mode.
Copyright 2007 The McGraw-Hill Companies. All rights reserved.
Current Otolaryngology > VIII. Larynx & Hypopharynx > Chapter 30. Malignant Laryngeal Lesions >
| General Considerations Each year, 11,000 new cases of larynx cancer will be diagnosed in the United States (1% of new cancer diagnoses), and approximately one third of these patients will die of their disease. The current male-to- female ratio for larynx cancer is 4:1, but the relative percentage of women with this, as with other smoking- related illness , has been on the rise. Larynx cancer is most prevalent in the sixth and seventh decades of life and is more prevalent among lower socioeconomic groups, for whom it is often not diagnosed until more advanced stages. More than 90% of larynx cancer is squamous cell carcinoma (SCC) and is directly linked to tobacco and excessive alcohol use. Because of the complex and multifaceted nature of this disease, treatment planning is best delivered through a multidisciplinary tumor board format. | | Anatomy The larynx functions not only to produce voice, but also to divide and protect the respiratory from the digestive tracts. It acts as a sphincter during deglutition, protecting against the penetration of bypassing food by closing off the trachea at two sites: the epiglottic flap and the closure of the vocal cords. The larynx consists of a framework of cartilages connected by ligaments, membranes, and muscles covered by a respiratory and stratified squamous mucosal epithelium (Figure 301).
The larynx can be divided into three parts : the supraglottis, the glottis, and the subglottis (Figure 302). The supraglottic larynx extends from the tip of the epiglottis and vallecula superiorly to the ventricle and undersurface of the "false" cords inferiorly; it includes the arytenoid cartilages, the aryepiglottic folds , the false vocal cords, and the epiglottis. The glottic larynx encompasses the "true" vocal cords, extending from the ventricle between the true and false cords to 0.5 cm below the free edge of the true cords, including the anterior commissure and interarytenoid area. The subglottic larynx extends from the inferior extent of the glottis to the inferior edge of the cricoid cartilage.
Understanding the embryologic origin of these regions of the larynx helps to explain the difference in clinical behavior between cancers arising from these laryngeal subsites. The supraglottis derives from the midline buccopharyngeal primordium and branchial arches 3 and 4 with rich bilateral lymphatics. The glottis, on the other hand, forms from the midline fusion of lateral structures derived from the tracheobronchial primordium and arches 4, 5, and 6. There is a paucity of lymphatics and, compared with supraglottic primary neoplasms, malignant glottic tumors have less of a tendency for bilateral regional lymphatic spread and remain confined to the glottis for longer periods of time. Fibroelastic membranes and ligaments further divide the larynx into the pre-epiglottic and paraglottic spaces. These structures, including the conus elasticus, the quadrangular and thyrohyoid membranes, and the hyoepiglottic ligament, act as barriers to spread of tumor (Figure 303). The thyroid and cricoid cartilages and their perichondrium are further barriers to tumor spread. The anterior commissure tendon (Broyle's ligament) and thyroepiglottic ligaments are not effective barriers to tumor spread, and tumors involving the anterior commissure are more likely to have direct regional spread. The muscles of the larynx are divided into intrinsic and extrinsic groups. The intrinsic muscles are those of the vocal cords and cartilages contained within the larynx itself. The extrinsic muscles, the strap muscles and constrictors, help with laryngeal elevation and pharyngeal constriction. Innervation of the intrinsic muscles is from the recurrent laryngeal branches of the vagus nerve on both sides. Arterial blood supply is from the external carotid artery and off the thyrocervical trunk via the superior and inferior thyroid arteries. Venous drainage is into the internal jugular vein. Lymphatic drainage is to levels II, III, and IV, as well as sometimes to level VI of the neck. Kirchner JA. One hundred laryngeal cancers studied by serial section. Ann Otol. 1969;78:689. (Classic paper studying anatomic and histologic cross section of larynx cancers.) [PMID: 5799397]
| | | Pathogenesis More than 90% of patients with larynx cancer have a history of heavy tobacco and alcohol use. Cigarette smoke, in particular, is a risk factor for cancer of the larynx. The combination of smoking and alcohol use has a more than additive carcinogenic effect on the larynx. Other risk factors have been identified. Laryngeal infection with the human papillomavirus (HPV) results in laryngeal papillomatosis, which is usually benign , but subtypes 16 and 18 are known to degenerate into SCC. Gastroesophageal reflux has been implicated; however, a causal relationship with laryngeal cancer is still uncertain , although therapies directed at suppressing acid appear to decrease the recurrence of laryngeal cancer. Various occupational exposures and toxic inhalations (such as asbestos and mustard gas), nutritional deficiencies, and previous neck irradiation have all been linked to larynx cancer as well. Increasingly, molecular and genetic markers of malignant potential, degeneration, and metastasis are being identified, unlocking the genetic causes of larynx cancer. Attention is being paid to predictors of clinical outcome and the response to specific therapy . Once these pathways are understood , gene therapy and other novel therapeutic approaches can be developed. Genes and gene products being investigated for their link to larynx cancer include p53, the Bcl-2 family of genes and other markers of apoptosis, proliferating cell nuclear antigen (PCNA), Ki67, cyclin D1, the ras gene and other oncogenes, tumor suppressor genes, and the loss of heterozygosity and changes in the DNA content of tumors. Bradford CR. Predictive factors in head and neck cancer. Hematol Oncol Clin North Am. 1999;13(4):777. (Review of molecular and genetic predictive factors for head and neck cancer, with a focus on selecting patients for specific or adjuvant therapies.) [PMID: 10494513]
| Bradford CR, Wolf GT, Carey TE et al. Predictive markers for response to chemotherapy, organ preservation, and survival in patients with advanced laryngeal carcinoma. Otolaryngol Head Neck Surg. 1999;121(5):534. (The overexpression of p53 and elevated PCNA as well as the T-stage predicted successful organ preservation in the VA Larynx Trial.) [PMID: 10547465]
| Kreimer AR, et al. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: a systemic review. Cancer Epidemiol Biomarkers Prev. 2005;14(2):467. (Review of the relationship between the different subtypes of human papillomavirus and head and neck cancers.) [PMID: 15734974]
| Qadeer MA, Colablanchi N, Strome M et al. Gastroesophageal reflux and laryngeal cancer: causation or association? A critical review. Am J Otolaryngol. 2006;27(2):119. (A look at the literature on the relationship between gastroesophageal reflux disease and laryngeal cancer.) [PMID: 16500476]
| Qadeer MA, Lopez R, Wood BG et al. Does acid suppressive therapy reduce the risk of laryngeal cancer recurrence? Laryngoscope. 2005;115(10):1877. (Study to determine the effects of gastroesophageal reflux disease and acid-suppressive therapy on recurrence of laryngeal cancers after larynx- preserving therapies.) [PMID: 16222214]
| Staton J et al. Factors predictive of poor functional outcome after chemoradiation for advanced laryngeal cancer. Otolaryngol Head Neck Surg. 2002;127(1):43. (Study to determine the pre-treatment parameters that predict poor outcomes related to laryngeal function in patients who survived larynx-preservation therapies for advanced laryngeal cancers.) [PMID: 12161729]
| Syrjanen S. Human papillomavirus (HPV) in head and neck cancer. J Clin Virol. 2005;32(Suppl 1):S59. (Review of the data on relationship of human papillomavirus to head and neck cancers.) [PMID: 15753013]
| Torrente MC et al. Molecular detection and typing of human papillomavirus in laryngeal carcinoma specimens. Acta Otolaryngol. 2005;125(8):888. (Evidence for human papillomavirus infection as an etiologic factor in some laryngeal carcinomas.) [PMID: 16158538]
| | | Epidemiology Malignant disorders of the glottic larynx outnumber those of the supraglottis 1.5:1.0 in the United States (Table 301). This ratio does not hold worldwide. In Finland, for example, supraglottic cancers outnumber glottic cancers. The worldwide variation in the epidemiology of larynx cancer may reflect local tobacco and alcohol use customs , other environmental factors, or also the genetic makeup of the populations affected. | Table 301. Incidence of Larynx Cancer by Site.
| | | Supraglottic 40% | | Glottic 59% | | Subglottic 1% | |
| Malignant disorders arising in the subglottis are universally rare. For this reason, data on the incidence of nodal metastases and prognosis are scant, and the discussion of the diagnosis and management of larynx cancers that follows focuses on primary supraglottic and glottic cancers. Most larynx cancers involving the subglottis are extensions of primary cancers arising in the glottis or supralglottis. As explained above, cancers arising in the supraglottic larynx have a richer lymphatic drainage and are more often diagnosed with nodal metastases and, therefore, at a higher clinical stage (Table 302). | Table 302. Larynx Cancer: Incidence of Neck Metastases by Site.
| | | | T1 | T2 | T3 | T4 | All T | | Supraglottis | 1540% | 3542% | 5065% | > 65% | 2550% | | Glottis | < 5% | 510% | 1020% | 2540% | | | Subglottis | | | | | 50% | |
| Jemal A, Thomas A, Murray T et al. Cancer statistics, 2002. CA Cancer J Clin. 2002;52(1):23. (American Cancer Society statistics.) [PMID: 11814064]
| | | Prevention Many studies address the protective effect of retinoids, beta-carotene, and other antioxidants against the development of larynx cancer. A reversal of laryngeal leukoplakia after treatment with retinyl-palmitate has been demonstrated. Issing WJ, Struck R, Naumann A. Impact of retinyl palmitate in leukoplakia of the larynx. Eur Arch Otorhinolaryngol. 1997; 254;S105. (Study showing the reversal of laryngeal leukoplakia with this antioxidant therapy.) [PMID: 9065641]
| | | Staging Cancers of the larynx are staged according to the TNM (tumor, node, metastasis) system of the American Joint Committee on Cancer (Table 303). For staging purposes, positive neck nodes are considered locoregional metastases; metastases to other parts of the body (such as lung, mediastinum , liver, and bone) are considered distant. For the first time, T4 tumors are divided into resectable (T4a) and unresectable (T4b) tumors; accordingly , Stage IV tumors are now subdivided into IVA, IVB, and IVC ( distant metastases present) staging. Studies before this date, however, are based on the 1998 or earlier systems in which there was a single umbrella T4 and Stage IV designation. Accordingly, the discussion in the rest of this chapter refers to the older system. | Table 303. American Joint Committee on Cancer 2002, T (Tumor), N (Nodes), M (Metastases), Staging for Malignant Laryngeal Disorders.
| | | Supraglottis | T 1
| Tumor limited to one subsite of supraglottis | T 2
| Tumor involving more than one adjacent subsite of supraglottis, glottis, or region outside the supraglottis (vallecula, tongue base, medial wall of pyriform sinus) | T 3
| Tumor causes vocal cord fixation and/or invades pre-epiglottic space, postcricoid area | T 4a
| Tumor invades through thyroid cartilage, and/or extends to nonlaryngeal soft tissues of neck | T 4b
| Tumor invades prevertebral space or mediastinum, or encases carotid artery | | Glottis | T 1
| Tumor limited to vocal cord; may involve anterior or posterior commissure | T 2
| Tumor extends to supraglottis, glottis, and/or impaired vocal cord mobility | | T 3 | Vocal cord fixation | T 4a
| Tumor invades through thyroid cartilage, and/or extends to nonlaryngeal soft tissues of neck | T 4b
| Tumor invades prevertebral space or mediastinum, or encases carotid artery | | Subglottis | T 1
| Tumor limited to the subglottis | T 2
| Tumor extends to vocal cord with normal or impaired mobility | | T 3 | Vocal cord fixation | T 4a
| Tumor invades through cricoid or thyroid cartilage, and/or extends to nonlaryngeal soft tissues of neck | T 4b
| Tumor invades prevertebral space or mediastinum, or encases carotid artery | N
| No cervical lymph nodes positive | N 1
| Single ipsilateral lymph node  3 cm 3 cm | | N 2a | Single ipsilateral lymph node > 3 cm and 6 cm | N 2b
| Multiple ipsilateral lymph nodes, each 6 cm | N 2c
| Bilateral or contralateral lymph nodes, each 6 cm | N 3
| Single or multiple lymph nodes > 6 cm | M
| No distant metastases | M 1
| Distant metastases present | | Stage | T | N | M | | I | T 1
| N
| M
| | II | T 2
| N
| M
| | III | T 3
| N
| M
| | | T 13
| N 1
| M
| | IVA | T 4a
| N 02
| M
| | | T 14a
| N
| M
| | IVB | T 4b
| any N | M
| | | any T | N 3
| M
| | IVC | any T | any N | M 1
| |
Modified, with permission, from Greene FL, Page DL, Fleming ID et al (eds.): American Joint Committee on Cancer: AJCC Cancer Staging Manual, 6th ed. New York, Berlin, Heidelberg: Springer-Verlag, 2002. | A shortcoming of the TNM staging system, which the subdivision of the T4 and Stage IV categories is starting to address, is that tumors of varying size and prognosis are frequently categorized together. Other indicators of the prognosis in laryngeal carcinoma have been identified and proposals exist to incorporate these into staging systems. These indicators include (1) the histologic characteristics of the tumor, such as extracapsular spread in nodal metastases, angiolymphatic invasion, perineural spread, and a high histologic grade; (2) various chromosomal and molecular markers, such as p53 mutations , Ki67 or PCNA overexpression, DNA content, and loss of heterozygosity; and (3) the presence of patient comorbidities. Greene FL, Page DL, Fleming ID et al (eds.). American Joint Committee on Cancer: AJCC Cancer Staging Manual, 6th ed. New York, Berlin, Heidelberg: Springer Verlag, 2002. (The definitive reference for the currently used American Joint Committee on Cancer staging system.)
| Piccirillo JF. Importance of comorbidity in head and neck cancer. Laryngoscope. 2000;110(4):593. ( Prospective study, including 341 head and neck cancer patients, demonstrating the prognostic value of comorbidity and providing data in support of incorporating comorbidity into accepted staging systems.) [PMID: 10764003]
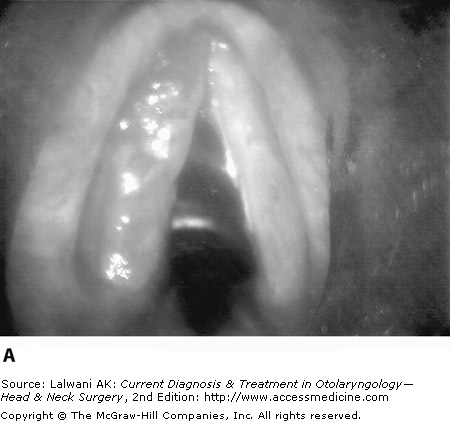
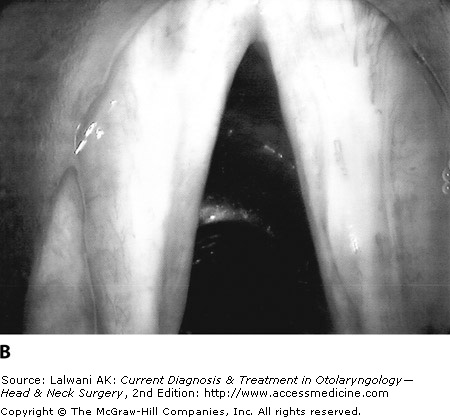
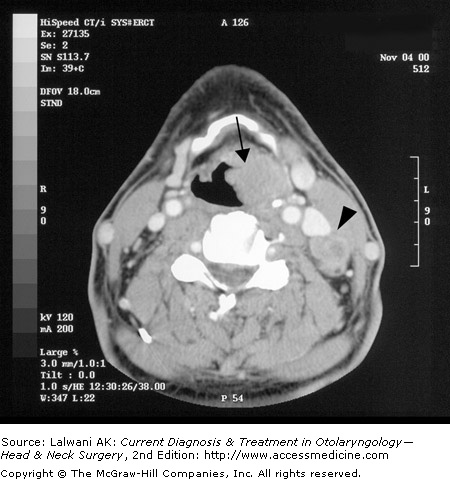
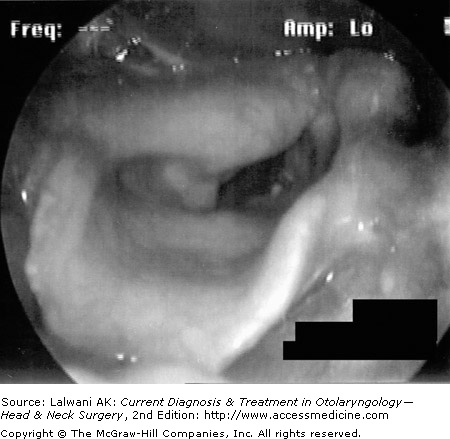
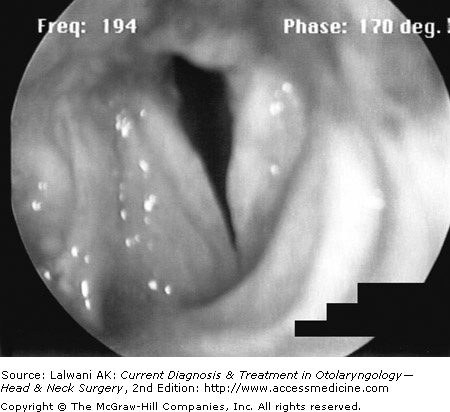
| | | Clinical Findings Symptoms and Signs Signs and symptoms of malignant laryngeal lesions include hoarseness, dysphagia, hemoptysis, a mass in the neck, throat pain, ear pain, airway compromise, and aspiration. Because only the slightest change in contour, thickness , or vibratory characteristics of the vocal cord results in perceived changes in the voice (namely, hoarseness), glottic larynx cancers often come to medical attention while still at an early stage. Patients with supraglottic cancers, however, typically present at a more advanced stage because tumors are bulkier (ie, at a higher T stage) before voice changes, dysphagia, airway compromise, or aspiration become apparent. Furthermore, because the supraglottis has a richer lymphatic supply, supraglottic primary lesions tend to metastasize earlier and are more often diagnosed at the advanced N stage. Clinical cervical adenopathy at the time of diagnosis portends a poor prognosis and advances the overall stage. Significant weight loss often accompanies the diagnosis of an advanced larynx cancer because of swallowing difficulties. Of note, throat and ear pain are usually symptoms of advanced-stage tumors. Physical Examination When a larynx cancer is suspected, complete head and neck examination is performed, focusing on the larynx and the neck. The quality of the voice is noted. A breathy voice may indicate a vocal cord paralysis and a muffled voice, a supraglottic lesion. Laryngoscopy Laryngoscopy (or visualization of the larynx) is done in the office setting using either a laryngeal mirror (indirect laryngoscopy) or a fiberoptic endoscope. Irregularities in the contour, color, vibratory characteristics, and mobility of the vocal cords are noted. Malignant laryngeal lesions can appear to be fungating, friable, nodular, or ulcerative, or simply as changes in mucosal color (Figure 304). A stroboscopic video laryngoscopy can highlight subtle irregularities in the mucosal vibration , periodicity, and closure of the vocal cords. Careful attention must be paid to the airway status. Some large, bulky lesions require urgent airway intervention with either intubation, tumor debulking, or tracheotomy. Direct laryngoscopy is performed under general anesthesia and provides the definitive examination of tumor extent. Neck Examination The neck is examined by palpation for enlarged lymph nodes and by noting their location, size, firmness, and mobility. Restricted laryngeal crepitus (the "clicking" movement from side to side across the pharynx and prevertebral fascia) can reveal postcricoid or even retropharyngeal invasion. Assessment of Nutritional Status Nutritional status should also be assessed and supplementation discussed, if indicated. Caloric dietary supplements may suffice in some cases; others may require gastrostomy or other feeding tube placement. Laboratory Findings and Special Tests Squamous cell carcinoma of the head and neck can spread to virtually any site of the body, but it is rare in the absence of lung, mediastinal, or liver metastases. Therefore, routine metastatic survey consists of the following tests. Biopsy Biopsy of a laryngeal lesion is necessary to establish the diagnosis of malignancy. Biopsy of the larynx is best accomplished in the operating room with the patient under general anesthesia and neuromuscular paralysis. Direct laryngoscopy is performed. A variety of laryngoscopes are available designed to enhance visualization of the endolarynx in a range of anatomic and clinical situations. The suspected lesion is mapped and possibly photographed/videotaped. The lesion can be palpated to assess the depth of invasion, and passive mobility of both vocal cords can be checked. Biopsies of suspected malignant sites are done with cup forceps. With the patient anesthetized and paralyzed, a thorough neck examination is obtained. Esophagoscopy and bronchoscopy can also be performed at this setting as part of a cancer staging workup. For patients who cannot tolerate a general anesthetic, the biopsy of laryngeal lesions can be performed as an office procedure. Under fiberoptic guidance, with generous topical anesthesia (typically using lidocaine or Cetacaine), a flexible biopsy forceps passed through the fiberoptic scope is used. Chest Imaging Cancer of the larynx spreads first to the regional cervical nodes. The next most common site of spread is the lungs. For this reason, patients with head and neck cancer should have a chest x-ray as part of a routine metastatic evaluation. This test should be repeated once or twice yearly to screen for metastases. If there are any significant abnormalities noted on the chest x-ray, a computed tomography (CT) scan of the chest should be performed to confirm the lesions. Bronchoscopy with cytologic evaluation of bronchial washings or transbronchial biopsy should be done if there are suspicious lesions. Alternately, thoracoscopy, mediastinoscopy, and biopsy are done if lesions are more amenable to these approaches. Chest and lung lesions may represent either metastases from the larynx primary neoplasm or second primary tumors, because the risk factor of smoking is common to both tumors. Imaging Studies Radiologic imaging of the larynx and neck is not necessary for an early-stage glottic cancer with a clinically N0 neck. Because the risk of occult nodal disease is high even for early-stage supraglottic cancer, it is sometimes recommended to obtain neck imaging in these cases. If there is any suspicion of impaired vocal cord mobility, a scan should be obtained. Radiologic imaging is generally performed for clinically advanced larynx cancers to aid with staging and treatment planning. CT scanning (Figure 305) or magnetic resonance imaging (MRI) is useful in identifying pre-epiglottic or paraglottic space invasion, laryngeal cartilage erosion , and cervical nodal metastases. Larynx cancers are clinically upstaged as frequently as 2540% on the basis of CT scanning or MRI. Both imaging modalities are useful to assess the above characteristics. MRI is more sensitive for soft tissue abnormalities, whereas CT scan is better for bony and cartilaginous defects. Other imaging modalities are being investigated for their role in larynx cancer, but at this time they are not the standard of care. Positron emission tomography (PET) scanning uses fluorescence-tagged glucose and the increased metabolic rate of malignant tissues to identify cancers. Application of PET in the head and neck has focused on (1) identifying occult nodal metastases, (2) distinguishing the recurrence of malignant growth from radionecrosis and other sequelae of prior treatment, and (3) identifying the location of an unknown primary cancer. Some evidence suggests that PET scan may be able to detect superficial laryngeal cancers that CT scan cannot. Nonetheless, PET scan information does not replace the accuracy of direct visualization and biopsy of the larynx and is not superior to CT or MRI in identifying the additional staging criteria of pre-epiglottic or paraglottic space invasion, cartilage erosion, soft tissue extension into the neck, and cervical metastasis. If there is a question of distant metastases, then bone scanning may be of use. Ultrasound of the neck can be useful in the diagnosis of larynx cancer. In Europe, this noninvasive imaging modality is used to identify cervical metastases and even to characterize laryngeal abnormalities, but it is not typically used in North America for these purposes. Anzai Y, Carroll WR, Qunit DJ et al. Recurrence of head and neck cancer after surgery or irradiation: prospective comparison of 2-deoxy-2-[F-18]fluoro-D-glucose PET and MR imaging diagnoses. Radiology. 1996;200(1):135. (Study of patients with recurrent head and neck cancer, demonstrating the improved sensitivity and specificity of PET over MRI and CT scans in detecting the recurrence.) [PMID: 8657901]
| Gordin A et al. Fluorodeoxyglucose-positron emission tomography/ computed tomography imaging in patients with carcinoma of larynx: diagnostic accuracy and impact on clinical management. Laryngoscope . 2006;116(2):273. (Study to assess the value of PET/CT on patients with laryngeal cancer compared with PET or CT alone and the impact that PET/CT had on clinical management.) [PMID: 1646778]
| McGuirt WF, Greven KM, Keyes JW et al. Laryngeal radionecrosis versus recurrent cancer: a clinical approach. Ann Otol Rhinol Laryngol. 1998;107:293. (Study showing the usefulness of the PET scan to distinguish recurrent laryngeal cancer from laryngeal radionecrosis.) [PMID: 9557763]
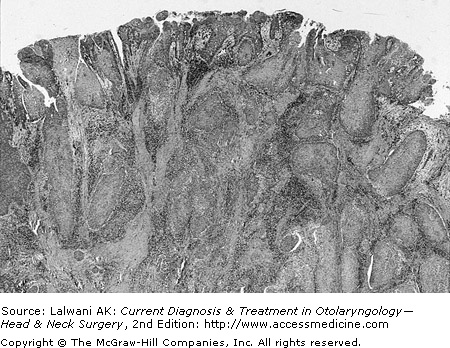
| | | Differential Diagnosis Definitive tissue diagnosis must be obtained before starting treatment for a laryngeal cancer because lesions that appear malignant may, in fact, be benign. These benign conditions include infectious, inflammatory, and granulomatous diseases such as tuberculosis, sarcoidosis, blastomycosis, papillomatosis, and granular cell tumors. The next section provides a discussion of malignant laryngeal lesions. | | Histologic Types Squamous Cell Carcinoma SCC represents > 90% of larynx cancers and is linked to tobacco and excessive alcohol use. Histologically, the carcinogenesis of SCC is viewed as a continuum of change from normal phenotype, to hyperplasia, to dysplasia, to carcinoma in situ, to invasive carcinoma. Invasive SCC can be well, moderately, or poorly differentiated and is characterized by nests of malignant epithelial cells in a surrounding desmoplastic, inflammatory stroma (Figure 306). Varying degrees of mitoses and necrosis are seen. Keratin pearls are a pathognomonic feature seen in well- and moderately differentiated SCC. SCC can invade blood and lymphatic vessels as well as nerves. Immunohistochemical staining is positive for keratin proteins . Variants of SCC include verrucous carcinoma, spindle cell carcinoma, basaloid SCC, and adenosquamous carcinoma. Verrucous carcinoma, which is characterized grossly by a warty, exophytic tumor that is highly differentiated with bulbous "rete pegs" pushing into the underlying stroma and low metastatic potential, is typically treated surgically because many physicians view this tumor as being radiation-resistant. Spindle cell carcinoma presents as malignant spindle cells seen in the stroma usually predominating over foci of conventional SCC and is often confused with sarcoma. The spindle cells typically stain positive for keratin on immunohistochemistry. Basaloid SCC presents as compact nests of subepithelial basaloid cells associated with SCC in situ or invasive SCC. Adenosquamous carcinoma is a high-grade malignant neoplasm with features of both SCC with epithelial differentiation and adenocarcinoma with glandular differentiation. Salivary Gland Cancers Malignant disorders can arise from the minor salivary glands that line the mucosa of the larynx. Adenoid cystic carcinoma (ACC) and mucoepidermoid carcinoma (MEC) are the most common, although other histologic types have been reported as well. Women and men are affected equally by ACC of the larynx. The histology resembles that of the major salivary gland counterparts, with cribriform, tubular, and solid architectural patterns for ACC and low-grade cystic patterns to high-grade solid patterns for MEC. The clinical behavior is also similar to that of the corresponding major salivary gland neoplasms. ACC has an indolent clinical course and tendency for perineural spread. Low-grade MEC has a better prognosis than high-grade MEC. Surgery is the preferred treatment for both, with guidelines for adjuvant radiation similar to those for malignant disorders of the major salivary glands. Sarcomas Malignant growths of mesenchymal origin are rarely seen in the larynx. The most common is chondrosarcoma. Chondrosarcoma of the larynx arises most often from the cricoid cartilage and is characterized by a submucosal mass of the posterior glottis with stippled calcification on CT scan (Figure 307). The diagnosis can be difficult both because an adequate biopsy may be challenging and because the histologic differentiation from a benign chondroma may be difficult. Chondrosarcomas have a nonaggressive clinical behavior, and, for this reason, partial laryngeal surgery with preservation of some laryngeal function is often attempted. Radiation is generally viewed as ineffective in treating laryngeal chondrosarcoma. Other types of laryngeal sarcoma include malignant fibrous histiocytoma, angiosarcoma, and synovial sarcoma. Other Neoplasms Other tumors that can occur in the larynx include neuroendocrine tumors such as carcinoid tumors, lymphoma, and metastases from other primary sites. Malignant tumors of the thyroid can invade into the larynx with or without vocal cord paralysis. Gripp S, Pape H, Schmitt G. Chondrosarcoma of the larynx: the role of radiotherapy revisiteda case report and review of the literature. Cancer. 1998;82:108. (Review of the literature and existing case reports on larynx chondrosarcoma, revisiting the idea of radiation as a treatment for this type of cancer.) [PMID: 9428486]
| | | Treatment Treatment of Early-Stage Larynx Cancer Early-stage larynx cancer (Stages I and II) can be treated with either surgery or radiation in single-modality therapy. Current recommendations by the American Society of Clinical Oncology are that all patients with T1 or T2 laryngeal cancer, with rare exceptions, should be treated initially with the intent to preserve the larynx. The advantages of surgery compared with radiation are a shorter treatment period (compared with 67 weeks for radiation) and the option of saving radiation for recurrence. Specific surgical procedures used in the treatment of early larynx cancer are discussed in the following section. In addition to the risks inherent in any surgical procedure, surgery often results in a poorer voice quality and, for external surgical approaches, a worse cosmetic outcome. The chief advantage of radiation therapy is better voice quality. Specific radiation therapy techniques for larynx cancer are discussed under "Nonsurgical Measures." For early-stage lesions, short-term complications of radiation include odynophagia and laryngeal edema. The long- term complications include a remote possibility of laryngeal fibrosis, radionecrosis, or hypothyroidism . Delayed development of sarcoma (radiation-induced), though possible, is exceedingly rare, with an incidence of 0.030.3%. Treatment of Advanced-Stage Larynx Cancer Advanced-stage larynx cancer (Stages III and IV) was historically treated by dual-modality therapy with surgery and radiation. For most T3 and T4 tumors, where total laryngectomy is required for the complete removal of the tumor with amply clear margins, organ preservation treatment with combined chemotherapy and radiation therapy is preferred in most centers because there is no difference in overall survival and a superior quality of life. Still, extirpative surgery may be used in selected patients, such as those with bone or cartilage destruction in which reasonable organ function is unlikely after conservation therapy. Voice rehabilitation after total laryngectomy is discussed below. For T1, T2, and some T3 lesions, partial laryngectomy procedures with preservation of the voice may be considered (see "Surgical Treatment of Larynx Cancer"). Patient selection is critical with the goal of rendering the patient disease free with surgery alone because postoperative radiation after partial laryngectomy may result in significant functional impairment . The type of neck dissection chosen is guided by the extent of the neck disease, also discussed below. Adjuvant radiation should start within 6 weeks of surgery and, on once-daily protocols, lasts 67 weeks. The primary site is treated with external-beam irradiation with doses of 5566 Gy whereas draining nodal basins typically receive a slightly lower dose, depending on the extent of neck disease. Complications of radiation therapy include those described for radiation given as single-modality treatment for early-stage larynx cancer; however, since the treated area is more extensive , side effects also include mucositis during therapy and chronic xerostomia after treatment. Less common complications include hypothyroidism, radionecrosis, and esophageal stricture. Organ-preserving protocols have evolved over the past decade . The landmark work study of the Veterans Administration Larynx Cancer Study Group randomized 332 patients to receive neoadjuvant chemotherapy followed by radiation, compared with traditional total laryngectomy with postoperative radiation. The study found that two thirds of patients responded favorably to chemotherapy after just one or two cycles. In two thirds of these cases, larynges were preserved, and survival was similar to the traditional approach of laryngectomy with postoperative radiation. As a subgroup , patients with larger T4 tumors did not fare as well and, for this reason, organ-preserving protocols sometimes are not offered to patients in this category, particularly if cartilaginous invasion is present. The VA study was followed by a three-arm randomized study comparing induction chemotherapy (cisplatin plus 5-fluorouracil) followed by radiation, concurrent chemoradiation with cisplatin, and once-daily radiation alone in 547 patients. At 2 years , superior organ preservation was achieved with the concurrent chemoradiation group; therefore, this treatment strategy has become the standard of care in most centers. Ongoing studies of combined-modality treatment include radiation with different systemic therapies and systemic therapy with altered radiation schedules, including twice-daily treatment. Treatment of the Neck in Larynx Cancer A neck without clinically apparent nodal metastases should be treated in larynx cancer if the risk of nodal metastasis exceeds 2030% (see Table 302). The treatment of both the ipsilateral and contralateral necks should be considered, therefore, for early-stage, primary cancers of the supraglottis in general and for all advanced laryngeal cancers. Neck disease staged as N0 or N1 can be treated with a single modalitysurgery or radiation. Neck disease staged as N2 or N3 requires a combined-modality treatment. Neck dissection is tailored to the extent of neck disease. Selective neck dissection (preserving the sternocleidomastoid muscle, internal jugular vein, and spinal accessory nerve) can be performed for clinically N0 necks. For N1 necks, dissection is usually limited to levels IIIV, as metastasis to levels I or V is rare in this condition. Radical or extended radical neck dissection, sacrificing the sternocleidomastoid muscle, the internal jugular vein, and the spinal accessory nerve, and addressing neck levels IV or more, is performed for extensive neck disease with the involvement of vessels, nerves, muscles, or any combination of these structures. A modified radical neck dissection preserves some of these structures, according to feasibility. Surgical Treatment of Larynx Cancer Surgical options for treating larynx cancer include a variety of partial laryngectomy procedures in addition to total laryngectomy. Understanding the lymphatic drainage patterns of the laryngeal subsites permits the surgeon to resect more closely than the 1- to 2-cm margins that typically are recommended at other head and neck sites. This helps preserve functional voice, respiration, and deglutition in partial laryngectomy procedures. A preoperative consultation with a speech therapist is appropriate if significant voice or swallowing changes are anticipated. These sessions help educate patients about the speech and swallowing functions of the larynx and prepare the patient for postoperative rehabilitation and therapy. Microlaryngeal Surgery The endoscopic removal of selected larynx cancers can be achieved safely and effectively with use of the operating microscope and microlaryngeal dissection instruments. The carbon dioxide laser, used with direct laryngoscopy and microscope guidance, is also a useful dissection tool, especially for supraglottic lesions. Laser cordectomy has been shown to provide excellent local control and laryngeal preservation of early-stage glottic cancer; it offers low morbidity and excellent retreatment options in case of local failure. Hemilaryngectomy Hemilaryngectomy is the removal of one vertical half of the larynx (or a part thereof; Figure 308). Appropriate tumors for this surgery are those with (1) subglottic extension no more than 1 cm below the true vocal cords; (2) a mobile affected cord; (3) unilateral involvement (involvement of the anterior commissure and anterior extent of the contralateral true cord can, in certain cases, also be treated with an extended vertical hemilaryngectomy); (4) no cartilage invasion; and (5) no extralaryngeal soft tissue involvement.
Vocal cord reconstruction is most often done by transposing a flap of strap muscle or microvascular free flap to provide bulk against which the remaining unaffected vocal cord can vibrate (Figure 309). Vertical hemilaryngectomy can be done in appropriate surgical candidates who have failed radiation therapy. Supraglottic Laryngectomy A supraglottic laryngectomy entails removal of the supraglottis or the upper part of the larynx (or a part thereof). This surgery may be considered when the following conditions are met: (1) for tumors with a T stage of T1, T2, or T3 by pre-epiglottic space involvement only; (2) the vocal cords are mobile; (3) cartilage is not involved; (4) the anterior commissure is not involved; (5) the patient has good pulmonary status/reserve; (6) the base of the tongue is not involved past the circumvallate papillae; (7) the apex of the pyriform sinus is not involved; and (8) the FEV 1 (the forced expiratory volume in the first second) is predicted to be > 50%. A supraglottic laryngectomy can be performed endoscopically using a carbon dioxide laser or with a more standard open , external approach. Endoscopic surgery typically removes just the involved portion of the supraglottis. The traditional supraglottic laryngectomy removes the entire supraglottis from the apex of the laryngeal ventricle, including the false cords, the epiglottis, and the pre-epiglottic space; the arytenoids and part of the thyroid cartilage are preserved (Figure 3010). Closure in an open supraglottic laryngectomy is done by collapsing the remaining glottic part of the larynx to the base of tongue (Figure 3011).
Although the patient's voice is generally normal in quality, some degree of aspiration is an expected side effect of this operation. For this reason, patients with borderline pulmonary function (FEV 1 predicted to be < 50%) who cannot tolerate chronic aspiration are generally not considered good candidates for supraglottic laryngectomy. Patients must learn a double-swallow technique called the supraglottic swallow to minimize aspiration with oral intake. Regular visits with a speech therapist are critical to properly learn this technique. Supracricoid Laryngectomy This is a newer surgical technique, which expands on the traditional supraglottic laryngectomy procedure to preserve voice for those with cancers located at the anterior gloltti s, including the commissure, or those with more extensive pre-epiglottic space involvement. The true vocal cords, the supraglottis, and thyroid cartilage are taken, preserving the cricoid and arytenoid cartilages (Figure 3012). Half of the patients remain dependent on their tracheotomy. Pulmonary function and prior radiation candidacy criteria for supraglottic laryngectomy apply for supracricoid laryngectomy as well. Voice results are reported as adequate. Supraglottic swallow techniques must be used. Near-Total Laryngectomy A near-total laryngectomy is a more extended partial laryngectomy procedure in which only one arytenoid is preserved and a tracheoesophageal conduit is constructed for speech (Figure 3013). Voice is generated by the lungs, but has a more limited range of pitch. Oral intake and swallowing are in the usual fashion, with some aspiration concerns. Patients remain dependent on a tracheotomy for breathing . This procedure is not offered to patients whose radiation treatments have failed, those with poor pulmonary reserve, or those with tumor invovement below the cricoid ring. Candidates are patients with large T3 and T4 lesions with one uninvolved arytenoid, or with unilateral transglottic tumors with cord fixation. Total Laryngectomy A total laryngectomy entails the removal of the entire larynx, including the thyroid and cricoid cartilages, possibly some upper tracheal rings, and the hyoid bone (Figure 3014). The proximal tracheal stump is anastomosed to an opening at the root of the neck anteriorly in a permanent tracheostoma; this results in the complete anatomic separation of the respiratory and digestive tracts. Indications for total laryngectomy are (1) T3 and T4 cancers not amenable to the above partial laryngectomy procedures or organ preservation therapy with chemoradiation, (2) extensive involvement of thyroid or cricoid cartilage, (3) the direct invasion of surrounding soft tissues of the neck, and (4) tongue base involvement beyond the circumvallate papillae. Closure is done by reapproximating the pharyngeal mucosa. If a partial or total pharyngectomy is also required because of the size of the tumor, then free flap or regional flap aids the closure and prevents pharyngoesophageal stricture. The goal is for patients to ingest nutrients by mouth and swallow in the usual manner.
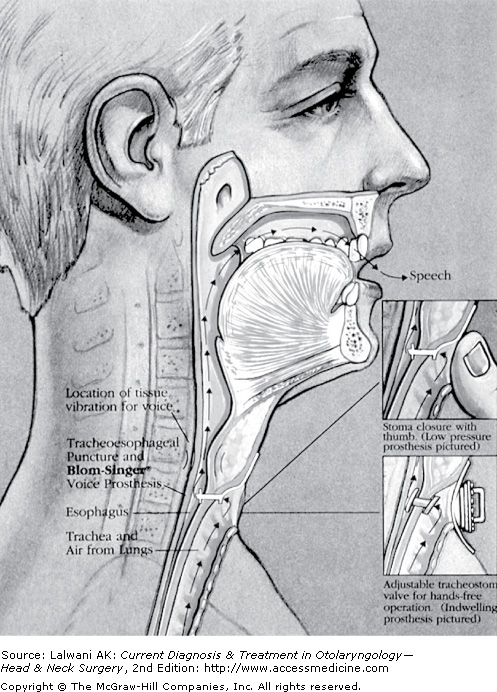
Voice rehabilitation after a total laryngectomy is best accomplished with tracheoesophageal speech, using a tracheostomal device that is a one-way valve directing air into the neopharynx during exhalation when the tracheostoma is occluded (Figure 3015). The individual accomplishes this with digital occlusion , but foam buttons and hands-free techniques also exist. There are several models of the electrolarynx, which achieves its sound by external vibration. Learning to use the device to optimize comprehensibility is a challenge to most patients; those listening to an individual using an electrolarynx must also be familiar with the sound to understand the speech. Some patients learn pure esophageal speech by forcing air into the esophagus and releasing the air while using the tongue, teeth, cheeks, and lips to produce speech. A speech therapist familiar with postlaryngectomy voice rehabilitation is an essential member of the patient care team for patients undergoing a partial or total laryngectomy. Nonsurgical Measures Photodynamic Therapy Photodynamic therapy is an emerging modality of treating early larynx cancer, as well as cancer arising from other primary mucosal sites of the head and neck. A photosensitizing agent (a chemical preferentially taken up by tumor tissue and sensitive to specific wavelengths of light) is administered intravenously. A laser is then used to activate the photosensitizing agent and induce the destruction of tumor tissue. This treatment has been shown to be effective in treating cancers as deep as 5 mm, with local control and survival rates similar to traditional treatment modalities. The side effects of photodynamic therapy include light sensitivity that can linger for several weeks after the administration of the photosensitizing agent. For this reason, patients must wear sun-protective clothing during this period of time and avoid being outside during the hours of maximal sun intensity. Radiation Treatment Techniques for Larynx Cancer Radiation given as the primary treatment for larynx cancer or as an adjuvant treatment after surgery is most often done using an external-beam technique; a dose of 60007000 cGy is administered to the primary site. When the risk of locoregional nodal metastasis in a clinically negative neck exceeds 1520%, 5000 cGy is delivered prophylactically to the neck as well. The indications for postoperative adjuvant radiation include advanced-stage disease, close or positive margins, extracapsular spread of tumor in a lymph node, perineural or angiolymphatic spread, subglottic extension, and the involvement of nodes in multiple neck levels (in particular, levels IV or V, or the mediastinum). Although conventional adjuvant radiation treatment consisted of radiation alone, two recent randomized trials have shown improved local control with concurrent radiation and cisplatin for certain risk factors. Patient selection for such treatment continues to be debated, but patients with good performance status and adverse tumor features should be seriously considered for postoperative adjuvant concurrent chemoradiation. As noted previously, newer protocols are using various combinations of radiation with systemic therapies for tumor sensitization and eradication of micrometastatic disease. Altered radiation schedules are also being studiedboth with and without systemic agents . Advances in treatment delivery with intensity-modulated radiation therapy (IMRT) have allowed for more accurate tumor dose delivery with greater sparing of normal tissue, including salivary gland preservation with reduced xerostomia. Before undergoing radiation, patients should have a thorough dental examination. When the field will encompass the oral cavity , carious teeth are extracted before starting radiation owing to the radiation-induced dental decay and increased risk of osteoradionecrosis. Short-term side effects of radiation, lasting up to 6 weeks after the conclusion of therapy, include mucositis, odynophagia, dysphagia, skin and erythema, altered taste, and edema. Common long-term side effects include varying degrees of xerostomia, fibrosis, and edema. Uncommon side effects include hypothyroidism, chondroradionecrosis, and osteoradionecrosis. As noted previously, an exceedingly rare complication is radiation-induced sarcoma. Chemotherapy for Larynx Cancer Chemotherapy had not traditionally been part of larynx cancer primary treatment protocols. Starting in the 1980s, organ-preserving protocols using chemotherapy in conjunction with radiation for advanced-stage laryngeal cancer have been compared with standard surgery and radiation treatment. Comparable survival rates have been shown with differing treatment morbidities. In general, lowered rates of distant metastasis are seen, although questionably higher rates of local recurrence are also cited in comparison with surgery and locoregional radiation protocols. Cisplatin and 5-fluorouracil are the two agents found to be the most effective against larynx cancer. Recently, paclitaxel (Taxol) and docetaxel (Taxotere) have demonstrated activity without the side effects of cisplatin, which include neurotoxicity, ototoxicity, and renal toxicity. Chemotherapy has been given in the neoadjuvant (induction) setting concurrent with radiation and also in the adjuvant setting. Even though successes have been reported for all three approaches, concurrent chemoradiation has generally been deemed the most successful. Trials with neoadjuvant and concurrent intra-arterial chemotherapy have shown excellent local tumor response in selected cases, but with enhanced local toxicity. Cisplatin is the most commonly used agent in concurrent protocols. Agents, such as amifostine, are being used to mitigate side effects and preserve salivary function in the setting of radiation. Chemotherapy may also be used for the palliation of advanced larynx cancer. Once again, cisplatin is the preferred agent, but methotrexate was historically used with some benefit. Chemotherapy is not considered a first-line treatment or standard of care for early-stage (Stages I and II) larynx cancer. Complications of Treatment The complications of larynx cancer reflect the treatment modality (or modalities) used. Vocal Problems Hoarseness may complicate any treatment of larynx cancer, even the smallest larynx cancer. Voice changes can be as subtle as the loss of vocal range, vocal fatigue, and lowered threshold for bouts of laryngitis. Deepening of the voice or a raspy, rough quality of the voice is common. Failure to achieve tracheoesophageal speech after a total laryngectomy can be due to hypertonicity or stricture of the neopharyngeal segment, an inappropriately positioned voice prosthesis, problems with digital occlusion of the stoma, or other neurologic impairment. Swallowing Problems After partial laryngectomy procedures, aspiration risk is significant. This can be due to surgical removal or to denervation, in whole or in part, of the protective mechanisms of the larynx. Acute side effects of radiation include mucositis, thick secretions, odynophagia, and edema, which all contribute to swallowing difficulties in the immediate peri-radiation period. Xerostomia is a long-term side effect of radiation that also contributes to dysphagia. Stricture, stenosis, or fibrosis of the pharyngoesophageal segment as a result of surgical scarring or as a residual effect of radiation can lead to intolerance of solid foods or an inability to take adequate nutrition by mouth. Loss of Taste and Smell Radiation can permanently damage taste buds, although this side effect is often transient. After total laryngectomy, anatomic changes result in a lack of airflow through the nose and mouth. This severely changes the patient's sense of smell and, therefore, the sense of taste. Fistula Development A fistula, or connection between the pharynx and skin of the neck, reflects the failure of the pharyngeal surgical closure to seal after laryngectomy. This results in the leakage of saliva and pharyngeal contents (including food) into the neck. When this initial fluid collection ruptures, leakage of mucoid and fluid material occurs onto the skin. Fistulas are more prone to occur in patients who have undergone previous radiation (up to 35% more likely) or surgery, and in those in whom the pharyngeal closure is tight. A fistula is more likely to occur if the nutritional status of the patient is poor (common) and may reflect a residual underlying cancer. Most fistulas close by secondary intention with conservative management, including feeding through a nasogastric or gastrostomy tube. Occasionally, surgical closure with a flap is advisable for vascular protection, for control of infection, or for facilitation of the delivery of indicated postoperative adjuvant therapy. Airway Problems Some patients undergoing partial laryngectomy procedures are left with either an inadequate laryngeal airway or significant aspiration; for these reasons, they remain dependent on tracheotomy tubes. Excessive laryngeal edema can also happen as a sequela of radiation treatment alone. For patients who undergo a total laryngectomy, excessive secretions and crusting mucus can occlude the tracheostoma. Patients who undergo total laryngectomy often have an increased air temperature sensitivity, which manifests by cough; the lack of airway protection may also result in increased risk of aspiration and drowning. Cranial Nerve Injury During the surgical dissection for a partial or total laryngectomy with neck dissection, cranial nerves VII (the marginal mandibular branch), IX, X, XI, and XII are encountered and are therefore at risk for potential injury. Injury can be temporary or permanent. Preoperatively, patients need to be counseled about the following potential postoperative complications: asymmetric smile and mouth closure, swallowing difficulties, hoarseness and aspiration, shoulder drop and range-of-motion limitation, hoarseness, and the impairment of tongue mobility. Similarly, patients with aggressive larynx tumors with neck extension or locoregional metastases may present with or develop these cranial nerve deficits because of tumor involvement of the nerve. Vascular Injuries and Events Stroke is a risk of laryngectomy and neck dissection, but occurs surprisingly infrequently. A long-term sequela of radiation to the neck is acceleration of carotid atherosclerosis, and patients who have undergone radiation to the neck have a greater risk for stroke because of this. In advanced tumors with necrosis and the resulting exposure of the carotid artery or the internal jugular vein, rupture (a carotid or jugular "blowout") is a risk. In cases of sentinel bleeds, angiographic embolization or stenting can prevent or stave off further bleeding. Flap coverage with vascularized tissue, when feasible , can protect against further bleeding. For patients who do experience a carotid blowout, the incidence of major debilitating stroke is > 50% in attempts at surgical salvage. Surgical salvage consists of ligating the carotid artery or more rarely attempting bypass. Major vessel rupture is otherwise a commonly fatal event. Dropped Shoulder Injury to the spinal accessory nerve during neck dissection results in a loss of trapezius muscle function, an inability to abduct the arm past 90, and downward and inward rotation of the shoulder. These limitations can also occur as a result of primary tumor or neck metastases involving the spinal accessory nerve. Patients complain of a loss of shoulder function and pain. With intensive physical therapy, these deficits and pain can be overcome by increasing the strength of the other muscles of the shoulder girdle. Tissue Fibrosis Because of radiation and surgery, which are augmented by the loss of the function of cranial nerve XI (when it occurs), larynx cancer patients often experience significant fibrosis of neck tissues. This manifests by stiffening, loss of range of motion, and pain. Fibrosis of the larynx and ankylosis of the cricoarytenoid joint have also been observed as a result of radiation treatment, leading to bilateral vocal cord immobility many years after the treatment. Hypothyroidism A loss of thyroid function can occur as a result of radiation to the lower anterior neck from a thyroidectomy done as part of laryngectomy, devascularization, or as a combined result of both. Hypothyroidism may not become apparent clinically or by serum tests until 612 months (or longer) after the completion of treatment for larynx cancer. Severe hypofunction may be responsible for poor healing of flaps and fistulas. For this reason, thyroid function tests should be performed periodically. Replacing the thyroid hormone with appropriately titrated doses of enteral thyroxin is curative, but requires periodic monitoring. Other Complications Other risks of laryngectomy include hematoma and infection. Long-Term Clinical Follow-Up Patients with larynx cancer should be followed up clinically in the same manner in which patients with cancer of the head and neck are generally followed up. After treatment is completed, routine office visits are scheduled at 4- to 6-week intervals. During these visits, a complete head and neck examination is performed, focusing on the primary site for signs of recurrence, but also screening for metachronous primary malignant lesions. So-called "second" primary lesions have an annual incidence of 47%. After the first year, visits can extend to every 2 months during the second year, every 3 months during the third and fourth years, and every 612 months thereafter. Most recurrences of head and neck cancer occur within the first 2 years after treatment. Individuals are considered to be cured of their index primary after 5 years of disease-free status. The signs and symptoms of recurrence are the same as those of the initial presentation, including hoarseness, dysphagia, otalgia, hemorrhage, cervical adenopathy, and pain. The findings of the physical examination, the evaluation for metastases, and the diagnostic tests are the same for recurrences as they were for the original occurrence. Ambrosch P, Kron M, Steiner W. Carbon dioxide laser microsurgery for early supraglottic carcinoma. Ann Otol Rhinol Laryngol. 1998;107(8):680. (Results of patients treated with laser microsurgery for early-stage supraglottic carcinoma showing comparable results to open supraglottic laryngectomy and superior functional results.) [PMID: 9716871]
| Back G, Sood S. The management of early laryngeal cancer: options for patients and therapists. Curr Opin Otolaryngol Head Neck Surg. 2005;13(2):85. (Study to evaluate the different treatment modalities for early laryngeal cancer.) [PMID: 15761281]
| Bernier J, Domenge C et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med. 2004;350:1945. (Study showing that the addition of concurrent chemotherapy to adjuvant radiation improves local control in selected patients with high-risk squamous cell carcinoma who have primary surgical treatment.) [PMID: 15128894]
| Chao KS, Majhail N, Huang CJ et al. Intensity modulated radiation therapy reduces late salivary toxicity without compromising tumor control in patients with oropharyngeal carcinoma: a comparison with conventional techniques. Radiother Oncol. 2001;61(3):275. (Series illustrating the efficacy of intensity-modulated radiation therapy in sparing salivary flow in patients with head and neck cancer without compromising tumor control.) [PMID: 11730977]
| Cooper JS, Pajak TF et al. Postoperative concurrent radiotherapy and chemotherapy for high risk squamous cell carcinoma of the head and neck. N Engl J Med. 2004;350:1937. (Study showing that the addition of concurrent chemotherapy to adjuvant radiation improves local control in selected patients with high-risk squamous cell carcinoma who have primary surgical treatment.) [PMID: 15128893]
| Dilkes MG et al. Treatment of primary mucosal head and neck squamous cell cancer using photodynamic therapy: results after 25 treated cases. J Laryngol Otol. 2003;117(9):713. (Study demonstrating the efficacy of Foscan, a photosensitizer, in the treatment of a variety of primary mucosal head and neck cancers.) [PMID: 14561360]
| Forastiere A, Goepfert H, Maor M et al. Concurrent chemotherapy and radiotherapy for organ preservation in laryngeal cancer. N Engl J Med. 2003;349(22):2091. (Trial establishing concurrent chemoradiation as the superior to sequential chemoradiation for locally advanced larynx cancer. Concurrent therapy is now the mainstay of treatment.) [PMID: 14645636]
| Galli J, De Corso E, Volante M et al. Postlaryngectomy pharyngocutaneous fistula: incidence, predisposing factors, and therapy. Otolaryng Head Neck Surg. 2005;133(5):689. (Study evaluating the predisposing factors, incidence, and management of pharyngocutaneous fistula.) [PMID: 16274794]
| Gallo A, Manciocco V, Simonelli M et al. Supracricoid partial laryngectomy in the treatment of laryngeal cancer: univariate and multivariate analysis of prognostic factors. Arch Otolaryngol Head Neck Surg. 2005;131(7):620. (Study evaluating the results of supracricoid laryngectomy in the treatment of glottic and supraglottic cancers, showing that it is effective in maintaining laryngeal functions while achieving a high rate of local control.) [PMID: 16027286]
| Krengli M, Policarpio, Manfredda I et al. Voice quality after T1a glottic carcinoma. Acta Oncologica. 2004;33(3):284. (Study examining the functional outcome of patients treated with radiation or CO 2 laser excision and shows that radiation results in superior voice quality.) laser excision and shows that radiation results in superior voice quality.) [PMID: 15244235]
| Laccourreye O, Hans S, Borzog-Grayeli A, Maulard-Durdux C, Brasnu D, Housset M. Complications of postoperative radiation therapy after partial laryngectomy in supraglottic cancer: a long term evaluation. Otolaryngol Head Neck Surg. 2000;122(5):752. (Series examining complications and functional status of patients treated with partial laryngectomy and postoperative radiation therapy.) [PMID: 10793360]
| Mortuaire G, Francois J, Wiel E, Chevalier D. Local recurrence after CO 2 laser cordectomy for early glottic carcinoma. Laryngoscope. 2006;116(1):101. (Study evaluating the prognostic factors of local recurrence after endoscopic cordectomies.) [PMID: 16481819]
| Patel S, See A, Williamson P et al. Radiation induced sarcoma of the head and neck. Head Neck. 1999;21(4):346. (Series illustrating the incidence of delayed sarcoma development in patients treated with definitive radiation therapy for cancer of the head and neck.) [PMID: 10376755]
| Paydarfar JA, Birkmeyer NJ. Complications in head and neck surgery: a meta-analysis of postlaryngectomy pharyngocutaneous fistula. Arch Otolaryngol Head Neck Surg. 2006;132(1):67. (Paper summarizing the risk factors for postlaryngectomy pharyngocutaneous fistula.) [PMID: 16415432]
| Peretti G, Piazza C, Bolzoni A. Endoscopic management for early glottic cancer: indications and oncologic outcome. Otolaryngol Clin North Am. 2006;39(1):173. (Review of the indications and outcome for endoscopic management of early glottic cancer.) [PMID: 16469662]
| Pfister DG, Laurie SA, Weinstein GS et al. American Society of Clinical Oncology Clinical Practice Guideline for the Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer. J Clin Oncol. 2006. (American Society of Clinical Oncology guidelines for treatment of laryngeal cancer.) [PMID: 16832122]
| Prepageran N, Raman R. Delayed complication of radiotherapy: Laryngeal fibrosis and bilateral vocal cord immobility. Med J Malaysia. 2005;60(3):377. (Case report of bilateral vocal cord immobility many years after treatment with radiation.) [PMID: 16379198]
| Schweitzer VG. Photofrin-mediated photodynamic therapy for treatment of early stage oral cavity and laryngeal malignancies. Lasers Surg Med. 2001;29(4):305. (Review of larynx and oral cavity carcinomas either not amenable to or failing conventional treatment in which photodynamic therapy demonstrated high rates of complete response and cure with minimal side effects.) [PMID: 11746107]
| Sessions DG, Lenox J, Spector GJ. Supraglottic laryngeal cancer: analysis of treatment results. Laryngoscope. 2005;115(8):1402. (Study analyzing the results of different management strategies for supraglottic laryngeal cancer.) [PMID: 16094113]
| Sigston E, de Mones E, Babin E et al. Early stage glottic cancer: oncological results and margins in laser cordectomy. Arch Otolaryngol Head Neck Surg. 2006;132(2):147. (Study assessing the local control of laser cordectomies compared with external partial laryngectomy procedures in the treatment of early-stage glottic cancers.) [PMID: 16490871]
| Strome SE, Weinman EC. Advanced larynx cancer. Curr Treat Options Oncol. 2002;3(1):11. (Review of treatment philosophy and options for advanced larynx cancer.) [PMID: 12057083]
| Terrell J, Fisher S, Wolf G. Long term quality of life after treatment of laryngeal cancer. Arch Otolaryngol Head Neck Surg. 1998;124: 964. (Study examining the quality of life in patients who enrolled in the VA larynx study with findings of superior results in those who had preserved larynges.) [PMID: 9738814]
| Urba S, Wolf G, Eisbruch A et al. Single-cycle induction chemotherapy selects patients with advanced laryngeal cancer for combined chemoradiation: a new treatment paradigm. J Clin Oncol. 2006;24(4):593. (Study comparing primary chemoradiation with radiation alone or conventional laryngectomy in the treatment of advanced laryngeal cancer.) [PMID: 16380415]
| Wolf GT. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer: The Department of Veterans Affairs Laryngeal Cancer Study Group. N Engl J Med. 1991;324:1685. (Study showing that survival with chemotherapy and radiation was equivalent to surgery in locally advanced larynx cancer, thus establishing the organ preservation as the mainstay of treatment.) [PMID: 2034244]
| Zacharek MA, Pasha R, Meleca RJ et al. Functional outcomes after supracricoid laryngectomy. Laryngoscope. 2001;111(9):1558. (Report of adequate voice and swallowing at 5-year follow-up on 10 patients who underwent supracricoid laryngectomy.) [PMID: 11568604]
| Zhang B, Xu ZG, Tang PZ. Elective neck dissection for laryngeal cancer in the clinically negative neck. J Surg Oncol. 2006;93(6):464. (Study evaluating the efficacy of a lateral neck dissection in the elective treatment of the clinically negative necks in patients with laryngeal cancer.) [PMID: 16615158]
| | | Prognosis Cure for larynx cancer, defined as 5-year disease-free survival, is generally better than for other primary site tumors of the upper aerodigestive tract (Table 304). This reflects the prevalence of primary glottic tumors over primary supraglottic tumors and the early stage at which glottic tumors are diagnosed. Persistent hoarseness is one indication for which an individual will seek clinical care usually before the emergence of nodal metastasis. Nonetheless, 5-year survival rates have not improved over the last three decades despite advances in surgical technique, the expansion of treatment options, and decrease in morbidity. | Table 304A. Larynx Cancer: 5-Year Survival Rates by Stage.
| | | Stage I > 95% | | Stage II 8590% | | Stage III 7080% | | Stage IV 5060% | | All Stages 68% | |
| | Table 304B. Larynx Cancer: 5-Year Survival Rates by Site and Stage.
| | | Supraglottis | Glottis | Subglottis | | Stage I 5382% | Stage I 74100% | All Stages 3642% | | Stage II 5064% | Stage II 6476% | | | Stage III 5060% | Stage III 5060% | | | Stage IV < 50% | Stage IV 3057% | | |
| Ganly I, Patel SG, Matsuo J et al. Results of surgical salvage after failure of definitive radiation therapy for early-stage squamous cell carcinoma of the glottic larynx. Arch Otolaryngol Head Neck Surg. 2006;132(1):59. (Study reporting the results of partial or total laryngectomy for recurrent or persistent laryngeal cancer after definitive radiotherapeutic treatment.) [PMID: 16415431]
| | | | |
 Print Close Window
Print Close Window